
Meconium Aspiration Syndrome: A Narrative Review

 , ,
, , 
{kind=link}
{kind=link}
Abstract
:1. Definition of Meconium Aspiration Syndrome
2. Epidemiology
3. Etiopathogenesis
4. Pathophysiology
- (a)
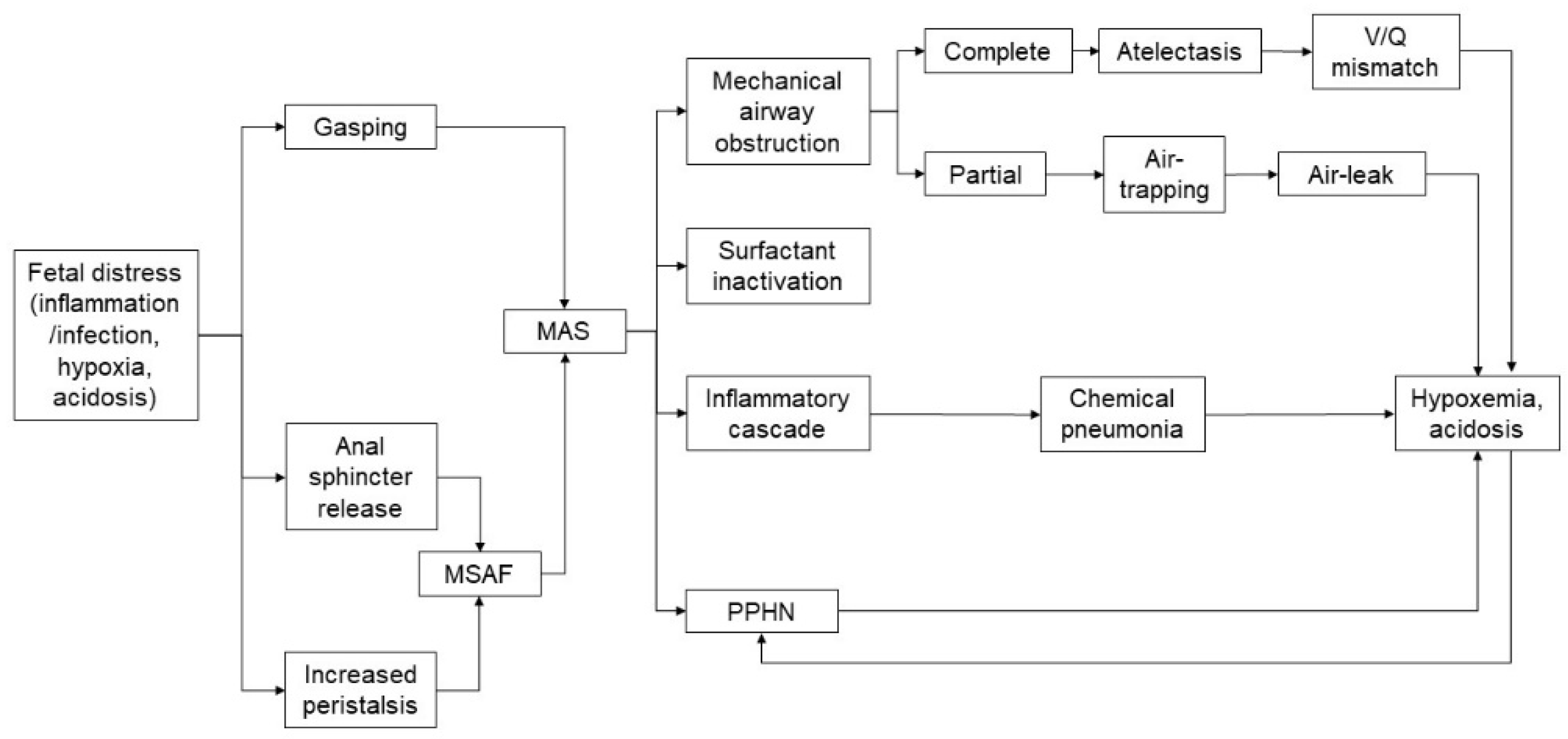
- Antenatal inflammation/infection [12,13,14,15]: as bacteria, endotoxin and high concentrations of inflammatory mediators have been found in MSAF, a fetus swallowing such microbial products and inflammatory mediators can experience increased intestinal peristalsis and passage of meconium, which can be aspirated by the fetus. A recent study reported the presence of meconium in the alveoli of stillbirths, which suggested an antemortem meconium passage in utero due to hypoxia and inflammatory processes. Further, histological findings showed an increased acute placental inflammation in MSAF. Although amniotic fluid has bacteriostatic properties, the addition of a small amount of meconium impairs its inhibitory effect and can enhance the growth of bacteria such as group B streptococcus and Escherichia coli.
- (b)
- Mechanical airway obstruction [4,7]: the occlusion of the airways by meconium plugs leads to a high resistance to air flow and air trapping according to the consistency and quantity of the meconium-stained liquid. If the obstruction is partial, valve effects lead to a hyperinflation condition; if the obstruction is total, “patchy” areas of atelectasis are caused. Trapped gas can lead to air leak such as interstitial emphysema, pneumothorax and pneumomediastinum. Partial or complete airway obstructions have been considered to be the main pathophysiological mechanism of MAS for many years.
