
Alveolar Ridge Augmentation with a Novel Combination of 3D-Printed Scaffolds and Adipose-Derived Mesenchymal Stem Cells—A Pilot Study in Pigs
 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Scaffold
2.2. Animals
2.3. Equipment and Surgical Items
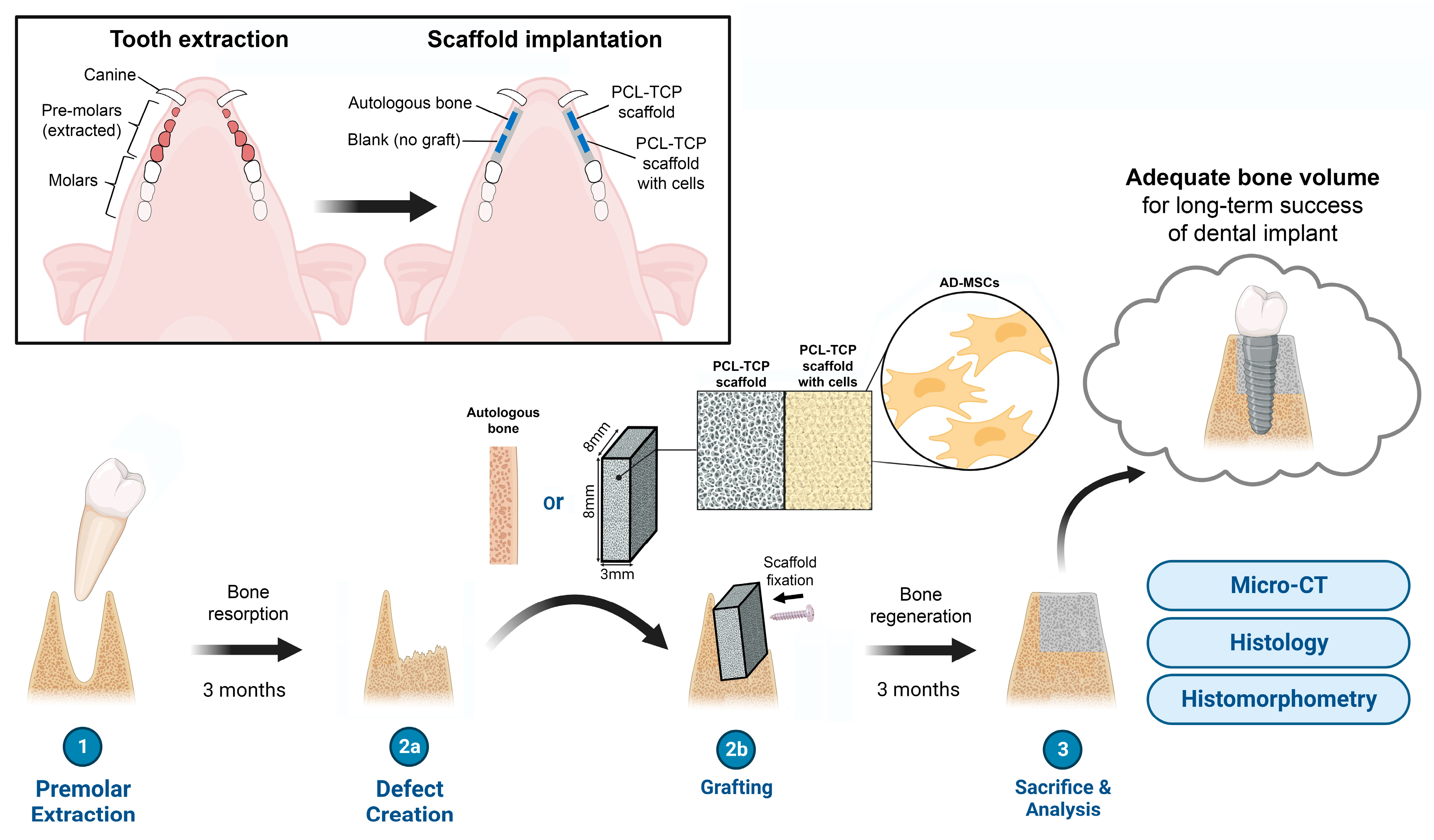
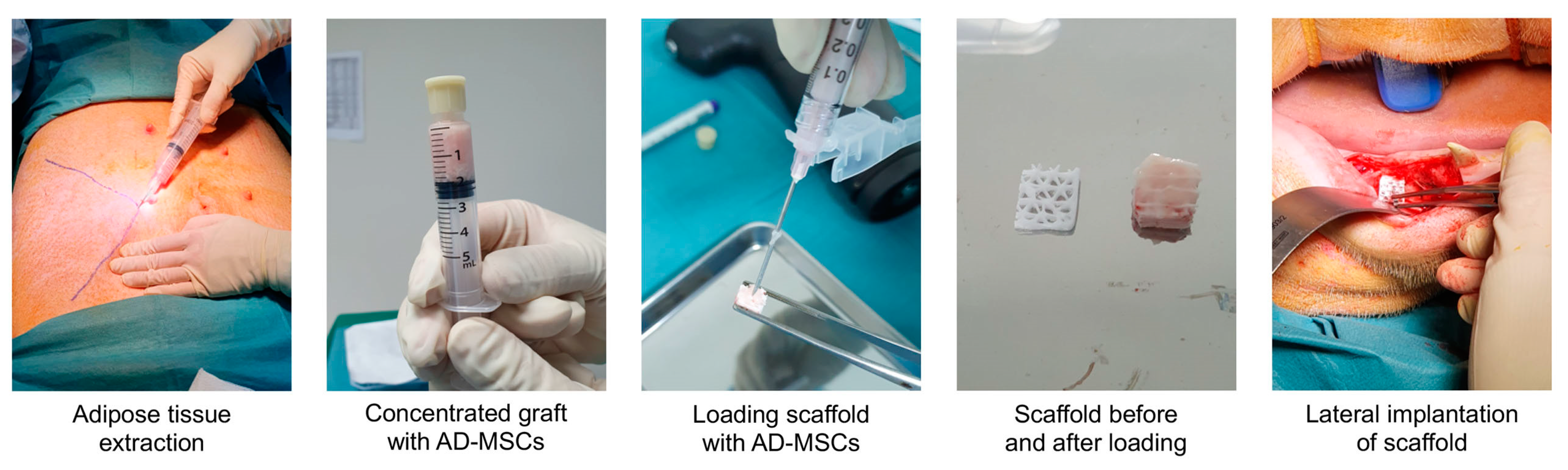
2.4. Surgery
2.5. Micro-Computed Tomography and Histology
2.6. Statistical Analysis
3. Results
3.1. Clinical Observations
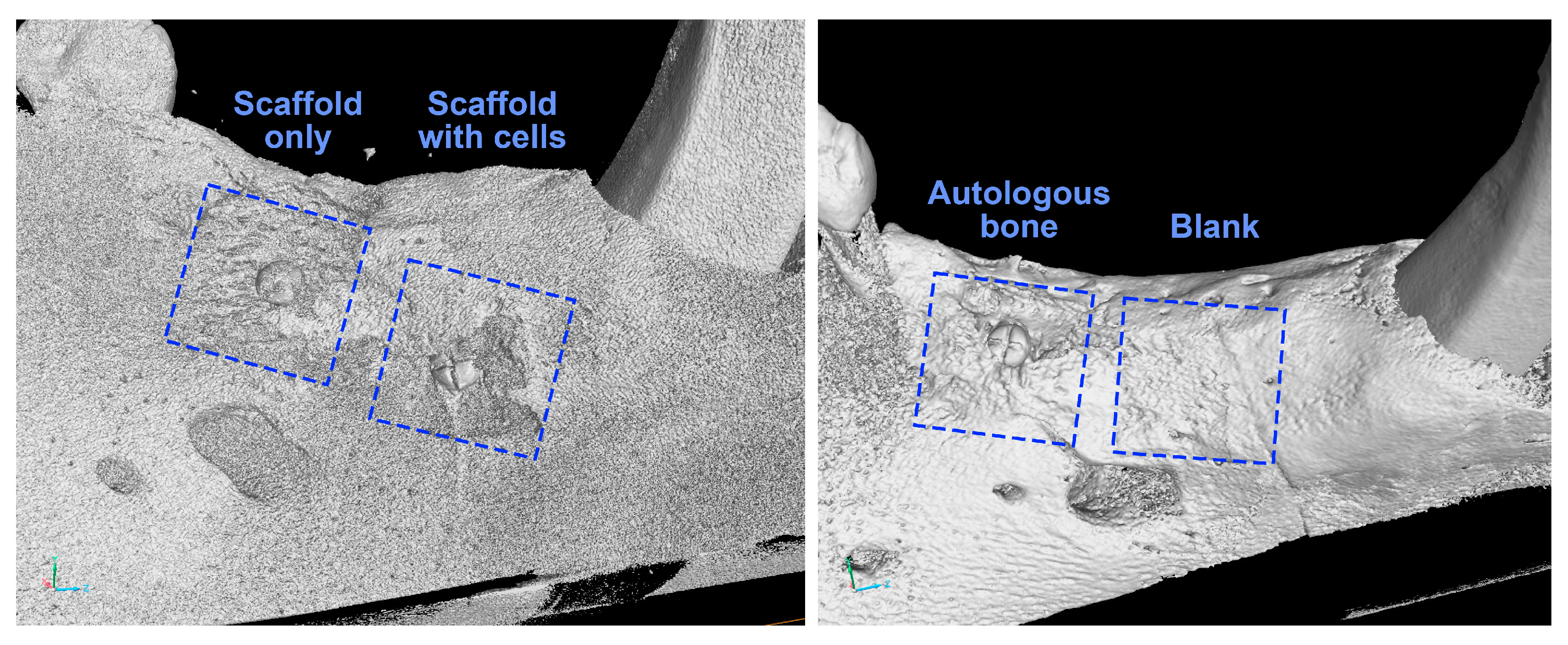
3.2. Visual Analysis of 3D Model
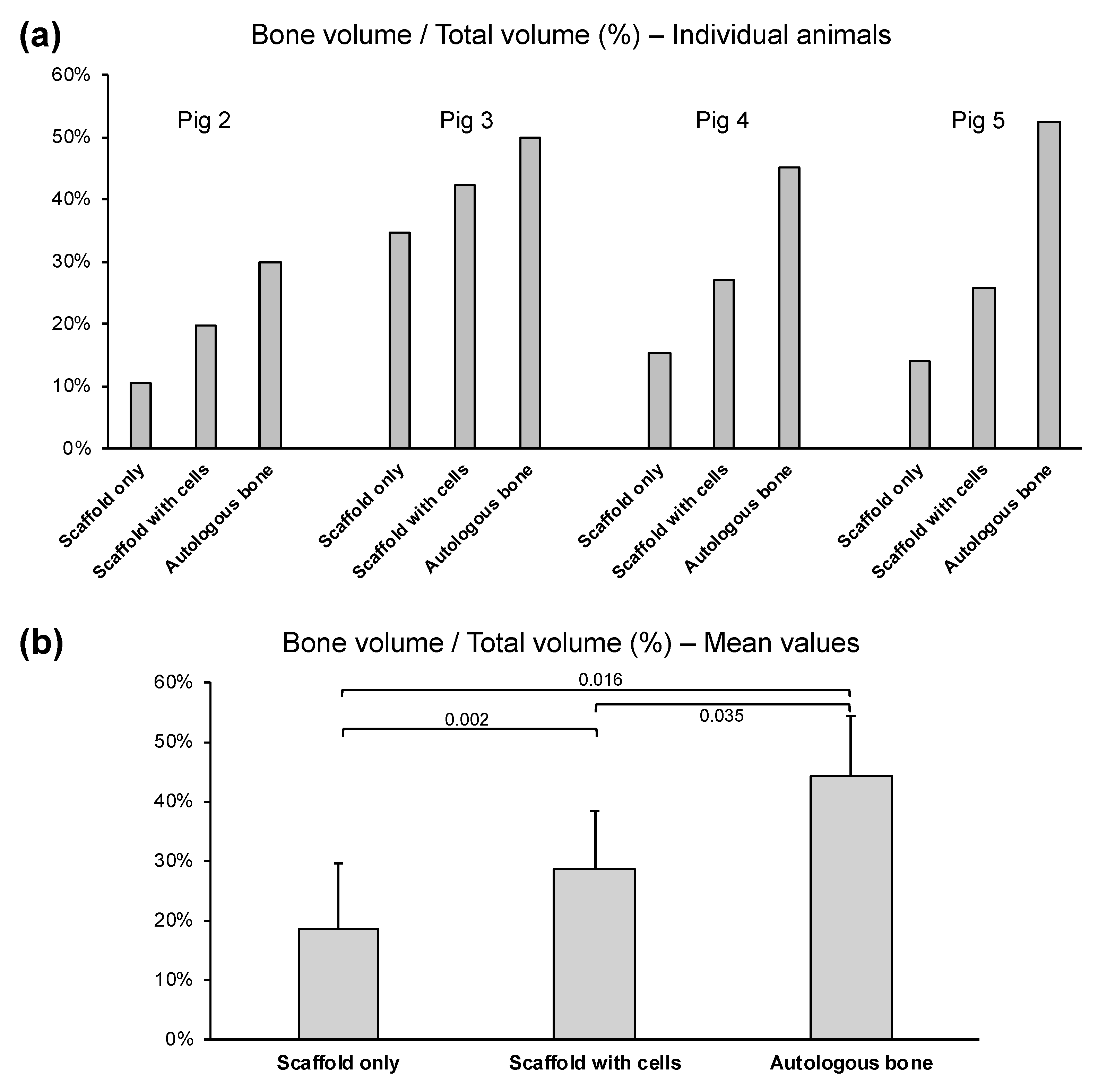
3.3. Quantitative µCT Analysis
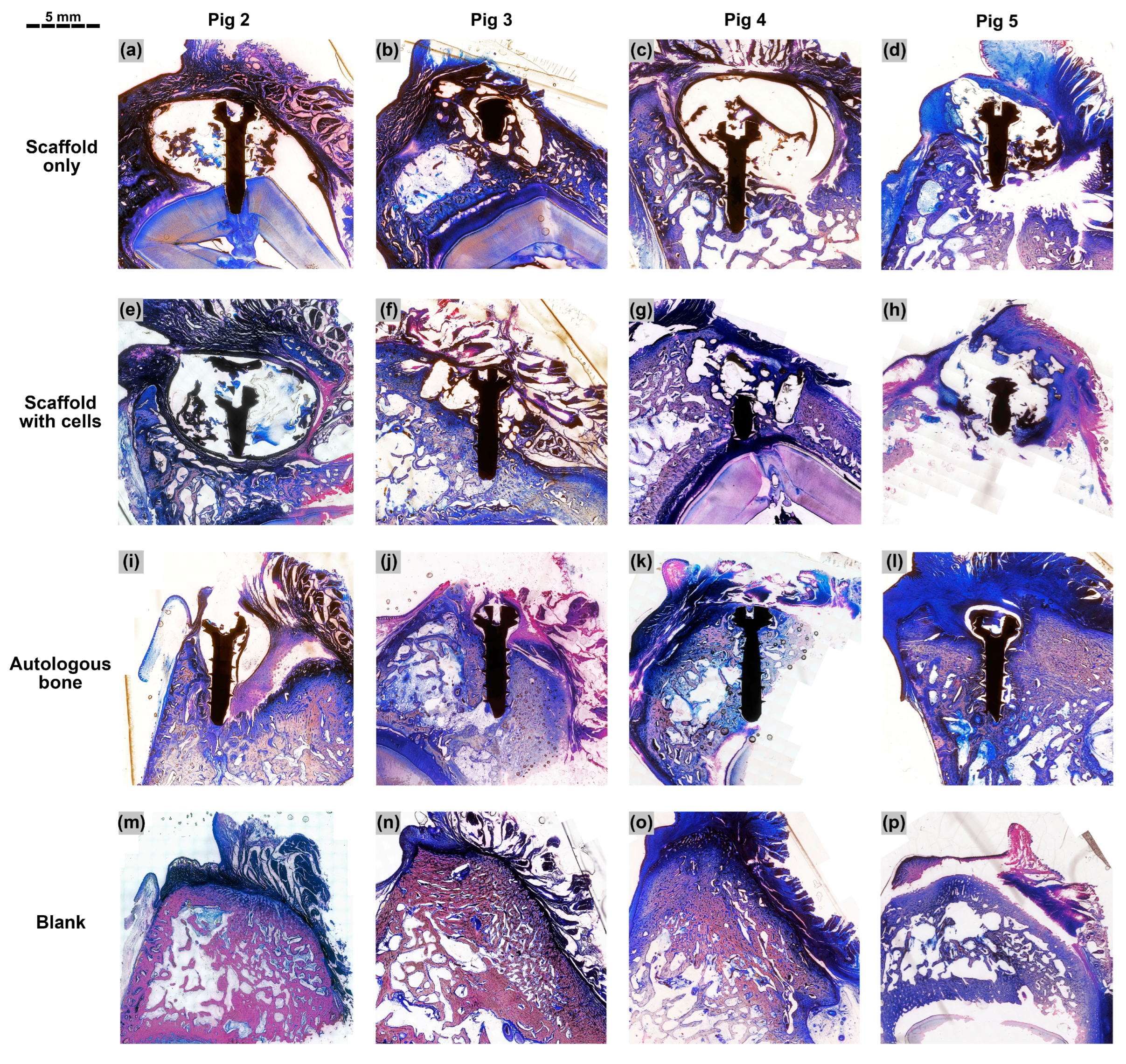
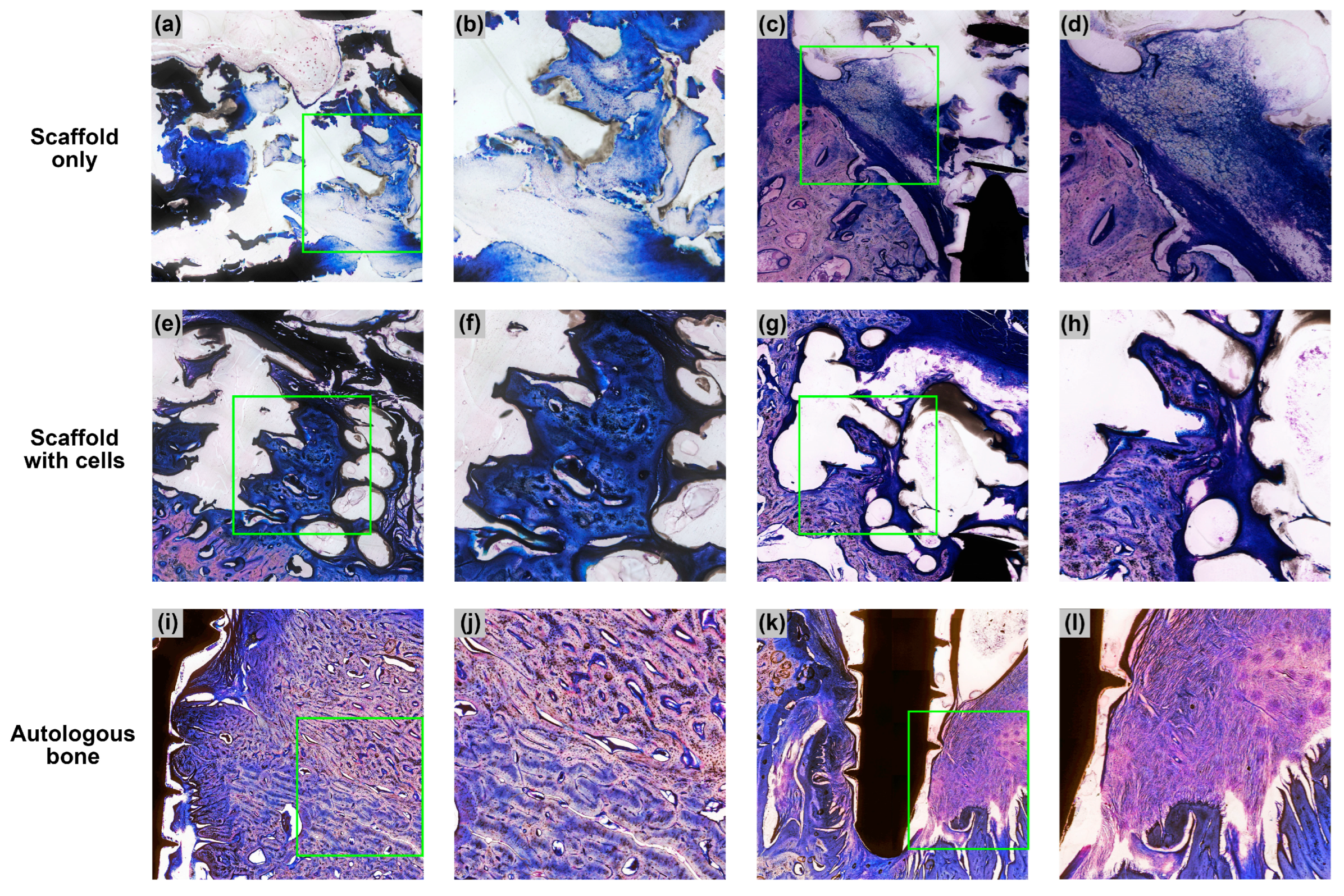
3.4. Descriptive Histology
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Paul, N.; Jyotsna, S.; Keshini, M.P. Alveolar Ridge Augmentation Using Autogenous Bone Graft and Platelet-Rich Fibrin to Facilitate Implant Placement. Contemp. Clin. Dent. 2022, 13, 90–94. [Google Scholar] [CrossRef]
- Tan, W.L.; Wong, T.L.T.; Wong, M.C.M.; Lang, N.P. A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. Clin. Oral Implant. Res. 2011, 23, 1–21. [Google Scholar] [CrossRef]
- Shin, S.Y.; Shin, S.I.; Kye, S.B.; Chang, S.W.; Hong, J.; Paeng, J.Y.; Yang, S.M. Bone cement grafting increases implant primary stability in circumferential cortical bone defects. J. Periodontal Implant. Sci. 2015, 45, 30–35. [Google Scholar] [CrossRef]
- Kim, Y.K.; Ku, J.K. Ridge augmentation in implant dentistry. J. Korean Assoc. Oral Maxillofac. Surg. 2020, 46, 211–217. [Google Scholar] [CrossRef]
- Sakkas, A.; Wilde, F.; Heufelder, M.; Winter, K.; Schramm, A. Autogenous bone grafts in oral implantology-is it still a “gold standard”? A consecutive review of 279 patients with 456 clinical procedures. Int. J. Implant. Dent. 2017, 3, 23. [Google Scholar] [CrossRef]
- Wang, W.; Yeung, K.W.K. Bone grafts and biomaterials substitutes for bone defect repair: A review. Bioact. Mater. 2017, 2, 224–247. [Google Scholar] [CrossRef]
- Rodriguez, A.E.; Nowzari, H. The long-term risks and complications of bovine-derived xenografts: A case series. J. Indian Soc. Periodontol. 2019, 23, 487–492. [Google Scholar] [CrossRef]
- Diaz-Rodriguez, P.; López-Álvarez, M.; Serra, J.; González, P.; Landín, M. Current Stage of Marine Ceramic Grafts for 3D Bone Tissue Regeneration. Mar. Drugs 2019, 17, 471. [Google Scholar] [CrossRef]
