
Early Phase Increase in Serum TIMP-1 in Patients with Acute Encephalopathy with Biphasic Seizures and Late Reduced Diffusion
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects and Sample Collection
2.2. MMP-9 and TIMP-1 Assays
2.3. Cytokine Assay
2.4. Statistical Analysis
2.5. Ethics
3. Results
3.1. Clinical Characteristics
3.2. Serum Concentrations of MMP-9 and TIMP-1
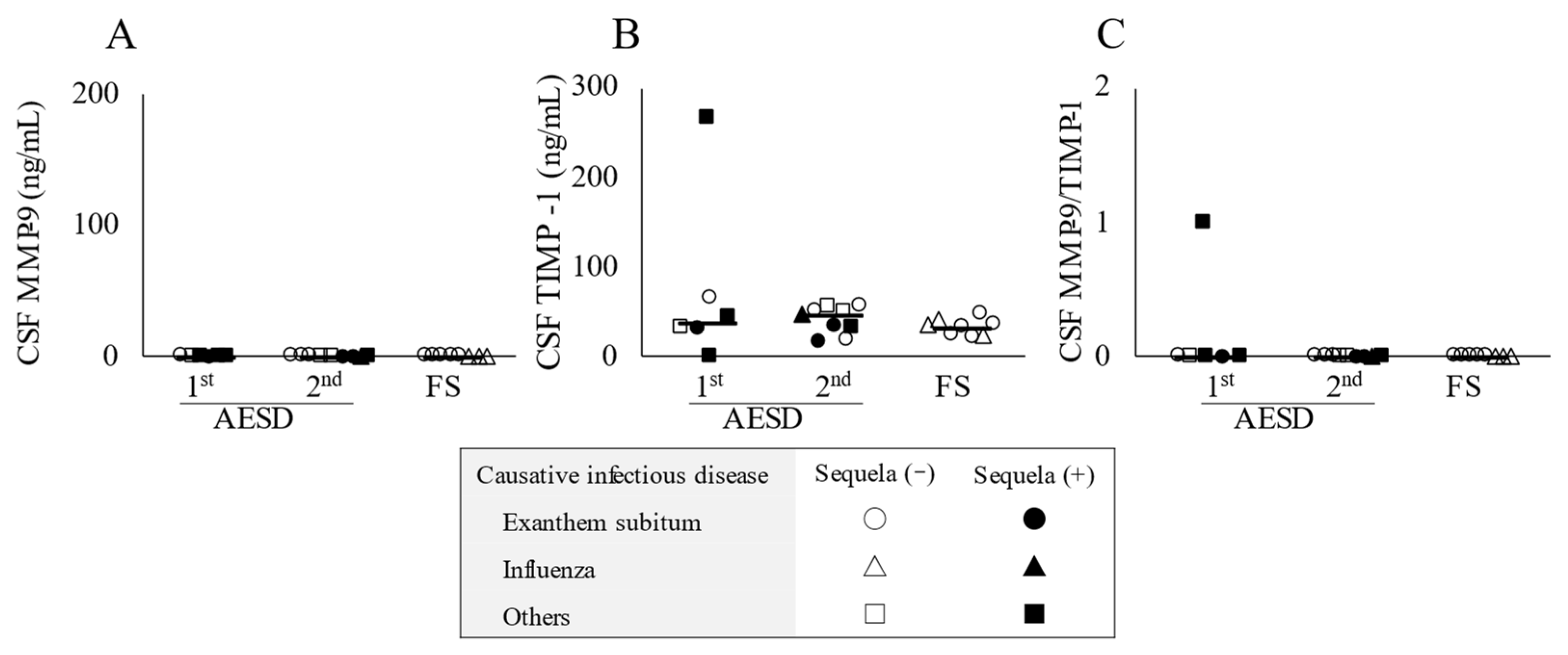
3.3. CSF Concentrations of MMP-9 and TIMP-1
3.4. Relationship between Serum Concentrations of MMP-9 and TIMP-1
3.5. Relationship between Serum TIMP-1 and CSF NSE Concentrations
3.6. Relationship between Serum Concentrations of TIMP-1 and Serum or CSF Concentrations of Seven Types of Cytokines
3.7. Cytokine Profiles in Serum and CSF
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hoshino, A.; Saitoh, M.; Oka, A.; Okumura, A.; Kubota, M.; Saito, Y.; Takanashi, J.; Hirose, S.; Yamagata, T.; Yamanouchi, H.; et al. Epidemiology of acute encephalopathy in Japan, with emphasis on the association of viruses and syndromes. Brain Dev. 2012, 34, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Kawamura, Y.; Sugata, K.; Ihira, M.; Mihara, T.; Mutoh, T.; Asano, Y.; Yoshikawa, T. Different characteristics of human herpesvirus 6 encephalitis between primary infection and viral reactivation. J. Clin. Virol. 2011, 51, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Hatanaka, M.; Kashiwagi, M.; Tanabe, T.; Nakahara, H.; Ohta, K.; Tamai, H. Overlapping MERS and mild AESD caused by HHV-6 infection. Brain Dev. 2015, 37, 334–338. [Google Scholar] [CrossRef] [PubMed]
- Asahi, M.; Wang, X.; Mori, T.; Sumii, T.; Jung, J.C.; Moskowitz, M.A.; Fini, M.E.; Lo, E.H. Effects of matrix metalloproteinase-9 gene knock-out on the proteolysis of blood-brain barrier and white matter components after cerebral ischemia. J. Neurosci. 2001, 21, 7724–7732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandooren, J.; Van den Steen, P.E.; Opdenakker, G. Biochemistry and molecular biology of gelatinase B or matrix metalloproteinase-9 (MMP-9): The next decade. Crit. Rev. Biochem. Mol. Biol. 2013, 48, 222–272. [Google Scholar] [CrossRef] [PubMed]
- Gomis-Rüth, F.X.; Maskos, K.; Betz, M.; Bergner, A.; Huber, R.; Suzuki, K.; Yoshida, N.; Nagase, H.; Brew, K.; Bourenkov, G.P.; et al. Mechanism of inhibition of the human matrix metalloproteinase stromelysin-1 by TIMP-1. Nature 1997, 389, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Ichiyama, T.; Morishima, T.; Kajimoto, M.; Matsushige, T.; Matsubara, T.; Furukawa, S. Matrix metalloproteinase-9 and tissue inhibitors of metalloproteinases 1 in influenza-associated encephalopathy. Pediatr. Infect. Dis. J. 2007, 26, 542–544. [Google Scholar] [CrossRef]
