

Association between Antihyperlipidemic Agent Use and Age-Related Macular Degeneration in Patients with Hyperlipidemia: A Population-Based Retrospective Cohort Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
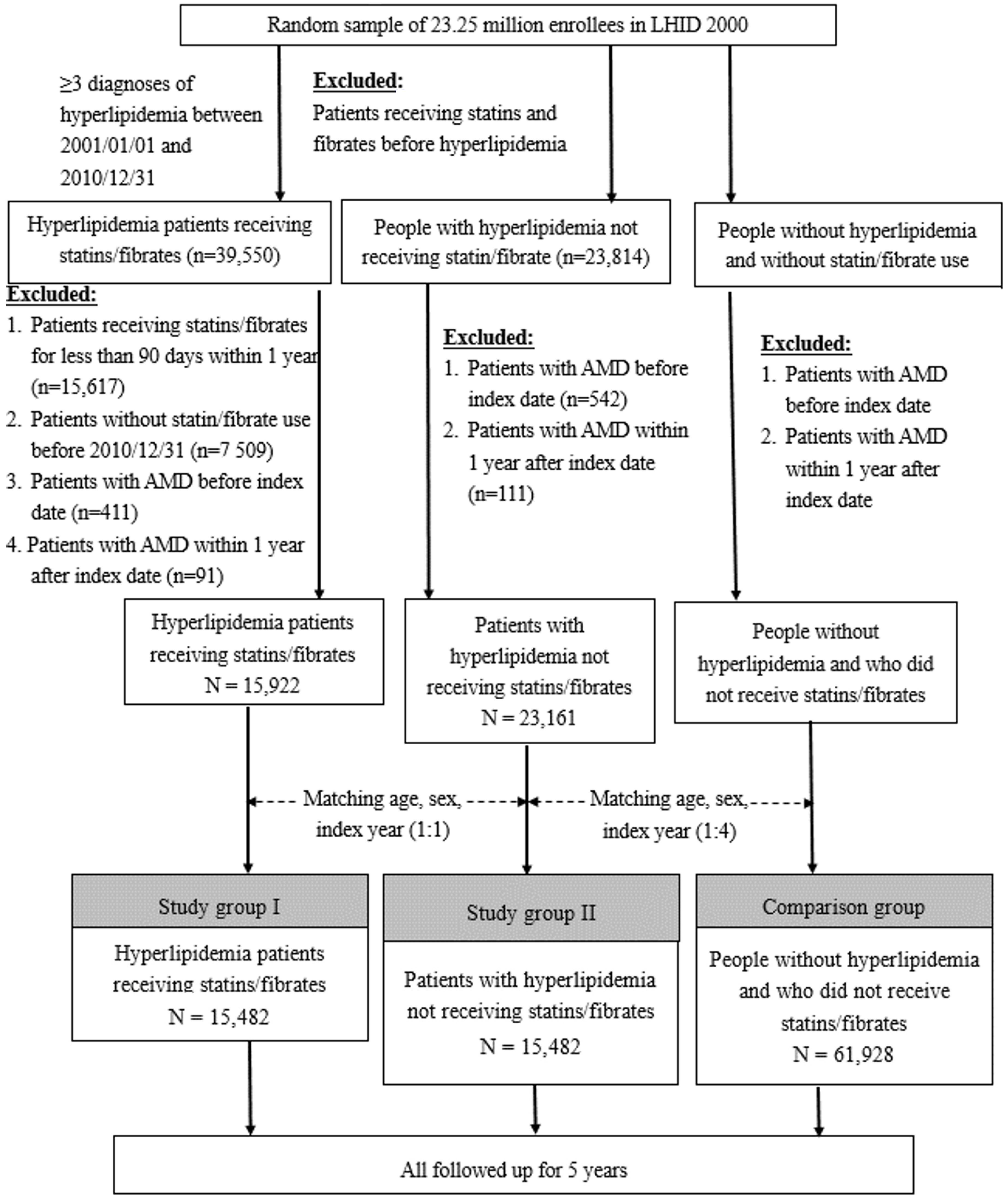
2.2. Study Population
2.2.1. Study Group I
2.2.2. Study Group II
2.2.3. Comparison Group
2.3. Primary Outcome Measurement
2.4. Secondary Outcome Measurement
2.5. Confounders
2.6. Statistical Analysis
3. Results
Baseline Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Crude HR (95% CI) | p-Value | Adjusted HR (95% CI) | p-Value | |
|---|---|---|---|---|
| Age, years (mean ± SD) | 1.048 (1.040–1.057) | <0.0001 | 1.045 (1.035–1.055) | <0.0001 |
| Gender/male (n, %) | 1.000 (0.852–1.174) | 1.0000 | 1.015 (0.86–1.199) | 0.8561 |
| Hypertension | 1.394 (1.162–1.674) | 0.0004 | 1.050 (0.864–1.276) | 0.6235 |
| DM | 1.332 (1.135–1.563) | 0.0004 | 1.153 (0.976–1.362) | 0.0932 |
| Cerebrovascular disease | 1.199 (0.944–1.523) | 0.1362 | 0.880 (0.622–1.247) | 0.4726 |
| CAD | 1.383 (1.170–1.634) | 0.0001 | 1.065 (0.884–1.283) | 0.5073 |
| Heart failure | 1.431 (1.100–1.861) | 0.0075 | 0.991 (0.751–1.308) | 0.9486 |
| Atrial fibrillation | 1.449 (0.868–2.419) | 0.1560 | 1.029 (0.608–1.739) | 0.9164 |
| Myocardial infarction | 1.079 (0.537–2.165) | 0.8316 | 0.839 (0.415–1.696) | 0.6241 |
| Atherosclerosis | 1.527 (1.095–2.130) | 0.0125 | 1.173 (0.836–1.644) | 0.3561 |