- (c)
- Inactivation of the surfactant [4,7]: the surfactant inactivation due to the action of meconium fatty acids causes atelectasis and impairs the ventilation-perfusion mismatch. Although the precise mechanism is not fully understood, fat-soluble and water-soluble components of the meconium seem to be involved in this process. Meconium is able to alter the viscosity and ultrastructure of the surfactant through direct toxicity on type II pneumocytes. Furthermore, it reduces the levels of proteins A and B and accelerates the conversion of active large aggregates into less active smaller forms and determines the displacement from the alveolar surface. Surfactant dysfunction is further worsened by binding to plasma proteins due to damage of the alveolar-capillary membrane and the presence of proteolytic enzymes and oxygen free radicals.
- (d)
- Activation of the inflammatory cascade [4,16,17]: the alveolar interstitium of patients with MAS shows inflammatory cellular infiltrates characterized by the release of cytokines and complement activation. Meconium contains substances with a chemotactic action for neutrophils; it also activates the complement, has a vasoactive function and is also a source of pro-inflammatory mediators (such as IL-1, IL-6 and IL-8 and TNF). Despite the repairing role of inflammation, its destructive potential can cause local tissue damage. For decades it has been widely known that meconium is toxic and induces inflammation and apoptosis and can lead to chemical pneumonia in the first 48 h of life with a risk of bacterial over-infection. However, the cellular mechanism underlying the initiation of the inflammatory cascade in humans remains to be clarified. As meconium is produced in the intestine and is therefore only minimally exposed to the immune system during fetal life, it may be recognized as “not self”, triggering the activation of innate immunity. It has been hypothesized that the two main systems of the recognition of innate immunity (the toll-like receptor and the complement system) may recognize meconium as dangerous and activate the inflammatory cascade. In vivo, it is reasonable to hypothesize that additional triggers for inflammation can be hypoxia due to MAS, baro- and volu-trauma related to ventilation and oxygen therapy. Understanding the mechanisms underlying the inflammatory cascade in MAS could be useful for addressing new therapeutic strategies.
- (e)
- Persistent pulmonary hypertension [4]: it occurs in 15–20% of MAS patients and has been linked to different mechanisms including pulmonary vasoconstriction (secondary to hypoxia/hypercapnia/acidosis), capillary hypertrophy (due to intrauterine hypoxia) and pulmonary hyperexpansion (increasing pulmonary resistance). The right-left shunts worsen the hypoxemia and can lead to a dangerous vicious circle.
5. Factors Associated with MAS
6. Clinical Features
7. Diagnosis
- Respiratory distress in a newborn born through MSAF;
- Oxygen requirement to maintain transcutaneous saturation over 92%;
- The need for oxygen therapy within 2 h of life and for at least 12 h
- The absence of malformations of the airways, lungs and heart.
8. Treatment
8.1. General Treatment
8.2. Respiratory Support
8.3. Surfactant
8.4. Inhaled Nitric Oxide
8.5. Steroids
8.6. Inotropic Therapy
- (a)
- If the echocardiographic features do not show a reduction of contractility and/or a reduction of the left ventricular output (LVO), hypotension is likely due to peripheral vasodilatation and vasopressors with action directed on systemic venous resistance (such as dopamine, norepinephrine or vasopressin);
- (b)
- If echocardiographic features show a low LV preload with RV/LV systolic dysfunction, positive inotropic agents with a pulmonary vasodilator effect (such as norepinephrine) are indicated; milrinone can be used in association with inotropes such as dobutamine or vasopressin because it causes pulmonary and systemic vasodilation;
- (c)
- If systemic blood pressure is stable, milrinone should be used in case of cardiac dysfunction; milrinone is a powerful vasodilator of the pulmonary circulation that also has a positive lusitropic and inotropic action while it also causes systemic vasodilation and reduces mean arterial pressure.
