
Neonatal Respiratory Distress Secondary to Meconium Aspiration Syndrome



{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Etiology
- Respiratory distress (tachypnea, grunting and/or retractions);
- Requirement for supplemental oxygen to maintain hemoglobin oxygen saturation >92%;
- Requirement for supplemental oxygen beginning prior to 2 h of life, and lasting at least 12 h;
- Absence of congenital anomalies of the airway or heart.
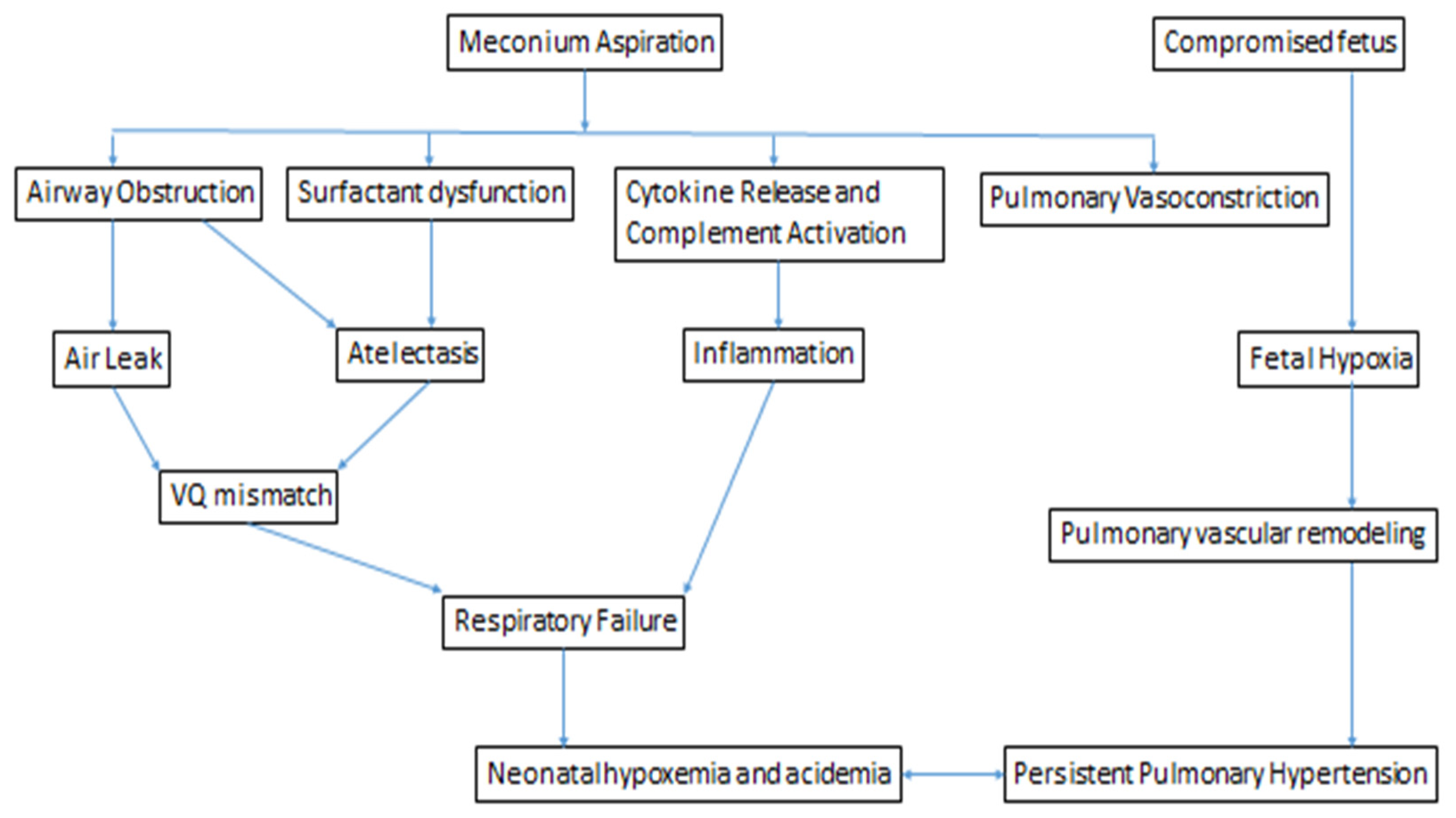
1.2. Pathophysiology
1.3. Airway Obstruction
1.4. Inflammation
1.5. Surfactant Dysfunction
1.6. Persistent Pulmonary Hypertension of the Newborn
1.7. Clinical
2. Management
2.1. Delivery Room
2.2. NICU
2.3. Prognosis
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Martin, R.J.; Fanaroff, A.A.; Walsh, M.C. Fanaroff and Martin’s Neonatal-Perinatal Medicine: Diseases of the Fetus and Infant, 11th ed.; Elsevier: Philadeplhia, PA, USA, 2020. [Google Scholar]
- Lindenskov, P.H.; Castellheim, A.; Saugstad, O.D.; Mollnes, T.E. Meconium aspiration syndrome: Possible pathophysiological mechanisms and future potential therapies. Neonatology 2015, 107, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Fanaroff, A.A.; Fanaroff, J.M.; Klaus, M.H. Klaus & Fanaroff’s Care of the High-Risk Neonate, 6th ed.; Elsevier/Saunders: Philadelphia, PA, USA, 2013; p. xiv. 626p. [Google Scholar]
- Yoder, B.A.; Kirsch, E.A.; Barth, W.H.; Gordon, M.C. Changing obstetric practices associated with decreasing incidence of meconium aspiration syndrome. Obstet. Gynecol. 2002, 99, 731–739. [Google Scholar] [CrossRef]
- Zhang, X.; Kramer, M.S. Variations in mortality and morbidity by gestational age among infants born at term. J. Pediatr. 2009, 154, 358–362. [Google Scholar] [CrossRef] [PubMed]
- Dargaville, P.A.; Copnell, B. The epidemiology of meconium aspiration syndrome: Incidence, risk factors, therapies, and outcome. Pediatrics 2006, 117, 1712–1721. [Google Scholar] [CrossRef] [PubMed]
- Lakshmanan, J.; Ahanya, S.N.; Rehan, V.; Oyachi, N.; Ross, M.G. Elevated plasma corticotrophin release factor levels and in utero meconium passage. Pediatr. Res. 2007, 61, 176–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramon y Cajal, C.L.; Martinez, R.O. Defecation in utero: A physiologic fetal function. Am. J. Obstet. Gynecol. 2003, 188, 153–156. [Google Scholar] [CrossRef] [PubMed]