| Stroke | 1.255 (1.035–1.522) | 0.0209 | 0.955 (0.717–1.271) | 0.7525 |
| Peripheral vascular disease | 1.367 (0.976–1.914) | 0.0690 | 1.111 (0.79–1.562) | 0.5463 |
| Glaucoma | 2.052 (1.613–2.609) | <0.0001 | 1.753 (1.372–2.241) | <0.0001 |
| Diabetic retinopathy | 1.541 (1.100–2.158) | 0.0119 | 1.234 (0.87–1.75) | 0.2391 |
| Cataract surgery | 1.613 (1.263–2.059) | 0.0001 | 0.951 (0.734–1.231) | 0.7021 |
| Obesity | 0.791 (0.328–1.908) | 0.6021 | 0.887 (0.367–2.141) | 0.7895 |
| Tobacco use disorder, alcohol abuse | 1.544 (0.909–2.623) | 0.1082 | 1.672 (0.979–2.857) | 0.06 |
| Aspirin | 1.323 (1.128–1.551) | 0.0006 | 0.594 (0.234–1.504) | 0.2716 |
| Warfarin | 1.346 (1.148–1.579) | 0.0003 | 1.727 (0.68–4.385) | 0.2502 |
| Hormone replacement therapy | 1.071 (0.742–1.545) | 0.7153 | 1.207 (0.83–1.756) | 0.3243 |
| NSAID | 1.124 (0.764–1.653) | 0.5533 | 1.080 (0.731–1.595) | 0.6999 |
| Antihypertensive agents | 1.375 (1.171–1.615) | 0.0001 | 1.136 (0.956–1.349) | 0.147 |
References
- AAO PPP Retina/Vitreous Committee; Hoskins Center for Quality Eye Care. Age-Related Macular Degeneration Preferred Practice Pattern Guideline. Available online: https://www.aao.org/preferred-practice-pattern/age-related-macular-degeneration-ppp (accessed on 20 May 2021).
- American Optometric Association. Care of the Patient with Age-Related Macular Degeneration. Available online: https://www.aoa.org/practice/clinical-guidelines/clinical-practice-guidelines?sso=y (accessed on 20 May 2021).
