

Specific Cellular and Humoral Immune Responses to the Neoantigen RBD of SARS-CoV-2 in Patients with Primary and Secondary Immunodeficiency and Healthy Donors
 , , , ,
, , , ,  ,
,  , , add
Show full author list
, , add
Show full author list
Abstract
:1. Introduction
2. Material and Methods
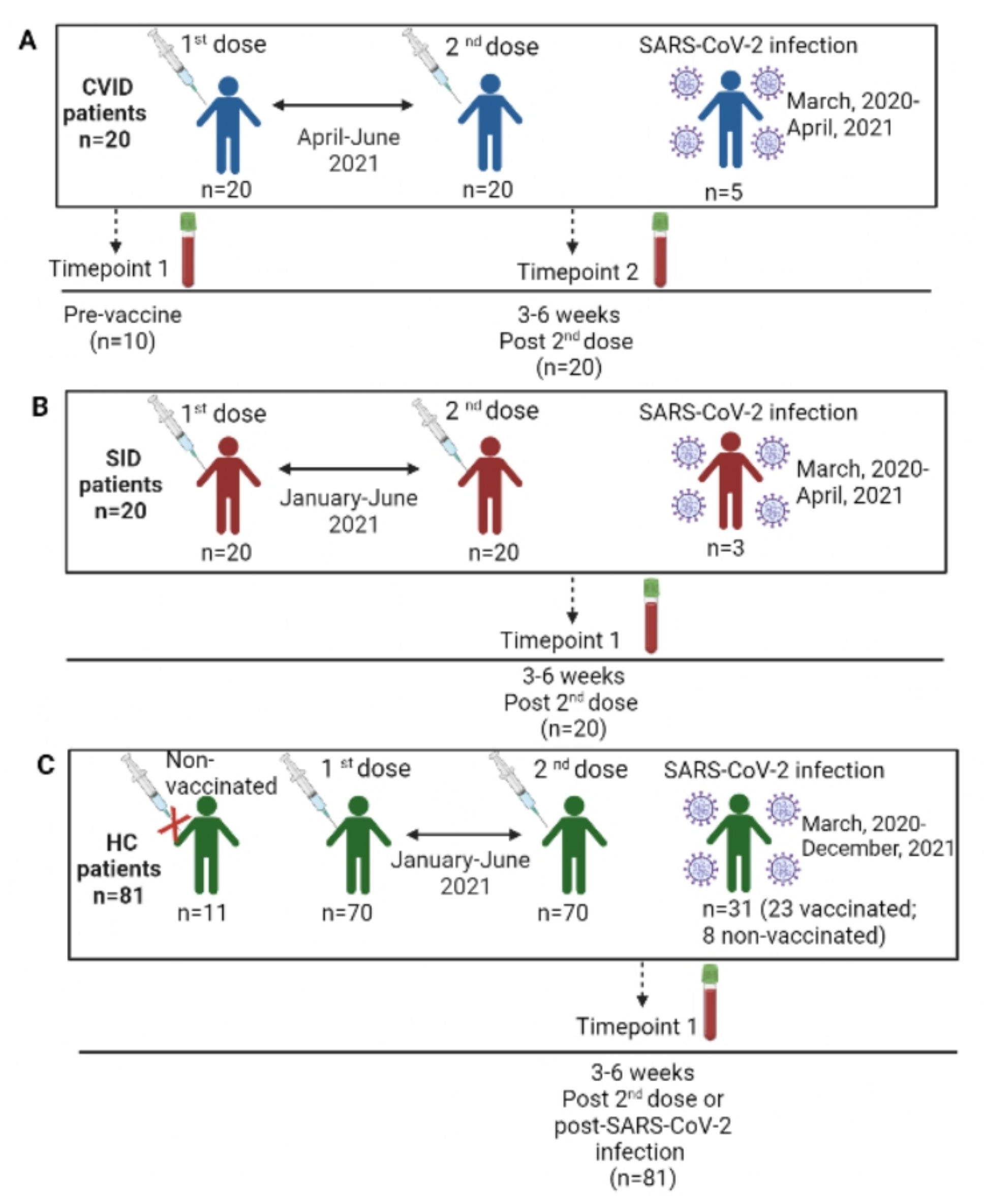
2.1. Study Design
2.2. Evaluation of SARS-CoV-2 Cellular Response
2.3. Evaluation of SARS-CoV-2 Humoral Response
2.4. Statistical Analysis
3. Results
3.1. Epidemiological and Immunological Characteristics of the Study Population
3.2. SARS-CoV-2 History
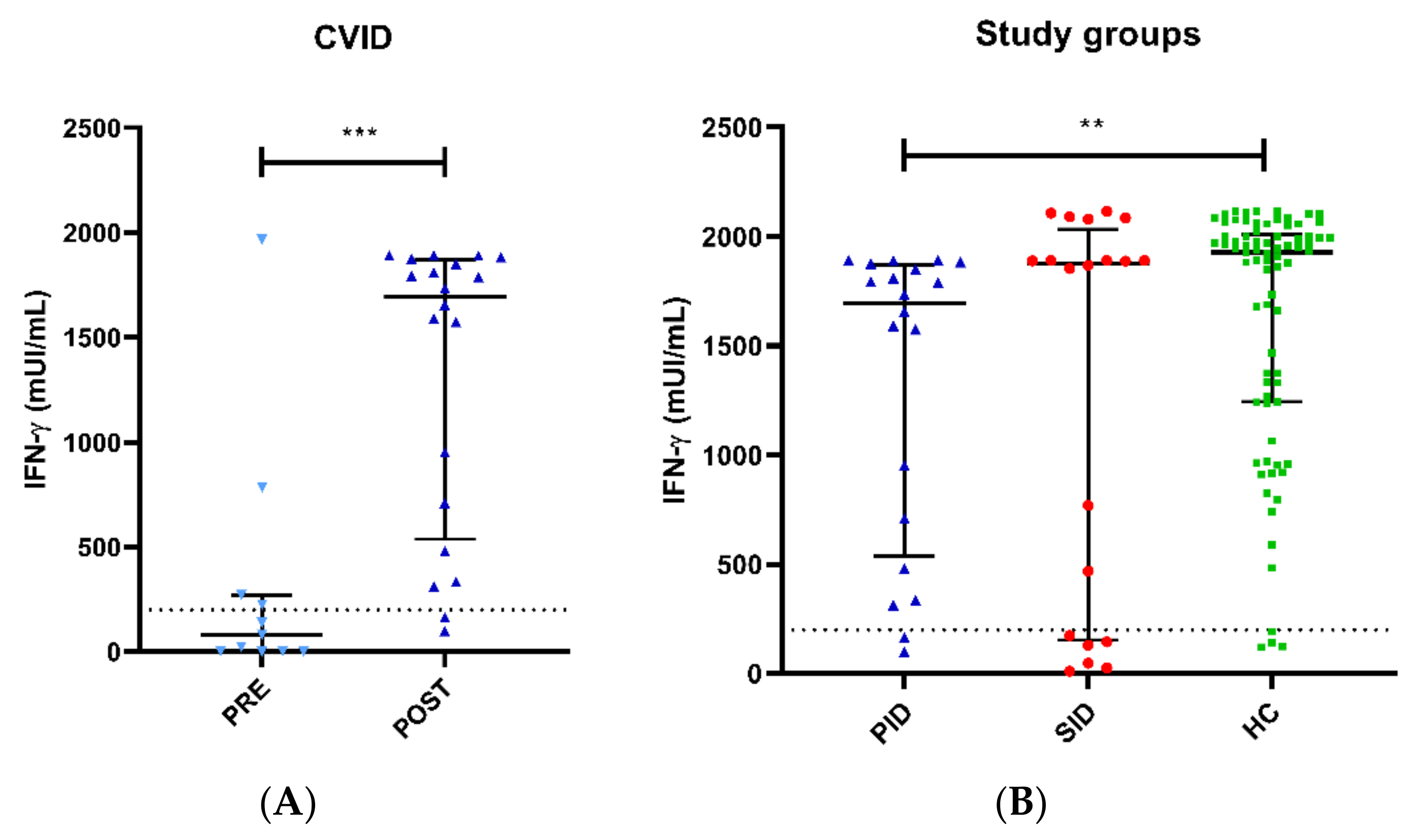
3.3. SARS-CoV-2 T-Cell Responses in PID and SID Patients
3.4. SARS-CoV-2-Specific T-Cell Responses in Healthy Donors
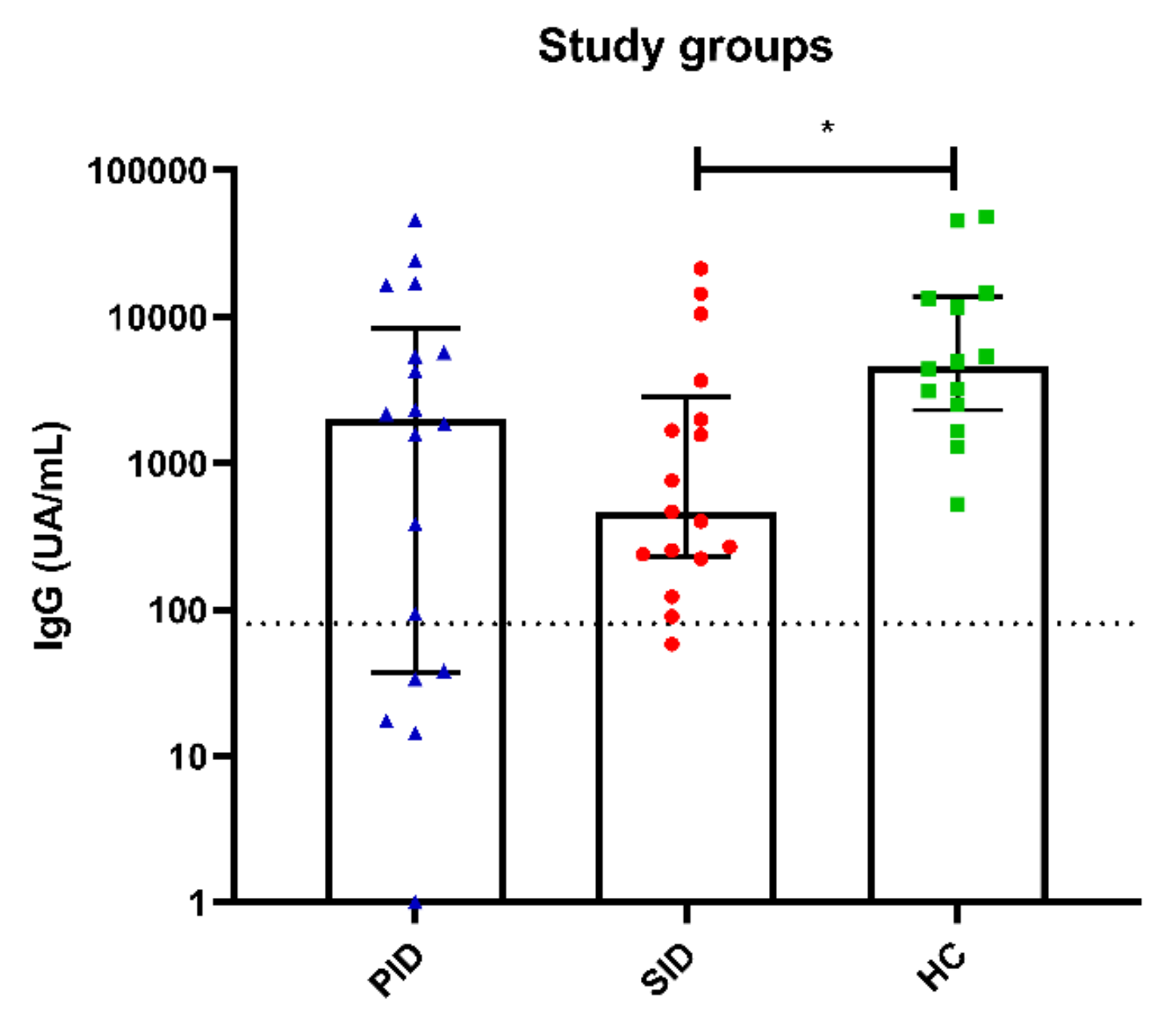
3.5. SARS-CoV-2 Antibody Responses
3.6. SARS-CoV-2 Infection Follow-Up and Correlate for Protection
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Babaha, F.; Rezaei, N. Primary Immunodeficiency Diseases in COVID-19 Pandemic: A Predisposing or Protective Factor? Am. J. Med. Sci. 2020, 360, 740–741. [Google Scholar] [CrossRef] [PubMed]
- Quinti, I.; Mezzaroma, I.; Milito, C. Clinical management of patients with primary immunodeficiencies during the COVID-19 pandemic. Expert Rev. Clin. Immunol. 2021, 17, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Abbott, J.K.; Gelfand, E.W. Common Variable Immunodeficiency: Diagnosis, Management, and Treatment. Immunol. Allergy Clin. N. Am. 2015, 35, 637–658. [Google Scholar] [CrossRef] [PubMed]
- Ameratunga, R.; Allan, C.; Woon, S.-T. Defining Common Variable Immunodeficiency Disorders in 2020. Immunol. Allergy Clin. N. Am. 2020, 40, 403–420. [Google Scholar] [CrossRef] [PubMed]