- Grawish, M.E.; Grawish, L.M.; Grawish, H.M.; Grawish, M.M.; Holiel, A.A.; Sultan, N.; El-Negoly, S.A. Demineralized Dentin Matrix for Dental and Alveolar Bone Tissues Regeneration: An Innovative Scope Review. Tissue Eng. Regen. Med. 2022, 19, 687–701. [Google Scholar] [CrossRef]
- Memè, L.; Strappa, E.M.; Monterubbianesi, R.; Bambini, F.; Mummolo, S. SEM and FT-MIR Analysis of Human Demineralized Dentin Matrix: An In Vitro Study. Appl. Sci. 2022, 12, 1480. [Google Scholar] [CrossRef]
- Battafarano, G.; Rossi, M.; De Martino, V.; Marampon, F.; Borro, L.; Secinaro, A.; Del Fattore, A. Strategies for Bone Regeneration: From Graft to Tissue Engineering. Int. J. Mol. Sci. 2021, 22, 1128. [Google Scholar] [CrossRef]
- Zhao, R.; Yang, R.; Cooper, P.R.; Khurshid, Z.; Shavandi, A.; Ratnayake, J. Bone Grafts and Substitutes in Dentistry: A Review of Current Trends and Developments. Molecules 2021, 26, 3007. [Google Scholar] [CrossRef]
- Pitt, G.; Gratzl, M.; Kimmel, G.; Surles, J.; Sohindler, A. Aliphatic polyesters II. The degradation of poly (DL-lactide), poly (epsilon-caprolactone), and their copolymers in vivo. Biomaterials 1981, 2, 215–220. [Google Scholar] [CrossRef]
- Bezwada, R.S.; Jamiolkowski, D.D.; Lee, I.-Y.; Agarwal, V.; Persivale, J.; Trenka-Benthin, S.; Erneta, M.; Suryadevara, J.; Yang, A.; Liu, S. Monocryl suture, a new ultra-pliable absorbable monofilament suture. Biomaterials 1995, 16, 1141–1148. [Google Scholar] [CrossRef]
- Darney, P.D.; Monroe, S.E.; Klaisle, C.M.; Alvarado, A. Clinical evaluation of the Capronor contraceptive implant: Preliminary report. Am. J. Obstet. Gynecol. 1989, 160, 1292–1295. [Google Scholar] [CrossRef]
- Middleton, J.C.; Tipton, A.J. Synthetic biodegradable polymers as orthopedic devices. Biomaterials 2000, 21, 2335–2346. [Google Scholar] [CrossRef]
- Hutmacher, D.W. Scaffolds in tissue engineering bone and cartilage. Biomaterials 2000, 21, 2529–2543. [Google Scholar] [CrossRef]
- Zein, I.; Hutmacher, D.W.; Tan, K.C.; Teoh, S.H. Fused deposition modeling of novel scaffold architectures for tissue engineering applications. Biomaterials 2002, 23, 1169–1185. [Google Scholar] [CrossRef]
