
Physiopathology of Osteoporosis: Nursing Involvement and Management

 , and
, and 
Abstract
:1. Introduction
2. Pathophysiology
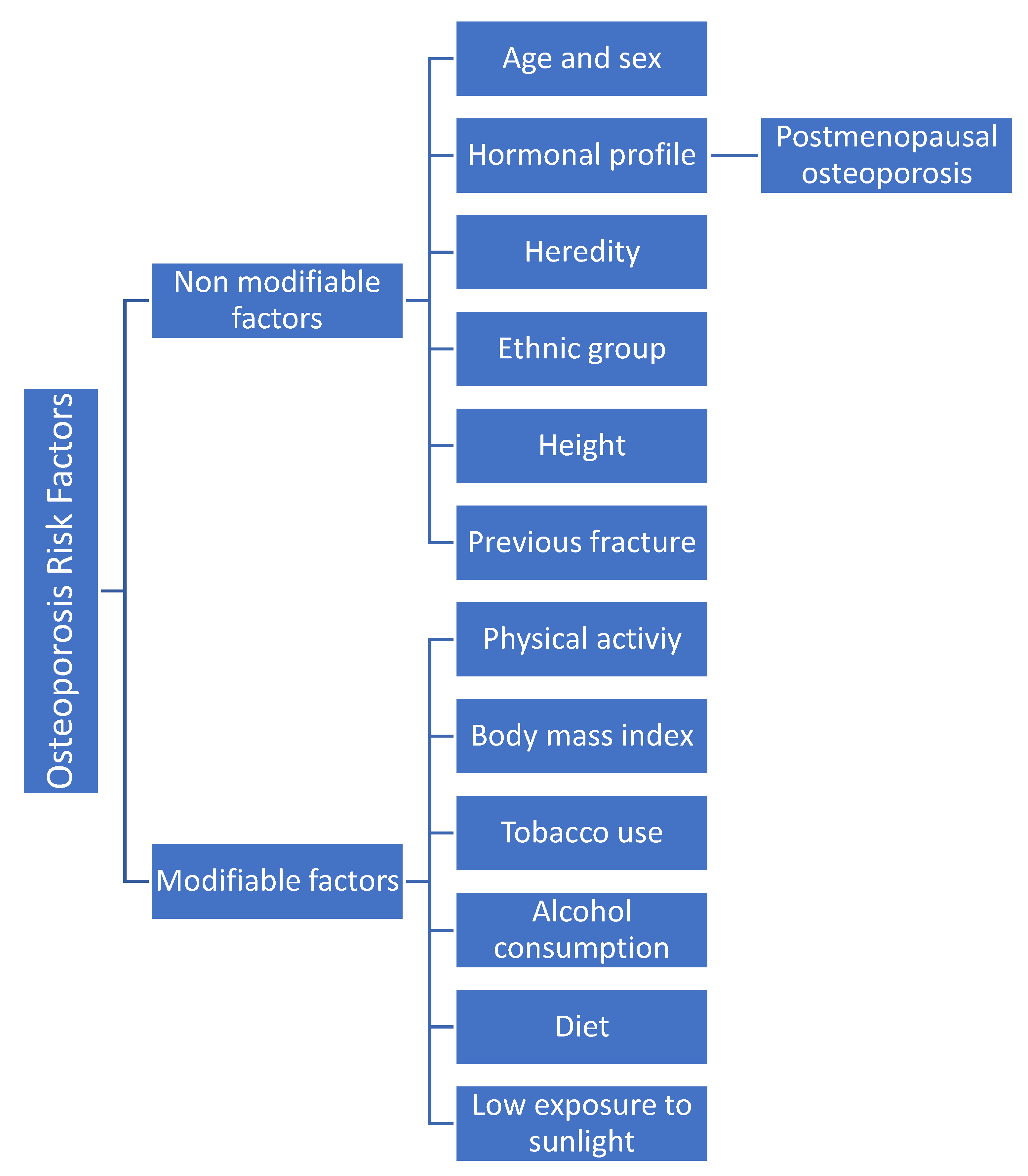
3. Risk Factors
3.1. Non-Modifiable Factors
3.1.1. Age and Sex
3.1.2. Hormonal Profile
3.1.3. Postmenopausal Osteoporosis
3.1.4. Heredity
3.1.5. Ethnic Group
3.1.6. Height
3.1.7. Previous Fracture
3.2. Modifiable Factors
3.2.1. Physical Activity
3.2.2. Body Mass Index (BMI)
3.2.3. Tobacco Use
3.2.4. Alcohol Consumption
3.2.5. Diet
3.2.6. Low Exposure to Sunlight
4. Comorbidities and Pharmacotherapy
5. Diagnosis of Osteoporosis
6. Prevention, Treatment, and Nursing Care in Patients with Osteoporosis
6.1. Physical Exercise
6.2. Diet
6.2.1. Nutrients Favorable for Bone Health
Calcium and Vitamin D
Vitamin K
6.2.2. Proteins
6.2.3. Other Compounds in the Diet
6.3. Nutrients Unfavorable for Bone Healths
7. Factors Unfavorable for Bone Health
7.1. Tobacco Use
7.2. Alcohol Consumption
7.3. Pharmacological Treatment
7.3.1. Alendronate
7.3.2. Risedronate
7.3.3. Ibandronate
7.3.4. Denosumab
7.3.5. Romosozumab
7.4. Hormonal Treatment
7.5. Health Information and Education
7.6. Osteoporosis Management
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Compston, J.; Cooper, A.; Cooper, C.; Gittoes, N.; Gregson, C.; Harvey, N.; Hope, S.; Kanis, J.A.; McCloskey, E.V.; Poole, K.E.S.; et al. UK clinical guideline for the prevention and treatment of osteoporosis. Arch. Osteoporos. 2017, 12, 43. [Google Scholar] [CrossRef] [PubMed]
- Faienza, M.F.; Ventura, A.; Marzano, F.; Cavallo, L. Postmenopausal osteoporosis: The role of immune system cells. Clin. Dev. Immunol. 2013, 2013, 575936. [Google Scholar] [CrossRef] [PubMed]
- Curtis, E.; Litwic, A.; Cooper, C.; Dennison, E. Determinants of Muscle and Bone Aging. J. Cell. Physiol. 2015, 230, 2618–2625. [Google Scholar] [CrossRef] [PubMed]
- Vina, J.; Rodriguez-Manas, L.; Salvador-Pascual, A.; Tarazona-Santabalbina, F.J.; Gomez-Cabrera, M.C. Exercise: The lifelong supplement for healthy ageing and slowing down the onset of frailty. J. Physiol. 2016, 594, 1989–1999. [Google Scholar] [CrossRef] [PubMed]
- Agostini, D.; Zeppa Donati, S.; Lucertini, F.; Annibalini, G.; Gervasi, M.; Ferri Marini, C.; Piccoli, G.; Stocchi, V.; Barbieri, E.; Sestili, P. Muscle and Bone Health in Postmenopausal Women: Role of Protein and Vitamin D Supplementation Combined with Exercise Training. Nutrients 2018, 10, 1103. [Google Scholar] [CrossRef] [PubMed]
- Svedbom, A.; Hernlund, E.; Ivergard, M.; Compston, J.; Cooper, C.; Stenmark, J.; McCloskey, E.V.; Jonsson, B.; Kanis, J.A.; EU review panel of the IOF. Osteoporosis in the European Union: A compendium of country-specific reports. Arch. Osteoporos. 2013, 8, 137. [Google Scholar] [CrossRef]