- Pennington, K.L.; DeAngelis, M.M. Epidemiology of age-related macular degeneration (AMD): Associations with cardiovascular disease phenotypes and lipid factors. Eye Vis. (Lond.) 2016, 3, 34. [Google Scholar] [CrossRef]
- Curcio, C.A.; Millican, C.L.; Bailey, T.; Kruth, H.S. Accumulation of cholesterol with age in human Bruch’s membrane. Investig. Ophthalmol. Vis. Sci. 2001, 42, 265–274. [Google Scholar]
- Chen, S.J.; Cheng, C.Y.; Peng, K.L.; Li, A.F.; Hsu, W.M.; Liu, J.H.; Chou, P. Prevalence and associated risk factors of age-related macular degeneration in an elderly Chinese population in Taiwan: The Shihpai Eye Study. Investig. Ophthalmol. Vis. Sci. 2008, 49, 3126–3133. [Google Scholar] [CrossRef] [PubMed]
- Huang, E.J.; Wu, S.H.; Lai, C.H.; Kuo, C.N.; Wu, P.L.; Chen, C.L.; Chen, C.Y.; King, Y.C.; Wu, P.C. Prevalence and risk factors for age-related macular degeneration in the elderly Chinese population in south-western Taiwan: The Puzih eye study. Eye (Lond. Engl.) 2014, 28, 705–714. [Google Scholar] [CrossRef] [PubMed]
- Heesterbeek, T.J.; Lorés-Motta, L.; Hoyng, C.B.; Lechanteur, Y.T.E.; den Hollander, A.I. Risk factors for progression of age-related macular degeneration. Ophthalmic Physiol. Opt. 2020, 40, 140–170. [Google Scholar] [CrossRef]
- Vassilev, Z.P.; Ruigómez, A.; Soriano-Gabarró, M.; García Rodríguez, L.A. Diabetes, Cardiovascular Morbidity, and Risk of Age-Related Macular Degeneration in a Primary Care Population. Investig. Ophthalmol. Vis. Sci. 2015, 56, 1585–1592. [Google Scholar] [CrossRef]
- Sasso, F.C.; Pafundi, P.C.; Gelso, A.; Bono, V.; Costagliola, C.; Marfella, R.; Sardu, C.; Rinaldi, L.; Galiero, R.; Acierno, C.; et al. High HDL cholesterol: A risk factor for diabetic retinopathy? Findings from NO BLIND study. Diabetes Res. Clin. Pract. 2019, 150, 236–244. [Google Scholar] [CrossRef]
- Davari, M.H.; Gheitasi, H.; Yaghobi, G.; Heydari, B. Correlation between serum lipids and age-related macular degeneration: A case-control study. J. Res. Health Sci. 2013, 13, 98–101. [Google Scholar]
- Ebrahimi, K.B.; Handa, J.T. Lipids, Lipoproteins, and Age-Related Macular Degeneration. J. Lipids 2011, 2011, 802059. [Google Scholar] [CrossRef]
- van Leeuwen, E.M.; Emri, E.; Merle, B.; Colijn, J.M.; Kersten, E.; Cougnard-Gregoire, A.; Dammeier, S.; Meester-Smoor, M.; Pool, F.M.; de Jong, E.K.; et al. A new perspective on lipid research in age-related macular degeneration. Prog. Retin. Eye Res. 2018, 6756–6786. [Google Scholar] [CrossRef]
- Peponis, V.; Chalkiadakis, S.E.; Bonovas, S.; Sitaras, N.M. The controversy over the association between statins use and progression of age-related macular degeneration: A mini review. Clin. Ophthalmol. (Auckl. NZ) 2010, 2010, 4865–4869. [Google Scholar] [CrossRef]
