Long-Term Analysis of Respiratory-Related Complications Following Gastrostomy Placement with or without Fundoplication in Neurologically Impaired Children: A Retrospective Cohort Study

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Analyzed Outcomes
2.2. Study Population
2.3. Statistical Analyses
3. Results
3.1. Overall Population
3.2. Short-Term Evaluation
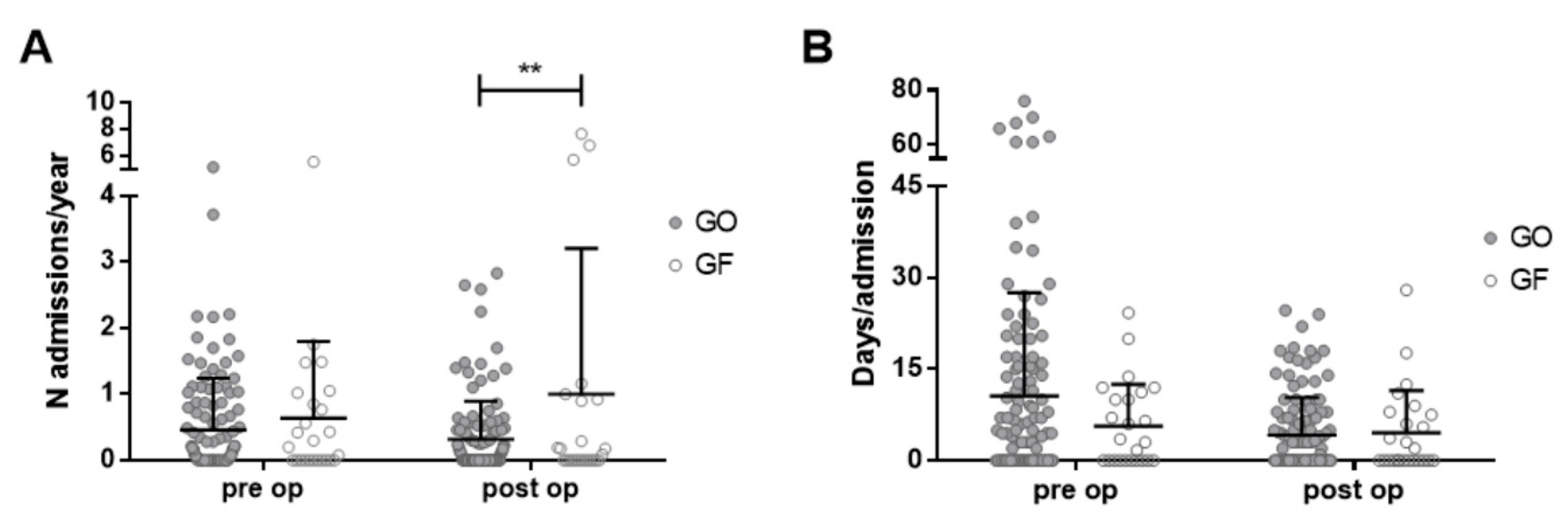
3.3. Long-Term Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sullivan, P.B. Gastrointestinal disorders in children with neurodevelopmental disabilities. Dev. Disabil. Res. Rev. 2008, 14, 128–136. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-S.; Han, Z.-A.; Song, D.; Oh, H.-M.; Chung, M.E. Characteristics of Dysphagia in Children with Cerebral Palsy, Related to Gross Motor Function. Am. J. Phys. Med. Rehabil. 2013, 92, 912–919. [Google Scholar] [CrossRef] [PubMed]
- Himmelmann, K.; Sundh, V. Survival with cerebral palsy over five decades in western Sweden. Dev. Med. Child Neurol. 2015, 57, 762–767. [Google Scholar] [CrossRef] [PubMed]
- Romano, C.; van Wynckel, M.; Hulst, J.; Broekaert, I.; Bronsky, J.; Dall’Oglio, L.; Nataša, M.F.; Iva, H.; Rok, O.; Alexandra, P.; et al. European Society for Paediatric Gastroenterology, Hepatology and Nutrition Guidelines for the Evaluation and Treatment of Gastrointestinal and Nutritional Complications in Children With Neurological Impairment. J. Pediatr. Gastroenterol. Nutr. 2017, 65, 242–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ponsky, T.A.; Gasior, A.C.; Parry, J.; Sharp, S.W.; Boulanger, S.; Parry, R.; Ostlie, D.J.; Peter, S.D.S. Need for subsequent fundoplication after gastrostomy based on patient characteristics. J. Surg. Res. 2013, 179, 1–4. [Google Scholar] [CrossRef]
- Srivastava, R.; Berry, J.G.; Hall, M.; Downey, E.C.; O’Gorman, M.; Dean, J.M.; Barnhart, D.C. Reflux related hospital admissions after fundoplication in children with neurological impairment: Retrospective cohort study. BMJ 2009, 339, b4411. [Google Scholar] [CrossRef] [Green Version]
- Lauriti, G.; Lisi, G.; Lelli Chiesa, P.; Zani, A.; Pierro, A. Gastroesophageal reflux in children with neurological impairment: A systematic review and meta-analysis. Pediatr. Surg. Int. 2018, 34, 1139–1149. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Rosenbaum, P.; Paneth, N.; Leviton, A.; Goldstein, M.; Bax, M.; Damiano, D.; Dan, B.; Jacobsson, B. A report: The definition and classification of cerebral palsy April 2006. Dev. Med. Child Neurol. 2007, 49, 8–14. [Google Scholar] [CrossRef]
- Berry, J.G.; Graham, D.A.; Graham, R.J.; Zhou, J.; Putney, H.L.; O’Brien, J.E.; Roberson, D.W.; Goldmann, D.A. Predictors of Clinical Outcomes and Hospital Resource Use of Children After Tracheotomy. Pediatrics 2009, 124, 563–572. [Google Scholar] [CrossRef] [Green Version]
- Weir, K.; McMahon, S.; Taylor, S.; Chang, A.B. Oropharyngeal Aspiration and Silent Aspiration in Children. Chest 2011, 140, 589–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, N.; Such-Neibar, T. Cerebral palsy diagnosis and management: The state of the art. Curr. Probl. Pediatr. Adolesc. Health Care 2003, 33, 146–169. [Google Scholar] [CrossRef]