- Seidel, M.G.; Kindle, G.; Gathmann, B.; Quinti, I.; Buckland, M.; van Montfrans, J.; Scheible, R.; Rusch, S.; Gasteiger, L.M.; Grimbacher, B.; et al. The European Society for Immunodeficiencies (ESID) Registry Working Definitions for the Clinical Diagnosis of Inborn Errors of Immunity. J. Allergy Clin. Immunol. Pract. 2019, 7, 1763–1770. [Google Scholar] [CrossRef]
- Vijenthira, A.; Gong, I.Y.; Fox, T.A.; Booth, S.; Cook, G.; Fattizzo, B.; Martín-Moro, F.; Razanamahery, J.; Riches, J.C.; Zwicker, J.; et al. Outcomes of patients with hematologic malignancies and COVID-19: A systematic review and meta-analysis of 3377 patients. Blood 2020, 136, 2881–2892. [Google Scholar] [CrossRef]
- Friman, V.; Winqvist, O.; Blimark, C.; Langerbeins, P.; Chapel, H.; Dhalla, F. Secondary immunodeficiency in lymphoproliferative malignancies. Hematol. Oncol. 2016, 34, 121–132. [Google Scholar] [CrossRef]
- Liang, W.; Guan, W.; Chen, R.; Wang, W.; Li, J.; Xu, K.; Li, C.; Ai, Q.; Lu, W.; Liang, H.; et al. Cancer patients in SARS-CoV-2 infection: A nationwide analysis in China. Lancet Oncol. 2020, 21, 335–337. [Google Scholar] [CrossRef]
- Hanitsch, L.G.; Löbel, M.; Mieves, J.F.; Bauer, S.; Babel, N.; Schweiger, B.; Wittke, K.; Grabowski, P.; Volk, H.-D.; Scheibenbogen, C. Cellular and humoral influenza-specific immune response upon vaccination in patients with common variable immunodeficiency and unclassified antibody deficiency. Vaccine 2016, 34, 2417–2423. [Google Scholar] [CrossRef]
- Friedmann, D.; Goldacker, S.; Peter, H.-H.; Warnatz, K. Preserved Cellular Immunity Upon Influenza Vaccination in Most Patients with Common Variable Immunodeficiency. J. Allergy Clin. Immunol. Pract. 2020, 8, 2332–2340.e5. [Google Scholar] [CrossRef]
- Kak, G.; Raza, M.; Tiwari, B.K. Interferon-gamma (IFN-γ): Exploring its implications in infectious diseases. Biomol. Concepts 2018, 9, 64–79. [Google Scholar] [CrossRef] [PubMed]