- Ma, L.; Wang, Y.; Du, J.; Wang, M.; Zhang, R.; Fu, Y. The association between statin use and risk of age-related macular degeneration. Sci. Rep. 2015, 5, 518280. [Google Scholar] [CrossRef] [PubMed]
- Gehlbach, P.; Li, T.; Hatef, E. Statins for age-related macular degeneration. Cochrane Database Syst. Rev. 2016, 2016, CD006927. [Google Scholar] [CrossRef] [PubMed]
- Prakash, G.; Agrawal, R.; Natung, T. Role of Lipids in Retinal Vascular and Macular Disorders. Indian J. Clin. Biochem. IJCB 2017, 32, 3–8. [Google Scholar] [CrossRef]
- Al-Janabi, A.; Lightman, S.; Tomkins-Netzer, O. Statins in retinal diseas’. Eye (Lond. Engl.) 2018, 32, 981–991. [Google Scholar] [CrossRef]
- Roizenblatt, M.; Naranjit, N.; Maia, M.; Gehlbach, P.L. The Question of a Role for Statins in Age-Related Macular Degeneration. Int. J. Mol. Sci. 2018, 19, 3688. [Google Scholar] [CrossRef]
- Garcia-Ramírez, M.; Hernández, C.; Palomer, X.; Vázquez-Carrera, M.; Simó, R. Fenofibrate prevents the disruption of the outer blood retinal barrier through downregulation of NF-κB activity. Acta Diabetol. 2016, 53, 109–118. [Google Scholar] [CrossRef]
- Qiu, F.; Matlock, G.; Chen, Q.; Zhou, K.; Du, Y.; Wang, X.; Ma, J.X. Therapeutic Effects of PPARα Agonist on Ocular Neovascularization in Models Recapitulating Neovascular Age-Related Macular Degeneration. Investig. Ophthalmol. Vis. Sci. 2017, 58, 5065–5075. [Google Scholar] [CrossRef]
- van der Schaft, T.L.; de Bruijn, W.C.; Mooy, C.M.; Ketelaars, D.A.; de Jong, P.T. Is Basal Laminar Deposit Unique for Age-Related Macular Degeneration? Arch. Ophthalmol. 1991, 109, 420–425. [Google Scholar] [CrossRef]
- Curcio, C.A.; Johnson, M.; Huang, J.D.; Rudolf, M. Aging, age-related macular degeneration, and the response-to-retention of apolipoprotein B-containing lipoproteins. Prog. Retin. Eye Res. 2009, 28, 393–422. [Google Scholar] [CrossRef]
- Kananen, F.; Strandberg, T.; Loukovaara, S.; Immonen, I. Early middle age cholesterol levels and the association with age-related macular degeneration. Acta Ophthalmol. 2021, 99, e1063–e1069. [Google Scholar] [CrossRef] [PubMed]
- VanderBeek, B.L.; Zacks, D.N.; Talwar, N.; Nan, B.; Stein, J.D. Role of statins in the development and progression of age-related macular degeneration. Retina 2013, 33, 414–422. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.B.; Halawa, O.A.; Husain, D.; Miller, J.W.; Vavvas, D.G. Dyslipidemia in age-related macular degeneration. Eye (Lond.) 2022, 36, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Klein, R.; Klein, B.E.; Tomany, S.C.; Cruickshanks, K.J. The association of cardiovascular disease with the long-term incidence of age-related maculopathy: The Beaver Dam Eye Study. Ophthalmology 2003, 110, 1273–1280. [Google Scholar] [CrossRef]
