
Role of Vitamin D in the Clinical Course of Nasal Polyposis



Abstract
:1. Introduction
2. Chronic Rhinosinusitis and Nasal Polyposis
3. Vitamin D3
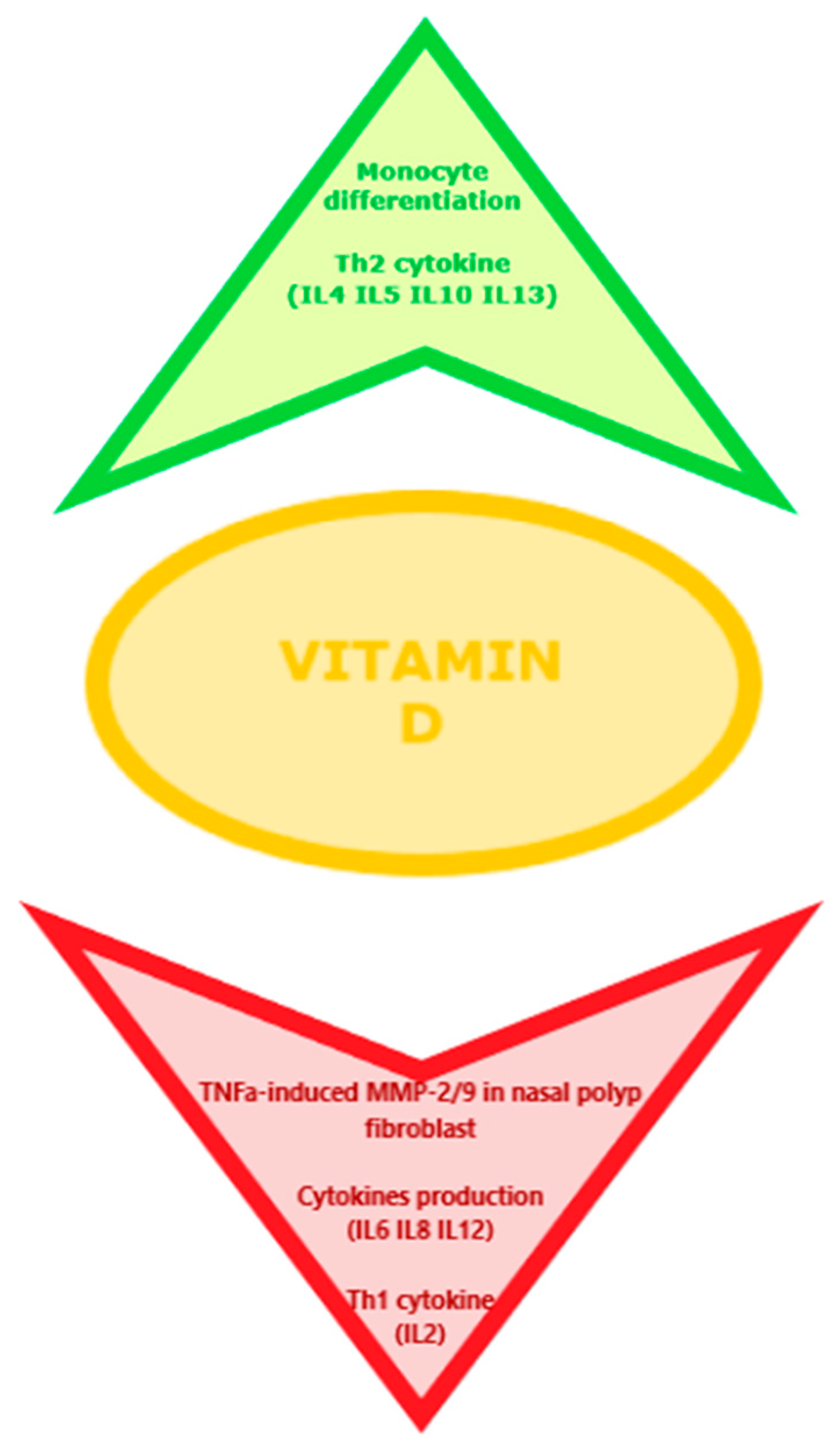
4. Immunological Correlation between VD3 and CRSwNP/CRSsNP
5. Results
6. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J.; Alobid, I.; et al. European position paper on rhinosinusitis and nasal polyps 2020. Rhinology 2020, 58 (Suppl. 29), 1–464. [Google Scholar] [CrossRef]
- Orlandi, R.R.; Kingdom, T.T.; Smith, T.L.; Bleier, B.; DeConde, A.; Luong, A.U.; Poetker, D.M.; Soler, Z.; Welch, K.C.; Wise, S.K.; et al. International consensus statement on allergy and rhinology: Rhinosinusitis 2021. Int. Forum Allergy Rhinol. 2021, 11, 213–739. [Google Scholar] [CrossRef]
- Tomassen, P.; Vandeplas, G.; Van Zele, T.; Cardell, L.-O.; Arebro, J.; Olze, H.; Förster-Ruhrmann, U.; Kowalski, M.L.; Olszewska-Ziąber, A.; Holtappels, G.; et al. Inflammatory endotypes of chronic rhinosinusitis based on cluster analysis of biomarkers. J. Allergy Clin. Immunol. 2016, 137, 1449–1456.e4. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Zhang, N.; Bo, M.; Holtappels, G.; Zheng, M.; Lou, H.; Wang, H.; Zhang, L.; Bachert, C. Diversity of TH cytokine profiles in patients with chronic rhinosinusitis: A multicenter study in Europe, Asia, and Oceania. J. Allergy Clin. Immunol. 2016, 138, 1344–1353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christensen, J.M.; Cheng, J.; Earls, P.; Gunton, J.; Sewell, W.; Sacks, R.; Harvey, R.J.R.J. Vitamin D pathway regulatory genes encoding 1α-hydroxylase and 24-hydroxylase are dysregulated in sinonasal tissue during chronic rhinosinusitis. Int. Forum Allergy Rhinol. 2016, 7, 169–176. [Google Scholar] [CrossRef]
- Sansoni, E.R.; Sautter, N.B.; Mace, J.C.; Smith, T.L.; Yawn, J.R.; Lawrence, L.A.; Schlosser, R.J.; Soler, Z.M.; Mulligan, J.K. Vitamin D3as a novel regulator of basic fibroblast growth factor in chronic rhinosinusitis with nasal polyposis. Int. Forum Allergy Rhinol. 2015, 5, 191–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saponaro, F.; Saba, A.; Zucchi, R. An Update on Vitamin D Metabolism. Int. J. Mol. Sci. 2020, 21, 6573. [Google Scholar] [CrossRef] [PubMed]
- Sassi, F.; Tamone, C.; D’Amelio, P. Vitamin D: Nutrient, Hormone, and Immunomodulator. Nutrients 2018, 10, 1656. [Google Scholar] [CrossRef] [Green Version]
- Murdaca, G.; Tonacci, A.; Negrini, S.; Greco, M.; Borro, M.; Puppo, F.; Gangemi, S. Emerging role of vitamin D in autoimmune diseases: An update on evidence and therapeutic implications. Autoimmun. Rev. 2019, 18, 102350. [Google Scholar] [CrossRef] [PubMed]
- Bakke, D.; Sun, J. Ancient Nuclear Receptor VDR with New Functions: Microbiome and Inflammation. Inflamm. Bowel Dis. 2018, 24, 1149–1154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Talsness, C.E.; Penders, J.; Jansen, E.H.J.M.; Damoiseaux, J.; Thijs, C.; Mommers, M. Influence of vitamin D on key bacterial taxa in infant microbiota in the KOALA Birth Cohort Study. PLoS ONE 2017, 12, e0188011. [Google Scholar] [CrossRef]
- Yamamoto, E.A.; Jørgensen, T.N. Relationships between Vitamin D, Gut Microbiome, and Systemic Autoimmunity. Front. Immunol. 2020, 10, 3141. [Google Scholar] [CrossRef] [PubMed]
- Ogbu, D.; Xia, E.; Sun, J. Gut instincts: Vitamin D/vitamin D receptor and microbiome in neurodevelopment disorders. Open Biol. 2020, 10, 200063. [Google Scholar] [CrossRef] [PubMed]