- Schantz, J.T.; Lim, T.C.; Ning, C.; Teoh, S.H.; Tan, K.C.; Wang, S.C.; Hutmacher, D.W. Cranioplasty after trephination using a novel biodegradable burr hole cover: Technical case report. Neurosurgery 2006, 58, ONS-E176, discussion ONS-E176. [Google Scholar] [CrossRef]
- Low, S.W.; Ng, Y.J.; Yeo, T.T.; Chou, N. Use of Osteoplug polycaprolactone implants as novel burr-hole covers. Singap. Med. J. 2009, 50, 777–780. [Google Scholar]
- Bao, C.; Chong, M.S.K.; Qin, L.; Fan, Y.; Teo, E.Y.; Sandikin, D.; Choolani, M.; Chan, J.K.Y. Effects of tricalcium phosphate in polycaprolactone scaffold for mesenchymal stem cell-based bone tissue engineering. Mater. Technol. 2019, 34, 361–367. [Google Scholar] [CrossRef]
- Rai, B.; Ho, K.H.; Lei, Y.; Si-Hoe, K.-M.; Jeremy Teo, C.-M.; Yacob, K.b.; Chen, F.; Ng, F.-C.; Teoh, S.H. Polycaprolactone-20% Tricalcium Phosphate Scaffolds in Combination with Platelet-Rich Plasma for the Treatment of Critical-Sized Defects of the Mandible: A Pilot Study. J. Oral Maxillofac. Surg. 2007, 65, 2195–2205. [Google Scholar] [CrossRef]
- Rai, B.; Teoh, S.H.; Ho, K.H.; Hutmacher, D.W.; Cao, T.; Chen, F.; Yacob, K. The effect of rhBMP-2 on canine osteoblasts seeded onto 3D bioactive polycaprolactone scaffolds. Biomaterials 2004, 25, 5499–5506. [Google Scholar] [CrossRef]
- Goh, B.T.; Teh, L.Y.; Tan, D.B.; Zhang, Z.; Teoh, S.H. Novel 3D polycaprolactone scaffold for ridge preservation—A pilot randomised controlled clinical trial. Clin. Oral. Implants Res. 2015, 26, 271–277. [Google Scholar] [CrossRef]
- Goh, B.T.; Chanchareonsook, N.; Tideman, H.; Teoh, S.H.; Chow, J.K.F.; Jansen, J.A. The use of a polycaprolactone-tricalcium phosphate scaffold for bone regeneration of tooth socket facial wall defects and simultaneous immediate dental implant placement in Macaca fascicularis. J. Biomed. Mater. Res. Part A 2013, 102, 1379–1388. [Google Scholar] [CrossRef]
- Chanchareonsook, N.; Tideman, H.; Feinberg, S.E.; Jongpaiboonkit, L.; Lee, S.; Flanagan, C.; Krishnaswamy, G.; Jansen, J. Segmental mandibular bone reconstruction with a carbonate-substituted hydroxyapatite-coated modular endoprosthetic poly(ɛ-caprolactone) scaffold in Macaca fascicularis. J. Biomed. Mater. Research. Part B Appl. Biomater. 2014, 102, 962–976. [Google Scholar] [CrossRef]
- Matichescu, A.; Ardelean, L.C.; Rusu, L.C.; Craciun, D.; Bratu, E.A.; Babucea, M.; Leretter, M. Advanced Biomaterials and Techniques for Oral Tissue Engineering and Regeneration—A Review. Materials 2020, 13, 5303. [Google Scholar] [CrossRef]