- van Leeuwen, R.; Klaver, C.C.; Vingerling, J.R.; Hofman, A.; van Duijn, C.M.; Stricker, B.H.; de Jong, P.T. Cholesterol and age-related macular degeneration: Is there a link? Am. J. Ophthalmol. 2004, 137, 750–752. [Google Scholar] [CrossRef]
- Cougnard-Grégoire, A.; Delyfer, M.N.; Korobelnik, J.F.; Rougier, M.B.; Le Goff, M.; Dartigues, J.F.; Barberger-Gateau, P.; Delcourt, C. Elevated high-density lipoprotein cholesterol and age-related macular degeneration: The Alienor study. PLoS ONE 2014, 9, e90973. [Google Scholar] [CrossRef]
- Colijn, J.M.; den Hollander, A.I.; Demirkan, A.; Cougnard-Grégoire, A.; Verzijden, T.; Kersten, E.; Meester-Smoor, M.A.; Merle, B.; Papageorgiou, G.; Ahmad, S.; et al. EYE-RISK Consortium. Increased High-Density Lipoprotein Levels Associated with Age-Related Macular Degeneration: Evidence from the EYE-RISK and European Eye Epidemiology Consortia. Ophthalmology 2019, 126, 393–406. [Google Scholar] [CrossRef]
- Rubins, H.B.; Robins, S.J.; Collins, D.; Fye, C.L.; Anderson, J.W.; Elam, M.B.; Faas, F.H.; Linares, E.; Schaefer, E.J.; Schectman, G.; et al. Gemfibrozil for the secondary prevention of coronary heart disease in men with low levels of high-density lipoprotein cholesterol. Veterans Affairs High-Density Lipoprotein Cholesterol Intervention Trial Study Group. N. Engl. J. Med. 1999, 341, 410–418. [Google Scholar] [CrossRef]
- Sahebkar, A.; Simental-Mendía, L.E.; Watts, G.F.; Serban, M.C.; Banach, M.; Lipid and Blood Pressure Meta-Analysis Collaboration (LBPMC) Group. Comparison of the effects of fibrates versus statins on plasma lipoprotein(a) concentrations: A systematic review and meta-analysis of head-to-head randomized controlled trials. BMC Med. 2017, 15, 22. [Google Scholar] [CrossRef]
- Melenovsky, V.; Malik, J.; Wichterle, D.; Simek, J.; Pisarikova, A.; Skrha, J.; Poledne, R.; Stavek, P.; Ceska, R. Comparison of the effects of atorvastatin or fenofibrate on nonlipid biochemical risk factors and the LDL particle size in subjects with combined hyperlipidemia. Am. Heart J. 2002, 144, E6. [Google Scholar] [CrossRef]
- Vavvas, D.G.; Daniels, A.B.; Kapsala, Z.G.; Goldfarb, J.W.; Ganotakis, E.; Loewenstein, J.I.; Young, L.H.; Gragoudas, E.S.; Eliott, D.; Kim, I.K.; et al. Regression of Some High-risk Features of Age-related Macular Degeneration (AMD) in Patients Receiving Intensive Statin Treatment. EBioMedicine 2016, 5, 198–203. [Google Scholar] [CrossRef] [PubMed]


| Variables | Patients with Hyperlipidemia (2001–2010) | p Value a | p Value b | ||
|---|---|---|---|---|---|
| Receive Statins/Fibrates (Study Group I) | Not Receive Statins/Fibrates (Study Group II) | Comparison Group | |||