- Khazardoost, S.; Hantoushzadeh, S.; Khooshideh, M.; Borna, S. Risk factors for meconium aspiration in meconium stained amniotic fluid. J. Obstet. Gynaecol. 2007, 27, 577–579. [Google Scholar] [CrossRef] [PubMed]
- Chettri, S.; Bhat, B.V.; Adhisivam, B. Current Concepts in the Management of Meconium Aspiration Syndrome. Indian J. Pediatr. 2016, 83, 1125–1130. [Google Scholar] [CrossRef] [PubMed]
- Rawat, M.; Nangia, S.; Chandrasekharan, P.; Lakshminrusimha, S. Approach to Infants Born Through Meconium Stained Amniotic Fluid: Evolution Based on Evidence? Am. J. Perinatol. 2018, 35, 815–822. [Google Scholar] [CrossRef] [PubMed]
- Wiswell, T.E.; Knight, G.R.; Finer, N.N.; Donn, S.M.; Desai, H.; Walsh, W.F.; Sekar, K.C.; Bernstein, G.; Keszler, M.; Visser, V.E.; et al. A multicenter, randomized, controlled trial comparing Surfaxin (Lucinactant) lavage with standard care for treatment of meconium aspiration syndrome. Pediatrics 2002, 109, 1081–1087. [Google Scholar] [CrossRef]
- Fuloria, M.; Wiswell, T.E. Resuscitation of the meconium-stained infant and prevention of meconium aspiration syndrome. J. Perinatol. 1999, 19, 234–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salvesen, B.; Nielsen, E.W.; Harboe, M.; Saugstad, O.D.; Mollnes, T.E. Mechanisms of complement activation and effects of C1-inhibitor on the meconium-induced inflammatory reaction in human cord blood. Mol. Immunol. 2009, 46, 688–694. [Google Scholar] [CrossRef] [PubMed]
- Goldsmith, J.P.; Karotkin, E.H. Assisted Ventilation of the Neonate, 5th ed.; Elsevier/Saunders: St. Louis, MO, USA, 2011; p. xvii. 631p. [Google Scholar]
- Natarajan, C.K.; Sankar, M.J.; Jain, K.; Agarwal, R.; Paul, V.K. Surfactant therapy and antibiotics in neonates with meconium aspiration syndrome: A systematic review and meta-analysis. J. Perinatol. 2016, 36 (Suppl. 1), S49–S54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janssen, D.J.; Carnielli, V.P.; Cogo, P.; Bohlin, K.; Hamvas, A.; Luijendijk, I.H.; Bunt, J.E.; Tibboel, D.; Zimmermann, L.J. Surfactant phosphatidylcholine metabolism in neonates with meconium aspiration syndrome. J. Pediatr. 2006, 149, 634–639. [Google Scholar] [CrossRef]