- Matsuura, T.; Tokutomi, K.; Sasaki, M.; Katafuchi, M.; Mizumachi, E.; Sato, H. Distinct characteristics of mandibular bone collagen relative to long bone collagen: Relevance to clinical dentistry. BioMed Res. Int. 2014, 2014, 769414. [Google Scholar] [CrossRef]
- Tsuji, W.; Rubin, J.P.; Marra, K.G. Adipose-derived stem cells: Implications in tissue regeneration. World J. Stem Cells 2014, 6, 312–321. [Google Scholar] [CrossRef]
- Alexander, R.; Harrell, D. Autologous fat grafting: Use of closed syringe microcannula system for enhanced autologous structural grafting. Clin. Cosmet. Investig. Dermatol. 2013, 6, 91–102. [Google Scholar] [CrossRef]
- Han, S.; Sun, H.M.; Hwang, K.C.; Kim, S.W. Adipose-Derived Stromal Vascular Fraction Cells: Update on Clinical Utility and Efficacy. Crit. Rev. Eukaryot. Gene Expr. 2015, 25, 145–152. [Google Scholar] [CrossRef]
- Alexander, R.W. Understanding Adipose-Derived Stromal Vascular Fraction (AD-SVF) Cell Biology and Use on the Basis of Cellular, Chemical, Structural, and Paracrine Components: A Concise Review. J. Prolotherapy 2012, 4, 855–869. [Google Scholar]
- Alexander, R.W. Use of Microcannula Closed Syringe System for Safe and Effective Lipoaspiration and Small Volume Autologous Fat Grafting. Am. J. Cosmet. Surg. 2013, 30, 94–104. [Google Scholar] [CrossRef]
- Lau, C.S.; Chua, J.; Pena, E.M.; Lim, J.; Saigo, L.; Goh, B.T. A Porcine Model Using Adipose Stem Cell-Loaded Scaffolds for Alveolar Ridge Augmentation. Tissue Eng. Part C Methods 2022, 28, 228–237. [Google Scholar] [CrossRef] [PubMed]
- Bose, S.; Roy, M.; Bandyopadhyay, A. Recent advances in bone tissue engineering scaffolds. Trends Biotechnol. 2012, 30, 546–554. [Google Scholar] [CrossRef]
- Shrivats, A.R.; McDermott, M.C.; Hollinger, J.O. Bone tissue engineering: State of the union. Drug Discov. Today 2014, 19, 781–786. [Google Scholar] [CrossRef]
- Rai, B.; Oest, M.E.; Dupont, K.M.; Ho, K.H.; Teoh, S.H.; Guldberg, R.E. Combination of platelet-rich plasma with polycaprolactone-tricalcium phosphate scaffolds for segmental bone defect repair. J. Biomed. Mater. Res. Part A 2007, 81A, 888–899. [Google Scholar] [CrossRef]
