
Respiratory Trajectory after Invasive Interventions for Patent Ductus Arteriosus of Preterm Infants

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Setting
2.3. Variable Collection or Definition
2.3.1. Clinical Variables
2.3.2. Definition of HS-PDA and the Procedure of Interventions
2.3.3. Primary Outcome: Post-Intervention Respiratory Trajectory
2.4. Statistic Analysis
3. Results
4. Discussion
4.1. Comparision of Invasive Techniques in Closing PDA in VLBW Infants
4.2. Respiratory Outcomes after Invasive PDA Closure
4.3. Potential Benefits and Disadvantages for Transcatheter Occlusion
4.4. Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Transcatheter Occlusion (n = 14) | Surgical Ligation (n = 17) | p-Value | |
|---|---|---|---|
| Bleeding tendency, n | 5 | 3 | 0.245 |
| Pulmonary hemorrhage, n | 5 | 1 | |
| Coagulopathy/Thrombocytopenia, n | 0 | 1 | |
| GI bleeding, n | 0 | 1 | |
| Failed medical treatment, n | 6 | 13 | |
| Necrotizing enterocolitis, n | 1 | 0 | |
| Renal failure, n | 2 | 1 |
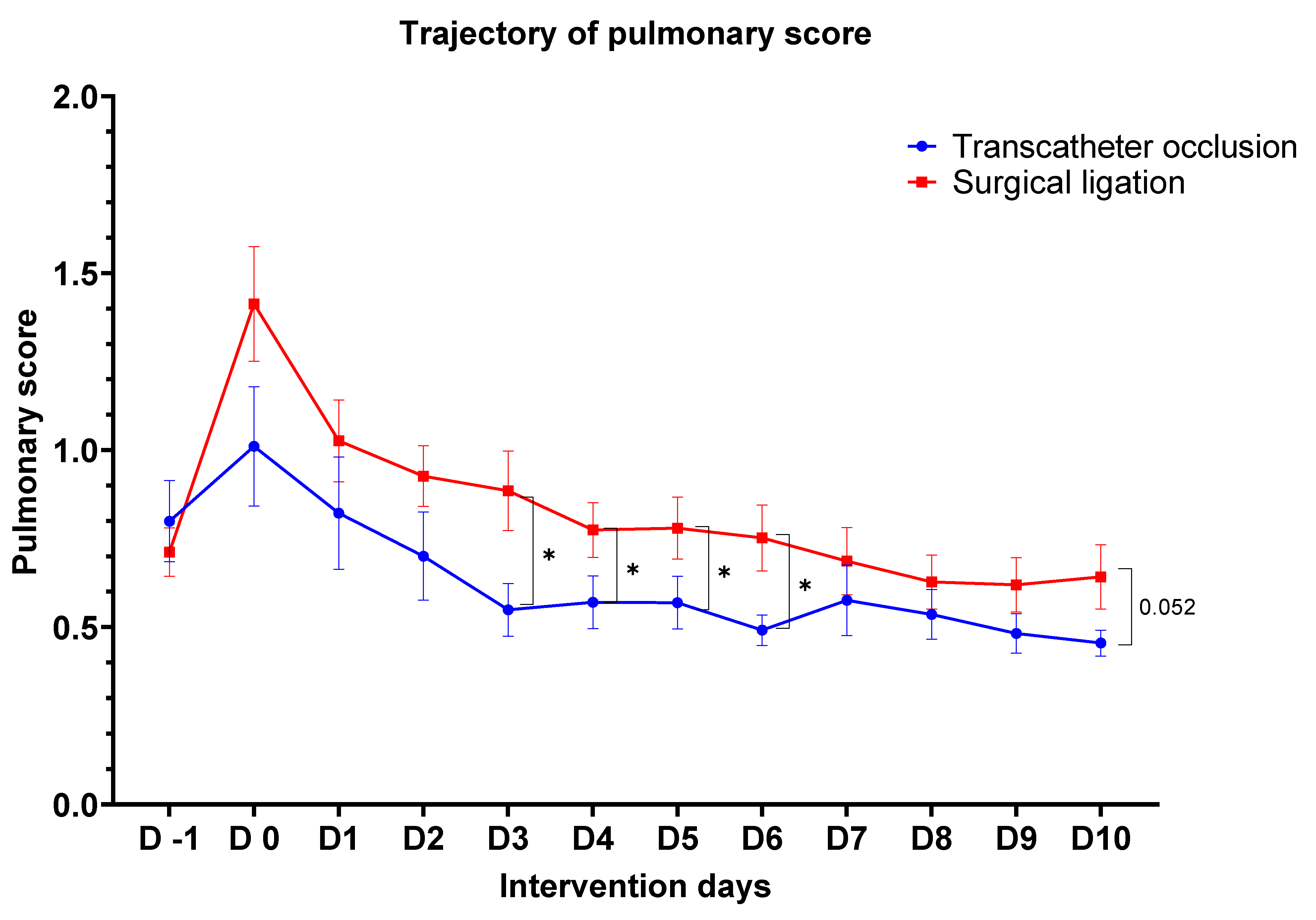
| D-1 | D0 | D1 | D2 | D3 | D4 | D5 | D6 | D7 | D8 | D9 | D10 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Group A (n = 14) | 0.80 | 1.01 | 0.82 | 0.70 | 0.55 | 0.57 | 0.57 | 0.49 | 0.58 | 0.54 | 0.48 | 0.46 |
| (0.11) | (0.17) | (0.16) | (0.12) | (0.07) | (0.07) | (0.07) | (0.04) | (0.10) | (0.07) | (0.06) | (0.04) | |
| Group B (n = 17) | 0.71 | 1.41 | 1.03 | 0.93 | 0.89 | 0.77 | 0.78 | 0.75 | 0.69 | 0.63 | 0.62 | 0.64 |
| (0.07) | (0.16) | (0.12) | (0.09) | (0.11) | (0.08) | (0.09) | (0.09) | (0.09) | (0.08) | (0.08) | (0.09) | |
| p-value | 0.504 | 0.097 | 0.296 | 0.072 | 0.014 | 0.037 | 0.047 | 0.011 | 0.285 | 0.241 | 0.102 | 0.052 |
| Transcatheter | Surgery | p-Value | |
|---|---|---|---|
| Mean arterial pressure, mmHg | |||
| Pre-procedural | 39.0 ± 10.0 | 43.5 ± 10.5 | 0.238 |
| Post-procedural | 47.4 ± 13.1 | 43.8 ± 11.4 | 0.429 |
| Inotropic equivalent | |||
| Pre-procedural | 5.0 ± 6.0 | 2.8 ± 5.6 | 0.309 |
| Post-procedural | 5.7 ± 6.6 | 3.9 ± 6.3 | 0.434 |
| Transcatheter | Surgery | p-Value | |
|---|---|---|---|
| NEC | 2 | 1 | 0.576 |
| IVH | 2 | 4 | 0.664 |
| BPD | 13 | 16 | 1.000 |
| ROP | 6 | 12 | 0.119 |
References
- Hamrick, S.E.; Hansmann, G. Patent ductus arteriosus of the preterm infant. Pediatrics 2010, 125, 1020–1030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gentile, R.; Stevenson, G.; Dooley, T.; Franklin, D.; Kawabori, I.; Pearlman, A. Pulsed Doppler echocardiographic determination of time of ductal closure in normal newborn infants. J. Pediatr. 1981, 98, 443–448. [Google Scholar] [CrossRef]
