
Checkpoint Inhibitors and Hepatotoxicity


Abstract
:1. Introduction
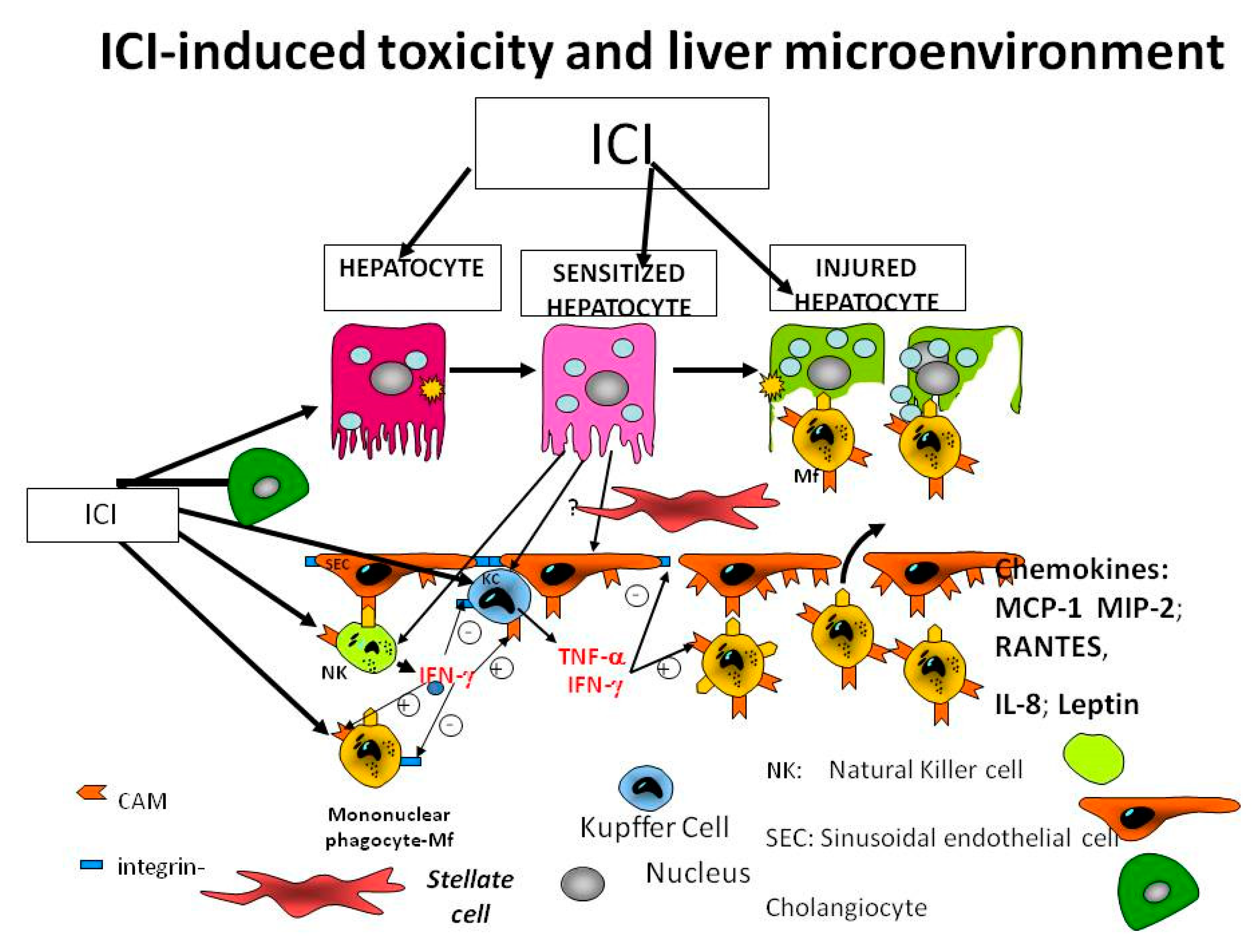
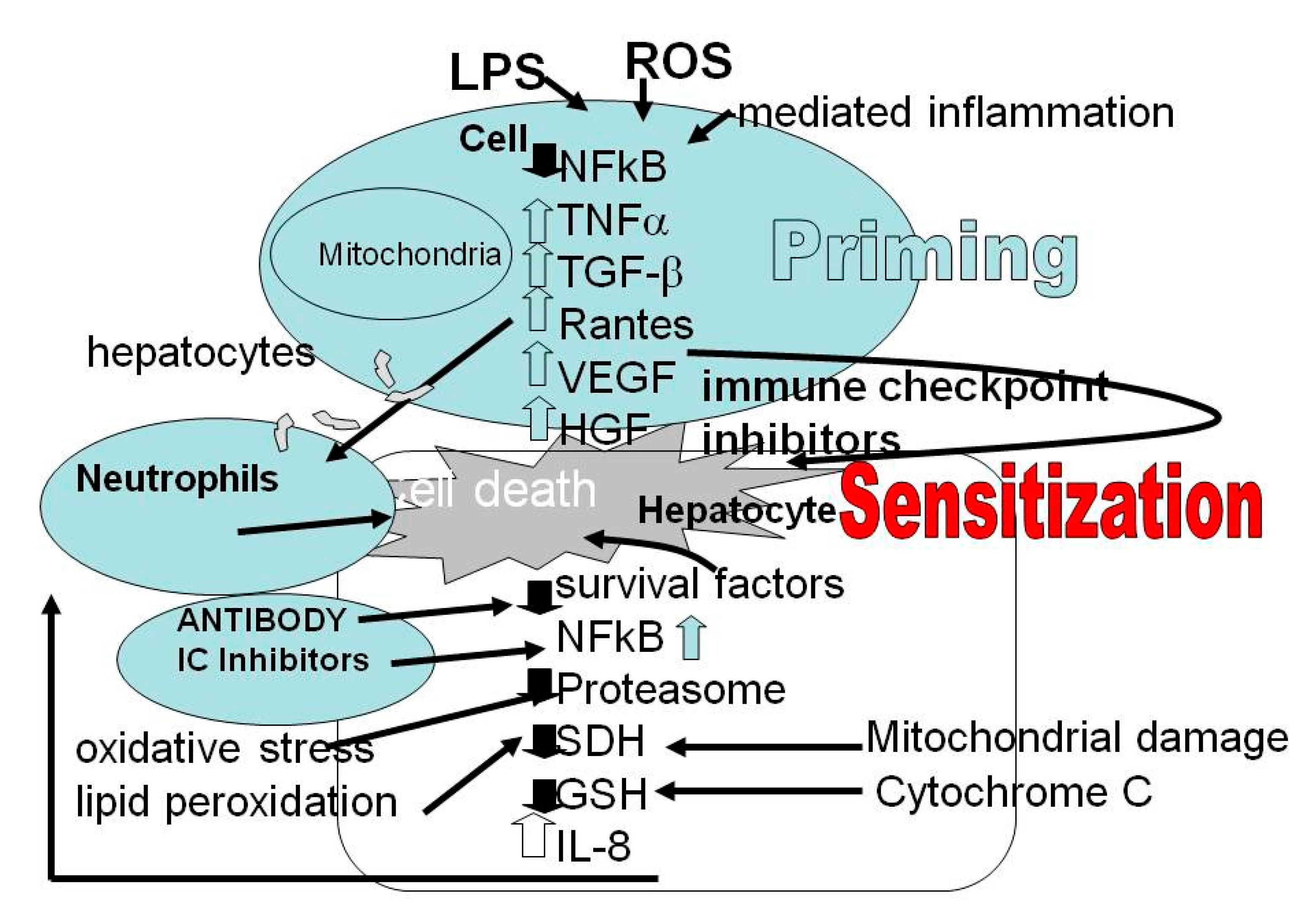
2. Tumor Microenvironment
3. Biomarkers for Severity of the Disease
4. Checkpoint Inhibitors
5. Approved Checkpoint Inhibitors
6. Hepatic Side Effects
7. Histology
8. Hepatic Injury Related to ICI Treatment
9. IPI Treatment of Hepatocellular Carcinoma
10. ICIs and Liver Transplant Recipients
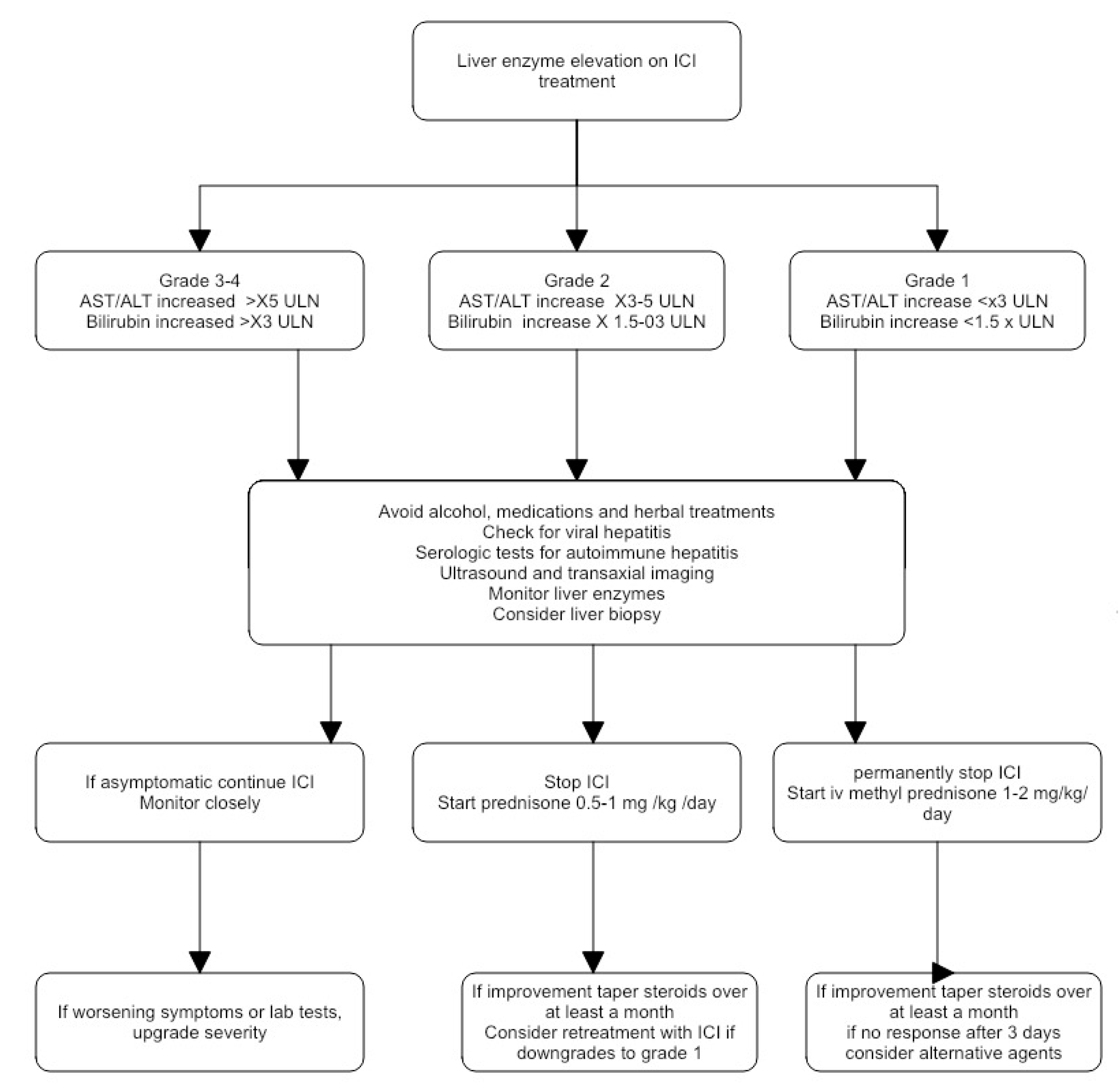
11. Clinical Management of Immune Check Point Inhibitors-Induced Hepatotoxicity
12. Patient Education
13. Summary
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| ALT | alanine aminotransferase = alanine transaminase = glutamic pyruvic transaminase (GPT) |
| ANA | antinuclear antibody |
| ALP | alkaline phosphatase |
| AST | aspartate aminotransferase = aspartate transaminase = glutamic oxalic transaminase (GOT) |
| BRCA | breast cancer susceptibility alleles |
| CS | corticosteroid |
| CS Tx | corticosteroid therapy |
| CTCAE CPIH | Common Terminology Criteria for Adverse Events Check point inhibitor hepatotoxicity |
| CTLA-4- cytotoxic T | lymphocytes associated antigen 4 |
| DC Dx | dendritic cells Dexametasone |
| DILI | drug-induced liver injury |
| DILIN | drug-induced liver injury network |
| dMMR | microscope set microsatellite instability high or mismatch repair deficiency |
| ECM | extracellular matrix |
| EMA | European Medicines Agency |
| FDA | United States Food and Drug Administration |
| FGF | fibroblast growth factor |
| FGFR | fibroblast growth factor signaling pathway |
| FISH | Fluorescence In-Situ Hybridization |
| GI | Gastrointestinal |
| GLDH | glutamate dehydrogenase |
| GGT | gamma-glutamyl-transferase |
| HER2 | Human estrogen receptor 2 |
| HMGB1 | High-mobility group box 1 |
| ICI | immune checkpoint inhibitor |
| ICOS | Inducible T-cell co-stimulator |
| IL | Interleukin |
| ICH | Immuno-Histochemistry |
| IFN-γ | interferon-gamma |
| KIR2DS2 | Killer cell immunoglobulin-like receptor |
| LFT | liver function test |
| LY403200 | hepatitis A virus cellular receptor 2 (HAVCR2) |
| M-CSFR | macrophage colony-stimulating factor |
| MMF | Mycophenolate |
| MYC | Oncogene c-MYC |
| p53 | tumor suppressor protein 53 |
| PD-1 | programmed cell death receptor 1 |
| PDL-1 | programmed cell death ligand 1 |
| PDL- 2 | programmed cell death ligand 2 |
| PIK3CA | protein IK3 oncogene |
| PTEN | Phosphatase and Tensin Homolog deleted on Chromosome 10 |
| RANTES | Regulated upon Activation, Normal T cell Expressed and presumably Secreted |
| RUCAM | Roussel Uclaf Causality Assessment Method |
| TBL | total bilirubin |
| TGF- β | transforming growth factor β |
| TIM 3 | T-cell immunoglobulin and mucin domain 3 (Tim-3) encoded in germline mutations in HAVCR2 |
| TME | tumor microenvironment |
| TNF-α | Tumor necrosis factor alpha |
| TNFRSF18 | Tumor necrosis factor receptor superfamily member 18 |
| Tx | Therapeutic agent |
| UDCA | urso-deoxycholic acid |
| ULN | upper limit of normal |
| VEGF | vascular endothelial growth factor. |
References
- Sharma, P.; Allison, J.P. The future of immune checkpoint therapy. Science 2015, 348, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Cabioglu, N.; Gong, Y.; Islam, R.; Broglio, K.R.; Sneige, N.; Sahin, A.; Gonzalez-Angulo, A.M.; Morandi, P.; Bucana, C.; Hortobagyi, G.N.; et al. Expression of growth factor and chemokine receptors: New insights in the biology of inflammatory breast cancer. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2007, 18, 1021–1029. [Google Scholar] [CrossRef] [PubMed]