- Le, B.Q.; Rai, B.; Hui Lim, Z.X.; Tan, T.C.; Lin, T.; Lin Lee, J.J.; Murali, S.; Teoh, S.H.; Nurcombe, V.; Cool, S.M. A polycaprolactone-β-tricalcium phosphate–heparan sulphate device for cranioplasty. J. Cranio-Maxillofac. Surg. 2019, 47, 341–348. [Google Scholar] [CrossRef]
- Yeo, A.; Wong, W.J.; Teoh, S.-H. Surface modification of PCL-TCP scaffolds in rabbit calvaria defects: Evaluation of scaffold degradation profile, biomechanical properties and bone healing patterns. J. Biomed. Mater. Res. Part A 2010, 93A, 1358–1367. [Google Scholar] [CrossRef]
- Khojasteh, A.; Behnia, H.; Hosseini, F.S.; Dehghan, M.M.; Abbasnia, P.; Abbas, F.M. The effect of PCL-TCP scaffold loaded with mesenchymal stem cells on vertical bone augmentation in dog mandible: A preliminary report. J. Biomed. Mater. Res. Part B Appl. Biomater. 2013, 101B, 848–854. [Google Scholar] [CrossRef] [PubMed]
- Yeo, A.; Cheok, C.; Teoh, S.H.; Zhang, Z.Y.; Buser, D.; Bosshardt, D.D. Lateral ridge augmentation using a PCL-TCP scaffold in a clinically relevant but challenging micropig model. Clin. Oral. Implants Res. 2012, 23, 1322–1332. [Google Scholar] [CrossRef] [PubMed]
- Morais, J.M.; Papadimitrakopoulos, F.; Burgess, D.J. Biomaterials/tissue interactions: Possible solutions to overcome foreign body response. AAPS J. 2010, 12, 188–196. [Google Scholar] [CrossRef]
- Kantarci, A. Biological Basis of Periodontal Regeneration. Dent. Clin. N. Am. 2022, 66, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Wang, Y.; Gou, W.; Lu, Q.; Peng, J.; Lu, S. Role of mesenchymal stem cells in bone regeneration and fracture repair: A review. Int. Orthop. 2013, 37, 2491–2498. [Google Scholar] [CrossRef]
- Strioga, M.; Viswanathan, S.; Darinskas, A.; Slaby, O.; Michalek, J. Same or not the same? Comparison of adipose tissue-derived versus bone marrow-derived mesenchymal stem and stromal cells. Stem Cells Dev. 2012, 21, 2724–2752. [Google Scholar] [CrossRef]
- Liao, H.T.; Chen, C.T. Osteogenic potential: Comparison between bone marrow and adipose-derived mesenchymal stem cells. World J. Stem Cells 2014, 6, 288–295. [Google Scholar] [CrossRef]
- Stolzing, A.; Jones, E.; McGonagle, D.; Scutt, A. Age-related changes in human bone marrow-derived mesenchymal stem cells: Consequences for cell therapies. Mech. Ageing Dev. 2008, 129, 163–173. [Google Scholar] [CrossRef]