- Clyman, R.I.; Couto, J.; Murphy, G.M. Patent ductus arteriosus: Are current neonatal treatment options better or worse than no treatment at all? Semin. Perinatol. 2012, 36, 123–129. [Google Scholar] [CrossRef] [Green Version]
- Ferguson, J.M. Pharmacotherapy for patent ductus arteriosus closure. Congenit. Heart Dis. 2019, 14, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Noori, S.; McCoy, M.; Friedlich, P.; Bright, B.; Gottipati, V.; Seri, I.; Sekar, K. Failure of ductus arteriosus closure is associated with increased mortality in preterm infants. Pediatrics 2009, 123, e138–e144. [Google Scholar] [CrossRef]
- Kluckow, M.; Evans, N. Ductal shunting, high pulmonary blood flow, and pulmonary hemorrhage. J. Pediatr. 2000, 137, 68–72. [Google Scholar] [CrossRef]
- Finlay, E.R.; Subhedar, N.V. Pulmonary haemorrhage in preterm infants. Eur. J. Pediatr. 2000, 159, 870–871. [Google Scholar] [CrossRef]
- Oh, W.; Poindexter, B.B.; Perritt, R.; Lemons, J.A.; Bauer, C.R.; Ehrenkranz, R.A.; Stoll, B.J.; Poole, K.; Wright, L.L.; Neonatal Research, N. Association between fluid intake and weight loss during the first ten days of life and risk of bronchopulmonary dysplasia in extremely low birth weight infants. J. Pediatr. 2005, 147, 786–790. [Google Scholar] [CrossRef] [PubMed]
- Redline, R.W. Placental and Other Perinatal Risk Factors for Chronic Lung Disease in Very Low Birth Weight Infants. Pediatr. Res. 2002, 52, 713–719. [Google Scholar] [CrossRef]
- Fowlie, P.W.; Davis, P.G. Prophylactic indomethacin for preterm infants: A systematic review and meta-analysis. Arch. Dis. Child. Fetal Neonatal Ed. 2003, 88, F464–F466. [Google Scholar] [CrossRef] [PubMed]
- Fowlie, P.W.; Davis, P.G. Prophylactic intravenous indomethacin for preventing mortality and morbidity in preterm infants. Cochrane Database Syst. Rev. 2002, CD000174. [Google Scholar] [CrossRef]
- Evans, N.; Kluckow, M. Early ductal shunting and intraventricular haemorrhage in ventilated preterm infants. Arch. Dis. Child. Fetal Neonatal Ed. 1996, 75, F183–F186. [Google Scholar] [CrossRef]
- Dollberg, S.; Lusky, A.; Reichman, B. Patent ductus arteriosus, indomethacin and necrotizing enterocolitis in very low birth weight infants: A population-based study. J. Pediatr. Gastroenterol. Nutr. 2005, 40, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Drougia, A.; Giapros, V.; Krallis, N.; Theocharis, P.; Nikaki, A.; Tzoufi, M.; Andronikou, S. Incidence and risk factors for cerebral palsy in infants with perinatal problems: A 15-year review. Early Hum. Dev. 2007, 83, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.W.; Pickering, D. Persistent ductus arteriosus complicating the respiratory distress syndrome. Arch. Dis. Child. 1977, 52, 274–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mezu-Ndubuisi, O.J.; Agarwal, G.; Raghavan, A.; Pham, J.T.; Ohler, K.H.; Maheshwari, A. Patent ductus arteriosus in premature neonates. Drugs 2012, 72, 907–916. [Google Scholar] [CrossRef] [Green Version]
