Stem Cell Surgery and Growth Factors in Retinitis Pigmentosa Patients: Pilot Study after Literature Review



Abstract
:1. Introduction
2. Materials and Methods
- Clinical diagnosis of RP based on a history of night blindness, visual field constriction, abnormalities on ERG testing, and specific ophthalmoscopic findings;
- Age ranging from 19 to 86 years;
- Normal intraocular pressure;
- Visual acuity for near (close-up) vision between 7 and 64 points (pts) in order to avoid difficult evaluations for both low visus (>64 pts) and normal visus (6 pts);
- Transparent lens;
- Signature of the informed consent;
- Retinitis pigmentosa pattern that can be detected at the macula.
- Hypermetropy or myopia with spherical equivalent ≥6 diopters;
- Existence of keratoconus, cataract, cystoid macular edema, keratitis, uveitis, etc.;
- Other ocular diseases, for example, glaucoma, optic neuritis, ocular trauma, etc.;
- Lack of patient compliance due to medical conditions, such as Parkinson’s disease, diabetes mellitus, hypertension, vasculitis, hypovitaminosis, multiple sclerosis, epilepsy, or other systemic acute or chronic diseases.
Statistical Analysis
3. Results
4. Discussion
- (1)
- (2)
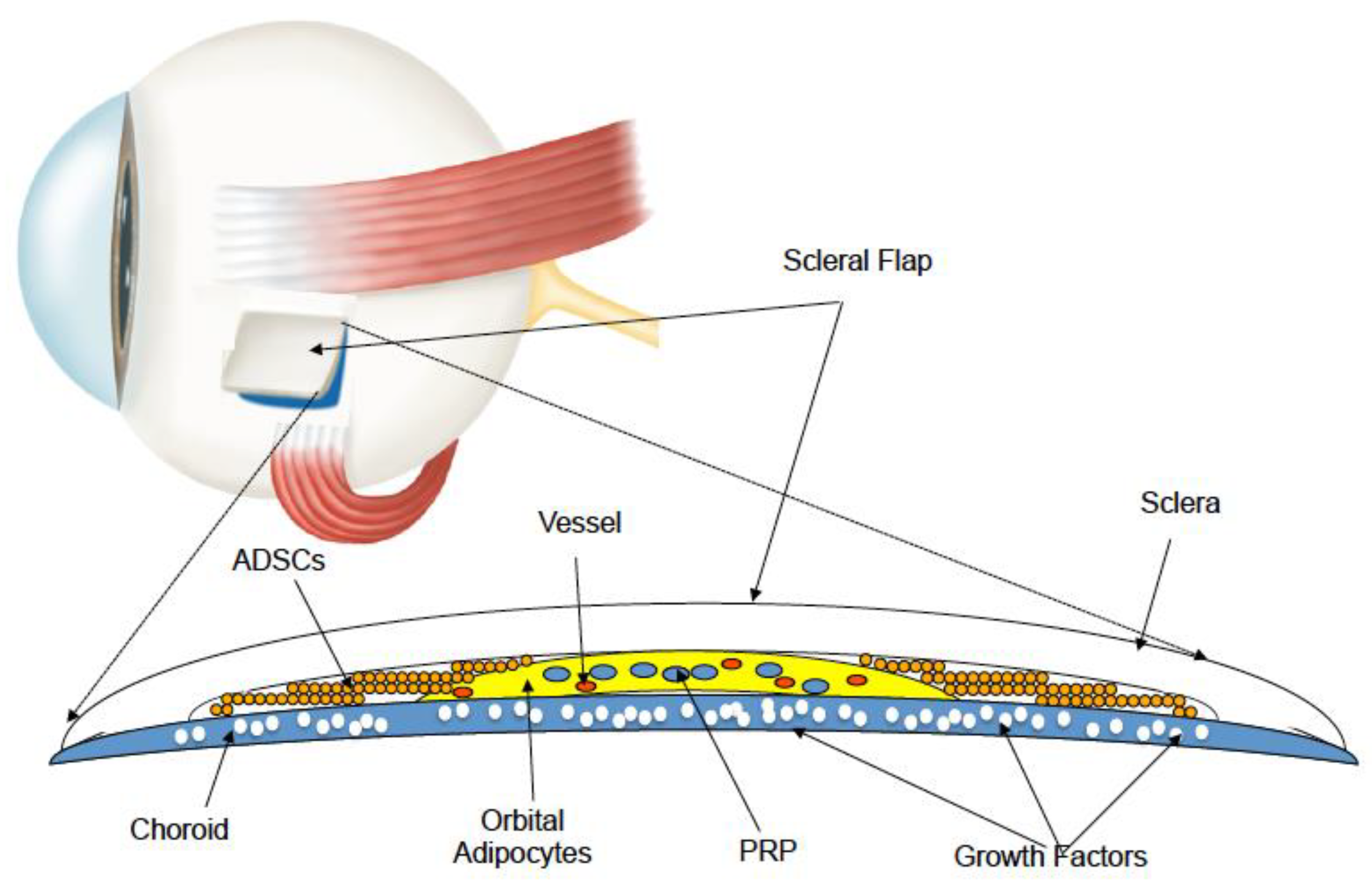
- ADSCs secrete bFGF, vascular endothelial GF (VEGF), granulocyte-macrophage colony-stimulating factor (GM-CSF), macrophage colony-stimulating factor (M-CSF), TGF, hepatocyte GF, IGF-1, IL, angiogenin, placental GF (PlGF), ciliary neurotrophic factor (CNTF), and brain-derived neurotrophic factor (BDNF) [39,40].
- (1)
- A greater number of patients and operated eyes with homogeneous age range;
- (2)
- Longitudinal studies to evaluate the longevity of the grafted tissue;
- (3)
- Biomolecular studies to understand the paracrine increment of the autograft;
- (4)
- Genetic tests obtained from patients to allow differentiation in homogeneous research groups, as genetic diagnosis will surely become more relevant in coming years, and it will be possible to determine the impact of MSC administration on different genetic groups of RP patients;
- (5)
- Evaluation of the suitable time in which the autograft must be performed in order to avoid failure in the presence of markedly degenerated retinal tissue. In particular, the results of this study show that FT might be considered a prognostic criterion for RP patients undergoing treatment by LRRT.