- Zuk, P.A.; Zhu, M.; Mizuno, H.; Huang, J.; Futrell, J.W.; Katz, A.J.; Benhaim, P.; Lorenz, H.P.; Hedrick, M.H. Multilineage cells from human adipose tissue: Implications for cell-based therapies. Tissue Eng. 2001, 7, 211–228. [Google Scholar] [CrossRef]
- Zuk, P.A.; Zhu, M.; Ashjian, P.; De Ugarte, D.A.; Huang, J.I.; Mizuno, H.; Alfonso, Z.C.; Fraser, J.K.; Benhaim, P.; Hedrick, M.H. Human adipose tissue is a source of multipotent stem cells. Mol. Biol. Cell 2002, 13, 4279–4295. [Google Scholar] [CrossRef]
- Halvorsen, Y.C.; Wilkison, W.O.; Gimble, J.M. Adipose-derived stromal cells--their utility and potential in bone formation. Int. J. Obes. Relat. Metab. Disord. 2000, 24 (Suppl. 4), S41–S44. [Google Scholar] [CrossRef]
- Russell, K.A.; Chow, N.H.; Dukoff, D.; Gibson, T.W.; LaMarre, J.; Betts, D.H.; Koch, T.G. Characterization and Immunomodulatory Effects of Canine Adipose Tissue- and Bone Marrow-Derived Mesenchymal Stromal Cells. PLoS ONE 2016, 11, e0167442. [Google Scholar] [CrossRef]
- Mohamed-Ahmed, S.; Fristad, I.; Lie, S.A.; Suliman, S.; Mustafa, K.; Vindenes, H.; Idris, S.B. Adipose-derived and bone marrow mesenchymal stem cells: A donor-matched comparison. Stem Cell Res. Ther. 2018, 9, 168. [Google Scholar] [CrossRef] [PubMed]
- Cowan, C.M.; Shi, Y.Y.; Aalami, O.O.; Chou, Y.F.; Mari, C.; Thomas, R.; Quarto, N.; Contag, C.H.; Wu, B.; Longaker, M.T. Adipose-derived adult stromal cells heal critical-size mouse calvarial defects. Nat. Biotechnol. 2004, 22, 560–567. [Google Scholar] [CrossRef]
- Hicok, K.C.; Du Laney, T.V.; Zhou, Y.S.; Halvorsen, Y.D.; Hitt, D.C.; Cooper, L.F.; Gimble, J.M. Human adipose-derived adult stem cells produce osteoid in vivo. Tissue Eng. 2004, 10, 371–380. [Google Scholar] [CrossRef]
- Cui, L.; Liu, B.; Liu, G.; Zhang, W.; Cen, L.; Sun, J.; Yin, S.; Liu, W.; Cao, Y. Repair of cranial bone defects with adipose derived stem cells and coral scaffold in a canine model. Biomaterials 2007, 28, 5477–5486. [Google Scholar] [CrossRef] [PubMed]
- Leong, D.T.; Khor, W.M.; Chew, F.T.; Lim, T.C.; Hutmacher, D.W. Characterization of osteogenically induced adipose tissue-derived precursor cells in 2-dimensional and 3-dimensional environments. Cells Tissues Organs 2006, 182, 1–11. [Google Scholar] [CrossRef]