- Shiraishi, M.; Ichiyama, T.; Matsushige, T.; Iwaki, T.; Iyoda, K.; Fukuda, K.; Makata, H.; Matsubara, T.; Furukawa, S. Soluble tumor necrosis factor receptor 1 and tissue inhibitor of metalloproteinase-1 in hemolytic uremic syndrome with encephalopathy. J. Neuroimmunol. 2008, 196, 147–152. [Google Scholar] [CrossRef]
- Lorente, L.; Martín, M.M.; Ramos, L.; Argueso, M.; Cáceres, J.J.; Solé-Violán, J.; Jiménez, A.; Borreguero-León, J.M.; González-Rivero, A.F.; Orbe, J.; et al. Persistently high circulating tissue inhibitor of matrix metalloproteinase-1 levels in non-survivor brain trauma injury patients. J. Crit. Care 2019, 51, 117–121. [Google Scholar] [CrossRef]
- Lorente, L.; Martín, M.M.; Ramos, L.; Argueso, M.; Cáceres, J.J.; Solé-Violán, J.; Jiménez, A.; Borreguero-León, J.M.; González-Rivero, A.F.; Orbe, J.; et al. High serum levels of tissue inhibitor of matrix metalloproteinase-1 during the first week of a malignant middle cerebral artery infarction in non-surviving patients. BMC Neurol. 2019, 19, 167. [Google Scholar] [CrossRef]
- Lorente, L.; Martín, M.M.; Ramos, L.; Argueso, M.; Cáceres, J.J.; Solé-Violán, J.; Jiménez, A. High Serum Tissue Inhibitor of Matrix Metalloproteinase-1 Levels and Mortality in Patients with Spontaneous Intracerebral Hemorrhage. World Neurosurg. 2020, 134, e476–e480. [Google Scholar] [CrossRef] [PubMed]
- Jordakieva, G.; Budge-Wolfram, R.M.; Budinsky, A.C.; Nikfardjam, M.; Delle-Karth, G.; Girard, A.; Godnic-Cvar, J.; Crevenna, R.; Heinz, G. Plasma MMP-9 and TIMP-1 levels on ICU admission are associated with 30-day survival. Wien Klin Wochenschr 2021, 133, 86–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; McCluskey, K.; Fujii, K.; Wahl, L.M. Differential regulation of monocyte matrix metalloproteinase and TIMP-1 production by TNF-alpha, granulocyte-macrophage CSF, and IL-1 beta through prostaglandin-dependent and -independent mechanisms. J. Immunol. 1998, 161, 3071–3076. [Google Scholar] [PubMed]
- Wurster, A.L.; Rodgers, V.L.; Satoskar, A.R.; Whitters, M.J.; Young, D.A.; Collins, M.; Grusby, M.J. Interleukin 21 is a T helper (Th) cell 2 cytokine that specifically inhibits the differentiation of naive Th cells into interferon gamma-producing Th1 cells. J. Exp. Med. 2002, 196, 969–977. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, K.; Sonoda, S.; Higashi, K.; Kondo, T.; Takahashi, H.; Takahashi, M.; Yamanishi, K. Predominant CD4 T-lymphocyte tropism of human herpesvirus 6-related virus. J. Virol. 1989, 63, 3161–3163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorente, L.; Martín, M.M.; Labarta, L.; Díaz, C.; Solé-Violán, J.; Blanquer, J.; Orbe, J.; Rodríguez, J.A.; Jiménez, A.; Borreguero-León, J.M.; et al. Matrix metalloproteinase-9, -10, and tissue inhibitor of matrix metalloproteinases-1 blood levels as biomarkers of severity and mortality in sepsis. Crit. Care 2009, 13, R158. [Google Scholar] [CrossRef] [Green Version]