- Plas, D.R.; Johnson, R.; Pingel, J.T.; Matthews, R.J.; Dalton, M.; Roy, G.; Chan, A.C.; Thomas, M.L. Direct regulation of ZAP-70 by SHP-1 in T cell antigen receptor signaling. Science 1996, 272, 1173–1176. [Google Scholar] [CrossRef] [PubMed]
- Triebel, F.; Jitsukawa, S.; Baixeras, E.; Roman-Roman, S.; Genevee, C.; Viegas-Pequignot, E.; Hercend, T. LAG-3, a novel lymphocyte activation gene closely related to CD4. J. Exp. Med. 1990, 171, 1393–1405. [Google Scholar] [CrossRef] [Green Version]
- Solinas, C.; Migliori, E.; de Silva, P.; Willard-Gallo, K. LAG3: The Biological Processes That Motivate Targeting This Immune Checkpoint Molecule in Human Cancer. Cancers 2019, 11, 1213. [Google Scholar] [CrossRef] [Green Version]
- Blackburn, S.D.; Shin, H.; Haining, W.N.; Zou, T.; Workman, C.J.; Polley, A.; Betts, M.R.; Freeman, G.J.; Vignali, D.A.A.; Wherry, E.J. Coregulation of CD8+ T cell exhaustion by multiple inhibitory receptors during chronic viral infection. Nat. Immunol. 2009, 10, 29–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Long, L.; Zhang, X.; Chen, F.; Pan, Q.; Phiphatwatchara, P.; Zeng, Y.; Chen, H. The promising immune checkpoint LAG-3: From tumor microenvironment to cancer immunotherapy. Genes Cancer 2018, 9, 176–189. [Google Scholar] [CrossRef] [Green Version]
- Matsuzaki, J.; Gnjatic, S.; Mhawech-Fauceglia, P.; Beck, A.; Miller, A.; Tsuji, T.; Eppolito, C.; Qian, F.; Lele, S.; Shrikant, P.; et al. Tumor-infiltrating NY-ESO-1-specific CD8+ T cells are negatively regulated by LAG-3 and PD-1 in human ovarian cancer. Proc. Natl. Acad. Sci. USA 2010, 107, 7875–7880. [Google Scholar] [CrossRef] [Green Version]
- Anderson, A.C. Tim-3: An emerging target in the cancer immunotherapy landscape. Cancer Immunol. Res. 2014, 2, 393–398. [Google Scholar] [CrossRef] [Green Version]
- Holderried, T.A.W.; de Vos, L.; Bawden, E.G.; Vogt, T.J.; Dietrich, J.; Zarbl, R.; Bootz, F.; Kristiansen, G.; Brossart, P.; Landsberg, J.; et al. Molecular and immune correlates of TIM-3 (HAVCR2) and galectin 9 (LGALS9) mRNA expression and DNA methylation in melanoma. Clin. Epigenet. 2019, 11, 161. [Google Scholar] [CrossRef]
- Monney, L.; Sabatos, C.A.; Gaglia, J.L.; Ryu, A.; Waldner, H.; Chernova, T.; Manning, S.; Greenfield, E.A.; Coyle, A.J.; Sobel, R.A.; et al. Th1-specific cell surface protein Tim-3 regulates macrophage activation and severity of an autoimmune disease. Nature 2002, 415, 536–541. [Google Scholar] [CrossRef] [PubMed]
- Fourcade, J.; Sun, Z.; Benallaoua, M.; Guillaume, P.; Luescher, I.F.; Sander, C.; Kirkwood, J.M.; Kuchroo, V.; Zarour, H.M. Upregulation of Tim-3 and PD-1 expression is associated with tumor antigen-specific CD8+ T cell dysfunction in melanoma patients. J. Exp. Med. 2010, 207, 2175–2186. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, N.; Lim, B.; Wang, Y.; Krishnamurthy, S.; Woodward, W.; Alvarez, R.H.; Lucci, A.; Valero, V.; Reuben, J.M.; Meric-Bernstam, F.; et al. Identification of frequent somatic mutations in inflammatory breast cancer. Breast Cancer Res. Treat. 2017, 163, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Rana, H.Q.; Sacca, R.; Drogan, C.; Gutierrez, S.; Schlosnagle, E.; Regan, M.M.; Speare, V.; LaDuca, H.; Dolinsky, J.; Garber, J.E.; et al. Prevalence of germline variants in inflammatory breast cancer. Cancer 2019, 125, 2194–2202. [Google Scholar] [CrossRef]
- Qi, Y.; Wang, X.; Kong, X.; Zhai, J.; Fang, Y.; Guan, X.; Wang, J. Expression signatures and roles of microRNAs in inflammatory breast cancer. Cancer Cell Int. 2019, 19, 23. [Google Scholar] [CrossRef] [Green Version]
- Ding, Q.; Wang, Y.; Zuo, Z.; Gong, Y.; Krishnamurthy, S.; Li, C.-W.; Lai, Y.-J.; Wei, W.; Wang, J.; Manyam, G.C.; et al. Decreased expression of microRNA-26b in locally advanced and inflammatory breast cancer. Hum. Pathol. 2018, 77, 121–129. [Google Scholar] [CrossRef]