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ADSCs | Adipose tissue-derived stem cells |
| Aµm2 | Average of retinal thickness in micron meters |
| BCVA | Best corrected visual acuity |
| BCEA | Bivariate contour ellipse area |
| BDNF | Brain-derived neurotrophic factor |
| bFGF | Basic fibroblast growth factor |
| Cµm | Thickness of central fovea in micron meters |
| CNTF | Ciliary neurotrophic factor |
| dB | DeciBel |
| EGF | Epidermal growth factor |
| ERG | Electroretinogram |
| ESCs | Embryonic stem cells |
| ETDRS | Early treatment diabetic retinopathy study charts at 4 meters in logMAR |
| FT | Foveal thickness |
| GF | Growth factor |
| IGF-1 | Insulin-like growth factor-1 |
| IL | Interleukin |
| IFN-β | Interferon-β |
| logMAR | Logarithm of the minimum angle of resolution |
| iPSCs | Induced pluripotent stem cells |
| ISCEV | International Society for Clinical Electrophysiology of Vision |
| LRRT | Limoli retinal restoration technique |
| MSCs | Mesenchimal stem cells |
| MY | Microperimetry |
| OCT | Optical coherence tomography |
| PDAF | Platelet-derived angiogenesis factor |
| PDGF | Platelet-derived growth factor |
| PEDF | Pigment epithelium-derived factor |
| PlGF | Placental growth factor |
| PLTs | Platelets |
| PRP | Platelet rich plasma |
| pts | Points or print size |
| RdCVF | Rod–cone viability factor |
| RGC | Retinal ganglion cell |
| ROS | Reactive 13 oxygen species |
| RP | Retinitis pigmentosa |
| RPE | Retinal pigment epithelium |
| SD-OCT | Spectral domain optical coherence tomography |
| SVF | Stromal vascular fraction |
| TGF | Transforming growth factor |
| T0; T180 | Time at baseline; time at 6 months after surgery |
| VEGF | Vascular endothelial growth factor |
References
- Hartong, D.T.; Berson, E.L.; Dryja, T.P. Retinitis pigmentosa. Lancet 2006, 368, 1795–1809. [Google Scholar] [CrossRef]
- Hamel, C. Retinitis pigmentosa. Orphanet J. Rare Dis. 2006, 1, 40. [Google Scholar] [CrossRef]
- Birch, D.G.; Anderson, J.L.; Fish, G.E. Yearly rates of rod and cone functional loss in retinitis pigmentosa and cone-rod dystrophy. Ophthalmology 1999, 106, 258–268. [Google Scholar] [CrossRef]
- Pagon, R.A. Retinitis pigmentosa. Surv. Ophthalmol. 1988, 33, 137–177. [Google Scholar] [CrossRef]
- Campochiaro, P.A.; Mir, T.A. The mechanism of cone cell death in retinitis pigmentosa. Prog. Retin. Eye Res. 2018, 62, 24–37. [Google Scholar] [CrossRef] [PubMed]
- Grover, S.; Fishman, G.A.; Alexander, K.R.; Anderson, R.J.; Derlacki, D.J. Visual acuity impairment in patients with retinitis pigmentosa. Ophthalmology 1996, 103, 1593–1600. [Google Scholar] [CrossRef]
- McCulloch, D.L.; Marmor, M.F.; Brigell, M.G.; Hamilton, R.; Holder, G.E.; Tzekov, R.; Bach, M. ISCEV Standard for full-field clinical electroretinography. Doc. Ophthalmol. 2015, 130, 1–12. [Google Scholar] [CrossRef]
- Liu, G.; Liu, X.; Li, H.; Du, Q.; Wang, F. Optical coherence tomographic analysis of retina in retinitis pigmentosa patients. Ophthalmic Res. 2016, 56, 111–122. [Google Scholar] [CrossRef]
- Leveillard, T.; Mohand-Said, S.; Lorentz, O.; Hicks, D.; Fintz, A.C.; Clerin, E.; Simonutti, M.; Forster, V.; Cavusoglu, N.; Chalmel, F.; et al. Identification and characterization of rod-derived cone viability factor. Nat. Genet. 2004, 36, 755–759. [Google Scholar] [CrossRef]
- Smith, L.E.H. Bone marrow–derived stem cells preserve cone vision in retinitis pigmentosa. J. Clin. Investig. 2004, 114, 755–757. [Google Scholar] [CrossRef]
- Uteza, Y.; Rouillot, J.S.; Kobetz, A.; Marchant, D.; Pecqueur, S.; Arnaud, E.; Prats, H.; Honiger, J.; Dufier, J.L.; Abitbol, M.; et al. Intravitreous transplantation of encapsulated fibroblasts secreting the human fibroblast growthfactor 2 delays photoreceptor cell degeneration in Royal College of surgeons rats. Proc. Natl. Acad. Sci. USA 1999, 96, 3126–3131. [Google Scholar] [CrossRef] [PubMed]