- Lacraz, S.; Nicod, L.P.; Chicheportiche, R.; Welgus, H.G.; Dayer, J.M. IL-10 inhibits metalloproteinase and stimulates TIMP-1 production in human mononuclear phagocytes. J. Clin. Invest. 1995, 96, 2304–2310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnatty, R.N.; Taub, D.D.; Reeder, S.P.; Turcovski-Corrales, S.M.; Cottam, D.W.; Stephenson, T.J.; Rees, R.C. Cytokine and chemokine regulation of proMMP-9 and TIMP-1 production by human peripheral blood lymphocytes. J. Immunol. 1997, 158, 2327–2333. [Google Scholar] [PubMed]
- Frenkel, N.; Schirmer, E.C.; Wyatt, L.S.; Katsafanas, G.; Roffman, E.; Danovich, R.M.; June, C.H. Isolation of a new herpesvirus from human CD4+ T cells. Proc. Natl. Acad. Sci. USA 1990, 87, 748–752. [Google Scholar] [CrossRef] [Green Version]
- Akira, S.; Uematsu, S.; Takeuchi, O. Pathogen recognition and innate immunity. Cell 2006, 124, 783–801. [Google Scholar] [CrossRef]
- Agut, H.; Bonnafous, P.; Gautheret-Dejean, A. Update on infections with human herpesviruses 6A, 6B, and 7. Med. Et Mal. Infect. 2017, 47, 83–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suenaga, N.; Ichiyama, T.; Kubota, M.; Isumi, H.; Tohyama, J.; Furukawa, S. Roles of matrix metalloproteinase-9 and tissue inhibitors of metalloproteinases 1 in acute encephalopathy following prolonged febrile seizures. J. Neurol. Sci. 2008, 266, 126–130. [Google Scholar] [CrossRef]
- Schmechel, D.; Marangos, P.J.; Brightman, M. Neurone-specific enolase is a molecular marker for peripheral and central neuroendocrine cells. Nature 1978, 276, 834–836. [Google Scholar] [CrossRef] [PubMed]
- Nagase, H.; Visse, R.; Murphy, G. Structure and function of matrix metalloproteinases and TIMPs. Cardiovasc. Res. 2006, 69, 562–573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brew, K.; Dinakarpandian, D.; Nagase, H. Tissue inhibitors of metalloproteinases: Evolution, structure and function. Biochim. Biophys. Acta 2000, 1477, 267–283. [Google Scholar] [CrossRef]
- Lee, M.A.; Palace, J.; Stabler, G.; Ford, J.; Gearing, A.; Miller, K. Serum gelatinase B, TIMP-1 and TIMP-2 levels in multiple sclerosis. A longitudinal clinical and MRI study. Brain 1999, 122 Pt 2, 191–197. [Google Scholar] [CrossRef] [Green Version]
- Kawamura, Y.; Nakai, H.; Sugata, K.; Asano, Y.; Yoshikawa, T. Serum biomarker kinetics with three different courses of HHV-6B encephalitis. Brain Dev. 2013, 35, 590–595. [Google Scholar] [CrossRef]