- Curtis, E.M.; Moon, R.J.; Harvey, N.C.; Cooper, C. The impact of fragility fracture and approaches to osteoporosis risk assessment worldwide. Bone 2017, 104, 29–38. [Google Scholar] [CrossRef]
- Gass, M.; Dawson-Hughes, B. Preventing osteoporosis-related fractures: An overview. Am. J. Med. 2006, 119, S3–S11. [Google Scholar] [CrossRef]
- Gianoudis, J.; Bailey, C.A.; Sanders, K.M.; Nowson, C.A.; Hill, K.; Ebeling, P.R.; Daly, R.M. Osteo-cise: Strong bones for life: Protocol for a community-based randomised controlled trial of a multi-modal exercise and osteoporosis education program for older adults at risk of falls and fractures. BMC Musculoskelet. Disord. 2012, 13, 78. [Google Scholar] [CrossRef]
- Kanis, J.A.; McCloskey, E.V.; Johansson, H.; Cooper, C.; Rizzoli, R.; Reginster, J.Y. on behalf of the Scientific Advisory Board of the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO) and the Committee of Scientific Advisors of the International Osteoporosis Foundation (IOF). European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos. Int. 2013, 24, 23–57. [Google Scholar] [CrossRef]
- Martin Jimenez, J.A.; Consuegra Moya, B.; Martin Jimenez, M.T. Nutritional factors in preventing osteoporosis. Nutr. Hosp. 2015, 32 (Suppl. S1), 49–55. [Google Scholar] [CrossRef] [PubMed]
- Tella, S.H.; Gallagher, J.C. Prevention and treatment of postmenopausal osteoporosis. J. Steroid Biochem. Mol. Biol. 2014, 142, 155–170. [Google Scholar] [CrossRef] [PubMed]
- Kamel, H.K. Postmenopausal osteoporosis: Etiology, current diagnostic strategies, and nonprescription interventions. J. Manag. Care Pharm. 2006, 12, S4–S9. [Google Scholar] [CrossRef] [PubMed]
- Rachner, T.D.; Khosla, S.; Hofbauer, L.C. Osteoporosis: Now and the future. Lancet 2011, 377, 1276–1287. [Google Scholar] [CrossRef] [PubMed]
- Fischer, V.; Haffner-Luntzer, M. Interaction between bone and immune cells: Implications for postmenopausal osteoporosis. Semin. Cell Dev. Biol. 2022, 123, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Bijelic, R.; Milicevic, S.; Balaban, J. Risk Factors for Osteoporosis in Postmenopausal Women. Med. Arch. 2017, 71, 25–28. [Google Scholar] [CrossRef]
- Osteoporosis—Prevention, diagnosis and treatment. A systematic literature review. SBU conclusions and summary. Lakartidningen 2003, 100, 3590–3595. [Google Scholar]
- Sayed, S.A.; Khaliq, A.; Mahmood, A. Evaluating The Risk Of Osteoporosis Through Bone Mass Density. J. Ayub Med. Coll. Abbottabad 2016, 28, 730–733. [Google Scholar]
