
The Effect of a Digital Manufacturing Technique, Preparation Taper, and Finish Line Design on the Marginal Fit of Temporary Molar Crowns: An In-Vitro Study
 , ,
, ,  ,
,  ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
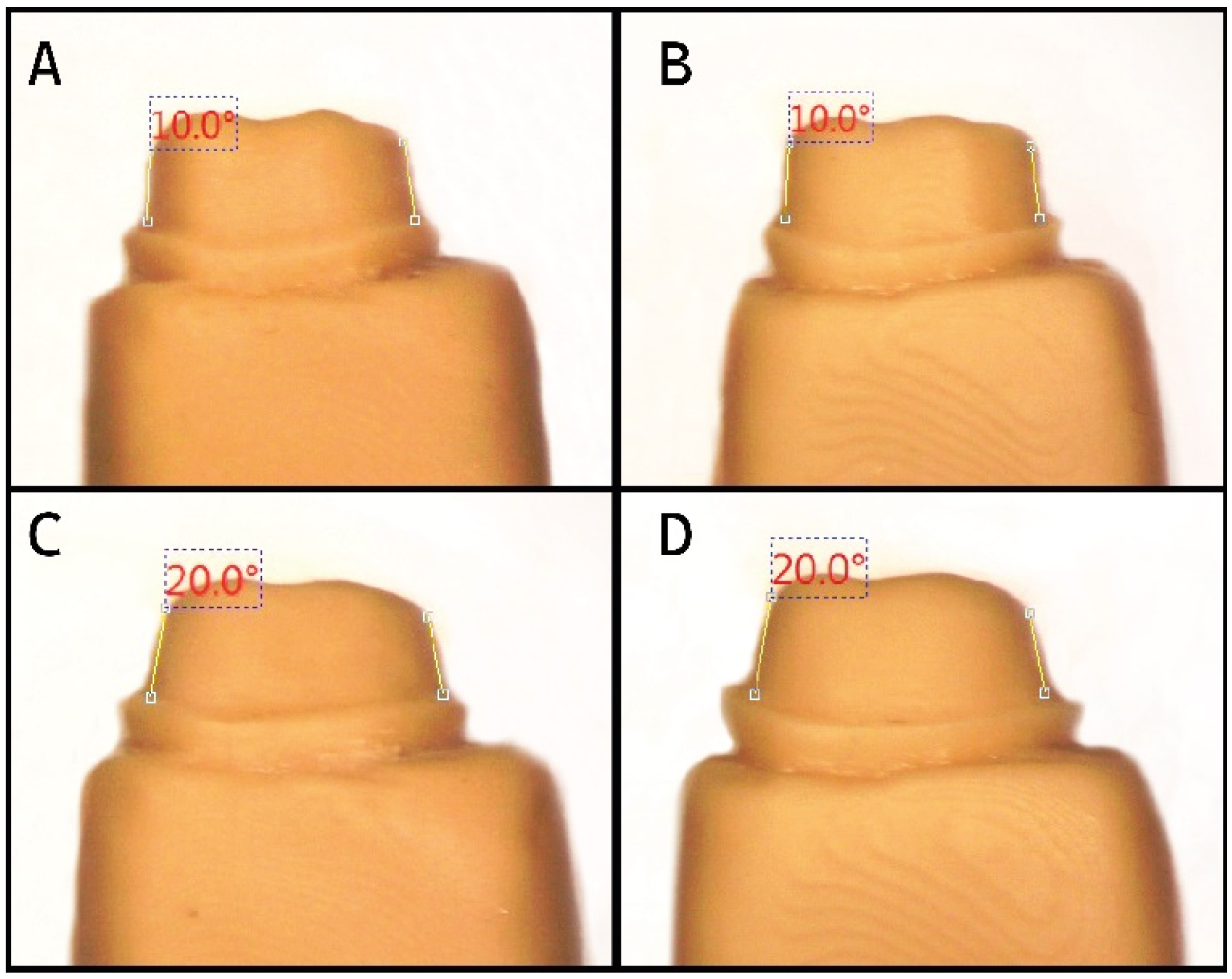
2.2. Preparation of the Master Models
2.3. Preparation of Working Models
2.4. Preparation of the Coping Specimens
2.5. Cementation of the Copings