- Bakke, D.; Chatterjee, I.; Agrawal, A.; Dai, Y.; Sun, A.J. Regulation of Microbiota by Vitamin D Receptor: A Nuclear Weapon in Metabolic Diseases. Nucl. Recept. Res. 2018, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poole, A.; Song, Y.; Brown, H.; Hart, P.H.; Zhang, G. (Brad) Cellular and molecular mechanisms of vitamin D in food allergy. J. Cell. Mol. Med. 2018, 22, 3270–3277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, A.; Mach, N. Role of Vitamin D in the Hygiene Hypothesis: The Interplay between Vitamin D, Vitamin D Receptors, Gut Microbiota, and Immune Response. Front. Immunol. 2016, 7, 627. [Google Scholar] [CrossRef] [Green Version]
- Jin, D.; Wu, S.; Zhang, Y.G.; Lu, R.; Xia, Y.; Dong, H.; Sun, J. Lack of Vitamin D Receptor Causes Dysbiosis and Changes the Functions of the Murine Intestinal Microbiome. Clin. Ther. 2015, 37, 996–1009. [Google Scholar] [CrossRef]
- Naderpoor, N.; Mousa, A.; Arango, L.F.G.; Barrett, H.L.; Nitert, M.D.; De Courten, B. Effect of Vitamin D Supplementation on Faecal Microbiota: A Randomised Clinical Trial. Nutrients 2019, 11, 2888. [Google Scholar] [CrossRef] [Green Version]
- Lombardi, C.; Passalacqua, G.; Italian Vitamin D Allergy Group. Vitamin D levels and allergic diseases. An italian cross-sectional multicenter survey. Eur. Ann. Allergy Clin. Immunol. 2017, 49, 75–79. [Google Scholar] [PubMed]
- Heine, R.G. Food Allergy Prevention and Treatment by Targeted Nutrition. Ann. Nutr. Metab. 2018, 72, 33–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murdaca, G.; Gerosa, A.; Paladin, F.; Petrocchi, L.; Banchero, S.; Gangemi, S. Vitamin D and Microbiota: Is There a Link with Allergies? Int. J. Mol. Sci. 2021, 22, 4288. [Google Scholar] [CrossRef] [PubMed]
- Erdag, O.; Turan, M.; Ucler, R.; Berkoz, M.; Garca, M.F.; Bozan, N.; Kıroglu, A.F.; Cankaya, H. Is Nasal Polyposis Related to Levels of Serum Vitamin D and Vitamin D Receptor Gene Expression? Med Sci. Monit. 2016, 22, 4636–4643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bozzetto, S.; Carraro, S.; Giordano, G.; Boner, A.; Baraldi, E. Asthma, allergy and respiratory infections: The vitamin D hypothesis. Allergy 2011, 67, 10–17. [Google Scholar] [CrossRef]
- Ozkara, S.; Keles, E.; Ilhan, N.; Gungor, H.; Kaygusuz, I.; Alpay, H.C. The relationship between Th1/Th2 balance and 1α,25-dihydroxyvitamin D3 in patients with nasal polyposis. Eur. Arch. Oto-Rhino-Laryngol. 2012, 269, 2519–2524. [Google Scholar] [CrossRef]
- Sikorska-Szaflik, H.; Sozańska, B. The Role of Vitamin D in Respiratory Allergies Prevention. Why the Effect Is so Difficult to Disentangle? Nutrients 2020, 12, 1801. [Google Scholar] [CrossRef]
- Bonanno, A.; Gangemi, S.; La Grutta, S.; Malizia, V.; Riccobono, L.; Colombo, P.; Cibella, F.; Profita, M. 25-Hydroxyvitamin D, IL-31, and IL-33 in Children with Allergic Disease of the Airways. Mediat. Inflamm. 2014, 2014, 520241. [Google Scholar] [CrossRef] [Green Version]
- Mirzakhani, H.; Al-Garawi, A.; Weiss, S.T.; Litonjua, A.A. Vitamin D and the development of allergic disease: How important is it? Clin. Exp. Allergy 2014, 45, 114–125. [Google Scholar] [CrossRef] [Green Version]
- Chandrakar, A.K.; Alexander, A.; Rajendiran, K.; Ramasamy, K. 25-Hydroxyl Vitamin D Deficiency in Nasal Polyposis. Mediat. Inflamm. 2014, 2014, 520241. [Google Scholar] [CrossRef]
- Mostafa, B.; Taha, M.; Hamid, T.A.; Omran, A.; Lotfi, N. Evaluation of vitamin D levels in allergic fungal sinusitis, chronic rhinosinusitis, and chronic rhinosinusitis with polyposis. Int. Forum Allergy Rhinol. 2015, 6, 185–190. [Google Scholar] [CrossRef]