- Kawamura, Y.; Yamazaki, Y.; Ohashi, M.; Ihira, M.; Yoshikawa, T. Cytokine and chemokine responses in the blood and cerebrospinal fluid of patients with human herpesvirus 6B-associated acute encephalopathy with biphasic seizures and late reduced diffusion. J. Med. Virol. 2014, 86, 512–518. [Google Scholar] [CrossRef]
- Yamaguchi, H.; Nagase, H.; Ito, Y.; Matsunoshita, N.; Mizutani, M.; Matsushige, T.; Ishida, Y.; Toyoshima, D.; Kasai, M.; Kurosawa, H.; et al. Acute focal bacterial nephritis characterized by acute encephalopathy with biphasic seizures and late reduced diffusion. J Infect Chemother 2018, 24, 932–935. [Google Scholar] [CrossRef]
- Shiba, T.; Hamahata, K.; Yoshida, A. Acute encephalopathy with biphasic seizures and late reduced diffusion in Kawasaki disease. Pediatr. Int. 2017, 59, 1276–1278. [Google Scholar] [CrossRef]
- Ichiyama, T.; Suenaga, N.; Kajimoto, M.; Tohyama, J.; Isumi, H.; Kubota, M.; Mori, M.; Furukawa, S. Serum and CSF levels of cytokines in acute encephalopathy following prolonged febrile seizures. Brain Dev. 2008, 30, 47–52. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| AESD | Prolonged FS Group Median (Range) or Number | ||
|---|---|---|---|
| 1st Seizure Phase Group Median (Range) or Number | 2nd Seizure Phase Group Median (Range) or Number | ||
| n | 7 | 10 | 8 |
| Age, years | 1.8 (0.8–4.5) | 1.8 (1.0–4.3) | 1.8 (1.1–4.4) |
| Male/Female | 5/2 | 6/4 | 4/4 |
| Causative infectious disease | |||
| Exanthema subitum | 2 | 5 | 5 |
| Influenza | 1 | 1 | 3 |
| Others | 4 | 4 | 0 |
| Underlying disorder | |||
| Febrile seizure | 1 | 2 | 2 |
| Tuberous sclerosis | 1 | 0 | 0 |
| Corpus callosum hypoplasia | 1 | 0 | 0 |
| Migratory testis | 0 | 1 | 0 |
| Prader-Willi syndrome | 0 | 0 | 1 |
| Congenital hypothyroidism | 0 | 0 | 1 |
| None | 4 | 7 | 4 |
| Number of patients with a prolonged seizure of more than 40 min | 4 | 3 | 1 |
| Blood examinations | |||
| Aspartate aminotransferase, U/L | 51 (38–299) | 48 (38–382) | 46 (41–63) |
| Creatinine, mg/dL | 0.34 (0.21–0.45) | 0.26 (0.13–0.39) | 0.30 (0.17–0.39) |
| Blood sugar, mg/dL | 110 (82–164) | 116 (85–196) | 107 (93–297) |
| C-reactive protein, mg/dL | 0.90 (0.38–5.11) * | 0.30 (0.08–1.66) | 0.31 (0.04–2.17) |
| Cerebrospinal fluid examinations | |||
| Cell counts, /µL | 1.4 (0.7–490.7) | 1.3 (0.0–3.0) | 0.5 (0.0–3.0) |
| Total protein, mg/dL | 16 (7–114) | 17 (6–172) | 13 (8–22) |
| Neuron specific enolase, ng/mL | 12.6 (6.0–61.0) | 81.1 (17.1–366.0) † | 7.8 (6.3–13.2) |
| Lactate, mg/dL | 17.8 (12.3–35.8) | 10.6 (8.9–17.5) | 13.3 (11.7–15.7) |
| Localization of the bright tree appearance on brain MRI | |||