- Zhu, M.; Zhu, Z.; Yang, J.; Hu, K. Performance Evaluation of IGRA-ELISA and T-SPOT.TB for Diagnosing Tuberculosis Infection. Clin. Lab. 2019, 65. [Google Scholar] [CrossRef] [PubMed]
- Mahmoodpoor, A.; Sanaie, S.; Samadi, P.; Yousefi, M.; Nader, N.D. SARS-CoV-2: Unique Challenges of the Virus and Vaccines. Immunol. Investig. 2021, 50, 802–809. [Google Scholar] [CrossRef]
- Sharma, O.; Sultan, A.A.; Ding, H.; Triggle, C.R. A Review of the Progress and Challenges of Developing a Vaccine for COVID-19. Front. Immunol. 2020, 11, 585354. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, H.; Durkee-Shock, J.; Jensen-Wachspress, M.; Kankate, V.V.; Lang, H.; Lazarski, C.A.; Keswani, A.; Webber, K.C.; Montgomery-Recht, K.; Walkiewicz, M.; et al. Robust Antibody and T Cell Responses to SARS-CoV-2 in Patients with Antibody Deficiency. J. Clin. Immunol. 2021, 41, 1146–1153. [Google Scholar] [CrossRef] [PubMed]
- Ameratunga, R.; Longhurst, H.; Steele, R.; Lehnert, K.; Leung, E.; Brooks, A.E.; Woon, S.-T. Common Variable Immunodeficiency Disorders, T-Cell Responses to SARS-CoV-2 Vaccines, and the Risk of Chronic COVID-19. J. Allergy Clin. Immunol. Pract. 2021, 9, 3575–3583. [Google Scholar] [CrossRef]
- D’Amelio, R.; Asero, R.; Cassatella, M.A.; Laganà, B.; Lunardi, C.; Migliorini, P.; Nisini, R.; Parronchi, P.; Quinti, I.; Racanelli, V.; et al. Anti-COVID-19 Vaccination in Patients with Autoimmune-Autoinflammatory Disorders and Primary/Secondary Immunodeficiencies: The Position of the Task Force on Behalf of the Italian Immunological Societies. Biomedicines 2021, 9, 1163. [Google Scholar] [CrossRef]