- Kalińczak-Górna, P.; Radajewski, K.; Burduk, P. Relationship between the Severity of Inflammatory Changes in Chronic Sinusitis and the Level of Vitamin D before and after the FESS Procedure. J. Clin. Med. 2021, 10, 2836. [Google Scholar] [CrossRef] [PubMed]
- Konstantinidis, I.; Fotoulaki, M.; Iakovou, I.; Chatziavramidis, A.; Mpalaris, V.; Shobat, K.; Markou, K. Vitamin D3 Deficiency and its Association with Nasal Polyposis in Patients with Cystic Fibrosis and Patients with Chronic Rhinosinusitis. Am. J. Rhinol. Allergy 2017, 31, 395–400. [Google Scholar] [CrossRef]
- Rostkowska-Nadolska, B.; Sliupkas-Dyrda, E.; Potyka, J.; Kusmierz, D.; Fraczek, M.; Krecicki, T.; Kubik, P.; Zatonski, M.; Latocha, M. Vitamin D derivatives: Calcitriol and tacalcitol inhibits interleukin-6 and interleukin-8 expression in human nasal polyp fibroblast cultures. Adv. Med. Sci. 2010, 55, 86–92. [Google Scholar] [CrossRef]
- Tomaszewska, M.; Sarnowska, E.; Rusetska, N.; Kowalik, K.; Sierdzinski, J.; Siedlecki, J.A.; Badmaev, V.; Stohs, S.J.; Popko, M. Role of Vitamin D and Its Receptors in the Pathophysiology of Chronic Rhinosinusitis. J. Am. Coll. Nutr. 2019, 38, 108–118. [Google Scholar] [CrossRef]
- Carroll, W.W.; Schlosser, R.J.; O’Connell, B.P.; Soler, Z.M.; Mulligan, J.K. Vitamin D deficiency is associated with increased human sinonasal fibroblast proliferation in chronic rhinosinusitis with nasal polyps. Int. Forum Allergy Rhinol. 2016, 6, 605–610. [Google Scholar] [CrossRef]
- Mulligan, J.K.; Pasquini, W.N.; Carroll, W.W.; Williamson, T.; Reaves, N.; Patel, K.J.; Mappus, E.; Schlosser, R.J.; Atkinson, C. Dietary vitamin D3 deficiency exacerbates sinonasal inflammation and alters local 25(OH)D3 metabolism. PLoS ONE 2017, 12, e0186374. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.-F.; Tai, C.-F.; Chien, C.-Y.; Chiang, F.-Y.; Chen, J.Y.-F. Vitamin D decreases the secretion of matrix metalloproteinase-2 and matrix metalloproteinase-9 in fibroblasts derived from Taiwanese patients with chronic rhinosinusitis with nasal polyposis. Kaohsiung J. Med Sci. 2015, 31, 235–240. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.-F.; Lee, C.-H.; Chien, C.-Y.; Chen, J.Y.-F.; Chiang, F.-Y.; Tai, C.-F. Serum 25-hydroxyvitamin D Levels are Lower in Chronic Rhinosinusitis with Nasal Polyposis and are Correlated with Disease Severity in Taiwanese Patients. Am. J. Rhinol. Allergy 2013, 27, e162–e165. [Google Scholar] [CrossRef]
- Zand, V.; Baradaranfar, M.; Vaziribozorg, S.; Mandegari, M.; Mansourimanesh, M.; Saeidieslami, N. Correlation of Serum Vitamin D Levels with Chronic Rhinosinusitis Disease Severity. Iran J. Otorhinolaryngol. 2020, 32, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Yang, Y.; Chen, H. Vitamin D deficiency are associated with subjective disease severity in Chinese patients with chronic rhinosinusitis with nasal polyps. Am. J. Otolaryngol. 2019, 40, 36–39. [Google Scholar] [CrossRef]
- Schlosser, R.J.; Soler, Z.M.; Schmedes, G.W.; Storck, K.; Mulligan, J.K. Impact of vitamin D deficiency upon clinical presentation in nasal polyposis. Int. Forum Allergy Rhinol. 2014, 4, 196–199. [Google Scholar] [CrossRef] [PubMed]
- Hashemian, F.; Sadegh, S.; Jahanshahi, J.; Rabiei, M.A.S.; Hashemian, F. Effects of Vitamin D Supplementation on Recurrence of Nasal Polyposis after Endoscopic Sinus Surgery. Iran J. Otorhinolaryngol. 2020, 32, 21–28. [Google Scholar] [CrossRef]
