
The Role of Physiotherapy in Pediatric Palliative Care: A Systematic Review


 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
- Qualitative, quantitative, and mixed-methods studies.
- Study population exclusively composed of children, children, and their families or physiotherapists.
- The sample must either have some disease susceptible to palliative care or be part of a palliative care program.
- Articles in which there is some relationship between physiotherapy and PPC.
- Articles published in the last 10 years.
- Articles published in English or Spanish.
- Articles available in full text.
3. Results
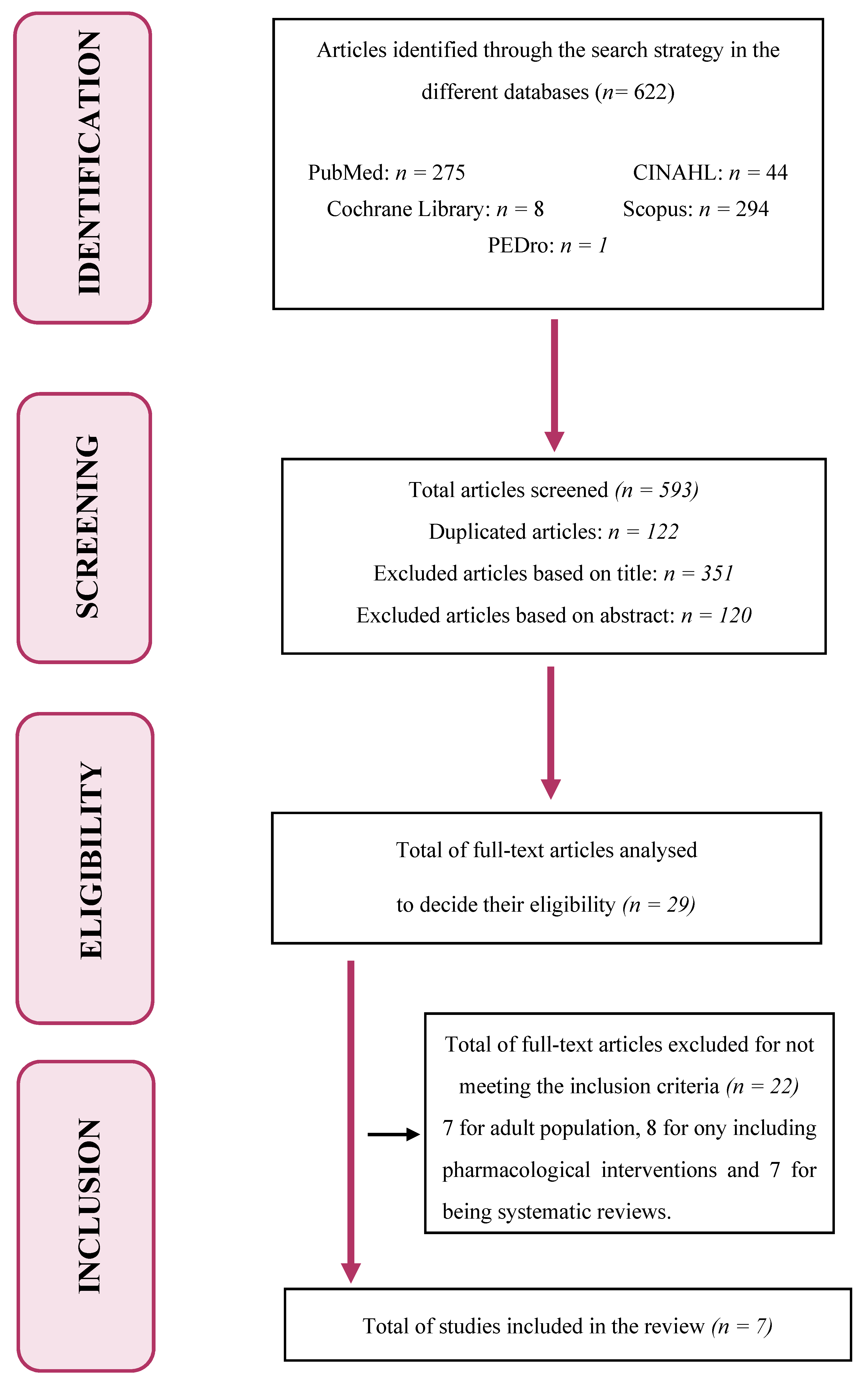
3.1. Article Selection Process
A Total of 622 Studies Were Initially Identified after the Search
3.2. Study Population
3.3. Study Variables and Data Gathering
3.4. Pathologies Treated with Physiotherapy in Pediatric Palliative Care (PPC)
3.5. Physiotherapeutic Interventions in PPC
3.6. Effects Observed in the Children in Palliative Care and their Families after the Physiotherapeutic Intervention
3.7. Knowledge of the Physiotherapists about PPC
4. Discussion
Limitations of the Study and Future Research Lines
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- World Health Organization. Integrating Palliative Care and Symptom Relief into Paediatrics: A WHO Guide for Health Care Planners, Implementers and Managers; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Salvador, C.; Salvador, V.; Segura, A.; Andrés, M.; Fernández, J.M.; Niño, O.M.; Reche, E. Actualidad de los cuidados paliativos. Revisión de una situación poco estandarizada. Pediatría Atención Primaria 2015, 67, 215–222. [Google Scholar] [CrossRef] [Green Version]
- European Association for Palliative Care. IMPaCCT: Standards for paediatric palliative care in Europe. Eur. J. Palliat. Care 2007, 14, 109–114. [Google Scholar]
- Ortiz San Román, L.; Martino, R.J. Enfoque paliativo en Pediatría. Pediatr. Integral. 2016, 2, 131.e1–131.e7. [Google Scholar]