- McGee Sanftner, L.H.; Abel, H.; Hauswirth, W.W.; Flannery, J.G. Glial cell line derived neurotrophic factor delays photoreceptor degeneration in a transgenic rat model of retinitis pigmentosa. Mol. Ther. 2001, 4, 622–629. [Google Scholar] [CrossRef] [PubMed]
- Bonfiglio, V.; Reibaldi, M.; Fallico, M.; Russo, A.; Pizzo, A.; Fichera, S.; Rapisarda, C.; Macchi, I.; Avitabile, T.; Longo, A. Widening use of dexamethasone implant for the treatment of macular edema. Drug Des. Dev. Ther. 2017, 11, 2359–2372. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.K.; Lu, B.; Girman, S.; Wang, S. Cell-based therapeutic strategies for replacement and preservation in retinal degenerative diseases. Prog. Retin. Eye Res. 2017, 58, 1–27. [Google Scholar] [CrossRef]
- Otani, A.; Dorrell, M.I.; Kinder, K.; Moreno, S.K.; Nusinowitz, S.; Banin, E.; Heckenlively, J.; Friedlander, M. Rescue of retinal degeneration by intravitreally injected adult bone marrow–derived lineage-negative hematopoietic stem cells. J. Clin. Investig. 2004, 114, 765–774. [Google Scholar] [CrossRef]
- Liang, F.Q.; Aleman, T.S.; Dejneka, N.S.; Dudus, L.; Fisher, K.J.; Maguire, A.M.; Jacobson, S.G.; Bennett, J. Long-term protection of retinal structure but not function using RAAV. CNTF in animal models of retinitis pigmentosa. Mol. Ther. 2001, 4, 461–472. [Google Scholar] [CrossRef]
- Guadagni, V.; Novelli, E.; Strettoi, E. Environmental enrichment reduces photoreceptor degeneration and retinal inflammation in a mouse model of retinitis pigmentosa. Investig. Ophthalmol. Vis. Sci. 2015, 56, 4261. [Google Scholar]
- Idelson, M.; Alper, R.; Obolensky, A.; Ben-Shushan, E.; Hemo, I.; Yachimovich-Cohen, N.; Khaner, H.; Smith, Y.; Wiser, O.; Gropp, M.; et al. Directed differentiation of human embryonic stem cells into functional retinal pigment epithelium cells. Cell Stem. Cell. 2009, 5, 396–408. [Google Scholar] [CrossRef]
- Klassen, H. Stem cells in clinical trials for treatment of retinal degeneration. Expert Opin. Biol. Ther. 2015, 16, 7–14. [Google Scholar] [CrossRef]
- Takahashi, K.; Yamanaka, S. Induced pluripotent stem cells in medicine and biology. Development 2013, 140, 2457–2461. [Google Scholar] [CrossRef]
- Ding, S.L.S.; Kumar, S.; Mok, P.L. Cellular reparative mechanisms of mesenchymal stem cells for retinal diseases. Int. J. Mol. Sci. 2017, 18, 1406. [Google Scholar] [CrossRef] [PubMed]
- Romanov, Y.A.; Darevskaya, A.N.; Merzlikina, N.V.; Buravkova, L.B. Mesenchymal stem cells from human bone marrow and adipose tissue: Isolation, characterization, and differentiation potentialities. Bull. Exp. Biol. Med. 2005, 140, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Lindroos, B.; Suuronen, R.; Miettinen, S. The potential of adipose stem cells in regenerative medicine. Stem Cell Rev. Rep. 2011, 7, 269–291. [Google Scholar] [CrossRef] [PubMed]
- Baddour, J.A.; Sousounis, K.; Tsonis, P.A. Organ repair and regeneration: An overview. Birth Defects Res. C 2012, 96, 1–29. [Google Scholar] [CrossRef] [PubMed]
- Kawamura, A.; Miyagawa, S.; Fukushima, S.; Kawamura, T.; Kashiyama, N.; Ito, E.; Masuda, S.; Toda, K.; Hatazawa, J.; Morii, E.; et al. Teratocarcinomas arising from allogeneic induced pluripotent stem cell-derived cardiac tissue constructs provoked host immune rejection in mice. Sci. Rep. 2016, 6, 19464. [Google Scholar] [CrossRef]
- Itakura, G.; Kobayashi, Y.; Nishimura, S.; Iwai, H.; Takano, M.; Iwanami, A.; Toyama, Y.; Okano, H.; Nakamura, M. Controlling immune rejection is a fail-safe system against potential tumorigenicity after human iPSC-derived neural stem cell transplantation. PLoS ONE 2015, 10, e0116413. [Google Scholar] [CrossRef]
- Rezanejad, H.; Soheili, Z.S.; Haddad, F.; Matin, M.M.; Samiei, S.; Manafi, A.; Ahmadieh, H. In vitro differentiation of adipose-tissue-derived mesenchymal stem cells into neural retinal cells through expression of human PAX6 (5a) gene. Cell Tissue Res. 2014, 356, 65–75. [Google Scholar] [CrossRef]