- Janiszewska, M.; Firlej, E.; Dziedzic, M.; Zolnierczuk-Kieliszek, D. Health beliefs and sense of one’s own efficacy and prophylaxis of osteoporosis in peri- and post-menopausal women. Ann. Agric. Environ. Med. 2016, 23, 167–173. [Google Scholar] [CrossRef]
- Maeda, S.S.; Lazaretti-Castro, M. An overview on the treatment of postmenopausal osteoporosis. Arq. Bras. De Endocrinol. Metabol. 2014, 58, 162–171. [Google Scholar] [CrossRef]
- Barrett-Connor, E.; Siris, E.S.; Wehren, L.E.; Miller, P.D.; Abbott, T.A.; Berger, M.L.; Santora, A.C.; Sherwood, L.M. Osteoporosis and fracture risk in women of different ethnic groups. J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 2005, 20, 185–194. [Google Scholar] [CrossRef] [PubMed]
- Berard, A.; Bravo, G.; Gauthier, P. Meta-analysis of the effectiveness of physical activity for the prevention of bone loss in postmenopausal women. Osteoporos. Int. 1997, 7, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Kortebein, P.; Ferrando, A.; Lombeida, J.; Wolfe, R.; Evans, W.J. Effect of 10 days of bed rest on skeletal muscle in healthy older adults. Jama 2007, 297, 1772–1774. [Google Scholar] [CrossRef]
- Johnell, O.; Gullberg, B.; Kanis, J.A.; Allander, E.; Elffors, L.; Dequeker, J.; Dilsen, G.; Gennari, C.; Lopes Vaz, A.; Lyritis, G.; et al. Risk factors for hip fracture in European women: The MEDOS Study. Mediterranean Osteoporosis Study. J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 1995, 10, 1802–1815. [Google Scholar] [CrossRef] [PubMed]
- De Laet, C.; Kanis, J.A.; Oden, A.; Johanson, H.; Johnell, O.; Delmas, P.; Eisman, J.A.; Kroger, H.; Fujiwara, S.; Garnero, P.; et al. Body mass index as a predictor of fracture risk: A meta-analysis. Osteoporos. Int. 2005, 16, 1330–1338. [Google Scholar] [CrossRef]
- Kanis, J.A.; Johansson, H.; Johnell, O.; Oden, A.; De Laet, C.; Eisman, J.A.; Pols, H.; Tenenhouse, A. Alcohol intake as a risk factor for fracture. Osteoporos. Int. 2005, 16, 737–742. [Google Scholar] [CrossRef]
- Xu, L.; McElduff, P.; D’Este, C.; Attia, J. Does dietary calcium have a protective effect on bone fractures in women? A meta-analysis of observational studies. Br. J. Nutr. 2004, 91, 625–634. [Google Scholar] [CrossRef]
- Darba, J.; Kaskens, L.; Perez-Alvarez, N.; Palacios, S.; Neyro, J.L.; Rejas, J. Disability-adjusted-life-years losses in postmenopausal women with osteoporosis: A burden of illness study. BMC Public Health 2015, 15, 324. [Google Scholar] [CrossRef]
- Siris, E.S.; Adler, R.; Bilezikian, J.; Bolognese, M.; Dawson-Hughes, B.; Favus, M.J.; Harris, S.T.; Jan de Beur, S.M.; Khosla, S.; Lane, N.E.; et al. The clinical diagnosis of osteoporosis: A position statement from the National Bone Health Alliance Working Group. Osteoporos. Int. 2014, 25, 1439–1443. [Google Scholar] [CrossRef]
