
Optimization of Thyroid Volume Determination by Stitched 3D-Ultrasound Data Sets in Patients with Structural Thyroid Disease
 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
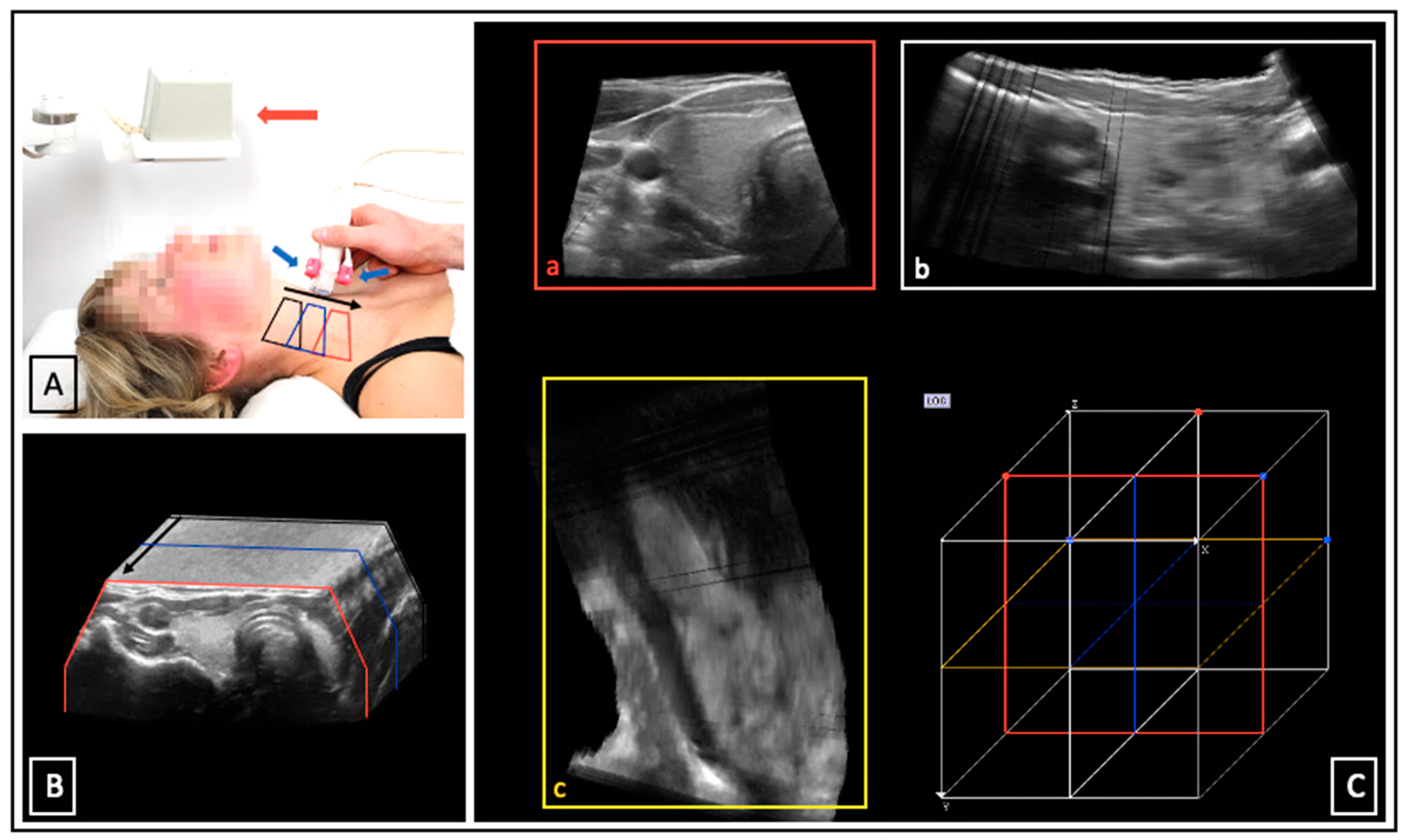
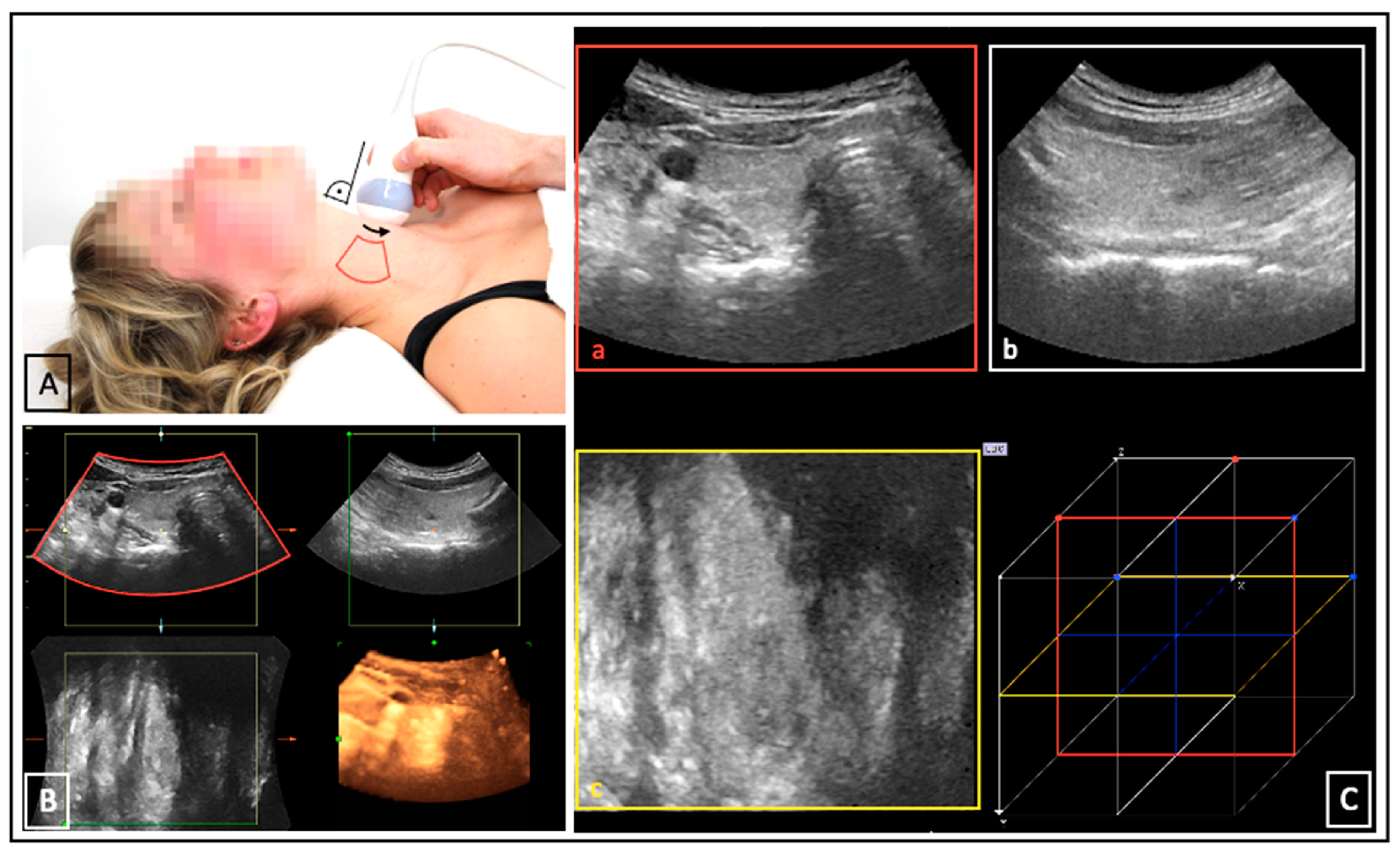
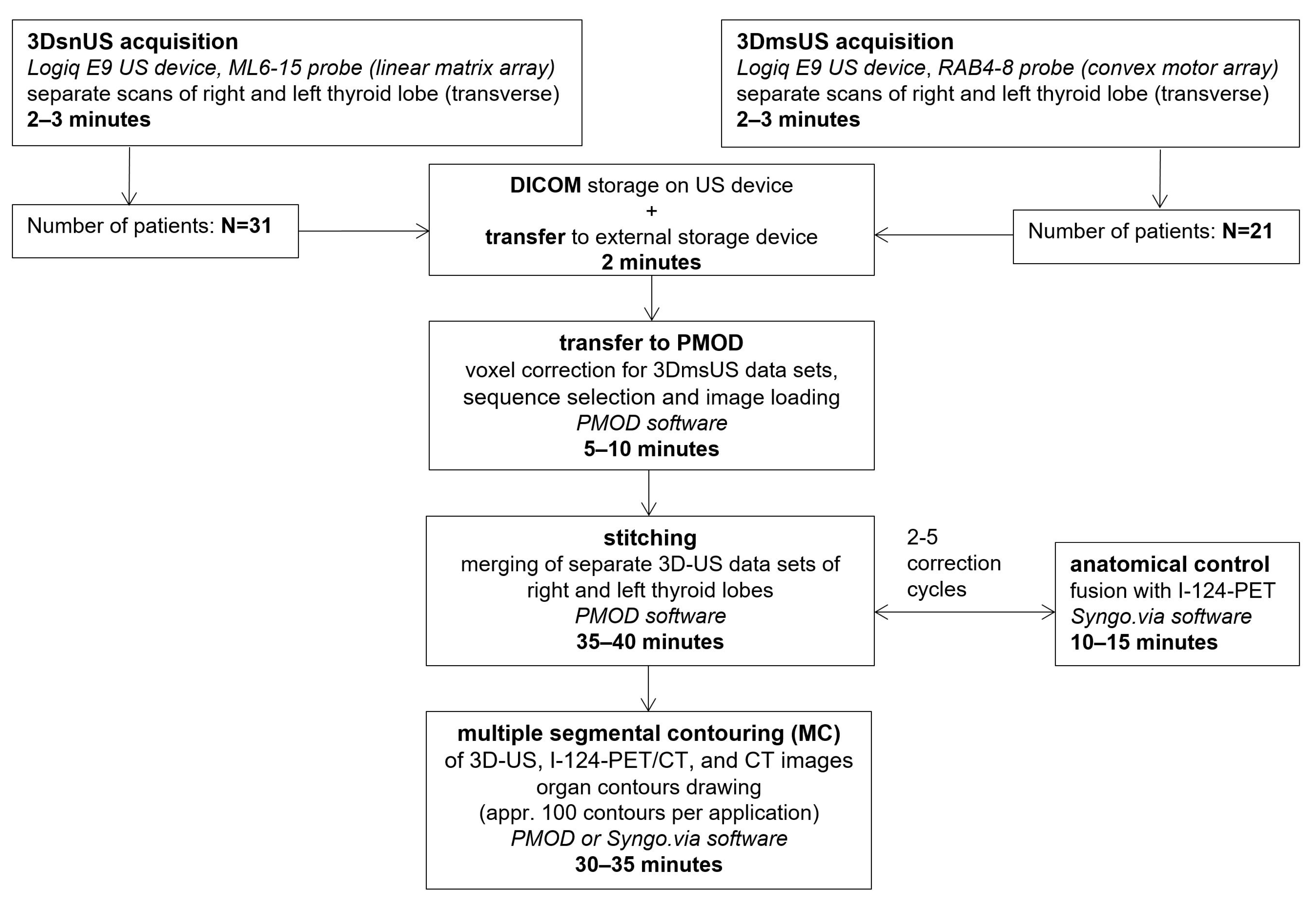
2.1. Ultrasound Examinations
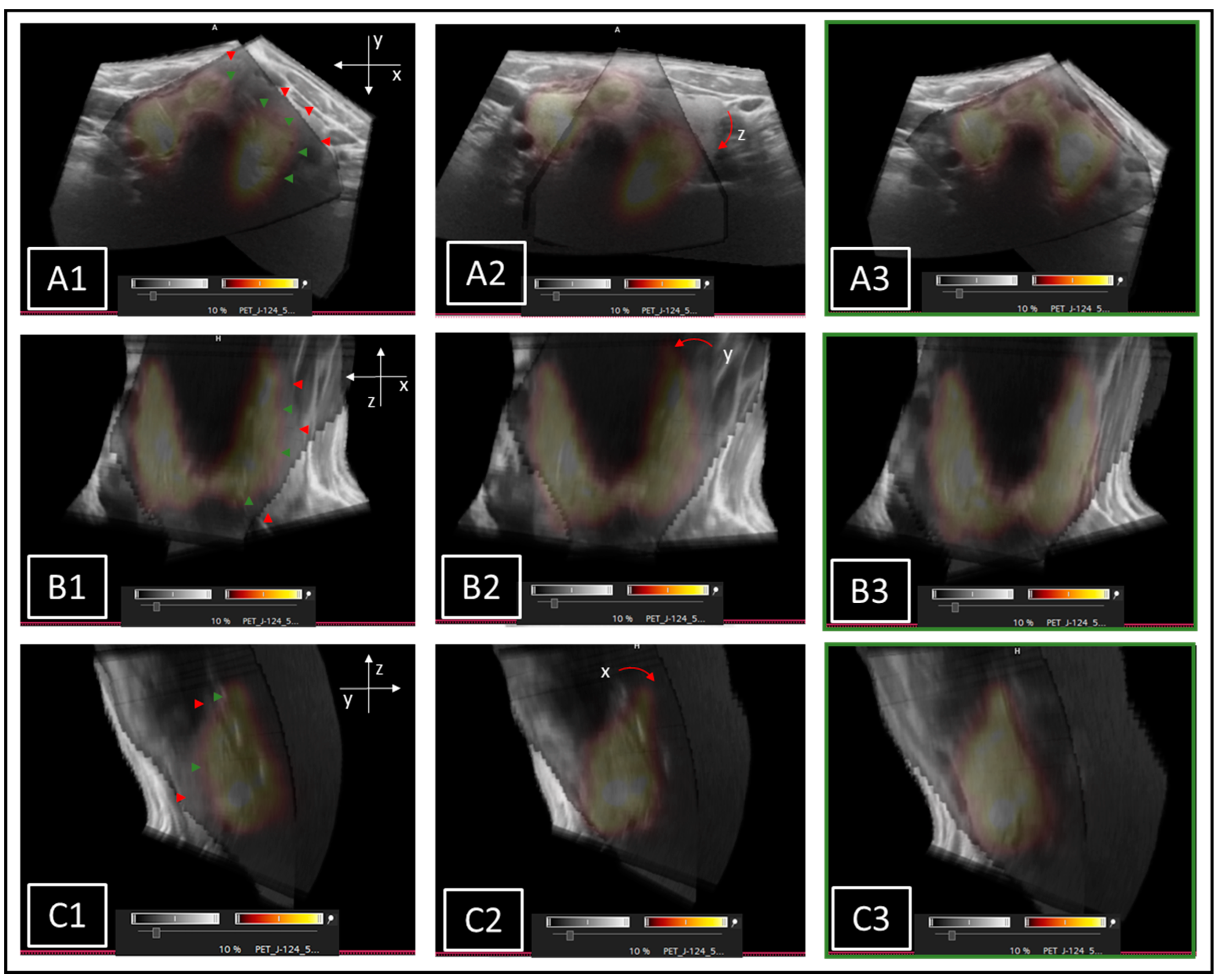
2.2. Stitching of 3D-US Data Sets
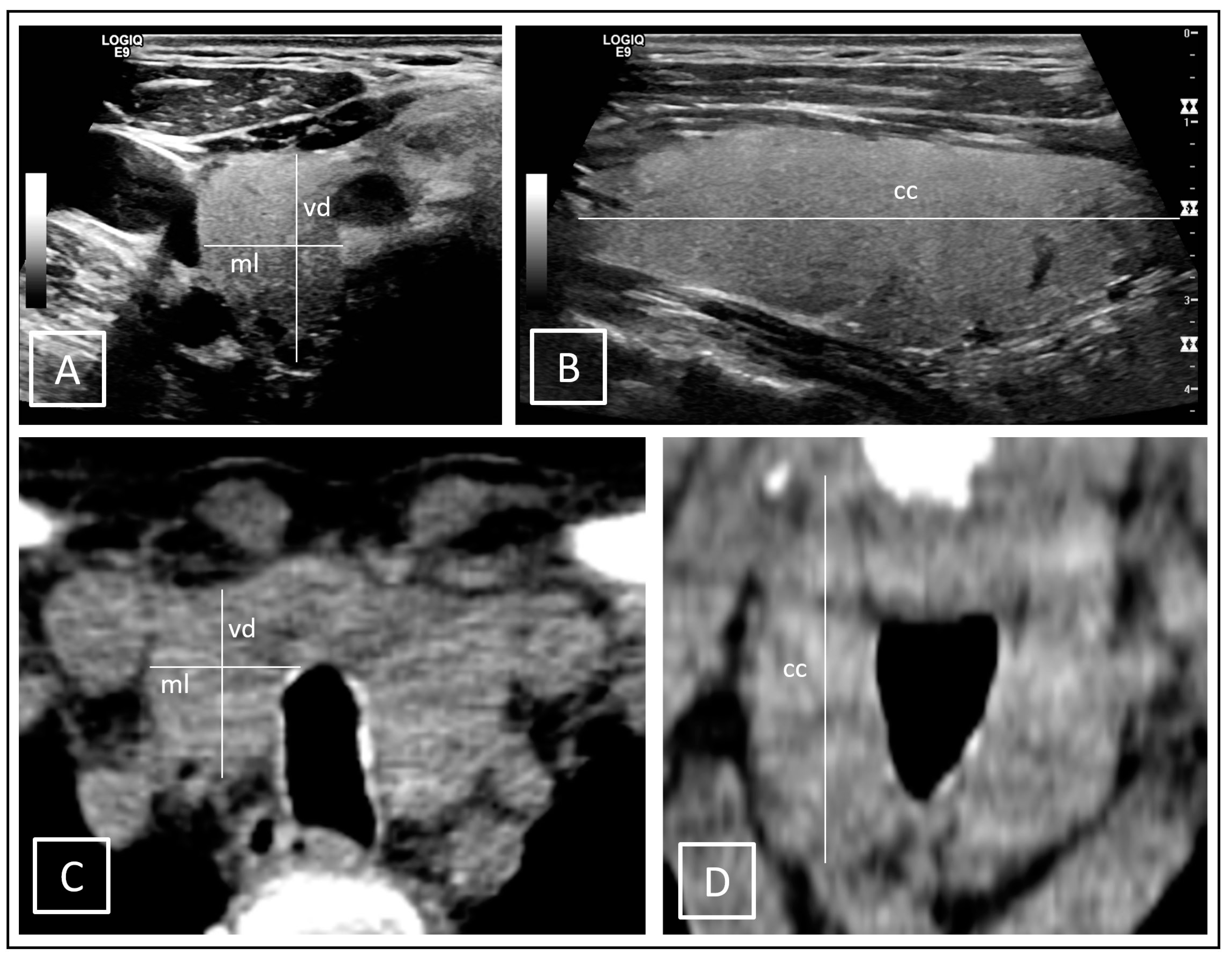
2.3. Volumetric Determination
2.4. Statistics
3. Results
4. Discussion
- in large thyroid glands, the maximum cranial–caudal diameter could not be measured correctly on conUS because the respective organ pols were not covered within the limited FOV
- substantial deviation of the organ shape from the estimated ellipsoid model due to nodules and cysts, especially in the isthmus.
Limitations
- The investigated patient group consisted of subjects who received further diagnostics due to unclear constellations of conventional diagnostics. Thus, the 3D-US data were collected from a complex pre-selected patient cohort that does not reflect the average population. In the present study, the focus was set to patients with structural thyroid diseases in order to investigate the value of the novel methodology with regard to this aspect.
- Due to the small number of cases, the results have limited reliability statistically. Furthermore, the sample sizes of patients with 3DsnUS and 3DmsUS were different; only 21 of the 31 patients received 3DmsUS.
- MC volume determinations were performed exclusively by one examiner. Accordingly, no statement regarding interobserver variability is possible. On the other hand, there was no bias due to different levels of experience.
- Intraobserver variability was not investigated because each measurement was only carried out once. Given a total of 5.183 manually drawn contours (MC analyses), no effort was made to repeat the measurements.
5. Conclusions and Outlook
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Reiners, C.; Wegscheider, K.; Schicha, H.; Theissen, P.; Vaupel, R.; Wrbitzky, R.; Schumm-Draeger, P.-M. Prevalence of thyroid disorders in the working population of Germany: Ultrasonography screening in 96,278 unselected employees. Thyroid 2004, 14, 926–932. [Google Scholar] [CrossRef]