- Arroyo-Sánchez, D.; Cabrera-Marante, O.; Laguna-Goya, R.; Almendro-Vázquez, P.; Carretero, O.; Gil-Etayo, F.J.; Suàrez-Fernández, P.; Pérez-Romero, P.; de Frías, E.R.; Serrano, A.; et al. Immunogenicity of Anti-SARS-CoV-2 Vaccines in Common Variable Immunodeficiency. J. Clin. Immunol. 2021, 42, 240–252. [Google Scholar] [CrossRef]
- Hagin, D.; Freund, T.; Navon, M.; Halperin, T.; Adir, D.; Marom, R.; Levi, I.; Benor, S.; Alcalay, Y.; Freund, N.T. Immunogenicity of Pfizer-BioNTech COVID-19 vaccine in patients with inborn errors of immunity. J. Allergy Clin. Immunol. 2021, 148, 739–749. [Google Scholar] [CrossRef] [PubMed]
- Ni, L.; Ye, F.; Cheng, M.-L.; Feng, Y.; Deng, Y.-Q.; Zhao, H.; Wei, P.; Ge, J.; Gou, M.; Li, X.; et al. Detection of SARS-CoV-2-Specific Humoral and Cellular Immunity in COVID-19 Convalescent Individuals. Immunity 2020, 52, 971–977.e3. [Google Scholar] [CrossRef]
- Bergman, P.; Blennow, O.; Hansson, L.; Mielke, S.; Nowak, P.; Chen, P.; Söderdahl, G.; Österborg, A.; Smith, C.I.E.; Wullimann, D.; et al. Safety and efficacy of the mRNA BNT162b2 vaccine against SARS-CoV-2 in five groups of immunocompromised patients and healthy controls in a prospective open-label clinical trial. Ebiomedicine 2021, 74, 103705. [Google Scholar] [CrossRef] [PubMed]
- Shields, A.M.; Faustini, S.E.; Hill, H.J.; Al-Taei, S.; Tanner, C.; Ashford, F.; Workman, S.; Moreira, F.; Verma, N.; Wagg, H.; et al. SARS-CoV-2 Vaccine Responses in Individuals with Antibody Deficiency: Findings from the COV-AD Study. J. Clin. Immunol. 2022, 42, 923–934. [Google Scholar] [CrossRef] [PubMed]
- Salinas, A.F.; Mortari, E.P.; Terreri, S.; Quintarelli, C.; Pulvirenti, F.; Di Cecca, S.; Guercio, M.; Milito, C.; Bonanni, L.; Auria, S.; et al. SARS-CoV-2 Vaccine Induced Atypical Immune Responses in Antibody Defects: Everybody Does their Best. J. Clin. Immunol. 2021, 41, 1709–1722. [Google Scholar] [CrossRef] [PubMed]