8.7. Extracorporeal Membrane Oxygenation (ECMO)
8.8. Therapeutic Hypothermia
8.9. Therapeutic Considerations
9. Prognosis
10. Prevention
11. Management of Infants Born through MSAF
12. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wiswell, T.E.; Tuggle, J.M.; Turner, B.S. Meconium aspiration syndrome: Have we made a difference? Pediatrics 1990, 85, 715–721. [Google Scholar] [PubMed]
- Clearly, G.M.; Wiswell, T.E. Meconium-stained amniotic fluid and the meconium aspiration syndrome: An update. Pediatr. Clin. N. Am. 1998, 45, 511–529. [Google Scholar] [CrossRef]
- Fischer, C.P.; Rybakowski, C.; Ferdynus, C.; Sagot, P.; Gouyon, J.B. A Population-Based Study of Meconium Aspiration Syndrome in Neonates Born between 37 and 43 Weeks of Gestation. Int. J. Pediatr. 2012, 2012, 321545. [Google Scholar] [CrossRef]
- Swarnam, K.; Soraisham, A.S.; Sivanandan, S. Advances in the Management of Meconium Aspiration Syndrome. Int. J. Pediatr. 2011, 2012, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Nangia, S.; Sundera, S.; Biswasb, R.; Saili, A. Endotracheal suction in term non vigorous meconium stained neonate. A pilot study. Resuscitation 2016, 105, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Wiswell, T.E.; Fuloria, M. Management of meconium-stained amniotic fluid. Clin. Perinatol. 1999, 26, 659–668. [Google Scholar] [CrossRef]
- Vain, N.E.; Batton, D.G. Meconium “aspiration” (or respiratory distress associated with meconium-stained amniotic fluid?). Semin. Fetal Neonatal Med. 2017, 22, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Paudel, P.; Sunny, A.K.; Poudel, P.G.; Gurung, R.; Gurung, A.; Bastola, R.; Chaudhary, R.N.; Budhathoki, S.S.; Ashish, K.C. Meconium aspiration syndrome: Incidence, associated risk factors and outcome-evidence from a multicentric study in low-resource settings in Nepal. J. Paediatr. Child Health 2020, 56, 630–635. [Google Scholar] [CrossRef]
- Rahman, S.; Unsworth, J.; Vause, S. Meconium in Labour. Obstet. Gynaecol. Reprod. Med. 2013, 23, 247–252. [Google Scholar] [CrossRef]
- Nangia, S.; Chandrasekharan, P.; Lakshminrusimha, S.; Rawat, M. Approach to Infants Born Through Meconium Stained Amniotic Fluid: Evolution Based on Evidence? Am. J. Perinatol. 2018, 35, 815–822. [Google Scholar] [CrossRef]
- Gandhi, C.K. Management of Meconium-Stained Newborns in the Delivery Room. Neonatal Netw. 2018, 37, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Romero, R.; A Lee, K.; Na Kim, E.; Korzeniewski, S.J.; Chaemsaithong, P.; Yoon, B.H. Meconium aspiration syndrome: A role for fetal systemic inflammation. Am. J. Obstet. Gynecol. 2016, 214, 366.e1–366.e9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacques, S.M.; Qureshi, F. Does in utero meconium passage in term stillbirth correlate with autopsy and placental findings of hypoxia or inflammation? J. Matern. Neonatal Med. 2020, 1–7. [Google Scholar] [CrossRef]
- Rao, S.; Pavlova, Z.; Incerpi, M.H.; Ramanathan, R. Meconium-Stained Amniotic Fluid and Neonatal Morbidity in Near-Term and Term Deliveries with Acute Histologic Chorioamnionitis and/or Funisitis. J. Perinatol. 2001, 21, 537–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saeed, H.; Jacques, S.M.; Qureshi, F. Meconium staining of the amniotic fluid and the presence and severity of acute placental inflammation: A study of term deliveries in a predominantly African-American population. J. Matern. Fetal Neonatal Med. 2018, 31, 3172–3177. [Google Scholar] [CrossRef] [PubMed]
- Lindenskov, P.H.H.; Castellheim, A.; Saugstad, O.D.; Mollnes, T.E. Meconium aspiration syndrome: Possible pathophysio-logical mechanisms and future potential therapies. Neonatology 2015, 107, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Tyler, D.C.; Murphy, J.; Cheney, F.W. Mechanical and chemical damage to lung tissue caused by meconium aspiration. Pediatrics 1978, 62, 454–459. [Google Scholar]
- Kim, B.; Oh, S.-Y.; Kim, J.-S. Placental Lesions in Meconium Aspiration Syndrome. J. Pathol. Transl. Med. 2017, 51, 488–498. [Google Scholar] [CrossRef] [Green Version]
- Choi, W.; Jeong, H.; Choi, S.-J.; Oh, S.-Y.; Kim, J.-S.; Roh, C.-R.; Kim, J.-H. Risk factors differentiating mild/moderate from severe meconium aspiration syndrome in meconium-stained neonates. Obstet. Gynecol. Sci. 2015, 58, 24–31. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, C.P.L.; Flôr-De-Lima, F.; Rocha, G.M.D.; Machado, A.P.; Guimarães Pereira Areias, M.H.F. Meconium aspiration syndrome: Risk factors and predictors of severity. J. Matern. Fetal Neonatal Med. 2017, 32, 1492–1498. [Google Scholar] [CrossRef]
- Meydanli, M.; Dilbaz, B.; Çalişkan, E.; Dilbaz, S.; Haberal, A. Risk factors for meconium aspiration syndrome in infants born through thick meconium. Int. J. Gynecol. Obstet. 2001, 72, 9–15. [Google Scholar] [CrossRef]