- Verburg, F.A.; Grelle, I.; Tatschner, K.; Reiners, C.; Luster, M. Prevalence of thyroid disorders in elderly people in Germany. A screening study in a country with endemic goitre. Nuklearmedizin 2017, 56, 9–13. [Google Scholar] [CrossRef]
- Meltzer, C.J.; Irish, J.; Angelos, P.; Busaidy, N.L.; Davies, L.; Dwojak, S.; Ferris, R.L.; Haugen, B.R.; Harrell, R.M.; Haymart, M.R.; et al. American Head and Neck Society Endocrine Section clinical consensus statement: North American quality statements and evidence-based multidisciplinary workflow algorithms for the evaluation and management of thyroid nodules. Head Neck 2019, 41, 843–856. [Google Scholar] [CrossRef] [Green Version]
- Richman, D.M.; Frates, M.C. Ultrasound of the Normal Thyroid with Technical Pearls and Pitfalls. Radiol. Clin. N. Am. 2020, 58, 1033–1039. [Google Scholar] [CrossRef] [PubMed]
- Hegedüs, L. Thyroid ultrasound. Endocrinol. Metab. Clin. N. Am. 2001, 30, 339–360. [Google Scholar] [CrossRef] [PubMed]
- Curriculum for Fundamentals of Ultrasound in Clinical Practice. J. Ultrasound Med. 2019, 38, 1937–1950. [CrossRef] [Green Version]
- Seifert, P.; Maikowski, I.; Winkens, T.; Kühnel, C.; Gühne, F.; Drescher, R.; Freesmeyer, M. Ultrasound Cine Loop Standard Operating Procedure for Benign Thyroid Diseases—Evaluation of Non-Physician Application. Diagnostics 2021, 11, 67. [Google Scholar] [CrossRef]
- Luster, M.; Pfestroff, A.; Hänscheid, H.; Verburg, F.A. Radioiodine Therapy. Semin. Nucl. Med. 2017, 47, 126–134. [Google Scholar] [CrossRef] [Green Version]
- Jongekkasit, I.; Jitpratoom, P.; Sasanakietkul, T.; Anuwong, A. Transoral Endoscopic Thyroidectomy for Thyroid Cancer. Endocrinol. Metab. Clin. N. Am. 2019, 48, 165–180. [Google Scholar] [CrossRef] [PubMed]
- Miccoli, P.; Fregoli, L.; Rossi, L.; Papini, P.; Ambrosini, C.E.; Bakkar, S.; De Napoli, L.; Aghababyan, A.; Matteucci, V.; Materazzi, G. Minimally invasive video-assisted thyroidectomy (MIVAT). Gland. Surg. 2020, 9 (Suppl. 1), 1–5. [Google Scholar] [CrossRef]
- Shapiro, R.S. Panoramic ultrasound of the thyroid. Thyroid 2003, 13, 177–181. [Google Scholar] [CrossRef]