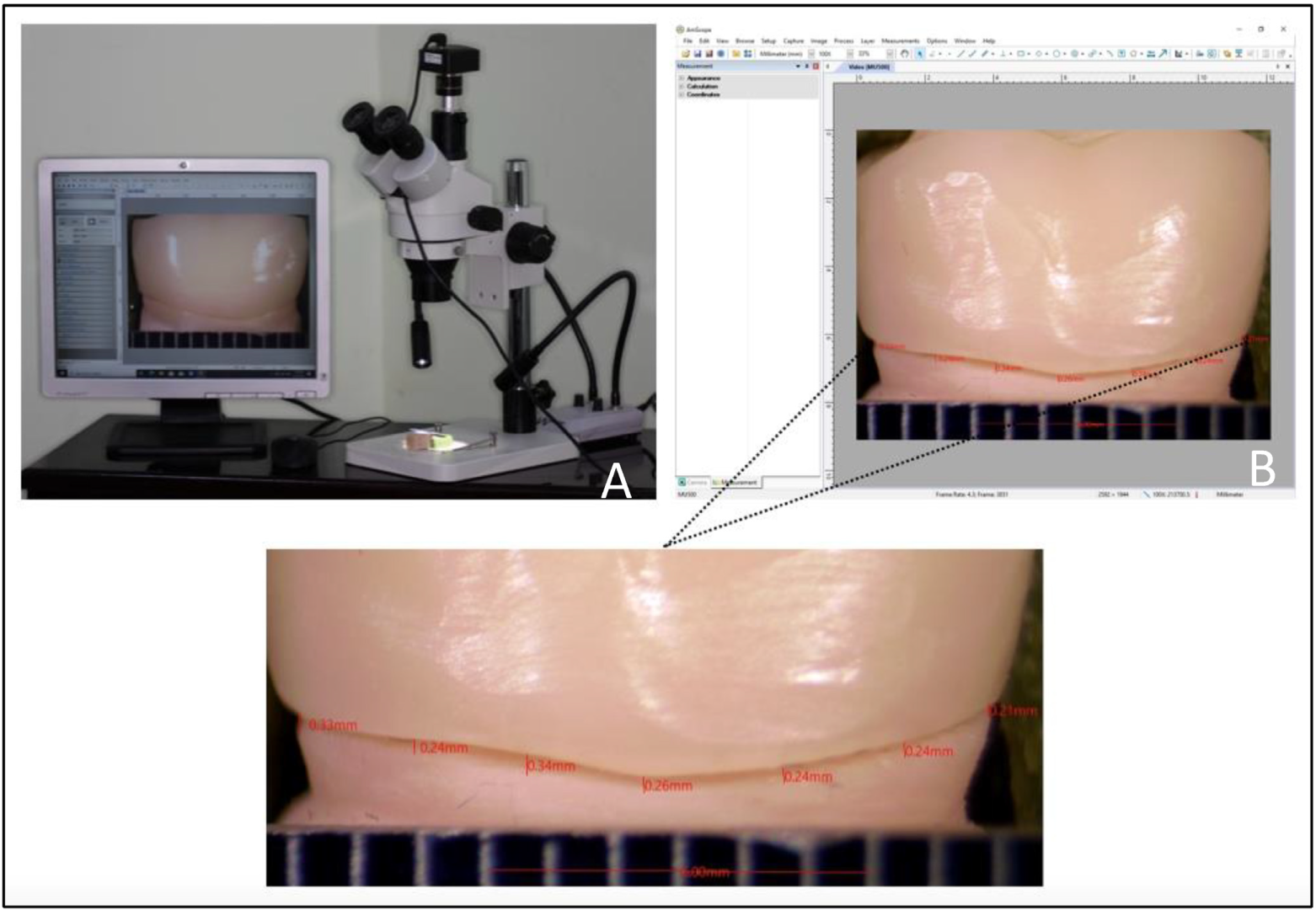
2.6. Measurement of Marginal Fit
2.7. Statistical Analysis
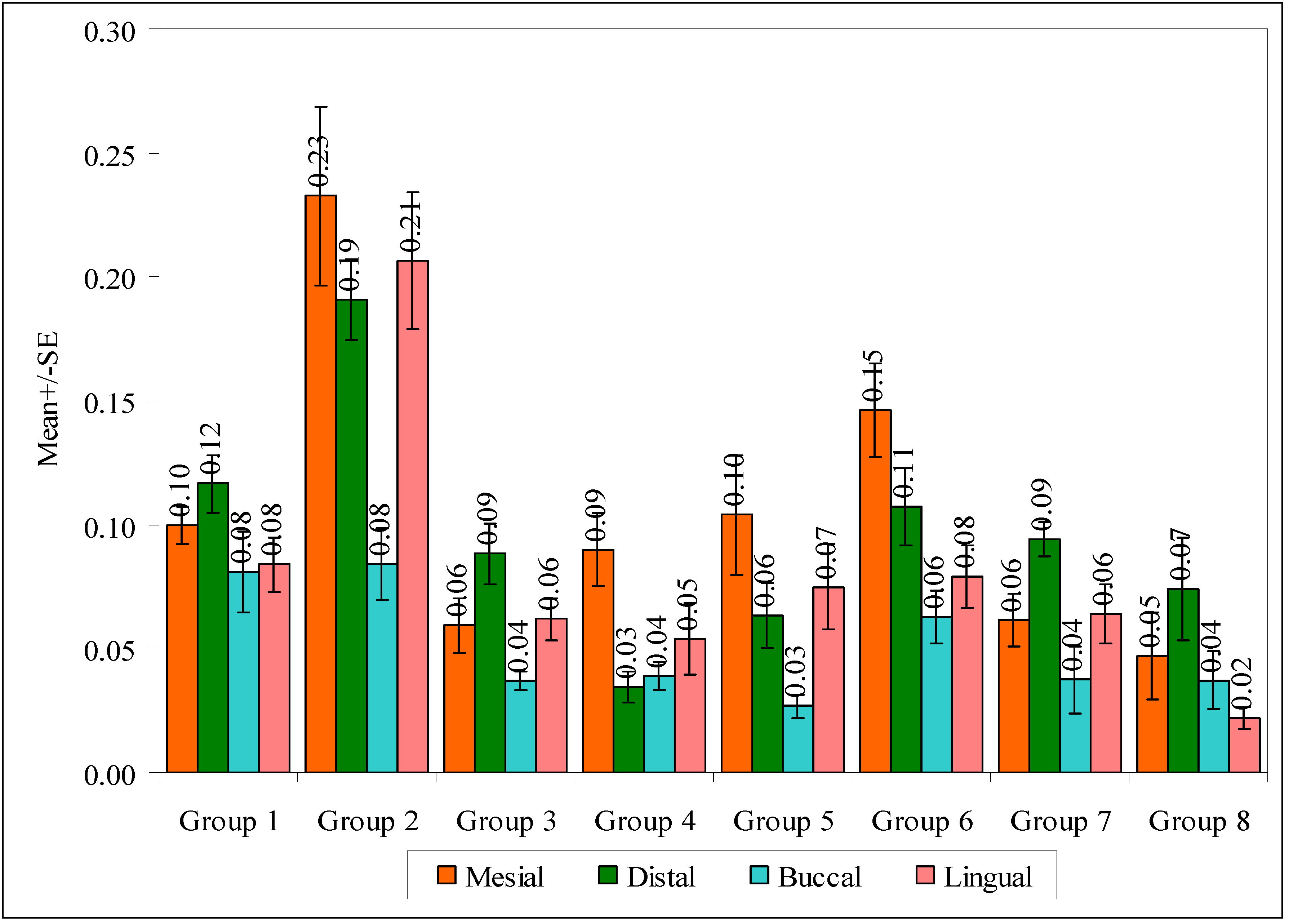
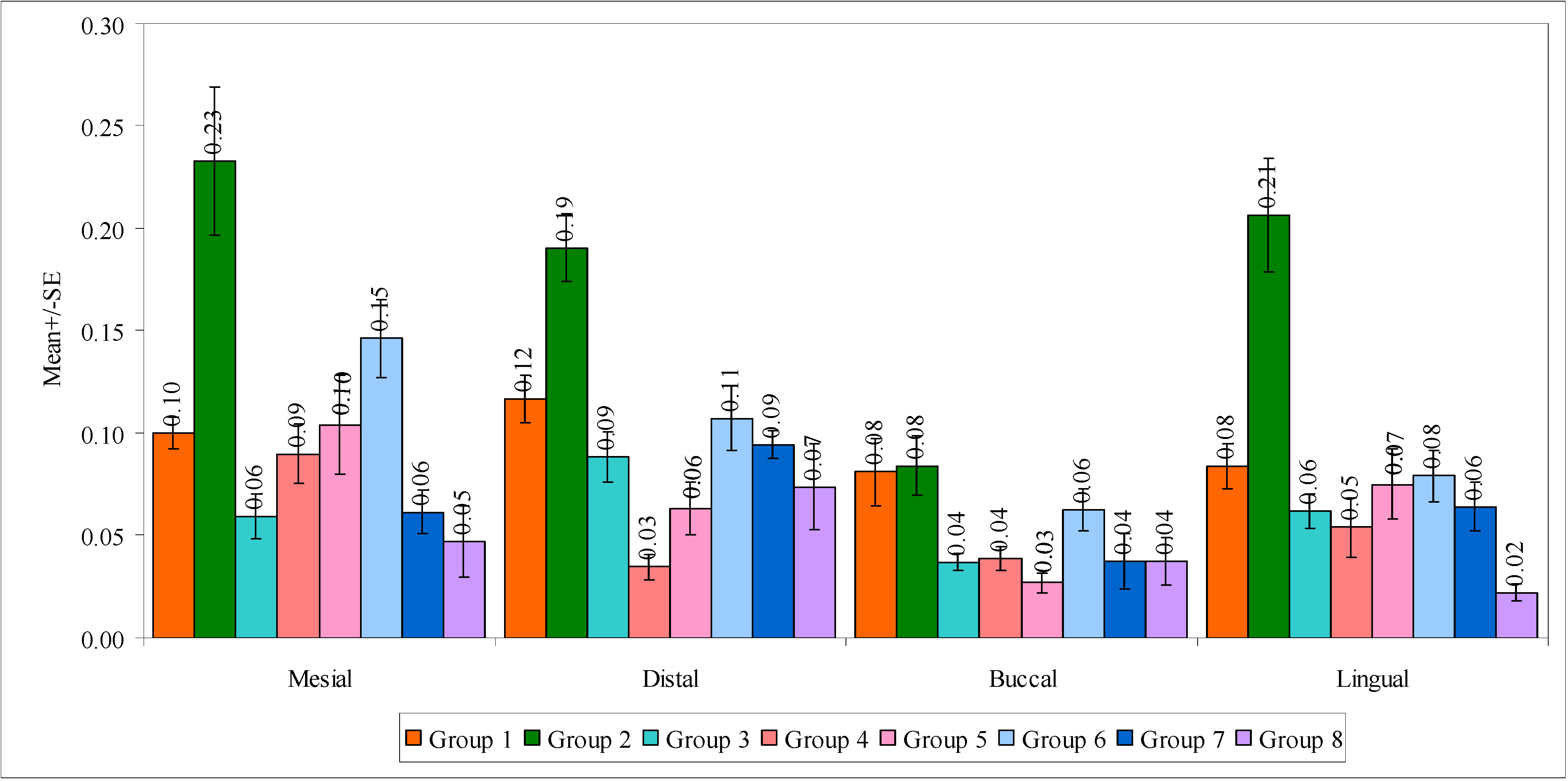
3. Results
4. Discussion
5. Limitations
6. Conclusions
- The best marginal fit was seen in group 8, while the poorest fit was noted in group 2.
- Shoulder finish lines and 10° TOC resulted in higher marginal gaps, especially in CAD/CAM milled group. The selection of 3D-printed crowns may provide a better marginal fit within the range of clinical acceptability.
- With the exception of one group (G2), the marginal gaps were within clinical acceptability (50 and 120 µm). Furthermore, 3D-printed crowns showed marginal gaps near the lower end of the clinical acceptability range, while marginal gaps of CAD/CAM milled crowns were near the upper end of that range.