- Kalra, V.K.; Lee, H.C.; Sie, L.; Ratnasiri, A.W.; Underwood, M.A.; Lakshminrusimha, S. Change in neonatal resuscitation guidelines and trends in incidence of meconium aspiration syndrome in California. J. Perinatol. 2020, 40, 46–55. [Google Scholar] [CrossRef]
- Chiruvolu, A.; Miklis, K.K.; Chen, E.; Petrey, B.; Desai, S. Delivery Room Management of Meconium-Stained Newborns and Respiratory Support. Pediatrics 2018, 142, e20181485. [Google Scholar] [CrossRef] [Green Version]
- Karabayir, N.; Demirel, A.; Bayramoglu, E. Blood lactate level and meconium aspiration syndrome. Arch. Gynecol. Obstet. 2015, 291, 849–853. [Google Scholar] [CrossRef]
- Gupta, S.K.; Haerr, P.; David, R.; Rastogi, A.; Pyati, S. Meconium aspiration syndrome in infants of HIV-positive women: A case-control study. J. Périnat. Med. 2016, 44, 469–475. [Google Scholar] [CrossRef]
- Khazardoost, S.; Hantoushzadeh, S.; Khooshideh, M.; Borna, S. Risk factors for meconium aspiration in meconium stained amniotic fluid. J. Obstet. Gynaecol. 2007, 27, 577–579. [Google Scholar] [CrossRef]
- Vivian-Taylor, J.; Sheng, J.; Hadfield, R.M.; Morris, J.M.; Bowen, J.R.; Roberts, C.L. Trends in obstetric practices and meconium aspiration syndrome: A population-based study. BJOG 2011, 118, 1601–1607. [Google Scholar] [CrossRef] [PubMed]
- Bhutani, V.K. Developing a systems approach to prevent meconium aspiration syndrome: Lessons learned from multinational studies. J. Perinatol. 2008, 28 (Suppl. S3), S30–S35. [Google Scholar] [CrossRef] [Green Version]
- Hernandez, C.; Little, B.B.; Dax, J.S.; Gilstrap, L.C., III; Rosenfeld, C.R. Prediction of the severity of meconium aspiration syndrome. Am. J. Obstet. Gynecol. 1993, 169, 61–70. [Google Scholar] [CrossRef]
- Kitsommart, R.; Thammawong, N.; Sommai, K.; Yangnoy, J.; Bowornkitiwong, W.; Paes, B. Impact of meconium consistency on infant resuscitation and respiratory outcomes: A retrospective-cohort study and systematic review. J. Matern. Fetal Neonatal Med. 2020, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Chettri, S.; Adhisivam, B.; Bhat, B.V. Endotracheal Suction for Nonvigorous Neonates Born through Meconium Stained Amniotic Fluid: A Randomized Controlled Trial. J. Pediatr. 2015, 166, 1208–1213.e1. [Google Scholar] [CrossRef]
- Fanaroff, A.A. Meconium aspiration syndrome: Historical aspects. J. Perinatol. 2008, 28 (Suppl. S3), S3–S7. [Google Scholar] [CrossRef] [Green Version]
- Walsh, M.C.; Fanaroff, J.M. Meconium stanied fluid: Approach to the mother and to the baby. Clin. Perinatol. 2007, 34, 653–665. [Google Scholar] [CrossRef]
- Goldsmith, J.; Karotkin, E.; Suresh, G.; Keszler, M. Assisted Ventilation of the Neonate, Evidence-Based Approach to Newborn Respiratory Care, 6th ed.; Elsevier: Amsterdam, The Netherlands, 2017. [Google Scholar]
- Vain, N.E.; Szyld, E.G.; Prudent, L.M.; E Wiswell, T.; Aguilar, A.M.; Vivas, N.I. Oropharyngeal and nasopharyngeal suctioning of meconium-stained neonates before delivery of their shoulders: Multicentre, randomised controlled trial. Lancet 2004, 364, 597–602. [Google Scholar] [CrossRef]
- El Amrousy, D.; Elgendy, M.; Eltomey, M.; Elmashad, A.E. Value of lung ultrasonography to predict weaning success in ventilated neonates. Pediatr. Pulmonol. 2020, 55, 2452–2456. [Google Scholar] [CrossRef]
- Corsini, I.; Parri, N.; Ficial, B.; Dani, C. Lung ultrasound in the neonatal intensive care unit: Review of the literature and future perspectives. Pediatr. Pulmonol. 2020, 55, 1550–1562. [Google Scholar] [CrossRef] [PubMed]
- Piastra, M.; Yousef, N.; Brat, R.; Manzoni, P.; Mokhtari, M.; De Luca, D. Lung ultrasound findings in meconium aspiration syndrome. Early Hum. Dev. 2014, 90 (Suppl. S2), S41–S43. [Google Scholar] [CrossRef]
- De Boode, W.P.; Singh, Y.; Molnar, Z.; Schubert, U.; Savoia, M.; Seghal, A.; Levy, P.Y.; McNamara, P.J.; El-Khuffash, A.; European Special Interest Group “Neonatologist Performed Echocardiography” (NPE). Application of Neonatologist Performed Echocardiography in the assessment and management of persistent pulmonary hypertension of the newborn. Pediatr. Res. 2018, 85 (Suppl. S1), 68–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhattacharya, S.; Sen, S.; Levy, P.T.; Rios, D.R. Comprehensive evaluation of right heart performance and pulmonary he-modynamics in neonatal pulmonary hypertension. Curr Treat. Options Cardiovasc. Med. 2019, 21, 10. [Google Scholar] [CrossRef] [PubMed]
- Mathew, B.; Lakshminrusimha, S. Persistent Pulmonary Hypertension in the Newborn. Children 2017, 4, 63. [Google Scholar] [CrossRef] [Green Version]
- ELSO Guidelines for Cardiopulmonary Extracorporeal Life Support. Extracorporeal Life Support Organization, Version 1.4 December Ann Arbor, MI, USA. Available online: https://www.elso.org/Portals/0/ELSOGuidelinesNeonatalRespiratoryFailurev1_4_1.pdf. (accessed on 16 March 2021).