- Leong, D.T.; Abraham, M.C.; Rath, S.N.; Lim, T.C.; Chew, F.T.; Hutmacher, D.W. Investigating the effects of preinduction on human adipose-derived precursor cells in an athymic rat model. Differ. Res. Biol. Divers. 2006, 74, 519–529. [Google Scholar] [CrossRef] [PubMed]
- Trivisonno, A.; Alexander, R.W.; Baldari, S.; Cohen, S.R.; Di Rocco, G.; Gentile, P.; Magalon, G.; Magalon, J.; Miller, R.B.; Womack, H.; et al. Intraoperative Strategies for Minimal Manipulation of Autologous Adipose Tissue for Cell- and Tissue-Based Therapies: Concise Review. Stem Cells Transl. Med. 2019, 8, 1265–1271. [Google Scholar] [CrossRef]
- Turner, L.G. Federal Regulatory Oversight of US Clinics Marketing Adipose-Derived Autologous Stem Cell Interventions: Insights from 3 New FDA Draft Guidance Documents. Mayo Clin. Proc. 2015, 90, 567–571. [Google Scholar] [CrossRef] [PubMed]
- Raposio, E.; Ciliberti, R. Clinical use of adipose-derived stem cells: European legislative issues. Ann. Med. Surg. 2017, 24, 61–64. [Google Scholar] [CrossRef]
- Simonacci, F.; Bertozzi, N.; Raposio, E. Off-label use of adipose-derived stem cells. Ann. Med. Surg. 2017, 24, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Pilgaard, L.; Lund, P.; Rasmussen, J.G.; Fink, T.; Zachar, V. Comparative analysis of highly defined proteases for the isolation of adipose tissue-derived stem cells. Regen. Med. 2008, 3, 705–715. [Google Scholar] [CrossRef]
- Aronowitz, J.A.; Lockhart, R.A.; Hakakian, C.S. Mechanical versus enzymatic isolation of stromal vascular fraction cells from adipose tissue. SpringerPlus 2015, 4, 713. [Google Scholar] [CrossRef]
- Condé-Green, A.; Kotamarti, V.S.; Sherman, L.S.; Keith, J.D.; Lee, E.S.; Granick, M.S.; Rameshwar, P. Shift toward Mechanical Isolation of Adipose-derived Stromal Vascular Fraction: Review of Upcoming Techniques. Plast. Reconstr. Surgery. Glob. Open 2016, 4, e1017. [Google Scholar] [CrossRef]
- Alexander, R.W. Biocellular Regenerative Medicine: Use of Adipose-Derived Stem/Stromal Cells and It's Native Bioactive Matrix. Phys. Med. Rehabil. Clin. N. Am. 2016, 27, 871–891. [Google Scholar] [CrossRef] [PubMed]
- Melief, S.M.; Zwaginga, J.J.; Fibbe, W.E.; Roelofs, H. Adipose tissue-derived multipotent stromal cells have a higher immunomodulatory capacity than their bone marrow-derived counterparts. Stem Cells Transl. Med. 2013, 2, 455–463. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Animal | Efficacy Ratio | |