- Susheel Kumar, T.K. Surgical management of patent ductus arteriosus. Congenit. Heart Dis. 2019, 14, 57–59. [Google Scholar] [CrossRef] [Green Version]
- Su, B.H.; Lin, H.Y.; Chiu, H.Y.; Tsai, M.L.; Chen, Y.T.; Lu, I.C. Therapeutic strategy of patent ductus arteriosus in extremely preterm infants. Pediatr. Neonatol. 2020, 61, 133–141. [Google Scholar] [CrossRef]
- Gay, J.H.; Daily, W.J.; Meyer, B.H.; Trump, D.S.; Cloud, D.T.; Molthan, M.E. Ligation of the patent ductus arteriosus in premature infants: Report of 45 cases. J. Pediatr. Surg. 1973, 8, 677–683. [Google Scholar] [CrossRef]
- Nelson, R.J.; Thibeault, D.W.; Emmanouilides, G.C.; Lippmann, M. Improving the results of ligation of patent ductus arteriosus in small preterm infants. J. Thorac. Cardiovasc. Surg. 1976, 71, 169–178. [Google Scholar] [CrossRef]
- Tashiro, J.; Perez, E.A.; Sola, J.E. Reduced Hospital Mortality With Surgical Ligation of Patent Ductus Arteriosus in Premature, Extremely Low Birth Weight Infants: A Propensity Score-matched Outcome Study. Ann. Surg. 2016, 263, 608–614. [Google Scholar] [CrossRef]
- Palder, S.B.; Schwartz, M.Z.; Tyson, K.R.T.; Marr, C.C. Management of patent ductus arteriosus: A comparison of operative V pharmacologic treatment. J. Pediatr. Surg. 1987, 22, 1171–1174. [Google Scholar] [CrossRef]
- Mikhail, M.; Lee, W.; Toews, W.; Synhorst, D.P.; Hawes, C.R.; Hernandez, J.; Lockhart, C.; Whitfield, J.; Pappas, G. Surgical and medical experience with 734 premature infants with patent ductus arteriosus. J. Thorac. Cardiovasc. Surg. 1982, 83, 349–357. [Google Scholar] [CrossRef]
- Chiang, M.C.; Lin, W.S.; Lien, R.; Chou, Y.H. Reexpansion pulmonary edema following patent ductus arteriosus ligation in a preterm infant. J. Perinat. Med. 2004, 32, 365–367. [Google Scholar] [CrossRef]
- Clement, W.A.; El-Hakim, H.; Phillipos, E.Z.; Cote, J.J. Unilateral vocal cord paralysis following patent ductus arteriosus ligation in extremely low-birth-weight infants. Arch. Otolaryngol. Head Neck Surg. 2008, 134, 28–33. [Google Scholar] [CrossRef] [Green Version]
- Barikbin, P.; Sallmon, H.; Wilitzki, S.; Photiadis, J.; Buhrer, C.; Koehne, P.; Schmalisch, G. Lung function in very low birth weight infants after pharmacological and surgical treatment of patent ductus arteriosus—A retrospective analysis. BMC Pediatr. 2017, 17, 5. [Google Scholar] [CrossRef] [Green Version]