- Mairhofer, M.; Kausche, L.; Kaltenbrunner, S.; Ghanem, R.; Stegemann, M.; Klein, K.; Pammer, M.; Rauscher, I.; Salzer, H.J.; Doppler, S.; et al. Humoral and cellular immune responses in SARS-CoV-2 mRNA-vaccinated patients with cancer. Cancer Cell 2021, 39, 1171–1172. [Google Scholar] [CrossRef]
- Liu, Y.; Wu, Y.; Lam, K.-T.; Lee, P.P.-W.; Tu, W.; Lau, Y.-L. Dendritic and T Cell Response to Influenza is Normal in the Patients with X-Linked Agammaglobulinemia. J. Clin. Immunol. 2012, 32, 421–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mieves, J.F.; Wittke, K.; Freitag, H.; Volk, H.-D.; Scheibenbogen, C.; Hanitsch, L.G. Influenza Vaccination in Patients with Common Variable Immunodeficiency (CVID). Curr. Allergy Asthma Rep. 2017, 17, 78. [Google Scholar] [CrossRef]
- Pulvirenti, F.; Salinas, A.F.; Milito, C.; Terreri, S.; Mortari, E.P.; Quintarelli, C.; Di Cecca, S.; Lagnese, G.; Punziano, A.; Guercio, M.; et al. B Cell Response Induced by SARS-CoV-2 Infection Is Boosted by the BNT162b2 Vaccine in Primary Antibody Deficiencies. Cells 2021, 10, 2915. [Google Scholar] [CrossRef]
- Bonifacius, A.; Tischer-Zimmermann, S.; Dragon, A.C.; Gussarow, D.; Vogel, A.; Krettek, U.; Gödecke, N.; Yilmaz, M.; Kraft, A.R.; Hoeper, M.M.; et al. COVID-19 immune signatures reveal stable antiviral T cell function despite declining humoral responses. Immunity 2021, 54, 340–354.e6. [Google Scholar] [CrossRef]
- Koerber, N.; Priller, A.; Yazici, S.; Bauer, T.; Cheng, C.-C.; Mijočević, H.; Wintersteller, H.; Jeske, S.; Vogel, E.; Feuerherd, M.; et al. Dynamics of spike-and nucleocapsid specific immunity during long-term follow-up and vaccination of SARS-CoV-2 convalescents. Nat. Commun. 2022, 13, 153. [Google Scholar] [CrossRef]