- Cui, Y.; Xu, N.; Xu, W.; Xu, G. Mesenchymal stem cells attenuate hydrogen peroxide-induced oxidative stress and enhance neuroprotective effects in retinal ganglion cells. Vitr. Cell Dev. Biol. Anim. 2016, 53, 328–335. [Google Scholar] [CrossRef]
- Kim, K.S.; Park, J.M.; Kong, T.H.; Kim, C.; Bae, S.H.; Kim, H.W.; Moon, J. Retinal angiogenesis effects of TGF-ß1 and paracrine factors secreted from human placental stem cells in response to a pathological environment. Cell Transplant. 2016, 25, 1145–1157. [Google Scholar] [CrossRef]
- Zhao, P.T.; Zhang, L.J.; Shao, H.; Bai, L.L.; Yu, B.; Su, C.; Dong, L.J.; Liu, X.; Li, X.R.; Zhang, X.M. Therapeutic effects of mesenchymal stem cells administered at later phase of recurrent experimental autoimmune uveitis. Int. J. Ophthalmol. 2016, 9, 1381–1389. [Google Scholar]
- Limoli, P.G.; Vingolo, E.M.; Limoli, C.; Scalinci, S.Z.; Nebbioso, M. Regenerative therapy by suprachoroidal cell autograft in dry age-related macular degeneration: Preliminary in vivo report. J. Vis. Exp. 2018, 132, 56469. [Google Scholar] [CrossRef] [PubMed]
- Limoli, P.G.; Vingolo, E.M.; Morales, M.U.; Nebbioso, M.; Limoli, C. Preliminary study on electrophysiological changes after cellular autograft in age-related macular degeneration. Medicine 2014, 93, 355. [Google Scholar] [CrossRef] [PubMed]
- Limoli, P.G.; Limoli, C.; Vingolo, E.M.; Scalinci, S.Z.; Nebbioso, M. Cell surgery and growth factors in dry age-related macular degeneration: Visual prognosis and morphological study. Oncotarget 2016, 7, 46913–46923. [Google Scholar] [CrossRef] [Green Version]
- Limoli, P.G.; Carpi, R.; Tassi, F.; Vingolo, E.M.; D’Amato, L.M.; Giacomotti, E.; Solari, R.; Di Corato, R. Prognostic standard in growth factors teraphy. Investig. Ophthalmol. Vis. Sci. 2012, 53, 277. [Google Scholar]
- Bakondi, B.; Girman, S.; Lu, B.; Wang, S. Multimodal delivery of isogenic mesenchymal stem cells yields synergistic protection from retinal degeneration and vision loss. Stem Cells Transl. Med. 2017, 6, 444–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, P.; Mariman, E.; Renes, J.; Keijer, J. The secretory function of adipocytes in the physiology of white adipose tissue. J. Cell Physiol. 2008, 216, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Trayhurn, P.; Beattie, J.H. Physiological role of adipose tissue: White adipose tissue as an endocrine and secretory organ. Proc. Nutr. Soc. 2001, 60, 329–339. [Google Scholar] [CrossRef] [Green Version]
- Tilg, H.; Moschen, A. Adipocytokines: Mediators linking adipose tissue, inflammation and immunity. Nat. Rev. Immunol. 2006, 6, 772–783. [Google Scholar] [CrossRef]
- Schaffler, A.; Buchler, C. Concise review: Adipose tissue-derived stromal cells-basic and clinical implications for novel cell-based therapies. Stem Cells 2007, 25, 818–882. [Google Scholar] [CrossRef]
- Mizuno, H. Adipose-derived stem cells for tissue repair and regeneration: Ten years of research and a literature review. J. Nippon Med. Sch. 2009, 76, 56–66. [Google Scholar] [CrossRef] [Green Version]
- Anitua, E.; Andia, I.; Ardanza, B.; Nurden, P.; Nurden, A.T. Autologous platelets as a source of proteins for healing and tissue regeneration. Thromb. Haemost. 2004, 91, 4–15. [Google Scholar] [CrossRef] [PubMed]
- Qureshi, A.H.; Chaoji, V.; Maiguel, D.; Faridi, M.H.; Barth, C.J.; Salem, S.M.; Singhal, M.; Stoub, D.; Krastins, B.; Ogihara, M.; et al. Proteomic and phospho-proteomic profile of human platelets in basal, resting state: Insights into integrin signaling. PLoS ONE. 2009, 4, e7627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Limoli, P. (Ed.) The retinal cell-neuroregeneration. Principles, applications and perspectives. In Limoli Retina Regeneration Tecnique; FGE Reg. San Giovanni 40: Canelli, Italy, 2014; pp. 159–206. [Google Scholar]