- Kling, J.M.; Clarke, B.L.; Sandhu, N.P. Osteoporosis prevention, screening, and treatment: A review. J. Womens Health 2014, 23, 563–572. [Google Scholar] [CrossRef]
- Simas, V.; Hing, W.; Pope, R.; Climstein, M. Effects of water-based exercise on bone health of middle-aged and older adults: A systematic review and meta-analysis. Open Access J. Sports Med. 2017, 8, 39–60. [Google Scholar] [CrossRef] [PubMed]
- Nikander, R.; Sievanen, H.; Heinonen, A.; Daly, R.M.; Uusi-Rasi, K.; Kannus, P. Targeted exercise against osteoporosis: A systematic review and meta-analysis for optimising bone strength throughout life. BMC Med. 2010, 8, 47. [Google Scholar] [CrossRef] [PubMed]
- Carter, N.D.; Khan, K.M.; McKay, H.A.; Petit, M.A.; Waterman, C.; Heinonen, A.; Janssen, P.A.; Donaldson, M.G.; Mallinson, A.; Riddell, L.; et al. Community-based exercise program reduces risk factors for falls in 65- to 75-year-old women with osteoporosis: Randomized controlled trial. CMAJ 2002, 167, 997–1004. [Google Scholar] [PubMed]
- Otero, M.; Esain, I.; Gonzalez-Suarez, A.M.; Gil, S.M. The effectiveness of a basic exercise intervention to improve strength and balance in women with osteoporosis. Clin. Interv. Aging 2017, 12, 505–513. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Kuang, X.; Li, K.; Guo, X.; Deng, Q.; Li, D. Effects of combined calcium and vitamin D supplementation on osteoporosis in postmenopausal women: A systematic review and meta-analysis of randomized controlled trials. Food Funct. 2020, 11, 10817–10827. [Google Scholar] [CrossRef]
- Weaver, C.M.; Alexander, D.D.; Boushey, C.J.; Dawson-Hughes, B.; Lappe, J.M.; LeBoff, M.S.; Liu, S.; Looker, A.C.; Wallace, T.C.; Wang, D.D. Calcium plus vitamin D supplementation and risk of fractures: An updated meta-analysis from the National Osteoporosis Foundation. Osteoporos. Int. 2016, 27, 367–376. [Google Scholar] [CrossRef]
- Chevalley, T.; Brandi, M.L.; Cashman, K.D.; Cavalier, E.; Harvey, N.C.; Maggi, S.; Cooper, C.; Al-Daghri, N.; Bock, O.; Bruyere, O.; et al. Role of vitamin D supplementation in the management of musculoskeletal diseases: Update from an European Society of Clinical and Economical Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO) working group. Aging Clin. Exp. Res. 2022, 34, 2603–2623. [Google Scholar] [CrossRef]
- Geyer, C. Postmenopausal Osteoporosis: The Role of Lifestyle in Maintaining Bone Mass and Reducing Fracture Risk. Am. J. Lifestyle Med. 2017, 11, 125–128. [Google Scholar] [CrossRef]
- Lim, S.Y.; Bolster, M.B. Profile of Romosozumab and its potential in the management of osteoporosis. Drug Des. Dev. Ther. 2017, 11, 1221–1231. [Google Scholar] [CrossRef]