- Goldberg, Y.; Mandel, M.; Bar-On, Y.M.; Bodenheimer, O.; Freedman, L.S.; Ash, N.; Alroy-Preis, S.; Huppert, A.; Milo, R. Protection and Waning of Natural and Hybrid Immunity to SARS-CoV-2. N. Engl. J. Med. 2022, 386, 2201–2212. [Google Scholar] [CrossRef]
- Krüttgen, A.; Haase, G.; Haefner, H.; Imöhl, M.; Kleines, M. Large inter-individual variability of cellular and humoral immunological responses to mRNA-1273 (Moderna) vaccination against SARS-CoV-2 in health care workers. Clin. Exp. Vaccine Res. 2022, 11, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Han, K.; Shao, X.; Zheng, H.; Wu, C.; Zhu, J.; Zheng, X.; Zhang, Y. Revaccination of non- and low- responders after a standard three dose hepatitis B vaccine schedule. Hum. Vaccines Immunother. 2012, 8, 1845–1849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pilz, S.; Theiler-Schwetz, V.; Trummer, C.; Krause, R.; Ioannidis, J.P. SARS-CoV-2 reinfections: Overview of efficacy and duration of natural and hybrid immunity. Environ. Res. 2022, 209, 112911. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CVID No. = 20 | SID No. = 20 | Healthy Controls No. = 81 | |
|---|---|---|---|
| M/F | 6/14 (30%/70%) | 5/15 (25%/75%) | 21/60 (26%/74%) |
| Age (years) | 49.8 ± 16.4 | 67.9 ± 8.8 | 48.1 ± 15.6 |
| IgG at diagnosis (mg/dL) | 464 ± 276 499 (269–595) | 720 ± 1106 369 (162–816) | NA |
| IgA at diagnosis (mg/dL) | 41 ± 44 40 (0–51) | 56 ± 64 25 (12–104) | NA |
| IgM at diagnosis (mg/dL) | 64 ± 112 17 (5–52) | 32 ± 45 11 (8–43) | NA |
| CD4+ T-lymphocytes (/uL) | 659 ± 288 598 (431–870) | 900 ± 650 725 (436–1222) | NA |
| CD8+ T-lymphocytes (/uL) | 574 ± 414 530 (257–682) | 751 ± 370 709 (440–1047) | NA |
| IgRT | SCIG 6/20 (30%) IVIG 13/20 (65%) | IVIG 15/20 (75%) | NA |