- Schlögl, S.; Andermann, P.; Luster, M.; Reiners, C.; Lassmann, M. A novel thyroid phantom for ultrasound volumetry: Determination of intraobserver and interobserver variability. Thyroid 2006, 16, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Andermann, P.; Schlögl, S.; Mäder, U.; Luster, M.; Lassmann, M.; Reiners, C. Intra- and interobserver variability of thyroid volume measurements in healthy adults by 2D versus 3D ultrasound. Nuklearmedizin 2007, 46, 1–7. [Google Scholar]
- Licht, K.; Darr, A.; Opfermann, T.; Winkens, T.; Freesmeyer, M. 3D ultrasonography is as accurate as low-dose CT in thyroid volumetry. Nuklearmedizin 2014, 53, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Lyshchik, A.; Drozd, V.; Reiners, C. Accuracy of three-dimensional ultrasound for thyroid volume measurement in children and adolescents. Thyroid 2004, 14, 113–120. [Google Scholar] [CrossRef]
- Freesmeyer, M.; Wiegand, S.; Schierz, J.-H.; Winkens, T.; Licht, K. Multimodal evaluation of 2-D and 3-D ultrasound, computed tomography and magnetic resonance imaging in measurements of the thyroid volume using universally applicable cross-sectional imaging software: A phantom study. Ultrasound Med. Biol. 2014, 40, 1453–1462. [Google Scholar] [CrossRef]
- Freesmeyer, M.; Darr, A.; Schierz, J.-H.; Schleußner, E.; Wiegand, S.; Opfermann, T. 3D ultrasound DICOM data of the thyroid gland. First experiences in exporting, archiving, second reading and 3D processing. Nuklearmedizin 2012, 51, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Prager, R.W.; Ijaz, U.Z.; Gee, A.H.; Treece, G.M. Three-dimensional ultrasound imaging. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2010, 224, 193–223. [Google Scholar] [CrossRef]
- Freesmeyer, M.; Knichel, L.; Kuehnel, C.; Winkens, T. Stitching of sensor-navigated 3D ultrasound datasets for the determination of large thyroid volumes—A phantom study. Med. Ultrason. 2018, 20, 480–486. [Google Scholar] [CrossRef] [Green Version]
- Seifert, P.; Winkens, T.; Knichel, L.; Kühnel, C.; Freesmeyer, M. Stitching of 3D ultrasound datasets for the determination of large thyroid volumes—Phantom study part II: Mechanically-swept probes. Med. Ultrason. 2019, 21, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Seifert, P.; Winkens, T.; Kühnel, C.; Gühne, F.; Freesmeyer, M. I-124-PET/US Fusion Imaging in Comparison to Conventional Diagnostics and Tc-99m Pertechnetate SPECT/US Fusion Imaging for the Function Assessment of Thyroid Nodules. Ultrasound Med. Biol. 2019, 45, 2298–2308. [Google Scholar] [CrossRef]