- CAD/CAM milled crowns and 3D printed crowns may be comparable to each other in preparations of 20° TOC, chamfer, and shoulder finish lines.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Keith, J.F.; Steven, M.M. (Eds.) Glossary of Prosthodontic Terms, Ninth Edition. J. Prosthet. Dent. 2017, 117, e49. [Google Scholar]
- Christensen, G.J. When is a full-crown restoration indicated? Am. Dent. Assoc. 2007, 138, 101–103. [Google Scholar] [CrossRef]
- Pine, C.M.; Pitts, N.B.; Steele, J.G.; Nunn, J.N.; Treasure, E. Adult dental health survey: Dental restorations in adults in the UK in 1998 and implications for the future. Br. Dent. J. 2001, 190, 4–8. [Google Scholar] [CrossRef] [PubMed]
- Christensen, G.J. Tooth-colored inlays and onlays. J. Am. Dent. Assoc. 1988, 117, 12E–17E. [Google Scholar] [CrossRef] [PubMed]
- Ehrenberg, D.; Weiner, G.I.; Weiner, S. Long-term effects of storageand thermal cycling on the marginal adaptation of provisionalresin crowns: A pilot study. J. Prosthet. Dent. 2006, 95, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Wassell, R.W.; George, G.S.; Ingledew, R.P.; Steele, J.G. Crowns and other extra-coronal restorations: Provisional restorations. Br. Dent. J. 2002, 192, 619–630. [Google Scholar] [CrossRef] [PubMed]
- Burke, F.J.T.; Murray, M.C.; Shortall, A.C.C. Trends in indirect dentistry. Provisional restorations, more than just a temporary. Dent. Update 2005, 32, 443–452. [Google Scholar] [CrossRef]
- Mou, S.-H.; Chai, T.; Wang, J.-S.; Shiau, Y.-Y. Influence of different convergence angles and tooth preparation heights on the internal adaptation of Cerec crowns. J. Prosthet. Dent. 2002, 87, 248–255. [Google Scholar] [CrossRef]
- Alammari, M.R.; Abdelnabi, M.H.; Swelem, A.A. Effect of total occlusal convergence on fit and fracture resistance of zirconia-reinforced lithium silicate crowns. Clin. Cosmet. Investig. Dent. 2018, 11, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Emtair, E.; Bakry, S.; Azer, A. The Effect of Tooth Preparation Taper on the Marginal FIT and Fracture Resistance of CAD/CAM Zirconia Copings. Alex. Dent. J. 2015, 40, 214–220. [Google Scholar] [CrossRef] [Green Version]
- Re, D.; Cerutti, F.; Augusti, G.; Cerutti, A.; Augusti, D. Comparison of marginal fit of Lava CAD/CAM crown-copings with two finish lines. Int. J. Esthet. Dent. 2014, 9, 426. [Google Scholar]
- Euán, R.; Figueras-Álvarez, O.; Cabratosa-Termes, J.; Barberà, M.B.-D.; Gomes-Azevedo, S. Comparison of the Marginal Adaptation of Zirconium Dioxide Crowns in Preparations with Two Different Finish Lines. J. Prosthodont. 2012, 21, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Baig, M.R.; Akbar, A.A.; Embaireeg, M. Effect of Finish Line Design on the Fit Accuracy of CAD/CAM Monolithic Polymer-Infiltrated Ceramic-Network Fixed Dental Prostheses: An In Vitro Study. Polymers 2021, 13, 4311. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, W.M.; Shariati, B.; Gazzaz, A.Z.; Sayed, M.E.; Carvalho, R.M. Fit of tooth-supported zirconia single crowns—A systematic review of the literature. Clin. Exp. Dent. Res. 2020, 6, 700–716. [Google Scholar] [CrossRef] [PubMed]
- Sinhori, B.S.; De Andrada, M.A.C.; Lopes, G.C.; Junior, S.M.; Baratieri, L.N. Influence of Teeth Preparation Finishing on the Adaptation of Lithium Disilicate Crowns. Int. J. Biomater. 2017, 2017, 2078526. [Google Scholar] [CrossRef]
- Paul, N.; Swamy, K.R.; Dhakshaini; Sowmya, S.; Meravini, M. Marginal and internal fit evaluation of conventional metal-ceramic versus zirconia CAD/CAM crowns. J. Clin. Exp. Dent. 2020, 12, e31–e37. [Google Scholar] [CrossRef]
- Al Hamad, K.Q.; Al Quran, F.A.; AlJalam, S.A.; Baba, N.Z. Comparison of the Accuracy of Fit of Metal, Zirconia, and Lithium Disilicate Crowns Made from Different Manufacturing Techniques. J. Prosthodont. 2018, 28, 497–503. [Google Scholar] [CrossRef]
- Meirowitz, A.; Bitterman, Y.; Levy, S.; Mijiritsky, E.; Dolev, E. An in vitro evaluation of marginal fit zirconia crowns fabricated by a CAD-CAM dental laboratory and a milling center. BMC Oral Health 2019, 19, 103. [Google Scholar] [CrossRef] [Green Version]