- Tian, H.-Q.; Cheng, L. The role of vitamin D in allergic rhinitis. Asia Pac. Allergy 2017, 7, 65–73. [Google Scholar] [CrossRef] [Green Version]
- Muehleisen, B.; Gallo, R.L. Vitamin D in allergic disease: Shedding light on a complex problem. J. Allergy Clin. Immunol. 2013, 131, 324–329. [Google Scholar] [CrossRef] [PubMed]
- Bakhshaee, M.; Sharifian, M.; Esmatinia, F.; Rasoulian, B.; Mohebbi, M. Therapeutic effect of vitamin D supplementation on allergic rhinitis. Eur. Arch. Oto-Rhino-Laryngol. 2019, 276, 2797–2801. [Google Scholar] [CrossRef] [PubMed]
- Bunyavanich, S.; Rifas-Shiman, S.L.; Platts-Mills, T.A.; Workman, L.; Sordillo, J.E.; Camargo, C.A.; Gillman, M.W.; Gold, D.R.; Litonjua, A.A. Prenatal, perinatal, and childhood vitamin D exposure and their association with childhood allergic rhinitis and allergic sensitization. J. Allergy Clin. Immunol. 2016, 137, 1063–1070.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bener, A.; Ehlayel, M.S.; Bener, H.Z.; Hamid, Q. The impact of Vitamin D deficiency on asthma, allergic rhinitis and wheezing in children: An emerging public health problem. J. Fam. Community Med. 2014, 21, 154–161. [Google Scholar] [CrossRef] [Green Version]
- Wjst, M.; Hypponen, E. Vitamin D serum levels and allergic rhinitis. Allergy 2007, 62, 1085–1086. [Google Scholar] [CrossRef] [PubMed]
- Penna, G.; Adorini, L. 1α,25-Dihydroxyvitamin D3Inhibits Differentiation, Maturation, Activation, and Survival of Dendritic Cells Leading to Impaired Alloreactive T Cell Activation. J. Immunol. 2000, 164, 2405–2411. [Google Scholar] [CrossRef] [Green Version]
- Farsani, Z.S.; Behmanesh, M.; Sahraian, M.A. Interleukin-10 but not transforming growth factor-β1 gene expression is up-regulated by vitamin D treatment in multiple sclerosis patients. J. Neurol. Sci. 2015, 350, 18–23. [Google Scholar] [CrossRef]
- Sudiro, M.; Lestari, B.W.; Madiadipoera, T.; Setiabudiawan, B.; Boesoirie, T.S. Vitamin D Deficiency Is Correlated with Severity of Allergic Rhinitis. OALib 2017, 04, 1–9. [Google Scholar] [CrossRef]
- Vatankhah, V.; Lotfizadeh, M.; Iranpoor, H.; Jafari, F.; Khazraei, H. Comparison vitamin D serum levels in allergic rhinitis patients with normal population. Rev. Franç. d’Allergol. 2016, 56, 539–543. [Google Scholar] [CrossRef]
- Alnori, H.; Alassaf, F.A.; Alfahad, M.; Qazzaz, M.E.; Jasim, M.; Abed, M.N. Vitamin D and Immunoglobulin E Status in Allergic Rhinitis Patients Compared to Healthy People. J. Med. Life 2020, 13, 463–468. [Google Scholar] [CrossRef]
- Sun, J. Dietary Vitamin D, Vitamin D Receptor, and Microbiome. Curr. Opin. Clin. Nutr. Metab. Care 2018, 21, 471–474. [Google Scholar] [CrossRef]
- Willits, E.K.; Wang, Z.; Jin, J.; Patel, B.; Motosue, M.; Bhagia, A.; Almasri, J.; Erwin, P.J.; Kumar, S.; Joshi, A.Y.; et al. Vitamin D and food allergies in children: A systematic review and meta-analysis. Allergy Asthma Proc. 2017, 38, 21–28. [Google Scholar] [CrossRef]
- Camargo, C.A., Jr.; Ganmaa, D.; Sidbury, R.; Erdenedelger, K.; Radnaakhand, N.; Khandsuren, B. Randomized trial of vitamin D supplementation for winter-related atopic dermatitis in children. J. Allergy Clin. Immunol. 2014, 134, 831–835. [Google Scholar] [CrossRef] [PubMed]
- Javanbakht, M.H.; Keshavarz, S.A.; Djalali, M.; Siassi, F.; Eshraghian, M.R.; Firooz, A.; Seirafi, H.; Ehsani, A.H.; Chamari, M.; Mirshafiey, A. Randomized controlled trial using vitamins E and D supplementation in atopic dermatitis. J. Dermatol. Treat. 2010, 22, 144–150. [Google Scholar] [CrossRef]