- Winkens, T.; Seifert, P.; Hollenbach, C.; Kühnel, C.; Gühne, F.; Freesmeyer, M. The FUSION iENA Study: Comparison of I-124-PET/US Fusion Imaging with Conventional Diagnostics for the Functional Assessment of Thyroid Nodules by Multiple Observers. Nuklearmedizin 2019, 58, 434–442. [Google Scholar] [CrossRef] [PubMed]
- Freesmeyer, M.; Winkens, T.; Weissenrieder, L.; Kühnel, C.; Gühne, F.; Schenke, S.; Drescher, R.; Seifert, P. Fusion iENA Scholar Study: Sensor-Navigated I-124-PET/US Fusion Imaging versus Conventional Diagnostics for Retrospective Functional Assessment of Thyroid Nodules by Medical Students. Sensors 2020, 20, 3409. [Google Scholar] [CrossRef]
- Brunn, J.; Block, U.; Ruf, G.; Bos, I.; Kunze, W.P.; Scriba, P.C. Volumetric analysis of thyroid lobes by real-time ultrasound (author’s transl). Dtsch. Med. Wochenschr 1981, 106, 1338–1340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nygaard, B.; Nygaard, T.; Court-Payen, M.; Jensen, L.I.; Soe-Jensen, P.; Gerhard Nielsen, K.; Fugl, M.; Hegedus, L. Thyroid volume measured by ultrasonography and CT. Acta Radiol. 2002, 43, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Shu, J.; Zhao, J.; Guo, D.; Luo, Y.; Zhong, W.; Xie, W. Accuracy and reliability of thyroid volumetry using spiral CT and thyroid volume in a healthy, non-iodine-deficient Chinese adult population. Eur. J. Radiol. 2011, 77, 274–280. [Google Scholar] [CrossRef]
- Cheung, W.; Stevenson, G.N.; de Melo Tavares Ferreira, A.E.G.; Alphonse, J.; Welsh, A.W. Feasibility of image registration and fusion for evaluation of structure and perfusion of the entire second trimester placenta by three-dimensional power Doppler ultrasound. Placenta 2020, 94, 13–19. [Google Scholar] [CrossRef]
- Brekke, S.; Rabben, S.I.; Støylen, A.; Haugen, A.; Haugen, G.U.; Steen, E.N.; Torp, H. Volume stitching in three-dimensional echocardiography: Distortion analysis and extension to real time. Ultrasound Med. Biol. 2007, 33, 782–796. [Google Scholar] [CrossRef]