|---|---|---|
| Scaffold Only | Scaffold with Cells | |
| Pig 2 | 0.35 | 0.65 |
| Pig 3 | 0.70 | 0.85 |
| Pig 4 | 0.34 | 0.60 |
| Pig 5 | 0.27 | 0.49 |
| Mean ± standard deviation | 0.41 ± 0.19 | 0.65 ± 0.15 |
| Animal | Surgery Location | Study Duration | Sample | BV% | Reference |
|---|---|---|---|---|---|
| Pig | Alveolar ridge | 3 months | PCL-TCP only | 18.6% | This study |
| PCL-TCP + ADMSC | 28.7% | ||||
| Autologous bone | 43.7% | ||||
| Rat | Femur | 12 weeks | PCL-TCP only | 4.2% | [37] |
| PCL-TCP + PRP * | 4.6% | ||||
| Rat | Calvaria | 12 weeks | PCL-TCP–fibrin | 23.7% | [38] |
| PCL-TCP–fibrin-HS3 * | 38.6% | ||||
| Rabbit | Calvaria | 12 weeks | PCL-TCP only | 18.3 mm3 ** | [39] |
| NaOH-treated PCL-TCP * | 21.5 mm3 ** | ||||
| Dog | Mandible | 8 weeks | PCL-TCP only | 17.3% | [40] |
| PCL-TCP + BMMSC * | 48.6% | ||||
| Micropig | Alveolar ridge | 6 months | PCL-TCP only | 18.0% | [41] |
| Autologous bone | 51.5% | ||||
| Monkey | Mandible | 6 months | PCL-TCP only | 6.8% *** | [25] |
| Autologous bone | 11.8% *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lau, C.S.; Chua, J.; Prasadh, S.; Lim, J.; Saigo, L.; Goh, B.T. Alveolar Ridge Augmentation with a Novel Combination of 3D-Printed Scaffolds and Adipose-Derived Mesenchymal Stem Cells—A Pilot Study in Pigs. Biomedicines 2023, 11, 2274. https://doi.org/10.3390/biomedicines11082274
Lau CS, Chua J, Prasadh S, Lim J, Saigo L, Goh BT. Alveolar Ridge Augmentation with a Novel Combination of 3D-Printed Scaffolds and Adipose-Derived Mesenchymal Stem Cells—A Pilot Study in Pigs. Biomedicines. 2023; 11(8):2274. https://doi.org/10.3390/biomedicines11082274
Chicago/Turabian StyleLau, Chau Sang, Jasper Chua, Somasundaram Prasadh, Jing Lim, Leonardo Saigo, and Bee Tin Goh. 2023. "Alveolar Ridge Augmentation with a Novel Combination of 3D-Printed Scaffolds and Adipose-Derived Mesenchymal Stem Cells—A Pilot Study in Pigs" Biomedicines 11, no. 8: 2274. https://doi.org/10.3390/biomedicines11082274
APA StyleLau, C. S., Chua, J., Prasadh, S., Lim, J., Saigo, L., & Goh, B. T. (2023). Alveolar Ridge Augmentation with a Novel Combination of 3D-Printed Scaffolds and Adipose-Derived Mesenchymal Stem Cells—A Pilot Study in Pigs. Biomedicines, 11(8), 2274. https://doi.org/10.3390/biomedicines11082274