- Association for Children with Life-Threatening or Terminal Conditions and Their Families (ACT)/the Royal College of Paediatrics and Child Health (RCPCH). A Guide to the Development of Children’s P alliative Care Services, 3rd ed.; ACT: Bristol, UK, 2009. [Google Scholar]
- Connor, S.R.; Downing, J.; Marston, J. Estimating the global need for palliative care for children: A cross sectional analysis. J. Pain Symptom Manag. 2017, 53, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Ine.es, Instituto Nacional de Estadística. Datos Definitivos a 1 de Enero del 2020 Población Residente por Fecha, Sexo y Edad. Disponible en. Available online: https://www.ine.es/jaxiT3/Datos.htm?t=31304 (accessed on 14 May 2021).
- De Sanidad, M.; e Igualdad, S.S. Criterios de Atención; Cuidados Paliativos Pediátricos en el Sistema Nacional de Salud: Madrid, Spain, 2014. [Google Scholar]
- Santos, P.; Losa, V.; Huidobro, B. Cuidados paliativos en Pediatría. Act. Pediatr. Aten. Prim. 2017, 10, 109–114. [Google Scholar]
- Fundación PORQUEVIVEN-CUIDADOS PALIATIVOS PEDIÁTRICOS Madrid. 2020 Unanimidad en las Cortes de Castilla-La Mancha ante una Proposición (PNL) Para Desarrollar los Cuidados Paliativos Pediátricos. Available online: https://porqueviven.org/ley-cuidados-paliativos-pediatricos/ (accessed on 18 May 2021).
- Suárez, E.; García, T. Cuidados paliativos pediátricos. Desde la perspectiva enfermera. NPunto 2020, III, 42–63. [Google Scholar]
- European Association for Palliative Care. Palliative Care for Infants, Children and Young People. Facts; The Maruzza Lefebvre D’Ovidio Foundation: Rome, Italy, 2009. [Google Scholar]
- Montagnini, M.; Javier, N.M. Physical therapy and other rehabilitation issues in the palliative care setting. UpToDate 2017, 16. Available online: https://www.uptodate.com/contents/physical-therapy-and-other-rehabilitation-issues-in-the-palliative-care-setting/print (accessed on 20 May 2021).