- Chen, Q.; Zhang, X.H.-F.; Massagué, J. Macrophage binding to receptor VCAM-1 transmits survival signals in breast cancer cells that invade the lungs. Cancer Cell 2011, 20, 538–549. [Google Scholar] [CrossRef] [Green Version]
- Pietras, K.; Pahler, J.; Bergers, G.; Hanahan, D. Functions of paracrine PDGF signaling in the proangiogenic tumor stroma revealed by pharmacological targeting. PLoS Med. 2008, 5, e19. [Google Scholar] [CrossRef]
- Champiat, S.; Lambotte, O.; Barreau, E.; Belkhir, R.; Berdelou, A.; Carbonnel, F.; Cauquil, C.; Chanson, P.; Collins, M.; Durrbach, A.; et al. Management of immune checkpoint blockade dysimmune toxicities: A collaborative position paper. Ann. Oncol. 2016, 27, 559–574. [Google Scholar] [CrossRef]
- Suzman, D.L.; Pelosof, L.; Rosenberg, A.; Avigan, M.I. Hepatotoxicity of immune checkpoint inhibitors: An evolving picture of risk associated with a vital class of immunotherapy agents. Liver Int. 2018, 38, 976–987. [Google Scholar] [CrossRef] [Green Version]
- Hargadon, K.M.; Johnson, C.E.; Williams, C.J. Immune checkpoint blockade therapy for cancer: An overview of FDA-approved immune checkpoint inhibitors. Int. Immunopharmacol. 2018, 62, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Naidoo, J.; Page, D.B.; Li, B.T.; Connell, L.C.; Schindler, K.; Lacouture, M.E.; Postow, M.A.; Wolchok, J.D. Toxicities of the anti-PD-1 and anti-PD-L1 immune checkpoint antibodies. Ann. Oncol. 2015, 26, 2375–2391. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M. Checkpoint inhibitors: What gastroenterologists need to know. World J. Gastroenterol. 2018, 24, 5433–5438. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Lie, P.; Guo, M.; He, J. Risk of hepatotoxicity in cancer patients treated with immune checkpoint inhibitors: A systematic review and meta-analysis of published data. Int. J. Cancer 2017, 141, 1018–1028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peeraphatdit, T.; Wang, J.; Odenwald, M.A.; Hu, S.; Hart, J.; Charlton, M.R. Hepatotoxicity from Immune Checkpoint Inhibitors: A Systematic Review and Management Recommendation. Hepatology 2020. [Google Scholar] [CrossRef]
- Parlati, L.; Vallet-Pichard, A.; Batista, R.; Hernvann, A.; Sogni, P.; Pol, S.; Mallet, V. Incidence of grade 3-4 liver injury under immune checkpoints inhibitors: A retrospective study. J. Hepatol. 2018, 69, 1396–1397. [Google Scholar] [CrossRef] [Green Version]
- Danan, G.; Teschke, R. Roussel UCLAF causality assessment method for drug-induced liver injury: Present and future. Front. Pharmacol. 2019, 10, 853. [Google Scholar] [CrossRef] [Green Version]
- Andersen, R.; Nørgaard, P.; Al-Jailawi, M.K.M.; Svane, I.M. Late development of splenic sarcoidosis-like lesions in a patient with metastatic melanoma and long-lasting clinical response to ipilimumab. Oncoimmunology 2014, 3, e954506. [Google Scholar] [CrossRef] [Green Version]
- Berthod, G.; Lazor, R.; Letovanec, I.; Romano, E.; Noirez, L.; Mazza Stalder, J.; Speiser, D.E.; Peters, S.; Michielin, O. Pulmonary sarcoid-like granulomatosis induced by ipilimumab. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2012, 30, e156–e159. [Google Scholar] [CrossRef]
- De Martin, E.; Michot, J.-M.; Papouin, B.; Champiat, S.; Mateus, C.; Lambotte, O.; Roche, B.; Antonini, T.M.; Coilly, A.; Laghouati, S.; et al. Characterization of liver injury induced by cancer immunotherapy using immune checkpoint inhibitors. J. Hepatol. 2018, 68, 1181–1190. [Google Scholar] [CrossRef]