- Chen, Y.; Manzanera, S.; Mompeán, J.; Ruminski, D.; Grulkowski, I.; Artal, P. Increased crystalline lens coverage in optical coherence tomography with oblique scanning and volume stitching. Biomed. Opt. Express 2021, 12, 1529–1542. [Google Scholar] [CrossRef]
- Sun, H.; Yang, J.; Fan, R.; Xie, K.; Wang, C.; Ni, X. Stepwise local stitching ultrasound image algorithms based on adaptive iterative threshold Harris corner features. Medicine 2020, 99, e22189. [Google Scholar] [CrossRef]
- Westphal, J.G.; Winkens, T.; Kühnel, C.; Freesmeyer, M. Low-activity 124I-PET/low-dose CT versus 131I probe measurements in pretherapy assessment of radioiodine uptake in benign thyroid diseases. J. Clin. Endocrinol. Metab. 2014, 99, 2138–2145. [Google Scholar] [CrossRef] [Green Version]
- Reinartz, P.; Sabri, O.; Zimny, M.; Nowak, B.; Cremerius, U.; Setani, K.; Büll, U. Thyroid volume measurement in patients prior to radioiodine therapy: Comparison between three-dimensional magnetic resonance imaging and ultrasonography. Thyroid 2002, 12, 713–717. [Google Scholar] [CrossRef]
- Miccoli, P.; Minuto, M.N.; Orlandini, C.; Galleri, D.; Massi, M.; Berti, P. Ultrasonography estimated thyroid volume: A prospective study about its reliability. Thyroid 2006, 16, 37–39. [Google Scholar] [CrossRef] [PubMed]
- Hussy, E.; Voth, E.; Schicha, H. Sonographic determination of thyroid volume—Comparison with surgical data. Nuklearmedizin 2000, 39, 102–107. [Google Scholar] [CrossRef] [PubMed]
- Shabana, W.; Peeters, E.; De Maeseneer, M. Measuring thyroid gland volume: Should we change the correction factor? Am. J. Roentgenol. 2006, 186, 234–236. [Google Scholar] [CrossRef] [PubMed]
- Knudsen, N.; Bols, B.; Bülow, I.; Jørgensen, T.; Perrild, H.; Ovesen, L.; Laurberg, P. Validation of ultrasonography of the thyroid gland for epidemiological purposes. Thyroid 1999, 9, 1069–1074. [Google Scholar] [CrossRef]
- Ying, M.; Yung, D.M.; Ho, K.K. Two-dimensional ultrasound measurement of thyroid gland volume: A new equation with higher correlation with 3-D ultrasound measurement. Ultrasound Med. Biol. 2008, 34, 56–63. [Google Scholar] [CrossRef]
- Schlögl, S.; Werner, E.; Lassmann, M.; Terekhova, J.; Muffert, S.; Seybold, S.; Reiners, C. The use of three-dimensional ultrasound for thyroid volumetry. Thyroid 2001, 11, 569–574. [Google Scholar] [CrossRef]