| N = 15,482 | N = 15,482 | N = 61,928 | |||
| Age, years (mean ± SD) | 61.74 ± 8.76 | 61.74 ± 8.76 | 61.74 ± 8.76 | 0.9928 | 0.9908 |
| Sex/male (n, %) | 6817 (44.03) | 6817 (44.03) | 27,268 (44.03) | 1 | 1 |
| Hypertension | 11,586 (74.84) | 9372 (60.53) | 20,342 (32.85) | <0.0001 | <0.0001 |
| Diabetes mellitus | 6662 (43.03) | 5451 (35.21) | 6220 (10.04) | <0.0001 | <0.0001 |
| Cerebrovascular disease | 1989 (12.85) | 1368 (8.84) | 3433 (5.54) | <0.0001 | <0.0001 |
| Coronary artery disease | 4902 (31.66) | 3792 (24.49) | 7505 (12.12) | <0.0001 | <0.0001 |
| Heart failure | 1330 (8.59) | 964 (6.23) | 2707 (4.37) | <0.0001 | <0.0001 |
| Atrial fibrillation | 291 (1.88) | 246 (1.59) | 734 (1.19) | 0.0501 | <0.0001 |
| Myocardial infarction | 270 (1.74) | 110 (0.71) | 281 (0.45) | <0.0001 | <0.0001 |
| Atherosclerosis | 688 (4.44) | 584 (3.77) | 993 (1.60) | 0.0029 | <0.0001 |
| Stroke | 3219 (20.79) | 2415 (15.60) | 6100 (9.85) | <0.0001 | <0.0001 |
| Peripheral vascular disease | 750 (4.84) | 623 (4.02) | 1370 (2.21) | 0.0005 | <0.0001 |
| Glaucoma | 1083 (7.0) | 963 (6.22) | 2582 (4.17) | 0.006 | <0.0001 |
| Diabetic retinopathy | 794 (5.13) | 433 (2.80) | 534 (0.86) | <0.0001 | <0.0001 |
| Cataract surgery | 1421 (9.28) | 1021 (6.59) | 3485 (5.63) | <0.0001 | <0.0001 |
| Obesity | 172 (1.11) | 149 (0.96) | 90 (0.15) | 0.1969 | <0.0001 |
| Tobacco use disorder, alcohol abuse | 243 (1.57) | 227 (1.47) | 669 (1.08) | 0.4571 | <0.0001 |
| Aspirin | 7352 (47.49) | 5305 (34.27) | 12,107 (19.55) | <0.0001 | <0.0001 |
| Warfarin | 7206 (46.54) | 5175 (33.43) | 11,804 (19.06) | <0.0001 | <0.0001 |
| Hormone replacement therapy | 701 (4.53) | 734 (4.74) | 1731 (2.80) | 0.3724 | <0.0001 |
| NSAID | 14,766 (95.38) | 14,661 (94.70) | 56,485 (91.21) | 0.006 | <0.0001 |
| Antihypertensive agents | 5895 (38.08) | 5116 (33.04) | 15,404 (24.87) | <0.0001 | <0.0001 |
| Results | Patients with Hyperlipidemia | ||
|---|---|---|---|
| Receive Statins/Fibrates (Study Group I) | Not Receive Statins/Fibrates (Study Group II) | Comparison Group | |
| N = 15,482 | N = 15,482 | N = 61,928 | |
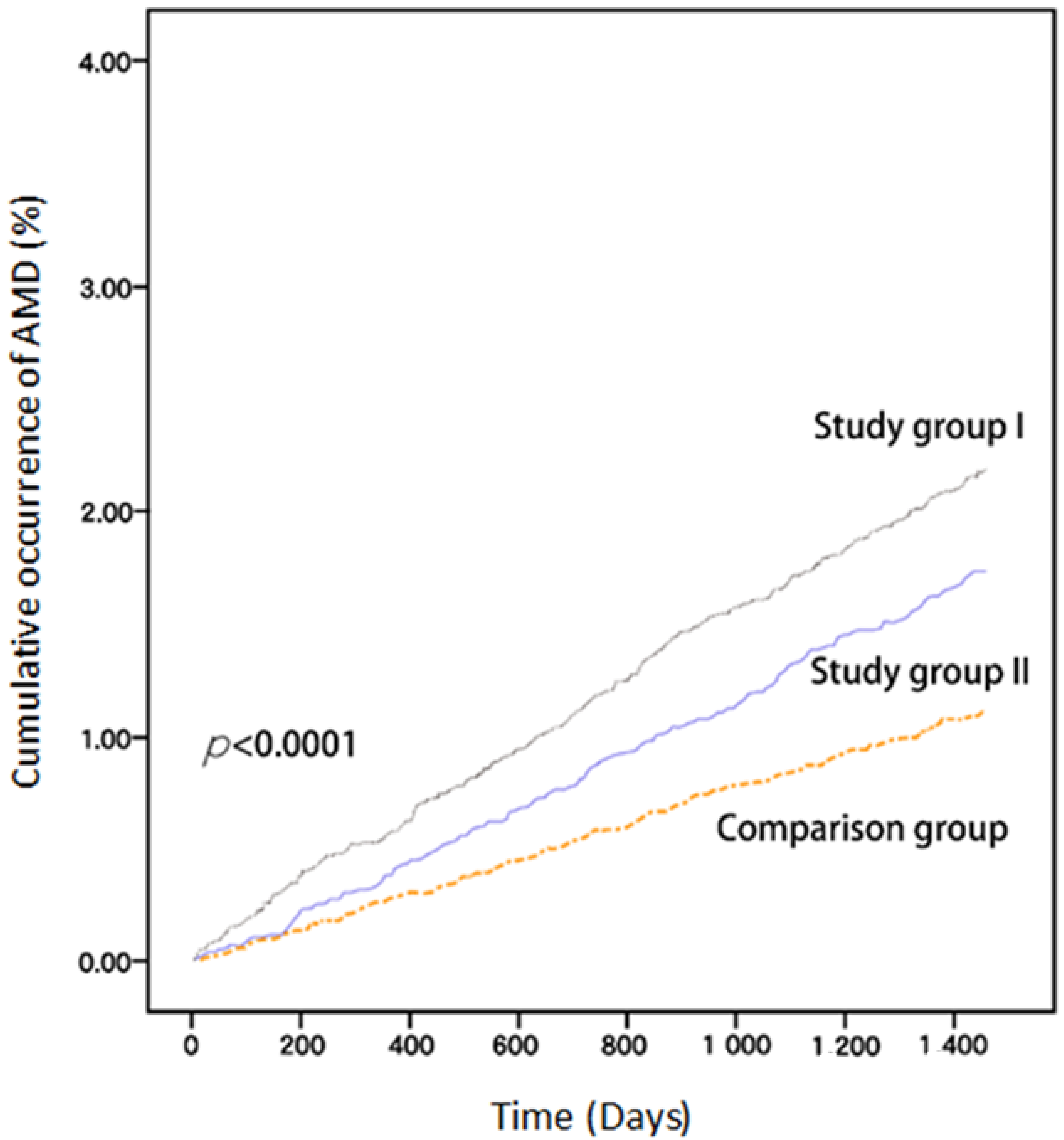
| AMD cases (n, %) | 338 (2.18) | 268 (1.73) | 692 (1.12) |
| Crude HR (95% CI) | 1.27 (1.08–1.48) ** | 1 | - |
| Adjusted HR (95% CI) | 1.23 (1.04–1.45) * | 1 | - |
| Crude HR (95% CI) | - | 1.56 (1.35–1.79) *** | 1 |
| Adjusted HR (95% CI) | - | 1.40 (1.20–1.63) *** | 1 |
| Results | Receive Statins/Fibrates (Study Group I) | Not Receive Statins/Fibrates (Study Group II) | |
|---|---|---|---|
| Fibrates Only | Statins Only | ||
| N = 1492 | N = 10,364 | N = 15,482 | |
| AMD cases (n, %) | 47 (3.15) | 228 (2.20) | 268 (1.73) |