- Singh, S.; Dutta, S.; Khasbage, S.; Kumar, T.; Sachin, J.; Sharma, J.; Varthya, S.B. A systematic review and meta-analysis of efficacy and safety of Romosozumab in postmenopausal osteoporosis. Osteoporos. Int. 2022, 33, 1–12. [Google Scholar] [CrossRef]
- Balemans, W.; Ebeling, M.; Patel, N.; Van Hul, E.; Olson, P.; Dioszegi, M.; Lacza, C.; Wuyts, W.; Van Den Ende, J.; Willems, P.; et al. Increased bone density in sclerosteosis is due to the deficiency of a novel secreted protein (SOST). Hum. Mol. Genet. 2001, 10, 537–543. [Google Scholar] [CrossRef]
- Krause, C.; Korchynskyi, O.; de Rooij, K.; Weidauer, S.E.; de Gorter, D.J.; van Bezooijen, R.L.; Hatsell, S.; Economides, A.N.; Mueller, T.D.; Lowik, C.W.; et al. Distinct modes of inhibition by sclerostin on bone morphogenetic protein and Wnt signaling pathways. J. Biol. Chem. 2010, 285, 41614–41626. [Google Scholar] [CrossRef]
- Brunkow, M.E.; Gardner, J.C.; Van Ness, J.; Paeper, B.W.; Kovacevich, B.R.; Proll, S.; Skonier, J.E.; Zhao, L.; Sabo, P.J.; Fu, Y.; et al. Bone dysplasia sclerosteosis results from loss of the SOST gene product, a novel cystine knot-containing protein. Am. J. Hum. Genet. 2001, 68, 577–589. [Google Scholar] [CrossRef]
- Cosman, F.; Crittenden, D.B.; Adachi, J.D.; Binkley, N.; Czerwinski, E.; Ferrari, S.; Hofbauer, L.C.; Lau, E.; Lewiecki, E.M.; Miyauchi, A.; et al. Romosozumab Treatment in Postmenopausal Women with Osteoporosis. N. Engl. J. Med. 2016, 375, 1532–1543. [Google Scholar] [CrossRef]
- Shoback, D.; Rosen, C.J.; Black, D.M.; Cheung, A.M.; Murad, M.H.; Eastell, R. Pharmacological Management of Osteoporosis in Postmenopausal Women: An Endocrine Society Guideline Update. J. Clin. Endocrinol. Metab. 2020, 105, dgaa048. [Google Scholar] [CrossRef]
- Alami, S.; Hervouet, L.; Poiraudeau, S.; Briot, K.; Roux, C. Barriers to Effective Postmenopausal Osteoporosis Treatment: A Qualitative Study of Patients’ and Practitioners’ Views. PLoS ONE 2016, 11, e0158365. [Google Scholar] [CrossRef]
- von Hurst, P.R.; Wham, C.A. Attitudes and knowledge about osteoporosis risk prevention: A survey of New Zealand women. Public Health Nutr. 2007, 10, 747–753. [Google Scholar] [CrossRef]


{kind=link}
| Age Groups | France | UK | Germany | Spain | Italy |
|---|---|---|---|---|---|
| 50–54 | 135 | 127 | 192 | 95 | 128 |
| 55–59 | 200 | 175 | 265 | 126 | 180 |
| 60–64 | 286 | 276 | 328 | 175 | 276 |
| 65–69 | 271 | 308 | 489 | 215 | 335 |
| 70–74 | 364 | 365 | 718 | 270 | 464 |
| 75–79 | 484 | 411 | 672 | 368 | 546 |
| 80–84 | 526 | 417 | 686 | 357 | 558 |