- Ng, E.; Chen, T.; Lam, R.; Sin, D.; Ying, M. Three-dimensional ultrasound measurement of thyroid volume in asymptomatic male Chinese. Ultrasound Med. Biol. 2004, 30, 1427–1433. [Google Scholar] [CrossRef]
- Ying, M.; Sin, M.-H. Comparison of extended field of view and dual image ultrasound techniques: Accuracy and reliability of distance measurements in phantom study. Ultrasound Med. Biol. 2005, 31, 79–83. [Google Scholar] [CrossRef]
- Rago, T.; Bencivelli, W.; Scutari, M.; Di Cosmo, C.; Rizzo, C.; Berti, P.; Miccoli, P.; Pinchera, A.; Vitti, P. The newly developed three-dimensional (3D) and two-dimensional (2D) thyroid ultrasound are strongly correlated, but 2D overestimates thyroid volume in the presence of nodules. J. Endocrinol. Investig. 2006, 29, 423–426. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.-R.; Lu, L.; Zhang, J.-Y.; Huo, T.-T.; Liu, S.-X.; Ye, Z.-W. Application of Artificial Intelligence in Medicine: An Overview. Curr. Med. Sci. 2021, 41, 1105–1115. [Google Scholar] [CrossRef] [PubMed]
- Castiglioni, I.; Rundo, L.; Codari, M.; Di Leo, G.; Salvatore, C.; Interlenghi, M.; Gallivanone, F.; Cozzi, A.; D’Amico, N.C.; Sardanelli, F. AI applications to medical images: From machine learning to deep learning. Phys. Med. 2021, 83, 9–24. [Google Scholar] [CrossRef] [PubMed]
- Feldkamp, A. Neue Entwicklungen im Ultraschall. Pädiatrie 2020, 32, 28–31. [Google Scholar] [CrossRef]
- Kollorz, E.N.K.; Hahn, D.A.; Linke, R.; Goecke, T.W.; Hornegger, J.; Kuwert, T. Quantification of thyroid volume using 3-D ultrasound imaging. IEEE Trans. Med. Imaging 2008, 27, 457–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, C.-Y.; Lei, Y.-F.; Tseng, C.-H.; Shih, S.-R. Thyroid segmentation and volume estimation in ultrasound images. IEEE Trans. Biomed. Eng. 2010, 57, 1348–1357. [Google Scholar] [CrossRef]
- Trimboli, P.; Ruggieri, M.; Fumarola, A.; D’Alò, M.; Straniero, A.; Maiuolo, A.; Ulisse, S.; D’Armiento, M. A mathematical formula to estimate in vivo thyroid volume from two-dimensional ultrasonography. Thyroid 2008, 18, 879–882. [Google Scholar] [CrossRef]