- Kumar, S.P.; Jim, A. Physical therapy in palliative care: From symptom control to quality of life: A critical review. Indian J. Palliat. Care 2010, 16, 138–146. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, J.L.; Brasile de Oliveira, S. What can the physiotherapist do for the child in palliative care? Point of view. Residência Pediátrica 2019. [Google Scholar] [CrossRef]
- Dangel, T.; Kmieć, T.; Januszaniec, A.; Ważny, B. Palliative care in 9 children with neurodegeneration with brain iron accumulation. Neurol. Sci. 2020, 41, 653–660. [Google Scholar] [CrossRef] [PubMed]
- Genik, L.M.; McMurtry, C.M.; Marshall, S.; Rapoport, A.; Stinson, J. Massage therapy for symptom reduction and improved quality of life in children with cancer in palliative care: A pilot study. Complement. Ther. Med. 2020, 48, 102263. [Google Scholar] [CrossRef] [PubMed]
- Rico-Mena, P.; Palacios-Ceña, D.; Martino-Alba, R.; Chocarro-Gonzalez, L.; Güeita-Rodríguez, J. The impact of home-based physical rehabilitation program on parents’ experience with children in palliative care: A qualitative study. Eur. J. Phys. Rehabil. Med. 2019, 55, 494–504. [Google Scholar] [CrossRef] [PubMed]
- Weingarten, K.; MacApagal, F.; Parker, D. Virtual Reality: Endless Potential in Pediatric Palliative Care: A Case Report. J. Palliat. Med. 2020, 23, 147–149. [Google Scholar] [CrossRef] [PubMed]
- Hully, M.; Barnerias, C.; Chabalier, D.; Le Guen, S.; Germa, V.; Deladriere, E.; Catherine, V.; Jean-Marie, C.; Brigitte, C.; Claude, C.; et al. Palliative Care in SMA Type 1: A Prospective Multicenter French Study Based on Parents’ Reports. Front. Pediatr. 2020, 18, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliveira, J.L.R.; Rodrigues, R.P.; Barreto, L.A. The knowledge of physical therapists on palliative care in pediatria em a maternal children´s. J. Physiother. Res. 2021, 11, 375–383. [Google Scholar]
- Sarmad, S.; Khan, I.; Rauf, W.; Jawad, M. Role of 24 Hours Handling on Gross Motor Function and Spasticity in Cerebral Palsy Children with GMFCS Level IV and V. Pak. Pediatr. J. 2021, 45, 40–45. [Google Scholar]


{kind=link}
| Groups | Definition | Examples |
|---|---|---|
| Group 1 | Potentially deadly diseases for which curative treatment may be feasible but may also fail. During the curative treatment, palliative care may be required during an acute crisis or if the treatment fails. | Cancer Heart, liver. or kidney failure Infections |
| Group 2 | Diseases that require long periods of intensive treatment aimed at prolonging life and enabling participation in normal activities but in which early death is possible. | Cystic fibrosis Extreme prematurity Cardiovascular anomalies |
| Group 3 | Progressive diseases with no options of curative treatment, where treatment is exclusively palliative since diagnosis and may extend for many years. | Neuromuscular or neurodegenerative disorders Progressive metabolic disorders Chromosomal anomalies |
| Group 4 | Irreversible non-progressive diseases that cause a severe disability, which leads to an extreme vulnerability to suffer from health complications and to the probability of early death. | Severe cerebral palsy Congenital malformations Brain or spinal cord lesions |
| Pediatric Descriptors | Descriptors of Palliative Care and Susceptible Diseases | Descriptors of Symptom Control | Descriptors of Physiotherapy |
|---|---|---|---|
| Pediatric Child Children Infant Childhood | Palliative care Terminal conditions Oncology/cancer Cerebral palsy Neuromuscular or neurodegenerative disorders Extremely premature Congenital malformations | Symptom management Symptom control Physical symptoms | Physical therapy Physiotherapy Exercise therapy Rehabilitation |
| Year and Authors | Study Design | Scale | Score |
|---|---|---|---|
| Dangel et al., 2019 | Descriptive quantitative study | STROBE | 13/22 |
| Genik et al., 2019 | Quasi-experimental study | TREND | 16/22 |
| Rico et al., 2019 | Qualitative study | COREQ | 26/32 |
| Weingarten et al., 2019 | Clinical case | CARE | 9/13 |
| Hully et al., 2020 | Descriptive quantitative study | STROBE | 18/22 |
| Oliveira et al., 2021 | Descriptive quantitative study | STROBE | 17/22 |
| Sarmad et al., 2021 | Quasi-experimental study | TREND | 16/22 |
| Year and Authors | Study Design | Population | Main Intervention | Study Variables | Data Gathering | Results |
|---|---|---|---|---|---|---|
| Dangel et al., 2019 [16] | Descriptive quantitative study | 9 children aged 7–14 years with neurodegeneration with brain iron accumulation (NBIA) | — Any main intervention applied | Home pediatric palliative care for children with NBIA and their families | Questionnaires filled by parents. The study was conducted between 1998 and 2018 | PPC reduces pain and improves symptom control in most cases, but not in all The quality of the home pediatric palliative care provided by the multidisciplinary team was valued as high, with very satisfied parents Regarding the rehabilitation, respiratory physiotherapy is highlighted as one of the most important therapies to prevent the early death of the patient |