| COVID-19 prior to vaccine | 5/20 (25%) | 3/20 (15%) | 31/81 (38%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohamed, K.M.; Guevara-Hoyer, K.; García, C.J.; Bravo, L.G.; Jiménez-Huete, A.; de la Peña, A.R.; Valeros, B.M.; Velázquez, C.C.; López, E.C.; Cabello, N.; et al. Specific Cellular and Humoral Immune Responses to the Neoantigen RBD of SARS-CoV-2 in Patients with Primary and Secondary Immunodeficiency and Healthy Donors. Biomedicines 2023, 11, 1042. https://doi.org/10.3390/biomedicines11041042
Mohamed KM, Guevara-Hoyer K, García CJ, Bravo LG, Jiménez-Huete A, de la Peña AR, Valeros BM, Velázquez CC, López EC, Cabello N, et al. Specific Cellular and Humoral Immune Responses to the Neoantigen RBD of SARS-CoV-2 in Patients with Primary and Secondary Immunodeficiency and Healthy Donors. Biomedicines. 2023; 11(4):1042. https://doi.org/10.3390/biomedicines11041042
Chicago/Turabian StyleMohamed, Kauzar Mohamed, Kissy Guevara-Hoyer, Carlos Jiménez García, Laura García Bravo, Adolfo Jiménez-Huete, Antonia Rodríguez de la Peña, Beatriz Mediero Valeros, Cristina Cañizares Velázquez, Esther Culebras López, Noemí Cabello, and et al. 2023. "Specific Cellular and Humoral Immune Responses to the Neoantigen RBD of SARS-CoV-2 in Patients with Primary and Secondary Immunodeficiency and Healthy Donors" Biomedicines 11, no. 4: 1042. https://doi.org/10.3390/biomedicines11041042
APA StyleMohamed, K. M., Guevara-Hoyer, K., García, C. J., Bravo, L. G., Jiménez-Huete, A., de la Peña, A. R., Valeros, B. M., Velázquez, C. C., López, E. C., Cabello, N., Estrada, V., Corbí, Á. L., Fernández-Arquero, M., Ocaña, A., Delgado-Iribarren, A., Martínez-Novillo, M., Bolaños, E., Anguita, E., Peña, A., ... Sánchez-Ramón, S. (2023). Specific Cellular and Humoral Immune Responses to the Neoantigen RBD of SARS-CoV-2 in Patients with Primary and Secondary Immunodeficiency and Healthy Donors. Biomedicines, 11(4), 1042. https://doi.org/10.3390/biomedicines11041042