- Benjamin, J.R.; Smith, P.B.; Cotten, C.M.; Jaggers, J.; Goldstein, R.F.; Malcolm, W.F. Long-term morbidities associated with vocal cord paralysis after surgical closure of a patent ductus arteriosus in extremely low birth weight infants. J. Perinatol. 2010, 30, 408–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roksund, O.D.; Clemm, H.; Heimdal, J.H.; Aukland, S.M.; Sandvik, L.; Markestad, T.; Halvorsen, T. Left vocal cord paralysis after extreme preterm birth, a new clinical scenario in adults. Pediatrics 2010, 126, e1569–e1577. [Google Scholar] [CrossRef] [PubMed]
- Sathanandam, S.; Agrawal, H.; Chilakala, S.; Johnson, J.; Allen, K.; Knott-Craig, C.; Rush Waller, B.; Philip, R. Can transcatheter PDA closure be performed in neonates ≦1000 grams? The Memphis experience Congenit. Heart Dis. 2019, 14, 79–84. [Google Scholar] [CrossRef] [Green Version]
- Sathanandam, S.; Balduf, K.; Chilakala, S.; Washington, K.; Allen, K.; Knott-Craig, C.; Rush Waller, B.; Philip, R. Role of Transcatheter patent ductus arteriosus closure in extremely low birth weight infants. Catheter. Cardiovasc. Interv. 2019, 93, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Pamukcu, O.; Tuncay, A.; Narin, N.; Baykan, A.; Korkmaz, L.; Argun, M.; Ozyurt, A.; Sunkak, S.; Uzum, K. Patent Ductus Arteriosus closure in preterms less than 2kg: Surgery versus transcatheter. Int. J. Cardiol. 2018, 250, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez Ogando, A.; Planelles Asensio, I.; de la Blanca, A.R.S.; Ballesteros Tejerizo, F.; Sanchez Luna, M.; Gil Jaurena, J.M.; Medrano Lopez, C.; Zunzunegui Martinez, J.L. Surgical Ligation Versus Percutaneous Closure of Patent Ductus Arteriosus in Very Low-Weight Preterm Infants: Which are the Real Benefits of the Percutaneous Approach? Pediatr. Cardiol. 2018, 39, 398–410. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Schechter, M.A.; Manning, P.B.; Eghtesady, P.; Balzer, D.T.; Shahanavaz, S.; Rockefeller, T.A.; Abarbanell, A.M. Surgical Versus Percutaneous Closure of PDA in Preterm Infants: Procedural Charges and Outcomes. J. Surg. Res. 2019, 243, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.N.; Lin, Y.C.; Hsieh, M.L.; Wei, Y.J.; Ju, Y.T.; Wu, J.M. Transcatheter Closure of Patent Ductus Arteriosus in Premature Infants With Very Low Birth Weight. Front. Pediatr. 2021, 8, 615919. [Google Scholar] [CrossRef] [PubMed]
- Yeh, T.F.; Raval, D.; Luken, J.; Thalji, A.; Lilien, L.; Pildes, R.S. Clinical evaluation of premature infants with patent ductus arteriosus: A scoring system with echocardiogram, acid-base, and blood gas correlations. Crit. Care Med. 1981, 9, 655–657. [Google Scholar] [CrossRef]
- Group, T.S.-R.M.S. Supplemental Therapeutic Oxygen for Prethreshold Retinopathy of Prematurity (STOP-ROP), a randomized, controlled trial. I: Primary outcomes. Pediatrics 2000, 105, 295–310. [Google Scholar] [CrossRef]