- Zen, Y.; Yeh, M.M. Hepatotoxicity of immune checkpoint inhibitors: A histology study of seven cases in comparison with autoimmune hepatitis and idiosyncratic drug-induced liver injury. Mod. Pathol. 2018, 31, 965–973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kluetz, P.G.; Chingos, D.T.; Basch, E.M.; Mitchell, S.A. Patient-Reported Outcomes in Cancer Clinical Trials: Measuring Symptomatic Adverse Events With the National Cancer Institute’s Patient-Reported Outcomes Version of the Common Terminology Criteria for Adverse Events (PRO-CTCAE). Am. Soc. Clin. Oncol. Educ. Book 2016. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, H.J. Hepatotoxicity: The Adverse Effects of Drug and Other Chemicals on the Hepatic; Lippinocott, Williams and Wilkins: Philadelphia, PA, USA, 1999. [Google Scholar]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.J.; Cowey, C.L.; Lao, C.D.; Schadendorf, D.; Dummer, R.; Smylie, M.; Rutkowski, P.; et al. Combined nivolumab and ipilimumab or monotherapy in untreated Melanoma. N. Engl. J. Med. 2015, 373, 23–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolchok, J.D.; Chiarion-Sileni, V.; Gonzalez, R.; Rutkowski, P.; Grob, J.J.; Cowey, C.L.; Lao, C.D.; Wagstaff, J.; Schadendorf, D.; Ferrucci, P.F.; et al. Overall Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2017, 377, 1345–1356. [Google Scholar] [CrossRef] [PubMed]
- Nadeau, B.A.; Fecher, L.A.; Owens, S.R.; Razumilava, N. Liver Toxicity with Cancer Checkpoint Inhibitor Therapy. Semin. Liver Dis. 2018, 38, 366–378. [Google Scholar] [CrossRef] [PubMed]
- Wolchok, J.D.; Kluger, H.; Callahan, M.K.; Postow, M.A.; Rizvi, N.A.; Lesokhin, A.M.; Segal, N.H.; Ariyan, C.E.; Gordon, R.A.; Reed, K.; et al. Nivolumab plus Ipilimumab in advanced melanoma. N. Engl. J. Med. 2013, 369, 122–133. [Google Scholar] [CrossRef] [Green Version]
- Weber, J.; Mandala, M.; del Vecchio, M.; Gogas, H.J.; Arance, A.M.; Cowey, C.L.; Dalle, S.; Schenker, M.; Chiarion-Sileni, V.; Marquez-Rodas, I.; et al. Adjuvant nivolumab versus ipilimumab in resected stage III or IV melanoma. N. Engl. J. Med. 2017, 377, 1824–1835. [Google Scholar] [CrossRef]
- Tsung, I.; Dolan, R.; Lao, C.; Fecher, L.; Riggenbach, K.; Yeboah-Korang, A.; Fontana, R. Liver injury is most commonly due to hepatic metastases rather than drug hepatotoxicity during pembrolizumab immunotherapy. Ailm. Pharmacol. Ther. 2019, 50, 800–808. [Google Scholar] [CrossRef] [Green Version]
- Touat, M.; Maisonobe, T.; Knauss, S.; ben Hadj Salem, O.; Hervier, B.; Auré, K.; Szwebel, T.A.; Kramkimel, N.; Lethrosne, C.; Bruch, J.F.; et al. Immune checkpoint inhibitor-related myositis and myocarditis in patients with cancer. Neurology 2018, 91, e985–e994. [Google Scholar] [CrossRef]
- Everett, J.; Srivastava, A.; Misdraji, J. Fibrin ring granulomas in checkpoint inhibitor-induced hepatitis. Am. J. Surg. Pathol. 2017, 41, 134–137. [Google Scholar] [CrossRef]
- Cheung, V.; Gupta, T.; Payne, M.; Middleton, M.R.; Collier, J.D.; Simmons, A.; Klenerman, P.; Brain, O.; Cobbold, J.F. Immunotherapy-related hepatitis: Real-world experience from a tertiary centre. Frontline Gastroenterol. 2019, 10, 364–371. [Google Scholar] [CrossRef] [PubMed]
- Gauci, M.-L.; Baroudjian, B.; Zeboulon, C.; Pages, C.; Poté, N.; Roux, O.; Bouattour, M.; Lebbé, C.; the PATIO Group. Immune-related hepatitis with immunotherapy: Are corticosteroids always needed? J. Hepatol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Pollack, M.H.; Betof, A.; Dearden, H.; Rapazzo, K.; Valentine, I.; Brohl, A.S.; Ancell, K.K.; Long, G.V.; Menzies, A.M.; Eroglu, Z.; et al. Safety of resuming anti-PD-1 in patients with immune-related adverse events (irAEs) during combined anti-CTLA-4 and anti-PD1 in metastatic melanoma. Ann. Oncol. 2018, 29, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Chmiel, K.D.; Suan, D.; Liddle, C.; Nankivell, B.; Ibrahim, R.; Bautista, C.; Thompson, J.; Fulcher, D.; Kefford, R. Resolution of severe ipilimumab-induced hepatitis after antithymocyte globulin therapy. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2011, 29, e237–e240. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, T.; Pandey, R.; Shah, B.; Black, J. Resolution of ipilimumab induced severe hepatotoxicity with triple immunosuppressants therapy. BMJ Case Rep. 2015, 2015, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Iwamoto, K.; Ishitsuka, Y.; Tanaka, R.; Sekine, I.; Fujimoto, M. Azathioprine combination therapy for steroid-refractory hepatic immune system-related adverse events. Eur. J. Dermatol. EJD 2017, 27, 301–303. [Google Scholar] [CrossRef] [Green Version]
- Spänkuch, I.; Gassenmaier, M.; Tampouri, I.; Noor, S.; Forschner, A.; Garbe, C.; Amaral, T. Severe hepatitis under combined immunotherapy: Resolution under corticosteroids plus anti-thymocyte immunoglobulins. Eur. J. Cancer 2017, 81, 203–205. [Google Scholar] [CrossRef]
- Huffman, B.M.; Kottschade, L.A.; Kamath, P.S.; Markovic, S.N. Hepatotoxicity after Immune Checkpoint Inhibitor Therapy in Melanoma: Natural Progression and Management. Am. J. Clin. Oncol. 2018, 41, 760–765. [Google Scholar] [CrossRef]
- Matsubara, T.; Nishida, T.; Higaki, Y.; Tomita, R.; Shimakoshi, H.; Shimoda, A.; Osugi, N.; Sugimoto, A.; Takahashi, K.; Nakamatsu, D.; et al. Nivolumab Induces Sustained Liver Injury in a Patient with Malignant Melanoma. Intern. Med. 2018, 57, 1789–1792. [Google Scholar] [CrossRef] [Green Version]
- McGuire, H.M.; Shklovskaya, E.; Edwards, J.; Trevillian, P.R.; McCaughan, G.W.; Bertolino, P.; McKenzie, C.; Gourlay, R.; Gallagher, S.J.; de St Groth, B.F.; et al. Anti-PD-1-induced high-grade hepatitis associated with corticosteroid-resistant T cells: A case report. Cancer Immunol. Immunother. CII 2018, 67, 563–573. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, R.; Fujisawa, Y.; Sae, I.; Maruyama, H.; Ito, S.; Hasegawa, N.; Sekine, I.; Fujimoto, M. Severe hepatitis arising from ipilimumab administration, following melanoma treatment with nivolumab. Jpn. J. Clin. Oncol. 2017, 47, 175–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Z.; Lai, L.; Li, M.; Zhang, L.; Zhang, W. Acute liver failure caused by pembrolizumab in a patient with pulmonary metastatic liver cancer: A case report. Medicine 2017, 96, e9431. [Google Scholar] [CrossRef] [PubMed]
- Yildirim, S.; Deniz, K.; Doğan, E.; Başkol, M.; Gürsoy, Ş.; Özkan, M. Ipilimumab-associated cholestatic hepatitis: A case report and literature review. Melanoma Res. 2017, 27, 380–382. [Google Scholar] [CrossRef] [PubMed]
- Kopecký, J.; Kubecek, O.; Geryk, T.; Podhola, M.; Ziaran, M.; Priester, P.; Hanisova, M.; Borilova, S. Hepatic Injury Induced by a Single Dose of Nivolumab—A Case Report and Literature Review. Klin. Onkol. Cas. Ceske Slov. Onkol. Spol. 2019, 32, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Forner, A.; Reig, M.; Bruix, J. Hepatocellular carcinoma. Lancet 2018, 391, 1301–1314. [Google Scholar] [CrossRef]
- Copur, M.S. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 2498. [Google Scholar] [PubMed]
- Finn, R.S.; Ryoo, B.-Y.; Merle, P.; Kudo, M.; Bouattour, M.; Yeong Lim, H.; Breder, V.; Edeline, J.; Chao, Y.; Ogasawara, S.; et al. Pembrolizumab As Second-Line Therapy in Patients with Advanced Hepatocellular Carcinoma in KEYNOTE-240: A Randomized, Double-Blind, Phase III Trial. J. Clin. Oncol. 2019, 38, 193–202. [Google Scholar] [CrossRef] [PubMed]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef]
- Engels, E.A.; Ruth Pfeiffer, M.M.; Fraumeni, J.F., Jr.; Kasiske, B.L.; Israni, A.K.; Jon Snyder, M.J.; Wolfe, R.A.; Goodrich, N.P.; Rana Bayakly, M.A.; Christina Clarke, M.A.; et al. Spectrum of Cancer Risk Among US Solid Organ Transplant Recipients. JAMA 2011, 306, 1891–1901. [Google Scholar] [CrossRef]