| 50–84 | 2266 | 2079 | 3350 | 1606 | 2487 |
| Food | Ca (mg) | Food | Vitamin D (IU) |
|---|---|---|---|
| Basil | 2.113 | Cod liver oil | 210 |
| Thyme | 1.890 | Eel | 110 |
| Oregano | 1.580 | Caviar | 35 |
| Emmental cheese | 1.185 | Grilled tuna | 25 |
| Semi-skimmed milk powder | 1.050 | Bonito in oil | 24 |
| Zamorano cheese | 999 | Smoked salmon | 19 |
| Laurel | 830 | Prawns | 18 |
| Tetilla cheese | 809 | Anchovies in oil | 11.8 |
| Manchego cheese | 765 | Eggs | 11.4 |
| Cereals, corn, and wheat | 453 | Cereals, wheat, and rice | 8.3 |
| Fresh cheese | 338 | Sardines | 8 |
| Skimmed condensed milk | 330 | Salmon | 8 |
| Sardines in oil | 314 | Anchovies | 8 |
| Eggs | 282 | Mackerel in oil | 4.6 |
| Almonds | 252 | Muesli | 4.2 |
| Milk chocolate | 247 | Pork liver | 2.2 |
| Hazelnuts | 226 | Chicken liver | 1.3 |
| Skimmed Yogurt | 183 | Beef liver | 1.2 |
| Curd | 178 | Natural, enriched yogurt | 1.2 |
| Greek Yogurt | 150 | Cured cheese | 0.9 |
| Chickpeas | 143 | Skimmed condensed milk | 0.8 |
| White beans | 126 | Croissant or cupcake | 0.8 |
| Whole cow’s milk | 124 | Donut | 0.8 |
| Semi-skimmed cow’s milk | 114 | Serrano ham | 0.6 |
| Babies | 0–6 Months Old | 250 mg/day | |
| 7–12 Months Old | 300 mg/day | ||
| Children and teenagers | 1–3 years old | 500 mg/day | |
| 4–9 years old | 800 mg/day | ||
| 10–19 years old | 1.300 mg/day | ||
| Pregnant women | 1.400 mg/day | ||
| Nursing mothers | 1.500 mg/day | ||
| Men | Women | ||
| Adults | 20–50 years old | 1.000 mg/day | 1.200 mg/day |
| 51–70 years old | 1.200 mg/day | 1.200 mg/day | |
| Over 70 years | 1.300 mg/day | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valenzuela-Martínez, S.; Ramírez-Expósito, M.J.; Carrera-González, M.P.; Martínez-Martos, J.M. Physiopathology of Osteoporosis: Nursing Involvement and Management. Biomedicines 2023, 11, 1220. https://doi.org/10.3390/biomedicines11041220
Valenzuela-Martínez S, Ramírez-Expósito MJ, Carrera-González MP, Martínez-Martos JM. Physiopathology of Osteoporosis: Nursing Involvement and Management. Biomedicines. 2023; 11(4):1220. https://doi.org/10.3390/biomedicines11041220
Chicago/Turabian StyleValenzuela-Martínez, Sandra, María Jesús Ramírez-Expósito, María Pilar Carrera-González, and José Manuel Martínez-Martos. 2023. "Physiopathology of Osteoporosis: Nursing Involvement and Management" Biomedicines 11, no. 4: 1220. https://doi.org/10.3390/biomedicines11041220
APA StyleValenzuela-Martínez, S., Ramírez-Expósito, M. J., Carrera-González, M. P., & Martínez-Martos, J. M. (2023). Physiopathology of Osteoporosis: Nursing Involvement and Management. Biomedicines, 11(4), 1220. https://doi.org/10.3390/biomedicines11041220