- Borges, G.; Faria, J.; Agarwal, P.; Spohr, A.; Correr-Sobrinho, L.; Miranzi, B. In Vitro Marginal Fit of Three All-Ceramic Crown Systems Before and After Cementation. Oper. Dent. 2012, 37, 641–649. [Google Scholar] [CrossRef]
- Ishikiriama, A.; Oliveira, J.D.F.; Vieira, D.F.; Mondelli, J. Influence of some factors on the fit of cemented crowns. J. Prosthet. Dent. 1981, 45, 400–404. [Google Scholar] [CrossRef]
- Zhang, Y.; Dudley, J. The influence of different cement spaces on the marginalgap of CAD/CAM all-ceramic crowns. Aust. Dent. J. 2019, 64, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Wise, M. Stability of gingival crest after surgery and before anterior crown placement. J. Prosthet. Dent. 1985, 53, 20–23. [Google Scholar] [CrossRef] [PubMed]
- Chiantella, G.C. Horizontal Guided Bone Regeneration in the Esthetic Area with rhPDGF-BB and Anorganic Bovine Bone Graft: A Case Report. Int. J. Periodontics Restor. Dent. 2016, 36, e9–e15. [Google Scholar] [CrossRef] [Green Version]
- Rayyan, M.M.; Aboushelib, M.; Sayed, N.M.; Ibrahim, A.; Jimbo, R. Comparison of interim restorations fabricated by CAD/CAM with those fabricated manually. J. Prosthet. Dent. 2015, 114, 414–419. [Google Scholar] [CrossRef] [PubMed]
- Al Wadei, M.H.D.; Sayed, M.E.; Jain, S.; Aggarwal, A.; Alqarni, H.; Gupta, S.G.; Alqahtani, S.M.; Alahmari, N.M.; Alshehri, A.H.; Jain, M.; et al. Marginal Adaptation and Internal Fit of 3D-Printed Provisional Crowns and Fixed Dental Prosthesis Resins Compared to CAD/CAM-Milled and Conventional Provisional Resins: A Systematic Review and Meta-Analysis. Coatings 2022, 12, 1777. [Google Scholar] [CrossRef]
- Dewan, H.; Sayed, M.E.; Alqahtani, N.M.; Alnajai, T.; Qasir, A.; Chohan, H. The Effect of Commercially Available Desensitizers on Bond Strength Following Cementation of Zirconia Crowns Using Self-Adhesive Resin Cement—An In Vitro Study. Materials 2022, 15, 514. [Google Scholar] [CrossRef]
- Sayed, M.; Dewan, H.; Mubaraki, M.; Khubrani, Z.; Hummadi, S.; Jurado, C.A. Evaluation of abutment parallelism and path of withdrawal using three intra- and one extra-oral methods: A survey and Invitro study. Eur. J. Gen. Dent. 2020, 9, 122–128. [Google Scholar] [CrossRef]
- Methani, M.M.; Revilla-León, M.; Zandinejad, A. The potential of additive manufacturing technologies and their processing parameters for the fabrication of all-ceramic crowns: A review. J. Esthet. Restor. Dent. 2019, 32, 182–192. [Google Scholar] [CrossRef]
- Alharbi, N.; Wismeijer, D.; Osman, R.B. Additive Manufacturing Techniques in Prosthodontics: Where Do We Currently Stand? A Critical Review. Int. J. Prosthodont. 2017, 30, 474–484. [Google Scholar] [CrossRef]
- Barazanchi, A.; Li, K.C.; Al-Amleh, B.; Lyons, K.; Waddell, J.N. Additive Technology: Update on Current Materials and Applications in Dentistry. J. Prosthodont. 2017, 26, 156–163. [Google Scholar] [CrossRef]
- Güth, J.F.; e Silva, J.A.; Edelhoff, D. Enhancing the predictability of complex rehabilitation with a removable CAD/CAM-fabricated long-term provisional prosthesis: A clinical report. J. Prosthet. Dent. 2012, 107, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Elagra, M.I.; Rayyan, M.R.; Alhomaidhi, M.M.; Alanaziy, A.A.; Alnefaie, M.O. Color stability and marginal integrity of interim crowns: An in vitro study. Eur. J. Dent. 2017, 11, 330–334. [Google Scholar] [CrossRef] [PubMed]
- Patras, M.; Naka, O.; Doukoudaki, S.; Pissiotis, A. Management of provisional restorations’ defciencies: A literature review. J. Esthet. Restor. Dent. 2012, 24, 26–38. [Google Scholar] [CrossRef] [PubMed]
- Srilekha, M.; Abirami, G. Awareness of diferent types of fnish lines of tooth preparation among working dental students—A questionnaire-based study. J. Pharm. Sci. Res. 2016, 8, 1210. [Google Scholar]
- Givens, E.J., Jr.; Neiva, G.; Yaman, P.; Dennison, J.B. Marginal adaptation and color stability of four provisional materials. J. Prosthodont. 2008, 17, 97–101. [Google Scholar] [CrossRef] [Green Version]