- Malago, R.; D’Onofrio, M.; Ferdeghini, M.; Mantovani, W.; Colato, C.; Brazzarola, P.; Motton, M.; Mucelli, R.P. Thyroid volumetric quantification: Comparative evaluation between conventional and volumetric ultrasonography. J. Ultrasound Med. 2008, 27, 1727–1733. [Google Scholar] [CrossRef]
- Poudel, P.; Illanes, A.; Sheet, D.; Friebe, M. Evaluation of Commonly Used Algorithms for Thyroid Ultrasound Images Segmentation and Improvement Using Machine Learning Approaches. J. Healthc. Eng. 2018, 2018, 8087624. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | 3DsnUS | 3DmsUS |
|---|---|---|
| Probe | ML6-15 (linear matrix array) | RAB4-8 (convex 3D motor array) |
| contrast harmonic imaging (CHI) | on | on |
| CrossBeam function | max | max |
| VirtualConvex Mode | on | not available |
| used frequencies | 10–15 MHz (individually optimized) | 6–8 MHz (individually optimized) |
| depth; mean (min-max) | 5 cm (3–7 cm) | 5.5 cm (5–8 cm) |
| number of foci; mean (min-max) | 3 (1–3) | not adjustable |
| gain value; mean (min-max) | 47 (38–67) | 62 (58–90) |
| transmitting power | 100% | 100% |
| dynamic range | 69 dB | 69 dB |
| angle | not applicable | 84° (max) |
| image quality | not applicable | max |
| Method | N | r | Mean | SD | Median | Range (Min–Max) | LoA (Min) | LoA (Max) |
|---|---|---|---|---|---|---|---|---|
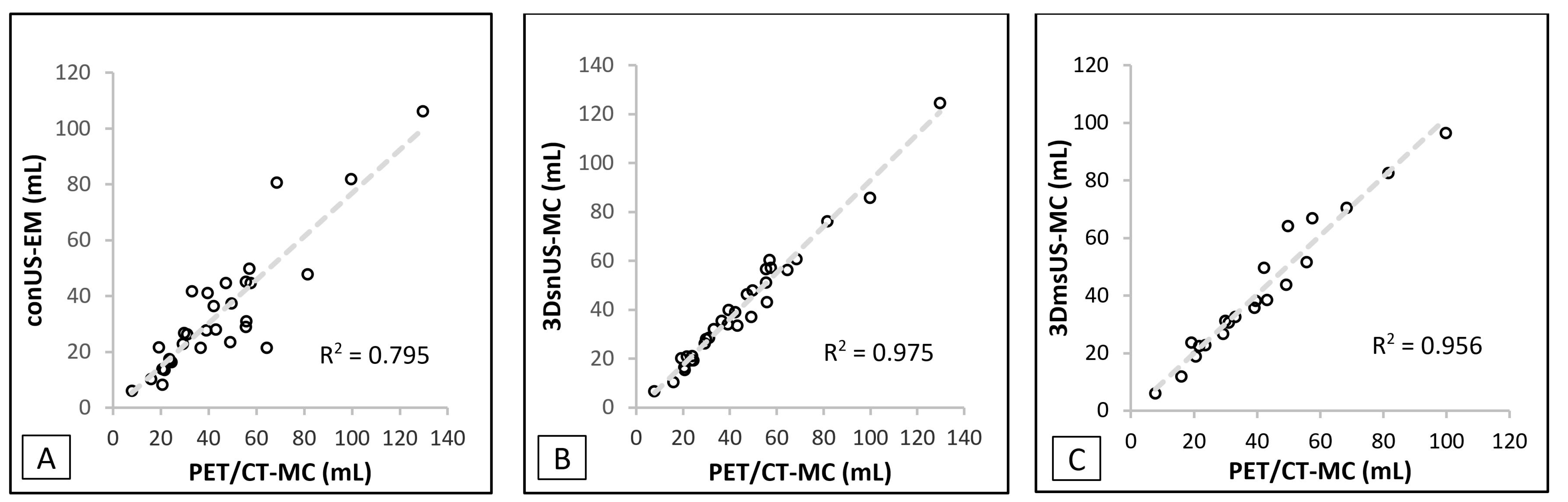
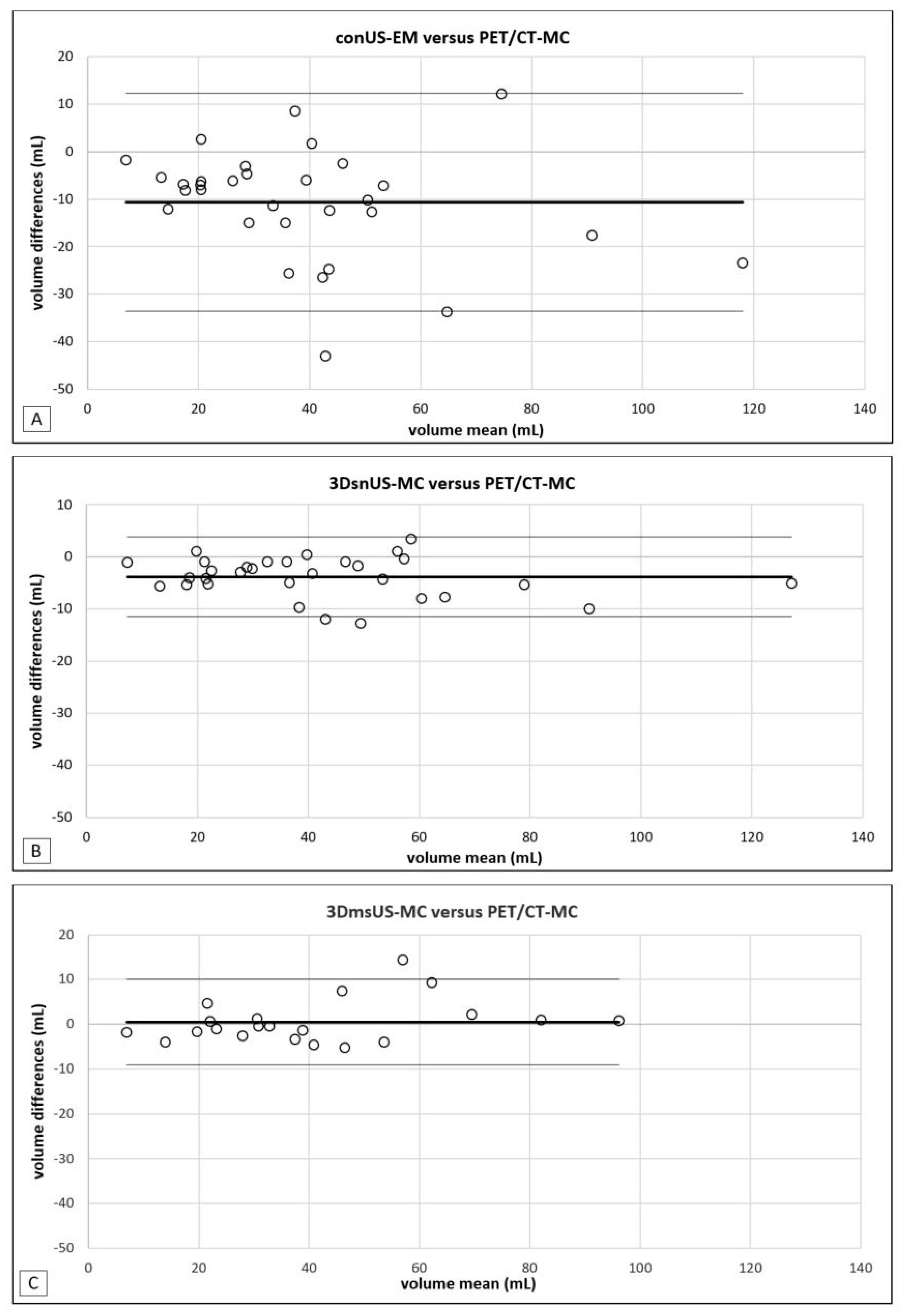
| conUS-EM | 31 | 0.892, p < 0.0001 | 33.6 | 22.5 | 27.8 | 6.0–106.2 | −10.5 | 77.7 |
| 3DsnUS-MC | 31 | 0.988, p < 0.0001 | 40.3 | 24.6 | 35.7 | 6.8–124.7 | −7.9 | 88.5 |
| 3DmsUS-MC | 21 | 0.978, p < 0.0001 | 41.2 | 23.6 | 35.8 | 6.0–96.5 | −5.1 | 87.5 |
| CT-EM | 31 | 0.956, p < 0.0001 | 41.9 | 27.0 | 35.3 | 6.0–121.6 | −11.0 | 94.8 |
| CT-MC | 31 | 0.986, p < 0.0001 | 44.5 | 24.9 | 41.2 | 7.3–126.5 | −4.3 | 93.3 |
| PET/CT-MC | 31 | reference | 44.1 | 25.8 | 39.5 | 7.8–129.7 | −6.3 | 94.9 |
| Authors | Objects | 3D-US | Stitching | Method | Reference Standard | Results | |||
|---|---|---|---|---|---|---|---|---|---|
| Phantoms | Patients | sn | ms | EM | MC | ||||
| Schlögl et al., 2001 [38] | X | X | X | - | X | phantoms, post-mortem | D(%): 2.4 ± 8% (phantoms) D(%): −3.6 ± 9.7% (post-mortem) Vm: 29.1 mL | ||
| Ng et al., 2004 [39] | X | X | X | - | X | phantoms | r = 0.991–0.998 (p < 0.001) | ||