- Goldin, A.B.; Sawin, R.; Seidel, K.D.; Flum, D.R. Do antireflux operations decrease the rate of reflux-related hospitalizations in children? Pediatrics 2006, 118, 2326–2333. [Google Scholar] [CrossRef] [PubMed]
- Papaila, J.G.; Vane, D.W.; Colville, C.; Berned, M.; Mallik, G.; Canal, D.; Grosfeld, J.L. The effect of various types of gastrostomy on the lower esophageal sphincter. J. Pediatr. Surg. 1987, 22, 1198–1202. [Google Scholar] [CrossRef]
- Samuel, M.; Holmes, K. Quantitative and qualitative analysis of gastroesophageal reflux after percutaneous endoscopic gastrostomy. J. Pediatr. Surg. 2002, 37, 256. [Google Scholar] [CrossRef]
- Novotny, N.M.; Jester, A.L.; Ladd, A.P. Preoperative prediction of need for fundoplication before gastrostomy tube placement in children. J. Pediatr. Surg. 2009, 44, 173–177. [Google Scholar] [CrossRef]
- Lederhaas, G. Spinal anaesthesia in paediatrics. Best Pr. Res. Clin. Anaesthesiol. 2003, 17, 365–376. [Google Scholar] [CrossRef]
- Sandberg, F.; Brands Viktorsdóttir, M.; Salö, M.; Stenström, P.; Arnbjörnsson, E. Comparison of major complications in children after laparoscopy-assisted gastrostomy and percutaneous endoscopic gastrostomy placement: A meta-analysis. Pediatric Surg. Int. 2018, 34, 1321–132725. [Google Scholar] [CrossRef] [Green Version]
- Hament, J.; Bax, N.; Van Der Zee, D.; De Schryver, J.; Nesselaar, C. Complications of percutaneous endoscopic gastrostomy with or without concomitant antireflux surgery in 96 children. J. Pediatr. Surg. 2001, 36, 1412–1415. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.L.; Meehan, E.; Babl, F.E.; Reid, S.M.; Catto-Smith, A.; Williams, K.; Reddihough, D.S. Paediatric emergency department presentations due to feeding tube complications in children with cerebral palsy. J. Paediatr. Child Health 2019, 55, 1230–1236. [Google Scholar] [CrossRef]
- Barnhart, D.C.; Hall, M.; Mahant, S.; Goldin, A.B.; Berry, J.G.; Faix, R.G.; Dean, J.M.; Srivastava, R. Effectiveness of Fundoplication at the Time of Gastrostomy in Infants With Neurological Impairment. JAMA Pediatr. 2013, 167, 911–918. [Google Scholar] [CrossRef] [Green Version]
- King, M.; Barnhart, D.C.; O’Gorman, M.; Downey, E.C.; Jackson, D.; Mundorff, M.; Holubkov, R.; Feola, P.; Srivastava, R. Effect of Gastrojejunal Feedings on Visits and Costs in Children With Neurologic Impairment. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 518–524. [Google Scholar] [CrossRef]
- Mathei, J.; Coosemans, W.; Nafteux, P.; Decker, G.; De Leyn, P.; Van Raemdonck, D.; Hoffman, I.; DeBoeck, C.; Proesmans, M.; Lerut, T. Laparoscopic Nissen fundoplication in infants and children: Analysis of 106 consecutive patients with special emphasis in neurologically impaired vs. neurologically normal patients. Surg. Endosc. 2007, 22, 1054–1059. [Google Scholar] [CrossRef]
- Battaglia, S.; Orizio, P.; Boroni, G.; Cheli, M.; Colusso, M.M.; Parolini, F.; Bianchi, A.; Alberti, D. Total Oesophagogastric Dissociation in Neurologically Impaired Children. J. Pediatr. Gastroenterol. Nutr. 2020, 70, 457–461. [Google Scholar] [CrossRef]
- Peters, R.T.; Goh, Y.L.; Veitch, J.M.; Khalil, B.A.; Morabito, A. Morbidity and mortality in total esophagogastric dissociation: A systematic review. J. Pediatr. Surg. 2013, 48, 707–712. [Google Scholar] [CrossRef]