| Crude HR (95% CI) | 1.84 (1.35–2.51) ** | 1.28 (1.07–1.52) ** | 1 |
| Adjusted HR (95% CI) | 1.76 (1.29–2.41) ** | 1.23 (1.03–1.47) ** | 1 |
| Crude HR (95% CI) | 1.44 (1.05–1.97) * | 1 | - |
| Adjusted HR (95% CI) | 1.42 (1.04–1.96) * | 1 | - |
| Study Group I | ≤360 DDD | 361–720 DDD | ≥721 DDD | Study Group II |
|---|---|---|---|---|
| N = 7678 | N = 3768 | N = 4036 | N = 15,482 | |
| AMD cases (n, %) | 266 (3.46) | 50 (1.33) | 22 (0.05) | 268 (1.73) |
| Crude HR (95% CI) | 2.02 (1.71–2.40) *** | 0.76 (0.57–1.03) | 0.31 (0.20–0.48) *** | 1 |
| Adjusted HR (95% CI) | 1.87 (1.57–2.22) *** | 0.80 (0.59–1.08) | 0.34 (0.22–0.53) *** | 1 |
| Fibrates only | ≤360 DDD | 361–720 DDD | ≥721 DDD | Study group II |
| N = 1132 | N = 224 | N = 136 | N = 15,482 | |
| AMD cases (n, %) | 33 (2.91) | 7 (3.12) | 7 (5.14) | 268 (1.73) |
| Crude HR (95% CI) | 1.70 (1.18–2.44) ** | 1.83 (0.86–3.87) | 3.05 (1.44–6.47) *** | 1 |
| Adjusted HR (95% CI) | 1.60 (1.11–2.31) * | 1.77 (0.83–3.76) | 3.43 (1.61–7.30) ** | 1 |
| Statins only | ≤360 DDD | 361–720 DDD | ≥721 DDD | Study group II |
| N = 6791 | N = 2327 | N = 1246 | N = 15,482 | |
| AMD cases (n, %) | 185 (2.72) | 32 (1.37) | 11 (0.88) | 268 (1.73) |
| Crude HR (95% CI) | 1.58 (1.31–1.91) *** | 0.79 (0.55–1.14) | 0.51 (0.28–0.93) * | 1 |
| Adjusted HR (95% CI) | 1.49 (1.24–1.81) *** | 0.82 (0.57–1.19) | 0.56 (0.31–1.03) | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, C.-H.; Lin, H.-C.; Lin, H.-L.; Keller, J.J.; Wang, L.-H. Association between Antihyperlipidemic Agent Use and Age-Related Macular Degeneration in Patients with Hyperlipidemia: A Population-Based Retrospective Cohort Study. Biomedicines 2023, 11, 1508. https://doi.org/10.3390/biomedicines11061508
Chen C-H, Lin H-C, Lin H-L, Keller JJ, Wang L-H. Association between Antihyperlipidemic Agent Use and Age-Related Macular Degeneration in Patients with Hyperlipidemia: A Population-Based Retrospective Cohort Study. Biomedicines. 2023; 11(6):1508. https://doi.org/10.3390/biomedicines11061508
Chicago/Turabian StyleChen, Chun-Hao, Hsiu-Chen Lin, Hsiu-Li Lin, Joseph Jordan Keller, and Li-Hsuan Wang. 2023. "Association between Antihyperlipidemic Agent Use and Age-Related Macular Degeneration in Patients with Hyperlipidemia: A Population-Based Retrospective Cohort Study" Biomedicines 11, no. 6: 1508. https://doi.org/10.3390/biomedicines11061508
APA StyleChen, C. -H., Lin, H. -C., Lin, H. -L., Keller, J. J., & Wang, L. -H. (2023). Association between Antihyperlipidemic Agent Use and Age-Related Macular Degeneration in Patients with Hyperlipidemia: A Population-Based Retrospective Cohort Study. Biomedicines, 11(6), 1508. https://doi.org/10.3390/biomedicines11061508