- Rawat, M.; Chandrasekharan, P.K.; Williams, A.; Gugino, S.; Koenigsknecht, C.; Swartz, D.; Ma, C.X.; Mathew, B.; Nair, J.; Lakshminrusimha, S. Oxygen Saturation Index and Severity of Hypoxic Respiratory Failure. Neonatology 2015, 107, 161–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansen, A.R.; Eichenwald, E.C.; Stark, A.R.; Martin, C.R. Cloherty and Stark’s Manual of Neonatal Care, 8th ed.; Wolters Kluver: Alphen upon Rhine, The Netherlands, 2017. [Google Scholar]
- Goel, A.; Nangia, S.; Saili, A.; Garg, A.; Sharma, S.; Randhawa, V.S. Role of prophylactic antibiotics in neo-nates born through meconium-stained amniotic fluid (MSAF)—A randomized controlled trial. Eur. J. Pediatr. 2015, 174, 237–243. [Google Scholar] [CrossRef]
- Natarajan, C.K.; Sankar, M.J.; Jain, K.; Agarwal, R.; Paul, V.K. Surfactant therapy and antibiotics in neonates with meconium aspiration syndrome: A systematic review and meta-analysis. J. Perinatol. 2016, 36, S49–S54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glaser, M.A.; Hughes, L.M.; Jnah, A.; Newberry, D. Neonatal Sepsis: A Review of Pathophysiology and Current Management Strategies. Adv. Neonatal Care 2021, 21, 49–60. [Google Scholar] [CrossRef]
- Pandita, A.; Murki, S.; Oleti, T.P.; Tandur, B.; Kiran, S.; Narkhede, S.; Prajapati, A. Effect of Nasal Continuous Positive Airway Pressure on Infants With Meconium Aspiration Syndrome. JAMA Pediatr. 2018, 172, 161–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiswell, T.E.; Gannon, C.M.; Jacob, J.; Goldsmith, L.; Szyld, E.; Weiss, K.; Schutzman, D.; Cleary, G.M.; Filipov, P.; Kurlat, I.; et al. Delivery room management of the apparently vigorous meco-nium-stained neonate: Results of the multicenter, international collaborative trial. Pediatrics 2000, 105 Pt 2, 1–7. [Google Scholar] [CrossRef]
- Polin, R.A.; Carlo, W.A.; Committee on Fetus and Newborn; American Academy of Pediatrics. Surfactant Replacement Therapy for Preterm and Term Neonates With Respiratory Distress. Pediatriacs 2013, 133, 156–163. [Google Scholar] [CrossRef] [Green Version]
- Canadian Pediatric Society. Recommendation for neonatal surfactant therapy. Paediatr. Child. Health 2004, 2, 109–116. [Google Scholar]
- El Shahed, A.; Dargaville, P.A.; Ohlsson, A.; Soll, R. Surfactant for meconium aspiration syndrome in term and late preterm infants. Cochrane Database Syst. Rev. 2014, 12, CD002054. [Google Scholar] [CrossRef]
- Dargaville, P.A.; Mills, J.F. Surfactant therapy for meconium aspiration syndrome: Current status. Drugs 2005, 65, 2569–2591. [Google Scholar] [CrossRef] [PubMed]
- Burke-Strickland, M.; Edwards, N.B. Meconium aspiration in the newborn. Minn. Med. 1973, 56, 1031–1035. [Google Scholar] [PubMed]
- Carson, B.S.; Losey, R.W.; Bowes, W.A., Jr.; Simmons, M.A. Combined obstetric and pediatric approach to prevent meconium aspiration syndrome. Am. J. Obstet. Gynecol. 1976, 126, 712–715. [Google Scholar] [CrossRef]
- Ibara, S.; Ikenoue, T.; Murata, Y.; Sakamoto, H.; Saito, T.; Nakamura, Y.; Asano, H.; Hirano, T.; Kuraya, K.; Maruyama, H.; et al. Management of meconium aspiration syndrome by tracheobronchial lavage and replacement of Surfactant-TA. Acta Pediatr. Jpn. 1995, 37, 64–67. [Google Scholar] [CrossRef] [PubMed]
- Mosca, F.; Colnaghi, M.; Castoldi, F. Lung lavage with a saline volume similar to functional residual capacity followed by surfactant administration in newborns with severe meconium aspiration syndrome. Intensive Care Med. 1996, 22, 1412–1413. [Google Scholar] [CrossRef] [PubMed]
- Hahn, S.; Choi, H.J.; Soll, R.; Dargaville, P.A. Lung lavage for meconium aspiration syndrome in newborn infants. Cochrane Database Syst. Rev. 2013, 4, CD003486. [Google Scholar] [CrossRef] [PubMed]
- Sokol, G.M.; Konduri, G.G.; Van Meurs, K.P. Inhaled nitric oxide therapy for pulmonary disorders of the term and preterm infant. Semin. Perinatol. 2016, 40, 356–369. [Google Scholar] [CrossRef] [Green Version]