- Balkenhol, M.; Knapp, M.; Ferger, P.; Heun, U.; Wöstmann, B. Correlation between polymerization shrinkage and marginal ft of temporary crowns. Dent. Mater. 2008, 24, 1575–1584. [Google Scholar] [CrossRef]
- Karaokutan, I.; Sayin, G.; Kara, O. In vitro study of fracture strength of provisional crown materials. J. Adv. Prosthodont. 2015, 7, 27–31. [Google Scholar] [CrossRef] [Green Version]
- Keyf, F.; Anil, N. The effect of margin design on the marginal adaptation of temporary crowns. J. Oral Rehabil. 1994, 21, 367–371. [Google Scholar] [CrossRef]
- Tiu, J.; Al-Amleh, B.; Waddell, J.N.; Duncan, W.J. Clinical tooth preparations and associated measuring methods: A systematic review. J. Prosthet. Dent. 2015, 113, 175–184. [Google Scholar] [CrossRef]
- Naidoo, N.; Moipolai, P.D.; Motloba, P. A Comparison of Convergence Angles of Crown preparations in an undergraduate programme at a Tertiary Institution. S. Afr. Dent. J. 2022, 76, 602–606. [Google Scholar] [CrossRef]
- Larson, T.D. The clinical significance of marginal fit. Northwest Dent. 2012, 91, 22–30. [Google Scholar] [PubMed]
- Holmes, J.R.; Bayne, S.C.; Holland, G.A.; Sulik, W.D. Considerations in measurement of marginal fit. J. Prosthet. Dent. 1989, 62, 405–408. [Google Scholar] [CrossRef] [PubMed]
- Hasanzade, M.; Aminikhah, M.; Afrashtehfar, K.I.; Alikhasi, M. Marginal and internal adaptation of single crowns and fixed dental prostheses by using digital and conventional workflows: A systematic review and meta-analysis. J. Prosthet. Dent. 2020, 126, 360–368. [Google Scholar] [CrossRef]
- Jacobs, M.S.; Windeler, A.S. An investigation of dental luting cement solubility as a function of the marginal gap. J. Prosthet. Dent. 1991, 65, 436–442. [Google Scholar] [CrossRef] [PubMed]
- Felton, D.A.; Kanoy, B.E.; Bayne, S.C.; Wirthman, G.P. Effect of in vivo crown margin discrepancies on periodontal health. J. Prosthet. Dent. 1991, 65, 357–364. [Google Scholar] [CrossRef]
- Contrepois, M.; Soenen, A.; Bartala, M.; Laviole, O. Marginal adaptation of ceramic crowns: A systematic review. J. Prosthet. Dent. 2013, 110, 447–454. [Google Scholar] [CrossRef]
- Son, K.; Lee, S.; Kang, S.H.; Park, J.; Lee, K.-B.; Jeon, M.; Yun, B.-J. A Comparison Study of Marginal and Internal Fit Assessment Methods for Fixed Dental Prostheses. J. Clin. Med. 2019, 8, 785. [Google Scholar] [CrossRef] [Green Version]
- Laumbacher, H.; Strasser, T.; Knüttel, H.; Rosentritt, M. Long-term clinical performance and complications of zirconia-based tooth- and implant-supported fixed prosthodontic restorations: A summary of systematic reviews. J. Dent. 2021, 111, 103723. [Google Scholar] [CrossRef]
- Freire, Y.; Gonzalo, E.; Lopez-Suarez, C.; Pelaez, J.; Suarez, M.J. Evaluation of the marginal fit of monolithic crowns fabricated by direct and indirect digitization. J. Prosthodont. Res. 2020, 65, 291–297. [Google Scholar] [CrossRef]
- Del Piñal, M.; Lopez-Suarez, C.; Bartolome, J.F.; Volpato, C.A.; Suarez, M.J. Effect of cementation and aging on the marginal fit of veneered and monolithic zirconia and metal-ceramic CAD-CAM crowns. J. Prosthet. Dent. 2021, 125, 323.e1–323.e7. [Google Scholar] [CrossRef]
- Baltazar, I.C.; Vaz, J. Pimentel Coelho Lino Carracho, Marginal fit of zirconia copings fabricated after conventional impression making and digital scanning: An in vitro study. J. Prosthet. Dent. 2020, 124, 223.e1–223.e6. [Google Scholar] [CrossRef]
- Ahmed, W.M.; Abdallah, M.-N.; McCullagh, A.P.; Wyatt, C.C.; Troczynski, T.; Carvalho, R.M. Marginal Discrepancies of Monolithic Zirconia Crowns: The Influence of Preparation Designs and Sintering Techniques. J. Prosthodont. 2019, 28, 288–298. [Google Scholar] [CrossRef]
- Li, R.; Wang, Y.; Hu, M.; Wang, Y.; Xv, Y.; Liu, Y.; Sun, Y. Strength and Adaptation of Stereolithography-Fabricated Zirconia Dental Crowns: An In Vitro Study. Int. J. Prosthodont. 2019, 32, 439–443. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Yu, H.; Liu, Y.; Jiang, X.; Gao, B. Trueness analysis of zirconia crowns fabricated with 3-dimensional printing. J. Prosthet. Dent. 2019, 121, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Revilla-León, M.; Methani, M.M.; Morton, D.; Zandinejad, A. Internal and marginal discrepancies associated with stereolithography (SLA) additively manufactured zirconia crowns. J. Prosthet. Dent. 2020, 124, 730–737. [Google Scholar] [CrossRef] [PubMed]