- Garcia, T.B.; Hollborn, M.; Bringmann, A. Expression and signaling of NGF in the healthy and injured retina. Cytokine Growth Factor Rev. 2017, 34, 43–57. [Google Scholar] [CrossRef] [PubMed]
- Kalucka, J.; Missiaen, R.; Georgiadou, M.; Schoors, S.; Lange, C.; De Bock, K.; Dewerchin, M.; Carmeliet, P. Metabolic control of the cell cycle. Cell Cycle 2015, 14, 3379–3388. [Google Scholar] [CrossRef] [Green Version]
- Mahmoudifar, N.; Doran, P.M. Mesenchymal stem cells derived from human adipose tissue. Methods Mol. Biol. 2015, 1340, 53–64. [Google Scholar] [CrossRef]
- Mou, S.; Zhou, M.; Li, Y.; Wang, J.; Yuan, Q.; Xiao, P.; Sun, J.; Wang, Z. Extracellular vesicles from human adipose derived stem cells for the improvement of angiogenesis and fat grafting application. Plast. Reconstr. Surg. 2019, 144, 869–880. [Google Scholar] [CrossRef]
- Yu, D.Y.; Cringle, S.J. Retinal degeneration and local oxygen metabolism. Exp. Eye Res. 2005, 80, 745–751. [Google Scholar] [CrossRef]
- Punzo, C.; Xiong, W.; Cepko, C.L. Loss of daylight vision in retinal degeneration: Are oxidative stress and metabolic dysregulation to blame? J. Biol. Chem. 2012, 287, 1642–1648. [Google Scholar] [CrossRef] [Green Version]
- Campochiaro, P.A.; Strauss, R.W.; Lu, L.; Hafiz, G.; Wolfson, Y.; Shah, S.M.; Sophie, R.; Mir, T.A.; Scholl, H.P. Is there excess oxidative stress and damage in eyes of patients with retinitis pigmentosa? Antioxid. Redox Signal. 2015, 23, 643–648. [Google Scholar] [CrossRef] [Green Version]
- Yamada, H.; Yamada, E.; Ando, A.; Esumi, N.; Bora, N.; Saikia, J.; Sung, C.H.; Zack, D.J.; Campochiaro, P.A. Fibroblast growth factor-2 decreases hyperoxia-induced photoreceptor cell death in mice. Am. J. Pathol. 2001, 159, 1113–1120. [Google Scholar] [CrossRef] [Green Version]
- Okoye, G.; Zimmer, J.; Sung, J.; Gehlbach, P.; Deering, T.; Nambu, H.; Hackett, S.; Melia, M.; Esumi, N.; Zack, D.J.; et al. Increased expression of brain-derived neurotrophic factor preserves retinal function and slows cell death from rhodopsin mutation or oxidative damage. J. Neurosci. 2003, 23, 4164–4172. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Mohand-Said, S.; Danan, A.; Simonutti, M.; Fontaine, V.; Clerin, E.; Picaud, S.; Léveillard, T.; Sahel, J.A. Functional cone rescue by RdCVF protein in a dominant model of retinitis pigmentosa. Mol. Ther. 2009, 17, 787–795. [Google Scholar] [CrossRef] [PubMed]
- Aït-Ali, N.; Fridlich, R.; Millet-Puel, G.; Clérin, E.; Delalande, F.; Jaillard, C.; Blond, F.; Perrocheau, L.; Reichman, S.; Byrne, L.C.; et al. Rod-derived cone viability factor promotes cone survival by stimulating aerobic glycolysis. Cell 2015, 161, 817–832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Byrne, L.C.; Dalkara, D.; Luna, G.; Fisher, S.K.; Clerin, E.; Sahel, J.A.; Leveillard, T.; Flannery, J.G. Viral-mediated RdCVF and RdCVFL expression protects cone and rod photoreceptors in retinal degeneration. J. Clin. Investig. 2015, 125, 105–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, N.; Brown, K.E.; Milam, A.H. Activated microglia in human retinitis pigmentosa, late-onset retinal degeneration, and age related macular degeneration. Exp. Eye Res. 2003, 76, 463–471. [Google Scholar] [CrossRef]
- Zeng, H.Y.; Zhu, X.A.; Zhang, C.; Yang, L.P.; Wu, L.M.; Tso, M.O.M. Identification of sequential events and factors associated with microglial activation, migration, and cytotoxicity in retinal degeneration in rd mice. Investig. Ophthalmol. Vis. Sci. 2005, 46, 2992–2999. [Google Scholar] [CrossRef] [Green Version]
- Morohoshi, K.; Goodwin, A.M.; Ohbayashi, M.; Ono, S.J. Autoimmunity in retinal degeneration: Autoimmune retinopathy and age related macular degeneration. J. Autoimmun. 2009, 33, 247–254. [Google Scholar] [CrossRef]