- Wessel, D.L.; Adatia, I.; Van Marter, L.J.; Thompson, J.E.; Kane, J.W.; Stark, A.R.; Kourembanas, S. Improved oxygenation in a randomized trial of inhaled nitric oxide for persistent pulmonary hypertension of the newborn. Pediatrics 1997, 100, e7. [Google Scholar] [CrossRef] [Green Version]
- Kinsella, J.P.; Truog, W.E.; Walsh, W.F.; Goldberg, R.N.; Bancalari, E.; Mayock, D.E.; Redding, G.J.; Delemos, R.A.; Sardesai, S.; McCurnin, D.C.; et al. Randomized, multicenter trial of inhaled nitric oxide and high-frequency oscillatory ventilation in severe, persistent pulmonary hypertension of the newborn. J. Pediatr. 1997, 131 Pt 1, 55–62. [Google Scholar] [CrossRef]
- Abraham, E.; Evans, T. Corticosteroids and septic shock. JAMA 2002, 288, 886–887. [Google Scholar] [CrossRef]
- Subhedar, N.V.; Duffy, K.; Ibrahim, H. Corticosteroids for treating hypotension in preterm infants. Cochrane Database Syst. Rev. 2011, 12, CD003662. [Google Scholar] [CrossRef]
- Perez, M.; Lakshminrusimha, S.; Wedgwood, S.; Czech, L.; Gugino, S.F.; Russell, J.A.; Farrow, K.N.; Steinhorn, R.H. Hydro-cortisone normalizes oxygenation and cGMP regulation in lambs with persistent pulmonary hypertensio of the newborn. Am. J. Physiol. Lung Cell Mol. Physiol. 2012, 302, L595–L603. [Google Scholar] [CrossRef] [Green Version]
- Tripathi, S.; Saili, A. The Effect of Steroids on the Clinical Course and Outcome of Neonates with Meconium Aspiration Syndrome. J. Trop. Pediatr. 2007, 53, 8–12. [Google Scholar] [CrossRef]
- Alsaleem, M.; Malik, A.; Lakshminrusimha, S.; Kumar, V.H. Hydrocortisone Improves Oxygenation Index and Systolic Blood Pressure in Term Infants With Persistent Pulmonary Hypertension. Clin. Med. Insights Pediatr. 2019, 13. [Google Scholar] [CrossRef] [Green Version]
- Ward, M.C.; Sinn, J.K. Steroid therapy for meconium aspiration syndrome in newborn infants. Cochrane Database Syst. Rev. 2003, 2003, CD003485. [Google Scholar] [CrossRef] [PubMed]
- Garg, N.; Choudhary, M.; Sharma, D.; Dabi, D.; Choudhary, J.S.; Choudhary, S.K. The role of early inhaled budesonide therapy in meconium aspiration in term newborns: A randomized control study. J. Matern. Neonatal Med. 2016, 29, 36–40. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-H.; Jeng, M.-J.; Kuo, B.I.-T.; Kou, Y.R. Effects of Surfactant Lavage Combined With Intratracheal Budesonide Instillation on Meconium-Injured Piglet Lungs. Pediatr. Crit. Care Med. 2016, 17, e287–e295. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, E.; Rabe, H. The Use of Cardiotonic Drugs in Neonates. Clin. Perinatol. 2019, 46, 273–290. [Google Scholar] [CrossRef] [PubMed]
- Short, B.L. Extracorporeal membrane oxygenation: Use in meconium aspiration syndrome. J. Perinatol. 2008, 28 (Suppl. S3), S79–S83. [Google Scholar] [CrossRef] [Green Version]
- Wild, K.T.; Rintoul, N.; Kattan, J.; Gray, B. Extracorporeal Life Support Organization (ELSO): Guidelines for Neonatal Res-piratory Failure. ASAIO J. 2020, 66, 463–470. [Google Scholar] [CrossRef]
- Fliman, P.J.; Deregnier, R.-A.O.; Kinsella, J.P.; Reynolds, M.; Rankin, L.L.; Steinhorn, R.H. Neonatal extracorporeal life support: Impact of new therapies on survival. J. Pediatr. 2006, 148, 595–599. [Google Scholar] [CrossRef]
- Barbaro, R.P.; Paden, M.L.; Guner, Y.S.; Raman, L.; Ryerson, L.M.; Alexander, P.; Nasr, V.G.; Bembea, M.M.; Rycus, P.T.; Thiagarajan, R.R.; et al. Pediatric Extracorporeal Life Support Organization Registry International Report. ASAIO J. 2017, 63, 456–463. [Google Scholar] [CrossRef] [PubMed]
- Padalino, M.A.; Doglioni, N.; Nardo, D.; Baraldi, E.; Vida, V.L.; Trevisanuto, D. The “Hub and Spoke” (HandS) ECMO for “Resuscitating” Neonates with Respiratory Life-Threatening Conditions. Children 2021, 8, 24. [Google Scholar] [CrossRef] [PubMed]