- Wiswell, T.E.; Gannon, C.M.; Jacob, J.; Goldsmith, L.; Szyld, E.; Weiss, K.; Schutzman, D.; Cleary, G.M.; Filipov, P.; Kurlat, I.; et al. Delivery room management of the apparently vigorous meconium-stained neonate: Results of the multicenter, international collaborative trial. Pediatrics 2000, 105, 1–7. [Google Scholar] [CrossRef]
- Pierce, J.; Gaudier, F.L.; Sanchez-Ramos, L. Intrapartum amnioinfusion for meconium-stained fluid: Meta-analysis of prospective clinical trials. Obstet. Gynecol. 2000, 95, 1051–1056. [Google Scholar] [CrossRef]
- Fraser, W.D.; Hofmeyr, J.; Lede, R.; Faron, G.; Alexander, S.; Goffinet, F.; Ohlsson, A.; Goulet, C.; Turcot-Lemay, L.; Prendiville, W.; et al. Amnioinfusion for the prevention of the meconium aspiration syndrome. N. Engl. J. Med. 2005, 353, 909–917. [Google Scholar] [CrossRef]
- Practice, A.C.O. ACOG Committee Opinion Number 346, October 2006: Amnioninfusion does not prevent meconium aspiration syndrome. Obstet. Gynecol. 2006, 108, 1053. [Google Scholar] [CrossRef]
- Vain, N.E.; Szyld, E.G.; Prudent, L.M.; Wiswell, T.E.; Aguilar, A.M.; Vivas, N.I. Oropharyngeal and nasopharyngeal suctioning of meconium-stained neonates before delivery of their shoulders: Multicentre, randomised controlled trial. Lancet 2004, 364, 597–602. [Google Scholar] [CrossRef]
- American Heart Association. Textbook of Neonatal Resuscitation, 7th ed.; American Acadamy of Pediatrics and the American Heart Association: Elk Grove Village, IL, USA, 2016. [Google Scholar]
- Perlman, J.M.; Wyllie, J.; Kattwinkel, J.; Atkins, D.L.; Chameides, L.; Goldsmith, J.P.; Guinsburg, R.; Hazinski, M.F.; Morley, C.; Richmond, S.; et al. Part 11: Neonatal resuscitation: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Circulation 2010, 122, S516–S538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perlman, J.M.; Wyllie, J.; Kattwinkel, J.; Wyckoff, M.H.; Aziz, K.; Guinsburg, R.; Kim, H.S.; Liley, H.G.; Mildenhall, L.; Simon, W.M.; et al. Part 7: Neonatal Resuscitation: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Circulation 2015, 132, S204–S241. [Google Scholar] [CrossRef] [Green Version]
- Lakshminrusimha, S.; Swartz, D.D.; Gugino, S.F.; Ma, C.X.; Wynn, K.A.; Ryan, R.M.; Russell, J.A.; Steinhorn, R.H. Oxygen concentration and pulmonary hemodynamics in newborn lambs with pulmonary hypertension. Pediatr. Res. 2009, 66, 539–544. [Google Scholar] [CrossRef] [Green Version]