- Filgueira, N.A. Hepatocellular carcinoma recurrence after liver transplantation: Risk factors, screening and clinical presentation. World J. Hepatol. 2019, 11, 261–272. [Google Scholar] [CrossRef]
- Munker, S.; de Toni, E.N. Use of checkpoint inhibitors in liver transplant recipients. United Eur. Gastroenterol. J. 2018, 6, 970–973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sangro, B.; Gomez-Martin, C.; de La Mata, M.; Iñarrairaegui, M.; Garralda, E.; Barrera, P.; Riezu-Boj, J.I.; Larrea, E.; Alfaro, C.; Sarobe, P.; et al. A clinical trial of CTLA-4 blockade with tremelimumab in patients with hepatocellular carcinoma and chronic hepatitis C. J. Hepatol. 2013, 59, 81–88. [Google Scholar] [CrossRef] [PubMed]
- El-Khoueiry, A.B.; Sangro, B.; Yau, T.; Crocenzi, T.S.; Kudo, M.; Hsu, C.; Kim, T.Y.; Choo, S.P.; Trojan, J.; Welling, T.H.; et al. Nivolumab in patients with advanced hepatocellular carcinoma (CheckMate 040): An open-label, non-comparative, phase 1/2 dose escalation and expansion trial. Lancet 2017, 389, 2492–2502. [Google Scholar] [CrossRef]
- Zhu, A.X.; Finn, R.S.; Edeline, J.; Cattan, S.; Ogasawara, S.; Palmer, D.; Verslype, C.; Zagonel, V.; Fartoux, L.; Vogel, A.; et al. Pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib (KEYNOTE-224): A non-randomised, open-label phase 2 trial. Lancet Oncol. 2018, 19, 940–952. [Google Scholar] [CrossRef]
- Puzanov, I.; Diab, A.; Abdallah, K.; Bingham, C.O.; Brogdon, C.; Dadu, R.; Hamad, L.; Kim, S.; Lacouture, M.E.; LeBoeuf, N.R.; et al. Managing toxicities associated with immune checkpoint inhibitors: Consensus recommendations from the Society for Immunotherapy of Cancer (SITC) Toxicity Management Working Group. J. Immunother. Cancer 2017, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anastasopoulou, A.; Ziogas, D.C.; Samarkos, M.; Kirkwood, J.M.; Gogas, H. Reactivation of tuberculosis in cancer patients following administration of immune checkpoint inhibitors: Current evidence and clinical practice recommendations. J. Immunother. Cancer 2019, 7. [Google Scholar] [CrossRef] [Green Version]
- Alessandrino, F.; Tirumani, S.H.; Krajewski, K.M.; Shinagare, A.B.; Jagannathan, J.P.; Ramaiya, N.H.; di Salvo, D.N. Imaging of hepatic toxicity of systemic therapy in a tertiary cancer centre: Chemotherapy, haematopoietic stem cell transplantation, molecular targeted therapies, and immune checkpoint inhibitors. Clin. Radiol. 2017, 72, 521–533. [Google Scholar] [CrossRef]
- Dougan, M.; Wang, Y.; Rubio-Tapia, A.; Lim, J.K. AGA Clinical Practice Update on Diagnosis and Management of Immune Checkpoint Inhibitor (ICI) Colitis and Hepatitis: Expert Review. Gastroenterology 2020. [Google Scholar] [CrossRef]
- Lamb, C.A.; Kennedy, N.A.; Raine, T.; Hendy, P.A.; Smith, P.J.; Limdi, J.K.; Hayee, B.; Lomer, M.C.E.; Parkes, G.C.; Selinger, C.; et al. British Society of Gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults. Gut 2019, 68, s1–s106. [Google Scholar] [CrossRef] [Green Version]
- Nakano, K.; Nishizawa, M.; Fukuda, N.; Urasaki, T.; Wang, X.F.; Mitani, h.; Takahashi, S. Mycophenolate mofetil as a successful treatment of corticosteroid-resistant immune checkpoint inhibitor-induced hepatitis. Oxf. Med. Case Rep. 2020, 2020, 4–5. [Google Scholar] [CrossRef]