- Deeb, K.K.; Trump, D.L.; Johnson, C.S. Vitamin D signalling pathways in cancer: Potential for anticancer therapeutics. Nat. Rev. Cancer 2007, 7, 684–700. [Google Scholar] [CrossRef]
- Zeljic, K.; Supic, G.; Magic, Z. New insights into vitamin D anticancer properties: Focus on miRNA modulation. Mol. Genet. Genom. 2017, 292, 511–524. [Google Scholar] [CrossRef] [PubMed]
- Bachert, C.; Zhang, N.; Hellings, P.W.; Bousquet, J. Endotype-driven care pathways in patients with chronic rhinosinusitis. J. Allergy Clin. Immunol. 2018, 141, 1543–1551. [Google Scholar] [CrossRef] [PubMed]
- Fujieda, S.; Imoto, Y.; Kato, Y.; Ninomiya, T.; Tokunaga, T.; Tsutsumiuchi, T.; Yoshida, K.; Kidoguchi, M.; Takabayashi, T. Eosinophilic chronic rhinosinusitis. Allergol. Int. 2019, 68, 403–412. [Google Scholar] [CrossRef]
- Lou, H.; Zhang, N.; Bachert, C.; Zhang, L. Highlights of eosinophilic chronic rhinosinusitis with nasal polyps in definition, prognosis, and advancement. Int. Forum Allergy Rhinol. 2018, 8, 1218–1225. [Google Scholar] [CrossRef] [PubMed]
- Aslan, F.; Altun, E.; Paksoy, S.; Turan, G. Could Eosinophilia predict clinical severity in nasal polyps? Multidiscip. Respir. Med. 2017, 12, 21. [Google Scholar] [CrossRef] [Green Version]
- Wang, K.; Deng, J.; Yang, M.; Chen, Y.; Chen, F.; Gao, W.-X.; Lai, Y.; Shi, J.; Sun, Y. Concordant systemic and local eosinophilia relates to poorer disease control in patients with nasal polyps. World Allergy Organ. J. 2019, 12, 100052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bochner, B.S.; Stevens, W.W. Biology and Function of Eosinophils in Chronic Rhinosinusitis with or without Nasal Polyps. Allergy Asthma Immunol. Res. 2021, 13, 8–22. [Google Scholar] [CrossRef] [PubMed]
- Nasta, M.S.; Chatzinakis, V.A.; Georgalas, C. Updates on current evidence for biologics in chronic rhinosinusitis. Curr. Opin. Otolaryngol. Head Neck Surg. 2020, 28, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Kartush, A.G.; Schumacher, J.K.; Shah, R.; Patadia, M.O. Biologic Agents for the Treatment of Chronic Rhinosinusitis with Nasal Polyps. Am. J. Rhinol. Allergy 2018, 33, 203–211. [Google Scholar] [CrossRef]
- Brown, W.C.; Senior, B. A Critical Look at the Efficacy and Costs of Biologic Therapy for Chronic Rhinosinusitis with Nasal Polyposis. Curr. Allergy Asthma Rep. 2020, 20, 16. [Google Scholar] [CrossRef]


{kind=link}
| Author | Year | Type of Study | N Patients | Comorbidities | Objective | Outcome |
|---|---|---|---|---|---|---|
| Ali Faghih Habibi, Hooshang Gerami, et al. | 2019 | Case-Control Study | 117 | compare serum level of 25-OH-VitD in CRSw/sNP patients and control groups | serum 25-OH-VitD was significantly lower in CRS patients | |
| Ankur Kumar Chandrakar, Arun Alexander et al. | 2014 | cross-sectional study | 80 patients with nasal polyposis and 80 healthy subjects | Atopy | Assessment of the levels of 25-hydroxy vitamin D and high sensitivity C-reactive protein (hs-CRP) in patients with nasal polyposis and control subjects, and identified their association with disease severity in nasal polyposis. | The severity of polyposis correlated negatively with serum levels of 25-hydroxy vitamin D and positively with hs-CRP |