- Nagineni, C.N.; Samuel, W.; Nagineni, S.; Pardhasaradhi, K.; Wiggert, B.; Detrick, B.; Hooks, J.J. Transforming growth factor-beta induces expression of vascular endothelial growth factor in human retinal pigment epithelial cells: Involvement of mitogen-activated protein kinases. J. Cell Physiol. 2003, 197, 453–462. [Google Scholar] [CrossRef]
- Nagineni, C.N.; Kutty, V.; Detrick, B.; Hooks, J.J. Expression of PDGF and their receptors in human retinal pigment epithelial cells and fibroblasts: Regulation by TGF-beta. J. Cell Physiol. 2005, 203, 35–43. [Google Scholar] [CrossRef]
- Hooks, J.J.; Nagineni, C.N.; Hooper, L.C.; Hayashi, K.; Detrick, B. IFN-beta provides immuno-protection in the retina by inhibiting ICAM-1 and CXCL9 in retinal pigment epithelial cells. J. Immunol. 2008, 180, 3789–3796. [Google Scholar] [CrossRef] [Green Version]
- Di Pierdomenico, J.; García-Ayuso, D.; Agudo-Barriuso, M.; Vidal-Sanz, M.; Villegas-Pérez, M.P. Role of microglial cells in photoreceptor degeneration. Neural Regen. Res. 2019, 14, 1186–1190. [Google Scholar] [CrossRef] [PubMed]
- Langmann, T. Microglia activation in retinal degeneration. J. Leukoc. Biol. 2007, 81, 1345–1351. [Google Scholar] [CrossRef] [PubMed]
- Boje, K.M.; Arora, P.K. Microglial-produced nitric oxide and reactive nitrogen oxides mediate neuronal cell death. Brain Res. 1992, 587, 250–256. [Google Scholar] [CrossRef]
- Yoshida, N.; Ikeda, Y.; Notomi, S.; Ishikawa, K.; Murakami, Y.; Hisatomi, T.; Enaida, H.; Ishibashi, T. Laboratory evidence of sustained chronic inflammatory reaction in retinitis pigmentosa. Ophthalmology 2013, 120, 5–12. [Google Scholar] [CrossRef]
- Lieberthal, W.; Triaca, V.; Koh, J.S.; Pagano, P.J.; Levine, J.S. Role of superoxide in apoptosis induced by growth factor withdrawal. Am. J. Physiol. 1998, 275, 691–702. [Google Scholar] [CrossRef]
- Bost, L.M.; Aotaki-Keen, A.E.; Hjelmeland, L.M. Cellular adhesion regulates bFGF gene expression in human retinal pigment epithelial cells. Exp. Eye Res. 1994, 58, 545–552. [Google Scholar] [CrossRef]
- Sternfeld, M.D.; Robertson, J.E.; Shipley, G.D.; Tsai, J.; Rosenbaum, J.T. Cultured human retinal pigment epithelial cells express basic fibroblast growth factor and its receptor. Curr. Eye Res. 1989, 8, 1029–1037. [Google Scholar] [CrossRef]
- Tanihara, H.; Yoshida, M.; Matsumoto, M.; Yoshimura, N. Identification of transforming growth factor beta expressed in cultured human retinal pigment epithelial cells. Investig. Ophthalmol. Vis. Sci. 1993, 34, 413–419. [Google Scholar]
- Slomiany, M.G.; Rosenzweig, S.A. Autocrine effects of IGF-I-induced VEGF and IGFBP-3 secretion inretinal pigment epithelial cell line ARPE-19. Am. J. Physiol. Cell Physiol. 2004, 287, 746–753. [Google Scholar] [CrossRef] [Green Version]
- Walsh, N.; Valter, K.; Stone, J. Cellular and subcellular patterns of expression of bFGF and CNTF in the normal and light stressed adult rat retina. Exp. Eye Res. 2001, 72, 495–501. [Google Scholar] [CrossRef]
- Campochiaro, P.A.; Sugg, R.; Grotendorst, G.; Hjelmeland, L.M. Retinal pigment epithelial cells produce PDGF-like proteins and secrete them into their media. Exp. Eye Res. 1989, 49, 217–227. [Google Scholar] [CrossRef]
- Adamis, A.P.; Shima, D.T.; Yeo, K.T.; Yeo, T.K.; Brown, L.F.; Berse, B.; D’Amore, P.A.; Folkman, J. Synthesis and secretion of vascular permeability factor/vascular endothelial growth factor by human retinal pigment epithelial cells. Biochem. Biophys. Res. Commun. 1993, 193, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Wenkel, H.; Streilein, J.W. Evidence that retinal pigment epithelium functions as an immune-privileged tissue. Investig. Ophthalmol. Vis. Sci. 2000, 41, 3467–3473. [Google Scholar]