| Genik et al., 2019 [17] | Pre–post pilot study of a single group | 8 children with cancer: n = 1 carcinoma, n = 4 leukemia, n = 2 lymphoma, n = 1 sarcoma, (aged 10–17 years) who had been referred to PPC and one of the parents | Therapeutic massage (1 h) once per week in the hospital or at home for one month. Follow-up of 4–6 weeks | Quality of life of the child and his/her parents Pain and impact on the daily life of the child Concern and fear of the children | PedsQL Cancer Module PainSquad and FPS-R CFS | Significant decrease of the children’s pain and concern (p = 0.03) The effects do not persist in the long term No significant changes were observed in the quality of life |
| Rico et al., 2019 [18] | Qualitative study | 14 parents and 11 children in PPC (n = 5 CCP, n = 1 severe stroke, n = 1 polymarformative syndrome, n = 1 Patau’s syndrome, n = 1 hydranencephaly, n = 1 non-identified mitochondrial disorder, n = 1 Tay-Sachs disease) | Any main intervention applied | Experience and perspective of the parents about the home physical rehabilitation in PPC | Non-structured and semi-structured interviews for 8 months | The physical rehabilitation increased the quality of life of the children and improved their motor skills The home physical rehabilitation facilitated the learning of the techniques by the parents in the usual environment of the child In the socio-family environment, the home physical rehabilitation helped to maintain bonds with the family, reduced expenditures, and helped the child to better adapt to the environment |
| Weingarten et al., 2019 [19] | Clinical case | 12-year-old girl with acute myeloid leukemia who participates in a PPC program | Virtual reality in the hospital room | Symptom control Quality of life | Questionnaire before and after the VR experience | VR favored distraction and made her believe she came out of the room Pain decreased during VR Better experience with VR alone and unaccompanied by a professional. |
| Hully et al., 2020 [20] | Multicenter prospective cohort study | 37 SMA-1 patients (20 girls and 17 boys) with an average age of 3 months | Respiratory physiotherapy from 3 per week to every day, 10 min approx. Motor physiotherapy (postural management). Abdominal massage | Respiratory, nutritional, and motor management Child pain and comfort | Questionnaires filled out by parents and notes from professionals 2012–2016 | p < 0.05 - Airway clearance, comfort and no pain with respiratory physiotherapy, but tiring - Well-being, no pain with physical motor - Modifying feeding and massaging abdomen improve bowel function and constipation |
| Oliveira et al., 2021 [21] | Descriptive quantitative study | 44 physiotherapists (35 women and 9 men) between 20 and 50 years old from the pediatric and NICU units | — | Knowledge of physiotherapists about PPC | Socio-professional questionnaires BPW test | 93.2% have not received training on PPC during the degree, 34.1% have received it after graduating, 90.5% considered non-pharmacological therapies such as physical therapy important for pain management |
| Sarmad et al., 2021 [22] | Quasi-experimental study | 89 children aged 1–3 years with spastic cerebral palsy (level IV or V GMFCS) | Neurodevelopment and sensory stimulation Family training on postural management in different activities Duration: 3–4 h per week, for 3 months | Management of the mothers on the motor functions and spasticity in the time when their children are not in physiotherapy | GMFM before and after the intervention of the physiotherapist MTS | Adequate management of the child by the mothers led to significant changes in the gross motor activities in 100% of the children (p = 0.00), whereas the spasticity decreased in 77.53% of the patients. |
| Population Type | Number of Participants | Age | Sex |
|---|---|---|---|
| Children | 144 | 0.6 months–17 years | M: 22 * |
| F: 24 * | |||
| Parents | 14 | 21–59 years | M: 4 |
| F: 10 | |||
| Physiotherapists | 44 | 20–50 years | M: 9 |
| F: 35 | |||
| Total | 202 | M: 35 * | |
| F: 69 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortiz-Campoy, S.; Lirio-Romero, C.; Romay-Barrero, H.; Álvarez, D.M.-C.; López-Muñoz, P.; Palomo-Carrión, R. The Role of Physiotherapy in Pediatric Palliative Care: A Systematic Review. Children 2021, 8, 1043. https://doi.org/10.3390/children8111043
Ortiz-Campoy S, Lirio-Romero C, Romay-Barrero H, Álvarez DM-C, López-Muñoz P, Palomo-Carrión R. The Role of Physiotherapy in Pediatric Palliative Care: A Systematic Review. Children. 2021; 8(11):1043. https://doi.org/10.3390/children8111043
Chicago/Turabian StyleOrtiz-Campoy, Silvia, Cristina Lirio-Romero, Helena Romay-Barrero, David Martín-Caro Álvarez, Purificación López-Muñoz, and Rocío Palomo-Carrión. 2021. "The Role of Physiotherapy in Pediatric Palliative Care: A Systematic Review" Children 8, no. 11: 1043. https://doi.org/10.3390/children8111043
APA StyleOrtiz-Campoy, S., Lirio-Romero, C., Romay-Barrero, H., Álvarez, D. M. -C., López-Muñoz, P., & Palomo-Carrión, R. (2021). The Role of Physiotherapy in Pediatric Palliative Care: A Systematic Review. Children, 8(11), 1043. https://doi.org/10.3390/children8111043