- Wyckoff, M.H.; Wyllie, J.; Aziz, K.; de Almeida, M.F.; Fabres, J.; Fawke, J.; Guinsburg, R.; Hosono, S.; Isayama, T.; Kapadia, V.S.; et al. Neonatal Life Support Collaborators. Neonatal Life Support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation 2020, 142 (Suppl. 1), S185–S221. [Google Scholar] [CrossRef]
- Anand, V.; Basu, S.; Yadav, S.S.; Narayan, G.; Bhatia, B.D.; Kumar, A. Activation of Toll-like receptors in meconium aspiration syndrome. J. Perinatol. 2018, 38, 137–141. [Google Scholar] [CrossRef] [PubMed]
- Singh, B.S.; Clark, R.H.; Powers, R.J.; Spitzer, A.R. Meconium aspiration syndrome remains a significant problem in the NICU: Outcomes and treatment patterns in term neonates admitted for intensive care during a ten-year period. J. Perinatol. 2009, 29, 497–503. [Google Scholar] [CrossRef] [Green Version]
- Wilmott, R.W.; Bush, A.; Deterding, R.; Ratjen, F.; Sly, P.; Zar, H.J.; Li, A.P. Kendig’s Disorders of the Respiratory Tract in Children, 9th ed.; Elsevier: Amsterdam, The Netherlands, 2019. [Google Scholar]
- Gülmezoglu, A.M.; A Crowther, C.; Middleton, P.; Heatley, E. Induction of labour for improving birth outcomes for women at or beyond term. Cochrane Database Syst. Rev. 2012, 6, CD004945. [Google Scholar] [CrossRef] [PubMed]
- Beligere, N.; Rao, R. Neurodevelopmental outcome of infants with meconium aspiration syndrome: Report of a study and literature review. J. Perinatol. 2008, 28, S93–S101. [Google Scholar] [CrossRef] [Green Version]
- Saccone, G.; Berghella, V. Induction of labour at full term in uncomplicated singleton gestations: A systematic review and meta-analysis of randomized controlled trials. Am. J. Obstet. Gynecol. 2015, 213, 629–636. [Google Scholar] [CrossRef] [Green Version]
- Liu, W.F.; Harrington, T. Delivery Room Risk Factors for Meconium Aspiration Syndrome. Am. J. Perinatol. 2002, 19, 367–378. [Google Scholar] [CrossRef]
- Hofmeyr, G.J.; Xu, H.; Eke, A.C. Amnioinfusion for meconium-stained liquor in labour. Cochrane Database Syst. Rev. 2014, 2014, CD000014. [Google Scholar] [CrossRef] [PubMed]
- Chabra, S. Evolution of delivery room management for meconium-stained infants: Recent updates. Adv. Neonatal Care 2018, 18, 267–275. [Google Scholar] [CrossRef]
- James, L.S. Resuscitation of the Newborn Infant, 1st ed.; Abramson, H., Ed.; CV Mosby Co.: St. Louis, MO, USA, 1960; pp. 141–160. [Google Scholar]
- Gregory, G.A.; Gooding, C.A.; Phibbs, R.H.; Tooley, W.H. Meconium aspiration in infants—A prospective study. J. Pediatr. 1974, 85, 848–852. [Google Scholar] [CrossRef]
- Ting, P.; Brady, J.P. Tracheal suction in meconium aspiration. Am. J. Obstet. Gynecol. 1975, 122, 767–771. [Google Scholar] [CrossRef]
- Linder, N.; Aranda, J.; Tsur, M.; Matoth, I.; Yatsiv, I.; Mandelberg, H.; Rottem, M.; Feigenbaum, D.; Ezra, Y.; Tamir, I. Need for endotracheal intubation and suction in meconium-stained neonates. J. Pediatr. 1988, 112, 613–615. [Google Scholar] [CrossRef]
- Bloom, R.S.; Cropley, C. Textbook of Neonatal Resuscitation; AHA/AAP Neonatal Resuscitation Steering Committee, American Academy of Pediatrics and American Heart Association: Dallas, TX, USA, 1987. [Google Scholar]
- Emergency Cardiac Care Committee and Sub-committees, American Heart Association. Guidelines for cardiopulmonary resuscitation and emergency cardiac care. Part VII. Neonatal resuscitation. JAMA 1992, 268, 2276–2281. [Google Scholar]
- Bloom, R.S.; Cropley, C. Textbook of Neonatal Resuscitation; AHA/AAP Neonatal Resuscitation Steering Committee, American Academy of Pediatrics and American Heart Association: Dallas, TX, USA, 1994. [Google Scholar]
- Niermeyer, S.; Kattwinkel, J.; Van Reempts, P.; Nadkarni, V.; Phillips, B.; Zideman, D.; Azzopardi, D.; Berg, R.; Boyle, D.; Boyle, R.; et al. International Guidelines for Neonatal Resuscitation: An excerpt from the Guidelines 2000 for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care: International Consensus on Science. Contributors and Reviewers for the Neonatal Resuscitation Guidelines. Pediatrics 2000, 106, E29. [Google Scholar] [PubMed] [Green Version]