| Anna Bonanno, Sebastiano Gangemi et al. | 2014 | Case-control study | 28 controls (HC), 11 allergic rhinitis (AR) patients, and 35 allergic asthma with rhinitis (AAR) patients | Allergy and asthma | whether low vitamin D is linked with circulating IL-31 and IL-33 in children with allergic disease of the airways | low levels of 25(OH) Vit D might represent a risk factor for the development of concomitant asthma and rhinitis in children with allergic disease of the airways independently of IL-31/IL-33 Th2 activity |
| Arash Shahangian, Rodney J.Schlosser | 2016 | Review | 0 | Explore some of the contributions of VD3 to chronic rhinosinusitis with nasal polyposis and its role as a disease-modifying agent | There is likely a role for VD3 use as a disease-modifying agent in treatment of patients with recalcitrant CRSwNP | |
| B Rostkowska-Nadolska, E Sliupkas-Dyrda et al. | 2010 | investigate the influence of calcitriol and tacalcitol on the secretion of IL-6 and IL-8 by fibroblasts derived from NP | Calcitriol and tacalcitol are capable of affecting pro-inflammatory cytokine (IL-6 and IL-8) levels in NP cultures | |||
| Badr El-Din Mostafa, Mohammed Shehata Taha et al. | 2016 | Case-control study | 74 | Measure VD3 levels in patients with AFRS and chronic rhinosinusitis (CRS) | Serum level of VD3 in patients with CRSwNP and AFRS is significantly lower than that of patients with CRSsNP and control subjects | |
| Binayak Baruah, Ajay Gupta et al. | 2020 | retrospective 1-year study | 200 | Comparison of incidence of vitamin D deficiency in CRS patients to normal population and evaluation of the beneficial role of its supplementation in treatment | Higher prevalence of vitamin D deficiency in CRS patients and that vitamin D supplementation went a long way in alleviating their symptoms | |
| Bo Li, Miaowei Wang et al. | 2021 | meta-analysis | 337 chronic rhinosinusitis patients and 179 healthy controls | asthma and/or atopic status | Compare the serum vitamin D levels between patients with chronic rhinosinusitis and healthy controls and evaluate the associations of vitamin D level with its occurrence | Detection of a significant association between lower serum vitamin D status and chronic rhinosinusitis, especially in chronic rhinosinusitis with nasal polyps patients |
| E Ritter Sansoni, Nathan B Sautter et al. | 2015 | Case-control study | 57 (CRSsNP (n = 31), CRSwNP (n = 14), and controls (n = 12)) | Correlation between 25-VD3 levels and sinonasal mucus monocyte chemoattractant protein-1 (MCP-1), regulated upon activation normal T cell expressed and secreted (RANTES), and basic fibroblast growth factor (bFGF) levels in patients with CRS | 25-VD3 may play a role in regulation of RANTES and bFGF expression in CRSwNP. This may occur through regulation of NP fibroblasts or other immune cells | |
| F Bavi, R Movahed, M Salehi, et al. | 2019 | cross-sectional study | 166 cases with CRSwNP and 172 healthy subjects | Serum vitamin D3 levels in patients with CRSwNP and its association with disease severity | Disease severity, based on imaging, endoscopic and clinical criteria, was inversely associated with serum vitamin D levels | |
| Farnaz Hashemian, Sonya Sadegh, et al. | 2020 | triple-blind placebocontrolled clinical trial | Investigate the effects of oral VD3 on the recurrence of polyposis after FESS | Efficacy and safety of vitamin D supplementation in the reduction of polyposis recurrence after FESS in patients with CRSwNP | ||
| Feng Wang, Yang Yang, Haihong Chen | 2019 | Retrospective analysis of collected data | Atopic status and asthma | Serum vitamin D level in patients with chronic rhinosinusitis with nasal polyps and its correlation with the disease severity | Serum 25-hydroxyvitamin D3 levels are lower in Chinese CRSwNP patients. These 25-hydroxyvitamin D3 levels are associated with SNOT-22 score. Preoperative 25-hydroxyvitamin D3 level may impact the symptom improvement after surgery | |