- El Shahed, A.I.; Dargaville, P.; Ohlsson, A.; Soll, R.F. Surfactant for meconium aspiration syndrome in full term/near term infants. Cochrane Database Syst. Rev. 2007. [Google Scholar] [CrossRef]
- El Shahed, A.I.; Dargaville, P.A.; Ohlsson, A.; Soll, R. Surfactant for meconium aspiration syndrome in term and late preterm infants. Cochrane Database Syst. Rev. 2014. [Google Scholar] [CrossRef]
- Dargaville, P.A.; Mills, J.F.; Copnell, B.; Loughnan, P.M.; McDougall, P.N.; Morley, C.J. Therapeutic lung lavage in meconium aspiration syndrome: A preliminary report. J. Paediatr. Child Health 2007, 43, 539–545. [Google Scholar] [CrossRef] [PubMed]
- Dargaville, P.A.; Copnell, B.; Mills, J.F.; Haron, I.; Lee, J.K.; Tingay, D.G.; Rohana, J.; Mildenhall, L.F.; Jeng, M.J.; Narayanan, A.; et al. Randomized controlled trial of lung lavage with dilute surfactant for meconium aspiration syndrome. J. Pediatr. 2011, 158, 383–389 e382. [Google Scholar] [CrossRef] [PubMed]
- Lotze, A.; Mitchell, B.R.; Bulas, D.I.; Zola, E.M.; Shalwitz, R.A.; Gunkel, J.H. Multicenter study of surfactant (beractant) use in the treatment of term infants with severe respiratory failure. Survanta in Term Infants Study Group. J. Pediatr. 1998, 132, 40–47. [Google Scholar] [CrossRef]
- Davis, P.J.; Shekerdemian, L.S. Meconium aspiration syndrome and extracorporeal membrane oxygenation. Arch. Dis. Child. Fetal Neonatal Ed. 2001, 84, F1–F3. [Google Scholar] [CrossRef] [PubMed] [Green Version]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olicker, A.L.; Raffay, T.M.; Ryan, R.M. Neonatal Respiratory Distress Secondary to Meconium Aspiration Syndrome. Children 2021, 8, 246. https://doi.org/10.3390/children8030246
Olicker AL, Raffay TM, Ryan RM. Neonatal Respiratory Distress Secondary to Meconium Aspiration Syndrome. Children. 2021; 8(3):246. https://doi.org/10.3390/children8030246
Chicago/Turabian StyleOlicker, Arielle L., Thomas M. Raffay, and Rita M. Ryan. 2021. "Neonatal Respiratory Distress Secondary to Meconium Aspiration Syndrome" Children 8, no. 3: 246. https://doi.org/10.3390/children8030246
APA StyleOlicker, A. L., Raffay, T. M., & Ryan, R. M. (2021). Neonatal Respiratory Distress Secondary to Meconium Aspiration Syndrome. Children, 8(3), 246. https://doi.org/10.3390/children8030246