- Szegezdi, E.; Logue, S.E.; Gorman, A.M.; Samali, A. Mediators of endoplasmic reticulum stress-induced apoptosis. EMBO Rep. 2006, 7, 880–885. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Wu, F.; Kong, X.; Yang, J.; Chen, H.; Deng, L.; Cheng, Y.; Ye, L.; Zhu, S.; Zhang, X.; et al. Nerve growth factor improves functional recovery by inhibiting endoplasmic reticulum stress-induced neuronal apoptosis in rats with spinal cord injury. J. Transl. Med. 2014, 12, 130. [Google Scholar] [CrossRef] [Green Version]
- Ezquer, M.; Urzua, C.A.; Montecino, S.; Leal, K.; Conget, P.; Ezquer, F. Intravitreal administration of multipotent mesenchymal stromal cells triggers a cytoprotective microenvironment in the retina of diabetic mice. Stem Cell Res. Ther. 2016, 7, 42. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.Y.; Mocanu, C.; McLeod, D.S.; Bhutto, I.A.; Merges, C.; Eid, M.; Tong, P.; Lutty, G.A. Expression of pigment epithelium-derived factor (PEDF) and vascular endothelial growth factor (VEGF) in sickle cell retina and choroid. Exp. Eye Res. 2003, 77, 433–445. [Google Scholar] [CrossRef]
- Atashi, F.; Jaconi, M.E.; Pittet-Cuénod, B.; Modarressi, A. Autologous platelet-rich plasma: A biological supplement to enhance adipose-derived mesenchymal stem cell expansion. Tissue Eng. Part C Methods 2015, 21, 253–262. [Google Scholar] [CrossRef] [Green Version]
- Marc, R.E.; Jones, B.W. Retinal remodeling in inherited photoreceptor degenerations. Mol. Neurobiol. 2003, 28, 139–147. [Google Scholar] [CrossRef]
- Eysteinsson, T.; Hardarson, S.H.; Bragason, D.; Stefánsson, E. Retinal vessel oxygen saturation and vessel diameter in retinitis pigmentosa. Acta Ophthalmol. 2014, 92, 449–453. [Google Scholar] [CrossRef]
- Langham, M.E.; Kramer, T. Decreased choroidal blood flow associated with retinitis pigmentosa. Eye 1990, 4, 374–381. [Google Scholar] [CrossRef] [PubMed]
- Beutelspacher, S.C.; Serbecic, N.; Barash, H.; Burgansky-Eliash, Z.; Grinvald, A.; Krastel, H.; Jonas, J.B. Retinal blood flow velocity measured by retinal function imaging in retinitis pigmentosa. Graefe’s Arch. Clin. Exp. Ophthalmol. 2011, 249, 1855–1858. [Google Scholar] [CrossRef] [PubMed]
- Turksever, C.; Valmaggia, C.; Orgul, S.; Schorderet, D.F.; Flamme, J.; Todorova, M.G. Retinal vessel oxygen saturation and Its correlation with structural changes in retinitis pigmentosa. Acta Ophthalmol. 2014, 92, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Ayton, L.N.; Guymer, H.; Luu, C.D. Choroidal thickness profiles in retinitis pigmentosa. Clin. Exp. Ophthalmol. 2013, 41, 396–403. [Google Scholar] [CrossRef] [PubMed]
- Murakami, Y.; Ikeda, Y.; Akiyama, M.; Fujiwara, K.; Yoshida, N.; Nakatake, S.; Notomi, S.; Nabeshima, T.; Hisatomi, T.; Enaida, H.; et al. Correlation between macular blood flow and central visual sensitivity in retinitis pigmentosa. Acta Ophthalmol. 2016, 93, 644–648. [Google Scholar] [CrossRef] [PubMed]
- Anitua, E.; Pelacho, B.; Prado, R.; Aguirre, J.J.; Sánchez, M.; Padilla, S.; Aranguren, X.L.; Abizanda, G.; Collantes, M.; Hernandez, M.; et al. Infiltration of plasma rich in growth factors enhances in vivo angiogenesis and improves reperfusion and tissue remodeling after severe hind limb ischemia. J. Control. Release 2015, 202, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Mammoto, T.; Jiang, A.; Jiang, E.; Mammoto, A. Platelet rich plasma extract promotes angiogenesis through the angiopoietin1-Tie2 pathway. Microvasc. Res. 2013, 89, 15–24. [Google Scholar] [CrossRef]
- Cavallotti, C.; Artico, M.; Pescosolido, N.; Leali, F.M.T.; Feher, J. Age-related changes in the human retina. Can. J. Ophthalmol. 2004, 39, 61–68. [Google Scholar] [CrossRef]
- Cervelli, V.; Bocchini, I.; Di Pasquali, C.; De Angelis, B.; Cervelli, G.; Curcio, C.B.; Orlandi, A.; Scioli, M.G.; Tati, E.; Delogu, P.; et al. PRL platelet rich lipotransfert: Our experience and current state of art in the combined use of fat and PRP. Biomed. Res. Int. 2013, 2013, 434191. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients | Group A-FT ≤ 190 µm | Group B-FT > 190 µm | Total |