- Skippen, P.W.; Krahn, G.E. Acute renal failure in children undergoing cardiopulmonary bypass. Crit. Care Resusc. 2005, 7, 286–291. [Google Scholar]
- Simpson, J.M.; Moore, P.; Teitel, D.F. Cardiac catheterization of low birth weight infants. Am. J. Cardiol. 2001, 87, 1372–1377. [Google Scholar] [CrossRef]
- Backes, C.H.; Cheatham, S.L.; Deyo, G.M.; Leopold, S.; Ball, M.K.; Smith, C.V.; Garg, V.; Holzer, R.J.; Cheatham, J.P.; Berman, D.P. Percutaneous Patent Ductus Arteriosus (PDA) Closure in Very Preterm Infants: Feasibility and Complications. J. Am. Heart Assoc. 2016, 5. [Google Scholar] [CrossRef] [Green Version]
- Thukaram, R.; Suarez, W.A.; Sundararaghavan, S. Transcatheter closure of the patent arterial duct using the Flipper coil in a premature infant weighing 1,400 g: A case report. Catheter. Cardiovasc. Interv. 2005, 66, 18–20. [Google Scholar] [CrossRef]
- Haneda, N.; Kato, F.; Kim, S.H. Coil closure of a large patent arterial duct in a low-birthweight infant. Pediatr. Int. 2002, 44, 317–320. [Google Scholar] [CrossRef] [PubMed]
- Hijazi, Z.M.; Lloyd, T.R.; Beekman, R.H.; Geggel, R.L. Transcatheter closure with single or multiple Gianturco coils of patent ductus arteriosus in infants weighing ≤8 kg: Retrograde versus antegrade approach. Am. Heart J. 1996, 132, 827–835. [Google Scholar] [CrossRef]
- Thibeault, D.W.; Emmanouilides, G.C.; Nelson, R.J.; Lachman, R.S.; Rosengart, R.M.; Oh, W. Patent ductus arteriosus complicating the respiratory distress syndrome in preterm infants. J. Pediatr. 1975, 86, 120–126. [Google Scholar] [CrossRef]
- Clarke, D.R.; Paton, B.C.; Way, G.L.; Stewart, J.R. Patent ductus arteriosus ligation and respiratory distress syndrome in premature infants. Ann. Thorac. Surg. 1976, 22, 138–145. [Google Scholar] [CrossRef]
- Brandt, B.; Marvin, W.J.; Ehrenhaft, J.L.; Heintz, S.; Doty, D.B. Ligation of patent ductus arteriosus in premature infants. Ann. Thorac. Surg. 1981, 32, 166–172. [Google Scholar] [CrossRef]
- Raval, M.V.; Laughon, M.M.; Bose, C.L.; Phillips, J.D. Patent ductus arteriosus ligation in premature infants: Who really benefits, and at what cost? J. Pediatr. Surg. 2007, 42, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Hsu, K.H.; Wong, P.; Ram Kumar, S.; Evans, J.; Noori, S. Predictors of Respiratory Improvement 1 Week after Ligation of Patent Ductus Arteriosus in Preterm Infants. J. Pediatr. 2019, 205, 49–54. [Google Scholar] [CrossRef]
- Hsu, K.H.; Chiang, M.C.; Lien, R.; Chu, J.J.; Chang, Y.S.; Chu, S.M.; Wong, K.S.; Yang, P.H. Diaphragmatic paralysis among very low birth weight infants following ligation for patent ductus arteriosus. Eur. J. Pediatr. 2012, 171, 1639–1644. [Google Scholar] [CrossRef]