- Horvat, T.Z.; Adel, N.G.; Dang, T.-O.; Momtaz, P.; Postow, M.A.; Callahan, M.K.; Carvajal, R.D.; Dickson, M.A.; D’Angelo, S.P.; Woo, K.M.; et al. Immune-Related adverse events, need for systemic immunosuppression, and effects on survival and time to treatment failure in patients with melanoma treated with ipilimumab at Memorial Sloan Kettering cancer center. J. Clin. Oncol. 2015, 33, 3193–3198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simonaggio, A.; Michot, J.M.; Voisin, A.L.; Le Pavec, J.; Collins, M.; Lallart, A.; Cengizalp, G.; Vozy, A.; Laparra, A.; Varga, A.; et al. Evaluation of readministration of immune checkpoint inhibitors after immune-related adverse events in patients with cancer. JAMA Oncol. 2019, 5, 1310–1317. [Google Scholar] [CrossRef] [PubMed]
- Corrigan, M.; Haydon, G.; Thompson, F.; Rajoriya, N.; Peplow, C.L.; Hubscher, S.G.; Steven, N.; Hirschfield, G.M.; Armstrong, M.J. Infliximab for the treatment of refractory immune-related hepatitis secondary to checkpoint inhibitors: A case report. JHEP Rep. 2019, 1, 66–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stroud, C.R.; Hegde, A.; Cherry, C.; Naqash, A.R.; Sharma, N.; Addepalli, S.; Cherukuri, S.; Parent, T.; Hardin, J.; Walker, P. Tocilizumab for the management of immune mediated adverse events secondary to PD-1 blockade. J. Oncol. Pharm. Pract. Off. Publ. Int. Soc. Oncol. Pharm. Pract. 2019, 25, 551–557. [Google Scholar] [CrossRef]
- Riveiro-Barciela, M.; Muñoz-Couselo, E.; Fernandez-Sojo, J.; Diaz-Mejia, N.; Parra-López, R.; Buti, M. Acute liver failure due to immune-mediated hepatitis successfully managed with plasma exchange: New settings call for new treatment strategies? J. Hepatol. 2019, 70, 564–566. [Google Scholar] [CrossRef] [Green Version]
- Cheng, R.; Cooper, A.; Kench, J.; Watson, G.; Bye, W.; McNeil, C.; Shackel, N. Ipilimumab-induced toxicities and the gastroenterologist. J. Gastroenterol. Hepatol. 2015, 30, 657–666. [Google Scholar] [CrossRef]
- Ziogas, D.C.; Gkoufa, A.; Cholongitas, E.; Diamantopoulos, P.; Anastasopoulou, A.; Ascierto, P.A.; Gogas, H. When steroids are not enough in immune-related hepatitis: Current clinical challenges discussed on the basis of a case report. J. Immunother. Cancer 2020, 8, e001322. [Google Scholar] [CrossRef]
- Brahmer, J.R.; Schneider, B.J.; Gardner, J.M. Management of immune-related adverse events in patients treated with Immune Checkpoint Inhibitor Therapy: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2018, 36, 1714–1768. [Google Scholar] [CrossRef]
- Reynolds, K.; Thomas, M.; Dougan, M. Diagnosis and Management of Hepatitis in Patients on Checkpoint Blockade. Oncologist 2018, 23, 991–997. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Autoimmune Hepatitis | ICI Hepatotoxicity | |
|---|---|---|
| Gender | Female predominant | Equal sex incidence |
| Symptoms | Malaise, jaundice | Fever, rash |
| Antibody—ANA, ASMA | Positive | Negative or low titer |
| Gamma globulin level | Increased | Normal range |
| Histology | Interface hepatitis, fibrosis | Hepatitis (lobular, pan-lobular, centrilobular, granulomatous). Portal fibrosis. |
| Cell infiltration | Plasma cell: CD4+ CD8+ | Histiocyte: CD4+ CD8+ |
| Recurrence after ICI withdrawal | Yes | No |
| Ref | CPIH (N) | CPIH Severe (N) | CS Tx | CS Type | Duration CS Tx | Non-CS Tx | Time to Normal LFT | ALT (IU) | Serology | ICI | Liver Biopsy (N) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| [42] | 17 | 11 (8- G3/3-G4) | 12 | 1 no CS 12 PR, 1 mg/kg/day 1 IV Dx 3 MPR 1 g/day | 42 (7–78) day | 1 Azathio-prine, 1 Cyclospo-rine | 31 days | 447 (59–2355) | N/A | Ipilimumab/ nivolumab/ Pembrolizumab/ indoximod/ Vemurafenib/ dabrafenib | N/A |
| [43] | 10 | 9 (7-G3, 2-G4) | 5 | N/A | N/A | 0 | 2–55 weeks | 416 (155–1735) | ANA > 1:80 (1), AMA 1:1600 (1) PBC | anti-CTLA-4 (n = 6), Anti-PD-1/PD-L1 (n = 3), combination (n = 1) | 2 granulomatous hepatitis associated with a moderate and polymorphous inflammatory infiltrate, no interface hepatitis |