- Kattwinkel, J. Textbook of Neonatal Resuscitation, 4th ed.; American Academy of Pediatrics: Itasca, IL, USA, 2000. [Google Scholar]
- Kattwinkel, J. Textbook of Neonatal Resuscitation, 5th ed.; American Academy of Pediatrics: Itasca, IL, USA; American Heart Association: Dallas, TX, USA, 2006. [Google Scholar]
- The International Liaison Committee on Resuscitation. The International Liaison Committee on Resuscitation (ILCOR) Consensus on Science With Treatment Recommendations for Pediatric and Neonatal Patients: Pediatric Basic and Advanced Life Support. Pediatrics 2006, 117, e955–e977. [Google Scholar] [CrossRef] [PubMed]
- Perlman, J.M.; Wyllie, J.; Kattwinkel, J.; Atkins, D.L.; Chameides, L.; Goldsmith, J.P.; Guinsburg, R.; Hazinski, M.F.; Morley, C.; Richmond, S.; et al. Neonatal Resuscitation Chapter Collaborators. Part 11: Neonatal resuscitation: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation 2010, 122 (16 Suppl 2), S516–S538. [Google Scholar] [CrossRef] [Green Version]
- Perlman, J.M.; Wyllie, J.; Kattwinkel, J.; Wyckoff, M.H.; Aziz, K.; Guinsburg, R.; Kim, H.S.; Liley, H.G.; Mildenhall, L.; Simon, W.M.; et al. Neonatal Resuscitation Chapter Collaborators. Part 7: Neonatal Resuscitation: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation 2015, 132 (Suppl. 1), S204–S241. [Google Scholar] [CrossRef] [Green Version]
- Weiner, G.M. Textbook of Neonatal Resuscitation, 7th ed.; American Academy of Pediatrics: Itasca, IL, USA, 2016. [Google Scholar]
- Trevisanuto, D.; Strand, M.L.; Kawakami, M.D.; Fabres, J.; Szyld, E.; Nation, K.; Wyckoff, M.H.; Rabi, Y.; Lee, H.C. International Liaison Committee on Resuscitation Neonatal Life Support Task Force. Tracheal suctioning of meconium at birth for non-vigorous infants: A systematic review and meta-analysis. Resuscitation 2020, 149, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Phattraprayoon, N.; Tangamornsuksan, W.; Ungtrakul, T. Outcomes of endotracheal suctioning in non-vigorous neonates born through meconium-stained amniotic fluid: A systematic review and meta-analysis. Arch. Dis. Child. Fetal Neonatal Ed. 2021, 106, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Wiswell, T.E. Appropriate Management of the Nonvigorous Meconium-Stained Neonate: An Unanswered Question. Pediatrics 2018, 142, e20183052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oommen, V.I.; Ramaswamy, V.V.; Szyld, E.; Roehr, C.C. Resuscitation of non-vigorous neonates born through meconi-um-stained amniotic fluid: Post policy change impact analysis. Arch. Dis. Child. Fetal Neonatal Ed. 2020, 22. [Google Scholar] [CrossRef]
- Cavallin, F.; Res, G.; Monfredini, C.; Doglioni, N.; Villani, P.E.; Weiner, G.; Trevisanuto, D. Time needed to intubate and suction a manikin prior to instituting positive pressure ventilation: A simulation trial. Eur. J. Pediatr. 2021, 180, 247–252. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Monfredini, C.; Cavallin, F.; Villani, P.E.; Paterlini, G.; Allais, B.; Trevisanuto, D. Meconium Aspiration Syndrome: A Narrative Review. Children 2021, 8, 230. https://doi.org/10.3390/children8030230
Monfredini C, Cavallin F, Villani PE, Paterlini G, Allais B, Trevisanuto D. Meconium Aspiration Syndrome: A Narrative Review. Children. 2021; 8(3):230. https://doi.org/10.3390/children8030230
Chicago/Turabian StyleMonfredini, Chiara, Francesco Cavallin, Paolo Ernesto Villani, Giuseppe Paterlini, Benedetta Allais, and Daniele Trevisanuto. 2021. "Meconium Aspiration Syndrome: A Narrative Review" Children 8, no. 3: 230. https://doi.org/10.3390/children8030230
APA StyleMonfredini, C., Cavallin, F., Villani, P. E., Paterlini, G., Allais, B., & Trevisanuto, D. (2021). Meconium Aspiration Syndrome: A Narrative Review. Children, 8(3), 230. https://doi.org/10.3390/children8030230