- Sulaiman, F.; Chai, J.; Jameson, L.M.; Wozniak, W.T. A comparison of the marginal fit of In-Ceram, IPS Empress, and Procera crowns. Int. J. Prosthodont. 1997, 10, 478–484. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Materials/Machines | Manufacturer | Lot No. | Model No. | Composition |
|---|---|---|---|---|
| ATRIUM 200 mm Digital Electronic Angle Finder Goniometer Measuring Ruler Atrium digital protractor | Atrium Enterprise, Cardiff, UK | CR 2032 | ||
| Five-axis milling machine | DG SHAPE, Roland DGA, Irvine, CA, USA | DWX-52D | ||
| 3D-printing material | Asiga Pty Ltd., Alexandria, Australia | MO/16020 | 7,7,9(or 7,9,9)- trimethyl-4,13-dioxo-3,14-dioxa-5,12- diazahexadecane-1,16- diyl bismethacrylate, Tetrahydrofurfuryl methacrylate, Diphenyl(2,4,6- trimethylbenzoyl) phosphine oxide | |
| 3D-printing machine | Asiga 3D printer, Alexandria, Australia, Serial Number: 70B3D5362C6A | PN01233 | ||
| Copra temp | CopraTemp Shade A1, WhitePeaks Dental Solutions GmbH, Wesel, Germany | P10690 | PMMA (polymethylmethacrylate)/pigments | |
| Temp Bond Clear | Kerr, Romulus, MI, USA | 8375246 | Dibutyl phthalate, Hydroxyethylmethacrylate, Fumed silica, N-(2-Pyridyl)thiourea, Ethyldimethylaminobenzoate, Triclosan |
| Model Number | Axial Height | Occlusal Convergence | Finish Line |
|---|---|---|---|
| A | 4 mm | 10° | Chamfer |
| B | 4 mm | 10° | Shoulder |
| C | 4 mm | 20° | Chamfer |
| D | 4 mm | 20° | Shoulder |
| Groups | Description |
|---|---|
| GROUP 1 | 3D-Milled crowns (10 samples) based on the generated file by the software from Model A. |
| GROUP 2 | 3D-Milled crowns (10 samples) based on the generated file by the software from Model B. |
| GROUP 3 | 3D-Milled crowns (10 samples) based on the generated file by the software from Model C. |
| GROUP 4 | 3D-Milled crowns (10 samples) based on the generated file by the software from Model D. |
| GROUP 5 | 3D-Printed crowns (10 samples) based on the generated file by the software from Model A. |
| GROUP 6 | 3D-Printed crowns (10 samples) based on the generated file by the software from Model B. |
| GROUP 7 | 3D-Printed crowns (10 samples) based on the generated file by the software from Model C. |
| GROUP 8 | 3D-Printed crowns (10 samples) based on the generated file by the software from Model D. |
| Groups | Mesial | Distal | Buccal | Lingual | Total | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| Group 1 | 0.0998 | 0.0243 | 0.1166 | 0.0365 | 0.0810 | 0.0518 | 0.0839 | 0.0352 | 0.0953 | 0.0273 |
| Group 2 | 0.2328 | 0.1140 | 0.1906 | 0.0514 | 0.0841 | 0.0466 | 0.2063 | 0.0874 | 0.1785 | 0.0474 |
| Group 3 | 0.0594 | 0.0341 | 0.0884 | 0.0385 | 0.0370 | 0.0126 | 0.0619 | 0.0267 | 0.0617 | 0.0154 |
| Group 4 | 0.0900 | 0.0460 | 0.0346 | 0.0193 | 0.0389 | 0.0186 | 0.0540 | 0.0460 | 0.0544 | 0.0257 |
| Group 5 | 0.1040 | 0.0762 | 0.0632 | 0.0416 | 0.0269 | 0.0149 | 0.0749 | 0.0541 | 0.0672 | 0.0378 |
| Group 6 | 0.1462 | 0.0604 | 0.1074 | 0.0495 | 0.0626 | 0.0336 | 0.0791 | 0.0392 | 0.0988 | 0.0265 |
| Group 7 | 0.0616 | 0.0332 | 0.0944 | 0.0220 | 0.0374 | 0.0421 | 0.0640 | 0.0379 | 0.0644 | 0.0195 |
| Group 8 | 0.0470 | 0.0554 | 0.0738 | 0.0656 | 0.0373 | 0.0372 | 0.0220 | 0.0132 | 0.0450 | 0.0326 |
| F-value | 9.5989 | 11.5135 | 3.9719 | 13.2422 | 19.6429 | |||||
| p-value | 0.0001 * | 0.0001 * | 0.0010 * | 0.0001 * | 0.0001 * | |||||
| Group | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|
| MD/p-Value | MD/p-Value | MD/p-Value | MD/p-Value | MD/p-Value | MD/p-Value | MD/p-Value | MD/p-Value | |
| 1 | X | −0.08/0.0001 * | 0.03/0.2281 | 0.04/0.0689 | 0.03/0.4528 | −0.00/1.0000 | 0.03/0.3264 | 0.05/0.0101 * |
| 2 | 0.08/0.0001 * | X | 0.12/0.0001 * | 0.12/0.0001 * | 0.11/0.0001 * | 0.08/0.0001 * | 0.11/0.0001 * | 0.13/0.0001 * |
| 3 | −0.03/0.2281 | −0.12/0.0001 * | X | 0.01/0.9995 | −0.01/0.9999 | −0.04/0.1332 | −0.00/1.0000 | 0.012/0.9239 |