- Lansdale, N.; McNiff, M.; Morecroft, J.; Kauffmann, L.; Morabito, A. Long-term and ‘patient-reported’ outcomes of total esophagogastric dissociation versus laparoscopic fundoplication for gastroesophageal reflux disease in the severely neurodisabled child. J. Pediatr. Surg. 2015, 50, 1828–1832. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| GMFCS | All (145) | GO (119) | GF (26) |
|---|---|---|---|
| Grade 1, n (%) | 7 (4.8) | 5 (4.2) | 2 (7.7) |
| Grade 2, n (%) | 4 (2.8) | 3 (2.5) | 1 (3.8) |
| Grade 3, n (%) | 8 (5.5) | 6 (5) | 2 (7.7) |
| Grade 4, n (%) | 29 (20) | 21 (17.7) | 8 (30.8) |
| Grade 5, n (%) | 88 (60.7) | 75 (63) | 13 (50) |
| unknown, n (%) | 9 (6.2) | 9 (7.6) | 0 (0) |
| Diagnostic Test | Positive | Negative | Delayed Gastric Empting |
|---|---|---|---|
| 24-h pH monitoring | 29 (50) | 29 (50) | |
| UGI-BS | 20 (53) | 13 (34) | 5 (13) |
| VFS | 20 | 15 |
| Type of Complication | Short Term (n = 56) | Long Term (n = 57) | ||
|---|---|---|---|---|
| Minor (GF = 9, GO = 35) | Major (GF = 5, GO = 8) | Minor (GF = 5, GO = 30) | Major (GF = 7, GO = 15) | |
| Bleeding | 1 (GF) | 1 (GF) | 0 | 0 |
| Organ damage | 0 | 1 (GO) | 0 | 0 |
| Respiratory distress | 0 | 3 (GF 2, GO 1) | 0 | 5 (GF 2, GO 3) |
| Systemic infection/Fever | 24 (GF 4, GO 20) | 2 (GO 2) | 1 (GO) | 2 (GO 2) |
| Peritonitis/Bowel Obstruction | 0 | 1 (GO) | 0 | 4 (GF 1, GO 3) |
| Local infection/granuloma | 5 (GF 1, GO 4) | 0 | 15 (GF 3, GO 12) | 0 |
| Feeding difficulties/vomits | 13 (GF 3, GO 10) | 0 | 2 (GO) | 0 |
| Malfunctioning/Displacement | 0 | 5 (GF 2, GO 3) | 17 (GF 2, GO 15) | 11 (GF 4, GO 7) |
| TOTAL (% of the patients) | 43 (30%) | 13 (9%) | 35 (24%) | 22 (15%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zambaiti, E.; Virgone, C.; Bisoffi, S.; Stefanizzi, R.; Fascetti Leon, F.; Gamba, P. Long-Term Analysis of Respiratory-Related Complications Following Gastrostomy Placement with or without Fundoplication in Neurologically Impaired Children: A Retrospective Cohort Study. Children 2021, 8, 22. https://doi.org/10.3390/children8010022
Zambaiti E, Virgone C, Bisoffi S, Stefanizzi R, Fascetti Leon F, Gamba P. Long-Term Analysis of Respiratory-Related Complications Following Gastrostomy Placement with or without Fundoplication in Neurologically Impaired Children: A Retrospective Cohort Study. Children. 2021; 8(1):22. https://doi.org/10.3390/children8010022
Chicago/Turabian StyleZambaiti, Elisa, Calogero Virgone, Silvia Bisoffi, Roberta Stefanizzi, Francesco Fascetti Leon, and Piergiorgio Gamba. 2021. "Long-Term Analysis of Respiratory-Related Complications Following Gastrostomy Placement with or without Fundoplication in Neurologically Impaired Children: A Retrospective Cohort Study" Children 8, no. 1: 22. https://doi.org/10.3390/children8010022
APA StyleZambaiti, E., Virgone, C., Bisoffi, S., Stefanizzi, R., Fascetti Leon, F., & Gamba, P. (2021). Long-Term Analysis of Respiratory-Related Complications Following Gastrostomy Placement with or without Fundoplication in Neurologically Impaired Children: A Retrospective Cohort Study. Children, 8(1), 22. https://doi.org/10.3390/children8010022