| Bilaterally widespread | 3 | 3 | 0 |
| Bilateral frontal lobes | 1 | 4 | 0 |
| Unilaterally widespread | 3 | 1 | 0 |
| Unilaterally frontal lobe | 0 | 2 | 0 |
| None | 0 | 0 | 8 |
| Treatment | |||
| TTM | 7 | 10 | 1 |
| Dextromethorphan | 7 | 10 | 4 |
| Vitamin B1/B6/levocarnitine | 7 | 10 | 3 |
| Edaravone | 6 | 10 | 1 |
| Methylprednisolone pulse | 4 | 1 | 0 |
| Intravenous immunoglobulin | 1 | 1 | 0 |
| Acyclovir | 0 | 0 | 1 |
| None | 0 | 0 | 4 |
| Sequela | |||
| ID/DD | 2 | 4 | 0 |
| Epilepsy | 0 | 1 | 0 |
| ID/DD and Epilepsy | 3 | 0 | 0 |
| None | 2 | 5 | 8 |
| AESD | Prolonged FS Group Median (Range) or Number | ||
|---|---|---|---|
| 1st Seizure Phase Group Median (Range) or Number | 2nd Seizure Phase Group Median (Range) or Number | ||
| n | 7 | 10 | 8 |
| Serum | |||
| IL-1β, pg/mL | N.D. (N.D.–18.8) | N.D. | N.D. |
| IL-2, pg/mL | N.D. | N.D. | N.D. |
| IL-4, pg/mL | N.D. | N.D. | N.D. |
| IL-10, pg/mL | 28.7 (N.D.–125.4) | 31.2 (N.D.–74.1) | 41.7 (N.D.–72.0) |
| IL-17A, pg/mL | N.D. (N.D.–28.6) | N.D. | N.D. |
| IL-21, pg/mL | N.D. (N.D.–588.4) | N.D. | N.D. (N.D.–230.9) |
| MIP-1α, pg/mL | N.D. (N.D.–28.5) | N.D. | N.D. |
| CSF | |||
| IL-1β, pg/mL | N.D. | N.D. | N.D. |
| IL-2, pg/mL | N.D. | N.D. (N.D.–79.2) | N.D. |
| IL-4, pg/mL | N.D. | N.D. (N.D.–33.1) | N.D. |
| IL-10, pg/mL | N.D. (N.D.–948.6) | N.D. | N.D. |
| IL-17A, pg/mL | N.D. | N.D. (N.D.–12.6) | N.D. (N.D.–11.8) |
| IL-21, pg/mL | N.D. | N.D. (N.D.–173.3) | N.D. (N.D.–194.3) |
| MIP-1α, pg/mL | N.D. | N.D. | N.D. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kasai, A.; Kobayashi, J.; Nishioka, M.; Kubota, N.; Inaba, Y.; Motobayashi, M. Early Phase Increase in Serum TIMP-1 in Patients with Acute Encephalopathy with Biphasic Seizures and Late Reduced Diffusion. Children 2023, 10, 78. https://doi.org/10.3390/children10010078
Kasai A, Kobayashi J, Nishioka M, Kubota N, Inaba Y, Motobayashi M. Early Phase Increase in Serum TIMP-1 in Patients with Acute Encephalopathy with Biphasic Seizures and Late Reduced Diffusion. Children. 2023; 10(1):78. https://doi.org/10.3390/children10010078
Chicago/Turabian StyleKasai, Ayaka, Jun Kobayashi, Makoto Nishioka, Noriko Kubota, Yuji Inaba, and Mitsuo Motobayashi. 2023. "Early Phase Increase in Serum TIMP-1 in Patients with Acute Encephalopathy with Biphasic Seizures and Late Reduced Diffusion" Children 10, no. 1: 78. https://doi.org/10.3390/children10010078
APA StyleKasai, A., Kobayashi, J., Nishioka, M., Kubota, N., Inaba, Y., & Motobayashi, M. (2023). Early Phase Increase in Serum TIMP-1 in Patients with Acute Encephalopathy with Biphasic Seizures and Late Reduced Diffusion. Children, 10(1), 78. https://doi.org/10.3390/children10010078