| 4 | −0.04/0.0689 | −0.12/0.0001 * | −0.01/0.9995 | X | −0.01/0.9808 | −0.04/0.0350 * | −0.01/0.9958 | 0.01/0.9972 |
| 5 | −0.03/0.4528 | −0.11/0.0001 * | 0.01/0.9999 | 0.01/0.9808 | X | −0.03/0.3009 | 0.01/1.0000 | 0.02/0.7334 |
| 6 | 0.00/1.0000 | −0.08/0.0001 * | 0.04/0.1332 | 0.04/0.0350 * | 0.03/0.3009 | X | 0.01/0.2026 | 0.06/0.0045 * |
| 7 | −0.03/0.3264 | −0.11/0.0001 * | 0.00/1.0000 | 0.01/0.9958 | −0.01/1.0000 | −0.01/0.2026 | X | 0.02/0.8472 |
| 8 | −0.05/0.0101 * | −0.13/0.0001 * | −0.012/0.9239 | −0.01/0.9972 | −0.02/0.7334 | −0.06/0.0045 * | −0.02/0.8472 | X |
| Region | Group 1 | Group 2 | Group 3 | Group 4 | Group 5 | Group 6 | Group 7 | Group 8 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| Mesial | 0.10 | 0.02 | 0.23 | 0.11 | 0.06 | 0.03 | 0.09 | 0.05 | 0.10 | 0.08 | 0.15 | 0.06 | 0.06 | 0.03 | 0.05 | 0.06 |
| Distal | 0.12 | 0.04 | 0.19 | 0.05 | 0.09 | 0.04 | 0.03 | 0.02 | 0.06 | 0.04 | 0.11 | 0.05 | 0.09 | 0.02 | 0.07 | 0.07 |
| Buccal | 0.08 | 0.05 | 0.08 | 0.05 | 0.04 | 0.01 | 0.04 | 0.02 | 0.03 | 0.01 | 0.06 | 0.03 | 0.04 | 0.04 | 0.04 | 0.04 |
| Lingual | 0.08 | 0.04 | 0.21 | 0.09 | 0.06 | 0.03 | 0.05 | 0.05 | 0.07 | 0.05 | 0.08 | 0.04 | 0.06 | 0.04 | 0.02 | 0.01 |
| F-value | 1.8457 | 6.6890 | 5.0394 | 5.1191 | 3.8137 | 6.1135 | 4.5462 | 2.1245 | ||||||||
| p-value | 0.1564 | 0.0011 * | 0.0051 * | 0.0047 * | 0.0180 * | 0.0018 * | 0.0084 * | 0.1142 | ||||||||
| Pair wise comparisons by Tukey’s multiple posthoc procedures | ||||||||||||||||
| Mesial vs. Distal | p = 0.7603 | p = 0.6414 | p = 0.1461 | p = 0.0063 * | p = 0.3065 | p = 0.2661 | p = 0.1669 | p = 0.5884 | ||||||||
| Mesial vs. Buccal | p = 0.6922 | p = 0.0011 * | p = 0.3439 | p = 0.0129 * | p = 0.0103 * | p = 0.0018 * | p = 0.4133 | p = 0.9673 | ||||||||
| Mesial vs. Lingual | p = 0.7878 | p = 0.8790 | p = 0.9978 | p = 0.1199 | p = 0.5933 | p = 0.0145 * | p = 0.9987 | p = 0.6411 | ||||||||
| Distal vs. Buccal | p = 0.1784 | p = 0.0251 * | p = 0.0024 * | p = 0.9930 | p = 0.4069 | p = 0.1598 | p = 0.0042* | p = 0.3243 | ||||||||
| Distal vs. Lingual | p = 0.2400 | p = 0.9712 | p = 0.2061 | p = 0.6105 | p = 0.9576 | p = 0.5383 | p = 0.2209 | p = 0.0853 | ||||||||
| Buccal vs. Lingual | p = 0.9984 | p = 0.0082 | p = 0.2566 | p = 0.7715 | p = 0.1802 | p = 0.8579 | p = 0.3306 | p = 0.8871 | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mugri, M.H.; Dewan, H.; Sayed, M.E.; Shaabi, F.I.; Hakami, H.I.; Jokhadar, H.F.; Alqahtani, N.M.; Alshahrani, A.A.; Alabdullah, A.S.; Alshehri, A.H.; et al. The Effect of a Digital Manufacturing Technique, Preparation Taper, and Finish Line Design on the Marginal Fit of Temporary Molar Crowns: An In-Vitro Study. Biomedicines 2023, 11, 570. https://doi.org/10.3390/biomedicines11020570
Mugri MH, Dewan H, Sayed ME, Shaabi FI, Hakami HI, Jokhadar HF, Alqahtani NM, Alshahrani AA, Alabdullah AS, Alshehri AH, et al. The Effect of a Digital Manufacturing Technique, Preparation Taper, and Finish Line Design on the Marginal Fit of Temporary Molar Crowns: An In-Vitro Study. Biomedicines. 2023; 11(2):570. https://doi.org/10.3390/biomedicines11020570
Chicago/Turabian StyleMugri, Maryam H., Harisha Dewan, Mohammed E. Sayed, Fawzia Ibraheem Shaabi, Hanan Ibrahim Hakami, Hossam F. Jokhadar, Nasser M. Alqahtani, Ahid Amer Alshahrani, Abdullah S. Alabdullah, Abdullah Hasan Alshehri, and et al. 2023. "The Effect of a Digital Manufacturing Technique, Preparation Taper, and Finish Line Design on the Marginal Fit of Temporary Molar Crowns: An In-Vitro Study" Biomedicines 11, no. 2: 570. https://doi.org/10.3390/biomedicines11020570
APA StyleMugri, M. H., Dewan, H., Sayed, M. E., Shaabi, F. I., Hakami, H. I., Jokhadar, H. F., Alqahtani, N. M., Alshahrani, A. A., Alabdullah, A. S., Alshehri, A. H., Wadei, M. H. D. A., Arif, F. Y., Adawi, E. H., Al-Makramani, B. M. A., & Chohan, H. (2023). The Effect of a Digital Manufacturing Technique, Preparation Taper, and Finish Line Design on the Marginal Fit of Temporary Molar Crowns: An In-Vitro Study. Biomedicines, 11(2), 570. https://doi.org/10.3390/biomedicines11020570