|---|---|---|---|
| Number: Patients/eyes | 6/8 | 9/13 | 15/21 |
| Age years (± standard deviation (SD)) | 40.33 (13.98) | 59.88 (18.93) | 52.06 (19.31) |
| Range (years) | 19–54 | 32–86 | 21–82 |
| Female/male | 3/3 | 3/6 | 6/9 |
| Eye: Right/left | 2/6 | 7/6 | 9/12 |
| Parameters | Group | Mean ± SD Min–Max | Values (T0) | Values (T180) | % | Time Effect p-Value | Group Effect p-Value |
|---|---|---|---|---|---|---|---|
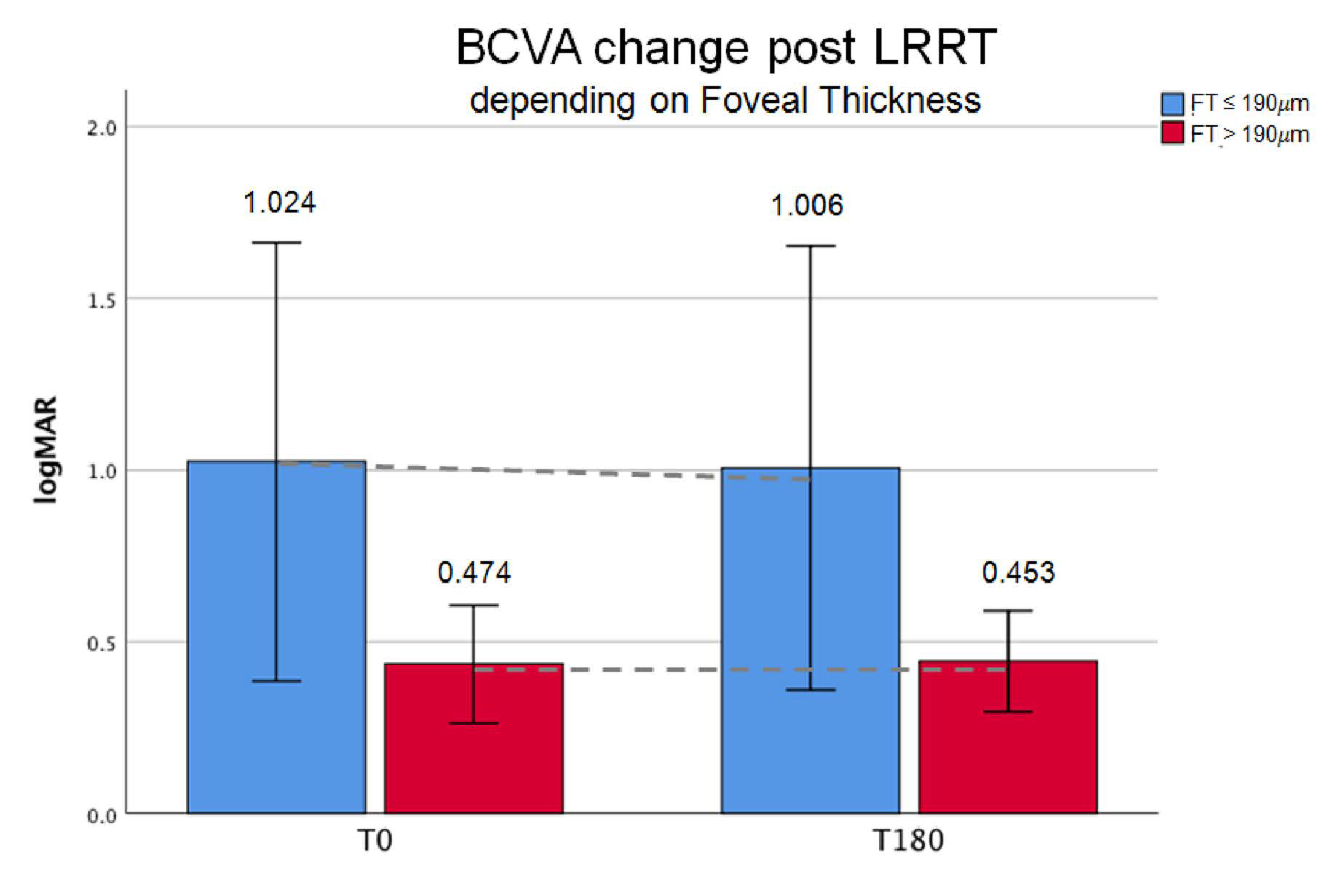
| logMAR | A-FT ≤190 µm | mean ± SD | 1.02 ± 0.76 | 1.01 ± 0.77 | +1.76 | ||
| min–max | 0.10–2.70 | 0.10–2.70 | |||||
| B-FT >190 µm | mean ± SD | 0.47 ± 0.21 | 0.45 ± 0.18 | +4.51 | |||
| min–max | 0.15–0.70 | 0.15–0.79 | 0.562 | 0.051 | |||
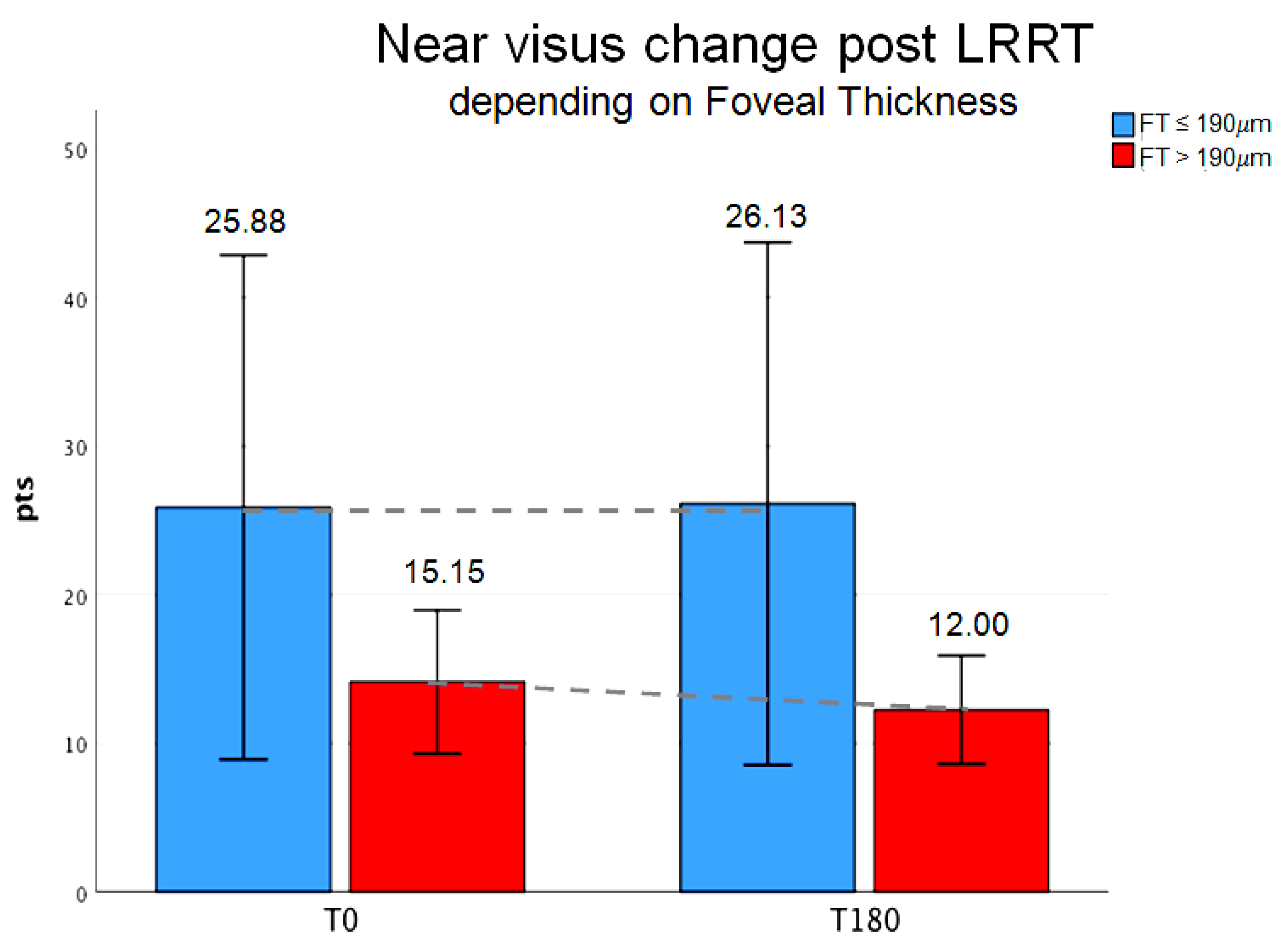
| pts | A-FT ≤190 µm | mean ± SD | 25.88 ± 20.29 | 26.13 ± 21.03 | +0.97 | ||
| min–max | 8–64 | 7–64 | |||||
| B-FT >190 µm | mean ± SD | 15.15 ± 5.86 | 12 ± 4 | +20.79 | |||
| min–max | 7–26 | 7–18 | 0.269 | 0.08 | |||
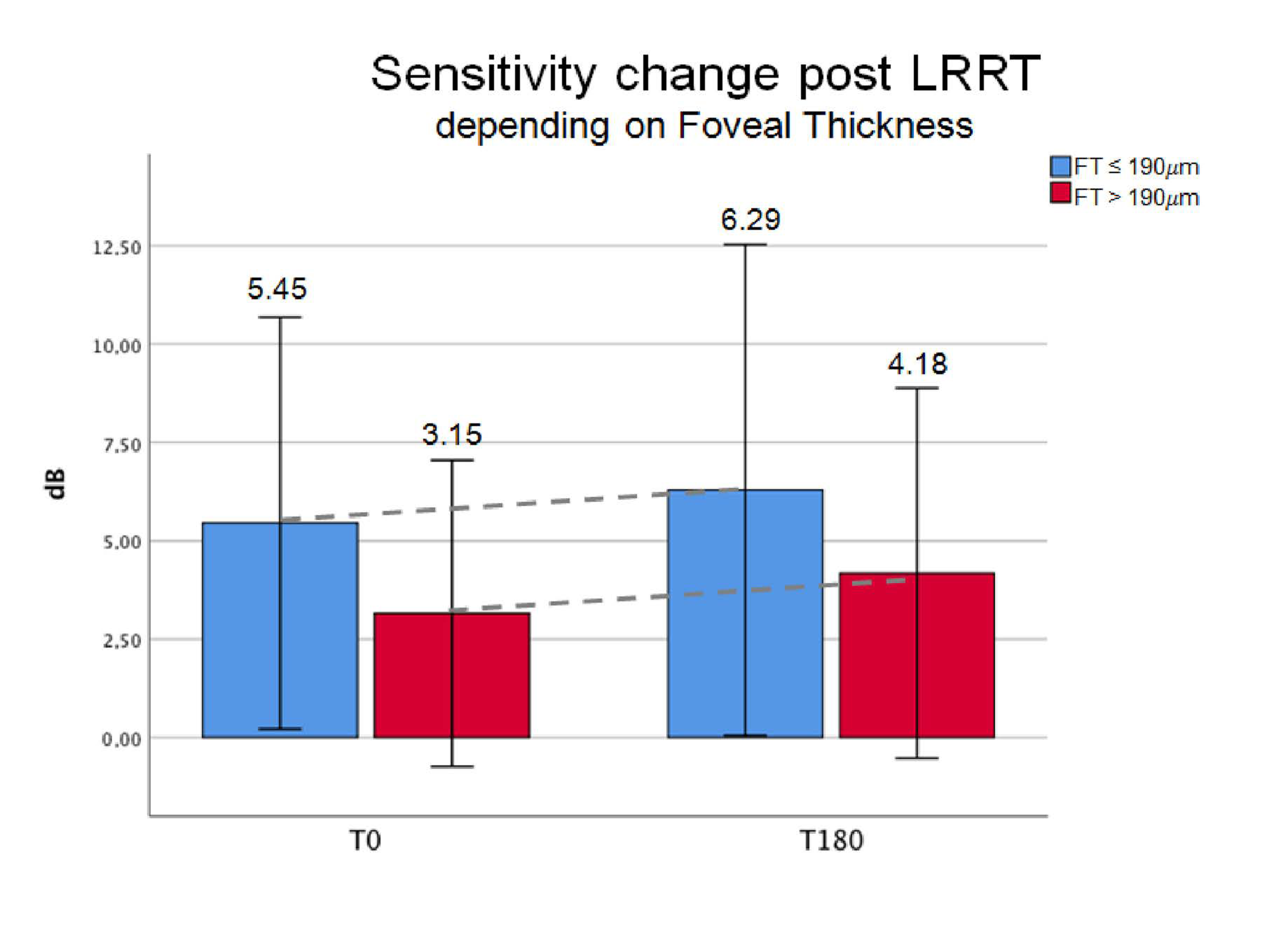
| dB MAIA | A-FT ≤190 µm | mean ± SD | 5.45 ± 6.8 | 6.29 ± 8.11 | +15.41 | ||
| min–max | 0–16 | 0–18.2 | |||||
| B-FT >190 µm | mean ± SD | 3.15 ± 6.45 | 4.18 ± 7.79 | +32.70 | |||
| min–max | 0–19.4 | 0–21.8 | 0.003 | 0.535 | |||
| Cµm | A-FT ≤190 µm | mean ± SD | 140.75 ± 37.42 | 133.88 ± 54.28 | −0.05 | ||
| min–max | 49–160 | 0–161 | |||||
| B-FT >190 µm | mean ± SD | 275.46 ± 88.1 | 275.08 ± 89 | 0.00 | |||
| min–max | 195–462 | 187–471 | 0.303 | <0.001 | |||
| µm3 | A-FT ≤190 µm | mean ± SD | 7.03 ± 1.39 | 7.67 ± 0.45 | +0.09 | ||
| min–max | 4.6–8.7 | 7.3–8.6 | |||||
| B-FT >190 µm | mean ± SD | 8.92 ± 1.38 | 8.79 ± 1.48 | −0.01 | |||
| min–max | 6.5–10.7 | 6.5–11 | 0.806 | 0.023 | |||
| Aµm2 | A-FT ≤190 µm | mean ± SD | 202.49 ± 23.4 | 212.86 ± 12.75 | +0.05 | ||
| min–max | 164.9–240 | 202–239 | |||||
| B-FT >190 µm | mean ± SD | 247.62 ± 38.69 | 244.15 ± 40.4 | -0.01 | |||
| min–max | 179–299 | 181–305 | 0.949 | 0.023 |
| Variation (T180–T0) | A-FT ≤190 µm 8 Eyes | B-FT >190 µm 13 Eyes | Interaction Effect p-Value | |
|---|---|---|---|---|
| logMAR | mean ± SD | −0.02 ± 0.07 | −0.02 ± 0.04 | 0.971 |
| pts | mean ± SD | 0.25 ± 3.76 | −3.15 ± 1.24 | 0.390 |
| dB MAIA | mean ± SD | 0.84 ± 0.59 | 1.02 ± 0.53 | 0.818 |
| Cµm | mean ± SD | −6.88 ± 6.71 | −0.38 ± 1.59 | 0.346 |
| µm3 | mean ± SD | 0.35 ± 0.37 | −0.12 ± 0.18 | 0.248 |
| Aµm2 | mean ± SD | 5.66 ± 5.63 | −3.46 ± 4.66 | 0.212 |
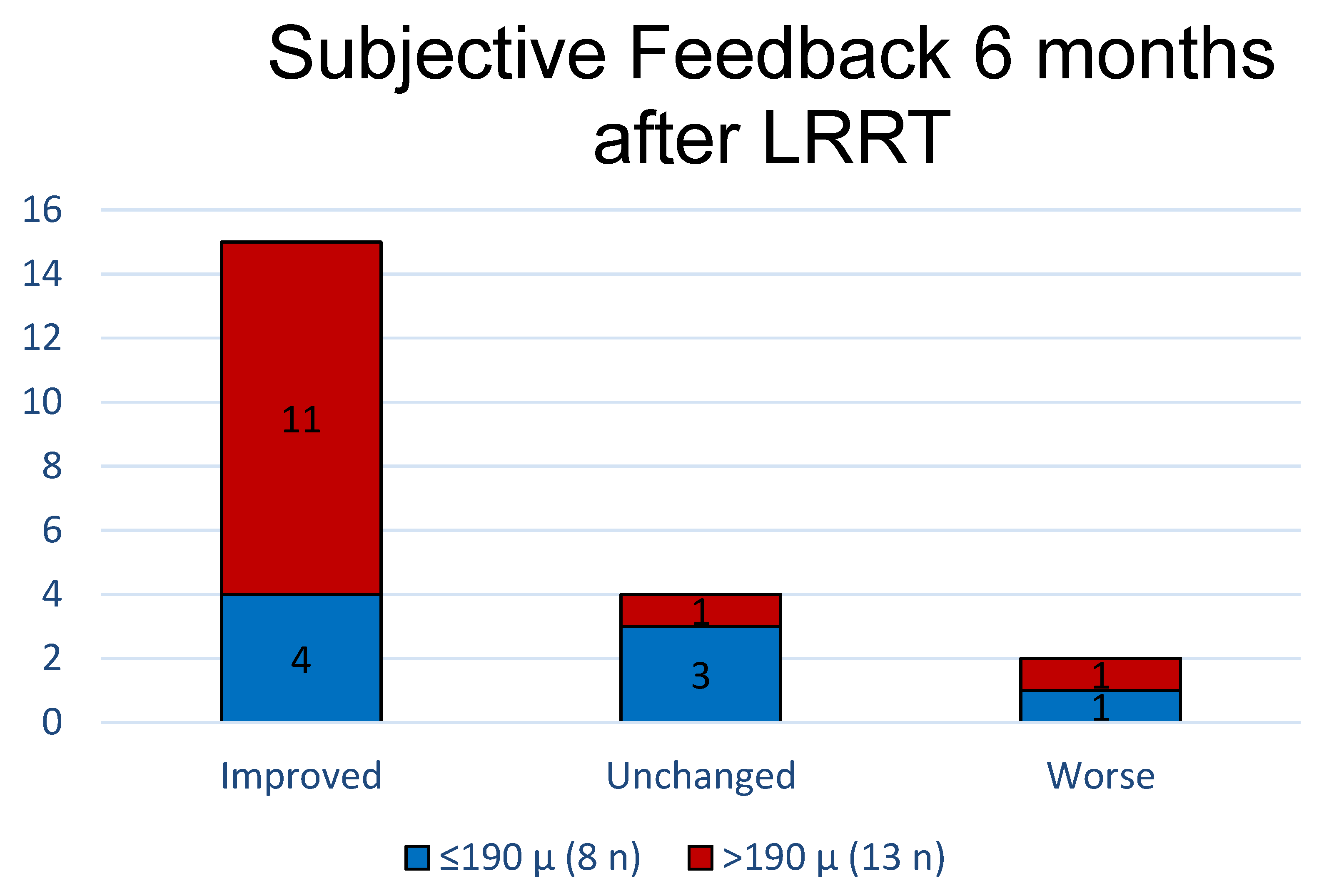
| Compliance | A-FT ≤ 190 µm (8 Eyes) | B-FT > 190 µm (13 Eyes) | ||
|---|---|---|---|---|
| Improved | 4 | 50.00% | 11 | 84.62% |
| Unchanged | 3 | 37.50% | 1 | 7.69% |
| Worse | 1 | 12.50% | 1 | 7.69% |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Limoli, P.G.; Vingolo, E.M.; Limoli, C.; Nebbioso, M. Stem Cell Surgery and Growth Factors in Retinitis Pigmentosa Patients: Pilot Study after Literature Review. Biomedicines 2019, 7, 94. https://doi.org/10.3390/biomedicines7040094
Limoli PG, Vingolo EM, Limoli C, Nebbioso M. Stem Cell Surgery and Growth Factors in Retinitis Pigmentosa Patients: Pilot Study after Literature Review. Biomedicines. 2019; 7(4):94. https://doi.org/10.3390/biomedicines7040094
Chicago/Turabian StyleLimoli, Paolo Giuseppe, Enzo Maria Vingolo, Celeste Limoli, and Marcella Nebbioso. 2019. "Stem Cell Surgery and Growth Factors in Retinitis Pigmentosa Patients: Pilot Study after Literature Review" Biomedicines 7, no. 4: 94. https://doi.org/10.3390/biomedicines7040094
APA StyleLimoli, P. G., Vingolo, E. M., Limoli, C., & Nebbioso, M. (2019). Stem Cell Surgery and Growth Factors in Retinitis Pigmentosa Patients: Pilot Study after Literature Review. Biomedicines, 7(4), 94. https://doi.org/10.3390/biomedicines7040094