| Lyshchik et al., 2004 [15] | X | X | - | X | Post-surgery | D(%): 1.8 ± 5.2%; Vm: 7 mL | |||
| Ying et al., 2005 [40] | X | X | - | X | 2D | - | |||
| Rago et al., 2006 [41] | X | X | - | X | 3D-US | - | |||
| Schlögl et al., 2006 [12] | X | X | - | X | phantoms | D(%): 0.6 ± 1.7% | |||
| Andermann et al., 2007 [13] | X | X | - | X | 3D-US | - | |||
| Ying et al., 2008 [37] | X | X | - | X | 3D-US | - | |||
| Freesmeyer et al., 2014 [16] | X | X | X | - | X | X | phantoms | D(%) 3DsnMC: −0.9 ± 5.2–0.9 ± 3.2% D(%) 3DmsMC: 0.7 ± 4.6–2.8 ± 3.4% volumes: 10–200 mL | |
| Licht et al., 2014 [14] | X | X | - | X | X | CT | D(%) MC: −1.1 ± 5.2%; Vm: 57.1 mL | ||
| Freesmeyer et al., 2018, Seifert et al., 2019 [19,20] | X | X | X | X | X | X | phantoms | D(%) 3DsnMC: −2.8 ± 2.4–1.4 ± 3.1% D(%) 3DmsMC: 1.1 ± 3.6–3.2 ± 2.2% volumes: 50–400 mL | |
| present study | X | X | X | X | X | I-124-PET/CT | D(%) 3DsnMC: −3.7 ± 3.7 D(%) 3DmsMC: 0.6 ± 4.8 Vm: 44.1 mL | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seifert, P.; Ullrich, S.-L.; Kühnel, C.; Gühne, F.; Drescher, R.; Winkens, T.; Freesmeyer, M. Optimization of Thyroid Volume Determination by Stitched 3D-Ultrasound Data Sets in Patients with Structural Thyroid Disease. Biomedicines 2023, 11, 381. https://doi.org/10.3390/biomedicines11020381
Seifert P, Ullrich S-L, Kühnel C, Gühne F, Drescher R, Winkens T, Freesmeyer M. Optimization of Thyroid Volume Determination by Stitched 3D-Ultrasound Data Sets in Patients with Structural Thyroid Disease. Biomedicines. 2023; 11(2):381. https://doi.org/10.3390/biomedicines11020381
Chicago/Turabian StyleSeifert, Philipp, Sophie-Luise Ullrich, Christian Kühnel, Falk Gühne, Robert Drescher, Thomas Winkens, and Martin Freesmeyer. 2023. "Optimization of Thyroid Volume Determination by Stitched 3D-Ultrasound Data Sets in Patients with Structural Thyroid Disease" Biomedicines 11, no. 2: 381. https://doi.org/10.3390/biomedicines11020381
APA StyleSeifert, P., Ullrich, S. -L., Kühnel, C., Gühne, F., Drescher, R., Winkens, T., & Freesmeyer, M. (2023). Optimization of Thyroid Volume Determination by Stitched 3D-Ultrasound Data Sets in Patients with Structural Thyroid Disease. Biomedicines, 11(2), 381. https://doi.org/10.3390/biomedicines11020381