| [44] | 16 | 16 | 10 | 6 spontaneous improvement 7 oral CS 0.5–1 mg/kg/day; 2 oral CS 0.2 mg/kg/day 1 IV steroid 2.5 mg/kg/day | N/A | 1 MMF | N/A | 437 (147–2289) | ANA > 1:80 (8), ASMA > 1:80 (3) | Anti-CTLA-4 (n = 7) Anti-PD-1/PD-L1 (n = 9) | the portal inflamatory infiltrate contained numerous eosinophilic polynuclear cells |
| [44] | 1 | 1 | MPR 1 mg/kg/day then Steroid | 152 days | UDCA | N/A | N/A | ANA 1:3 (20) | Nivolumab | moderate lymphocytic inflammatory infiltrate, bile duct injury; mild periportal necrosis; PD-L1 IHC, using anti-PD-L1/CD274 (clone SP142); a strong granular immuno-reactivity in the cytoplasm of Kupffer cells and hepatocytes. | |
| [45] | 29 | 19 (G3/4) | 28 | 1 no CS 28 PR 0.5–1 mg/kg/day | 35 (5–240) | 3 MMF | N/A | N/A | N/A | Combination | N/A |
| [46] | 21 | 14 (9-G3, 5-G4) | 19 | 2 no CS; 11 Pr 7 MPR1 IV DX | N/A | 8 MMF 1 Tacrolimus 1 Infliximab | 112 days | 732 (73–2857) | N/A | Combination | NO |
| [47] | 1 | 1 | 1 | MPR 500mg/day then PR 150 mg daily | 9 days then 6 weeks | MMF anti-thymocyte globulin | 37 | 1.peak 2521 2.peak 6362 | negative | Ipilimumab | NO |
| [48] | 1 | 1 | 1 | MPR 2 mg/kg/day then PR | 4 days then 6 weeks | MMF anti-thymocyte globulin | 30 | 4700 | Negative | Ipilimumab | NO |
| [49] | 3 | 3 | 3 | IV-MP 1g/kg then PR | 3-day pulse then tapering | 0 | rapidly | 886 (553–1211) | negative | Ipilimumab | NO |
| [50] | 1 | 1 | 1 | PR 1 mg/kg/day x 4 and 2 mg/kg/day | 30 days | 0 | 8 days | 250 | negative | Ipilimumab | N/A |
| [50] | 1 | 1 | 1 | PR 2 mg/kg/day | 15 days | Artificial liver plasma ex-change | LFT did not improve | 1269 | 0 | Pembro lizumab | N/A |
| [51] | 1 | G 3 | 0 | spontaneously recovered | N/A | N/A | N/A | N/A | N/A | Nivolumab | N/A |
| [52] | 1 | 1 | 1 | MPR 2 mg/kg/day and pulse therapy | N/A | Azathioprine | 30 | 539 | 0 | Nivolumab | N/A |
| [53] | 1 | 1 | 1 | MPR 2 mg/kg/day 10 days, PR 1 g/kg/day with tapering | ~90 days (all Cs tx with tape- ring) | MMF anti-thymocyte globulin | 27 | 1900 | 0 | Ipilimumab & nivolumab | N/A |
| [54] | 1 | 1 | 1 | MPR pulse for 6 day; MPR 1 g/kg/day then oral PR 1.25 mg/kg/day | 6-day pulse then tape ring | MMF | 104 | 1623 | 0 | Ipilimumab | N/A |
| [55] | 1 | G 4 | 1 | Oral MPR 0.6 mg/kg/day; half-pulse 500 mg/day | N/A | UDCA | 4 months after end of nivolu mab | 693 | 0 | Nivolumab | Portal area with inflammatory cells, including lymphocytes and eosinophils. |
| [55] | 1 | G 4 | 1 | MPR 2 mg/kg/day for 4 days; then, DX, 3 days MPR 1 g/day, followed by PR 150 mg | 7 days then tape ring | MMF anti- thymocyte globulin | Persis- ted with grade 1–2 CPIH | ~1250 | ASMS 1:1 (60) | anti-PD-1 | inflammatory infiltrate around the portal tracts and central veins, focal necrosis. PD-L1 was expressed on hepatocytes; in the infiltrating lymphocytes, PD-1 was expressed at low levels |
| [55] | 1 | 1 | 1 | MPR 2 mg/kg/day, then 4 & 6 mg/kg/day | 14 days | MMF | 55 days | ~350 | Nega- tive | nivolumab | Inflammation; eosinophilic and neutrophilic granulocytes; perivenular (zone 3) cholestasis. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malnick, S.D.H.; Abdullah, A.; Neuman, M.G. Checkpoint Inhibitors and Hepatotoxicity. Biomedicines 2021, 9, 101. https://doi.org/10.3390/biomedicines9020101
Malnick SDH, Abdullah A, Neuman MG. Checkpoint Inhibitors and Hepatotoxicity. Biomedicines. 2021; 9(2):101. https://doi.org/10.3390/biomedicines9020101
Chicago/Turabian StyleMalnick, Stephen D. H., Ali Abdullah, and Manuela G. Neuman. 2021. "Checkpoint Inhibitors and Hepatotoxicity" Biomedicines 9, no. 2: 101. https://doi.org/10.3390/biomedicines9020101
APA StyleMalnick, S. D. H., Abdullah, A., & Neuman, M. G. (2021). Checkpoint Inhibitors and Hepatotoxicity. Biomedicines, 9(2), 101. https://doi.org/10.3390/biomedicines9020101