| Iordanis Konstantinidis, Maria Fotoulaki et al. | 2017 | Case-control study | 152 adult participants were included in five phenotypic groups: CF with NP (CFwNP) (n = 27), CF without NP (CFsNP) (n = 31), CRS with NP (CRSwNP) (n = 32), CRS without NP (CRSsNP) (n = 30), and controls (n = 32) | Investigate if deficiency of VD3 is associated with the presence of NP in patients with cystic fibrosis (CF) and patients with chronic rhinosinusitis (CRS) | VD3 deficiency seemed to be associated with the presence of nasal polyps in the patients with CRS and in the patients with CF in a similar manner | |
| Jenna M Christensen, Jasmine Cheng et al. | 2017 | cross-sectional study | 31 patients (8 CRSsNP, 10 CRSwNP, and 13 controls) | Determine expression of genes encoding the vitamin D receptor (VDR), 25-hydroxylase (CYP2R1), 1α-hydroxylase (CYP27B1), and 24-hydroxylase (CYP24A1) | Vitamin D may be dysregulated at multiple levels, with decreased transcription of the metabolic gene CYP27B1 and increased transcription of the catabolic gene CYP24A1 observed | |
| Jennifer K Mulligan, Whitney N Pasquini et al. | 2017 | Observational studies | Impact of VD3 deficiency on inflammation and VD3 metabolism in an Aspergillus fumigatus (Af) mouse model of chronic rhinosinusitis (Af-CRS) | VD3 deficiency causes changes in sinonasal immunity. Both VD3 deficiency and Af-CRS were associated with reductions in local levels of the active VD3 metabolite even with adequate circulating levels | ||
| Ling-Feng Wang, Chih-Feng Tai et al. | 2015 | Observational study | Understand the role of vitamin D in chronic rhinosinusitis with nasal polyps (CRSwNP) by investigating its effect on the secretion of matrix metalloproteinase-2 (MMP-2) and MMP-9 | Vitamin D derivatives could significantly inhibit TNF-α-induced MMP-2 and MMP-9 secretion in nasal polyp-derived fibroblasts | ||
| Ling-Feng Wang, Chih-Hung Lee et al. | 2013 | Case-control study | Determine if serum Vitamin D level is lower in chronic rhinosinusitis with nasal polyposis (CRSwNP) patients and if low serum Vitamin D level is correlated with the severity of CRSwNP | A significantly lower vitamin D level was found in a group of Taiwanese CRSwNP patients, which revealed an association with greater nasal polyp size | ||
| Malgorzata Tomaszewska, Elzbieta Sarnowska et al. | 2019 | Case-control study | 52 patients with CRS without nasal polyps (sNP), 55 with CRS with nasal polyps (wNP), and 59 in the control group | Atopy | Relationships between the total concentration of vitamin D, vitamin D receptor (VDR) expression, 1α-hydroxylase expression, and clinical data, including age, gender, Sino-Nasal Outcome Test (SNOT-22), computerized tomography (CT) scan, allergy status, and vitamin D supplementation in CRS patients with (CRSwNP) and without nasal polyps (CRSsNP), and in a control group | vitamin D and its receptor and enzymes may play a role in CRS |
| Murdaca, G., Tonacci, A. et al. | 2019 | update | Find a correlation between vitamin D levels and its effect upon several autoimmune diseases | Inverse association between vitamin D and the development of several autoimmune diseases | ||
| Omer Erdag, Mahfuz Turan, et al. | 2016 | case-control study | 46 subjects with NP (NP group) and 40 volunteers (control group) | Assess the relation between levels of vitamin D receptor (VDR) gene expression and serum vitamin D with NP | VDR gene expression may be associated with the pathogenesis or progression of NP | |
| Patrick J Stokes, Joanne Rimmer | 2016 | systematic review | 539 | asthma and/or atopic status | Relationship among serum VD3 levels, CRS phenotype, and disease severity by using outcome assessments | Significantly lower VD3 levels in the polypoid phenotypes of CRS compared with controls. Low VD3 levels were often associated with an increased degree of inflammation |
| Pooja Thakur, Praneeth Potluri | 2020 | prospective casecontrol study | Evaluate the association of serum vitamin D levels with chronic rhinosinusitis (CRS) in population residing at high altitudes and to assess its correlation with severity of CRS | Lower vitamin D level is associated with CRS, irrespective of presence or absence of nasal polyposis in adults residing at high altitudes. Vitamin D is an independent predictive factor for CRS. There is an inverse moderate correlation of severity of CRS with vitamin D | ||
| Rodney J. Schlosser, Zachary M. Soler, et al. | 2014 | Retrospective review | Determine if CRSwNP populations are at risk for vitamin D3 (VD3) deficiency and if VD3 levels correlate with radiographic measures of disease severity or eosinophilia | VD3 insufficiency/deficiency is common in CRSwNP patients, especially those of African American race. Lower levels of VD3 are associated with worse LMS on CT | ||
| Sule Ozkara, Erol Keles, Nevin Ilhan et al. | 2012 | case-control study | 60 adult patients and 40 healthy volunteers | Allergic rhinitis | Study Th1/Th2 cell balance by measuring the levels of cytokines IL-4, IL-10, and IFN-γ and determine the correlation between Th1/Th2 cell balance and 1α,25-dihydroxyvitamin D(3) | vitamin D is effective on Th1/Th2 balance in patients with allergic rhinitis and that there is a significant relation between vitamin D deficiency and allergy |
| Vahid Zand, Mohammadhossein Baradaranfar et al. | 2020 | cross-sectional study | 93 patients suffering from chronic rhino sinusitis with nasal polyposis (CRS w NP) | Investigate the association between the serum vitamin D levels and severity of disease in chronic rhino sinusitis (CRS) patients | There was a significant relationship between the serum vitamin D levels and severity of disease in patients with CRS w NP | |
| William W Carroll, Rodney J Schlosser et al. | 2016 | Case-control study | 15 patients with CRSwNP and 12 control subjects | Investigate VD3 deficiency and HSNF proliferation in CRSwNP | VD3 deficiency is associated with increased HSNF proliferation in CRSwNP |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murdaca, G.; Paladin, F.; Gangemi, S. Role of Vitamin D in the Clinical Course of Nasal Polyposis. Biomedicines 2021, 9, 855. https://doi.org/10.3390/biomedicines9080855
Murdaca G, Paladin F, Gangemi S. Role of Vitamin D in the Clinical Course of Nasal Polyposis. Biomedicines. 2021; 9(8):855. https://doi.org/10.3390/biomedicines9080855
Chicago/Turabian StyleMurdaca, Giuseppe, Francesca Paladin, and Sebastiano Gangemi. 2021. "Role of Vitamin D in the Clinical Course of Nasal Polyposis" Biomedicines 9, no. 8: 855. https://doi.org/10.3390/biomedicines9080855
APA StyleMurdaca, G., Paladin, F., & Gangemi, S. (2021). Role of Vitamin D in the Clinical Course of Nasal Polyposis. Biomedicines, 9(8), 855. https://doi.org/10.3390/biomedicines9080855