- Satpute, M.D.; Donohue, P.K.; Vricella, L.; Aucott, S.W. Cardiovascular instability after patent ductus arteriosus ligation in preterm infants: The role of hydrocortisone. J. Perinatol. 2012, 32, 685–689. [Google Scholar] [CrossRef] [Green Version]
- Bravo, M.C.; Ybarra, M.; Madero, R.; Pellicer, A. Childhood Neurodevelopmental Outcome in Low Birth Weight Infants With Post-ligation Cardiac Syndrome After Ductus Arteriosus Closure. Front. Physiol. 2019, 10, 718. [Google Scholar] [CrossRef]
- Serrano, R.M.; Madison, M.; Lorant, D.; Hoyer, M.; Alexy, R. Comparison of ’post-patent ductus arteriosus ligation syndrome’ in premature infants after surgical ligation vs. percutaneous closure. J. Perinatol. 2020, 40, 324–329. [Google Scholar] [CrossRef]
- Dubbink-Verheij, G.H.; van Westerop, T.; Lopriore, E.; Te Pas, A.B. Hypothermia during umbilical catheterization in preterm infants. J. Matern. Fetal Neonatal Med. 2019, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zahn, E.M.; Nevin, P.; Simmons, C.; Garg, R. A novel technique for transcatheter patent ductus arteriosus closure in extremely preterm infants using commercially available technology. Catheter. Cardiovasc. Interv. 2015, 85, 240–248. [Google Scholar] [CrossRef] [PubMed]
- Morville, P.; Akhavi, A. Transcatheter closure of hemodynamic significant patent ductus arteriosus in 32 premature infants by amplatzer ductal occluder additional size-ADOIIAS. Catheter. Cardiovasc. Interv. 2017, 90, 612–617. [Google Scholar] [CrossRef]
- Rodriguez Ogando, A.; Ballesteros Tejerizo, F.; Blanco Bravo, D.; Sanchez Luna, M.; Zunzunegui Martinez, J.L. Transcatheter Occlusion of Patent Ductus Arteriosus in Preterm Infants Weighing Less Than 2 kg With the Amplatzer Duct Occluder II Additional Sizes Device. Rev. Esp. Cardiol. 2018, 71, 865–866. [Google Scholar] [CrossRef] [PubMed]


| Transcatheter Occlusion | Surgical Ligation | p-Value | |
|---|---|---|---|
| Patient information | n = 14 | n = 17 | |
| Sex, n (male: female) | 5:9 | 9:8 | 0.337 |
| Birth gestational age, weeks | 25.8 (23–29.4) | 24.7 (23.6–25.4) | 0.360 |
| Birth BW, grams | 772.5 (555–1330) | 731 (684–744) | 0.634 |
| Data related to intervention | |||
| Age of procedure, days | 20.5 (12–35) | 26 (18–38) | 0.439 |
| median (IQR) | |||
| Age range (days) | 2–91 | 11–47 | |
| D0 Body weight, grams | 1278 (478–1602) | 795 (551–1646) | 0.284 |
| median (range) | |||
| PMA on procedure day (weeks) | 30.4 ± 3.8 | 28.7 ± 1.9 | 0.149 |
| Hemodynamics before procedure | |||
| HR (beats per minutes) | 161 ± 15 | 158 ± 9 | 0.514 |
| MBP (mmHg) | 47.2 ± 13.4 | 43.6 ± 10.5 | 0.397 |
| Pre-procedural ventilation status | |||
| FiO2 (%) | 33.4 ± 14.2 | 31.1 ± 8.8 | 0.573 |
| PEEP (cmH2O) | 5 (5–6) | 5 (5–5.5) | 0.902 |
| Mean airway pressure (cmH2O) | 11 (8.0–16.3) | 8.65 (7.9–10.3) | 0.082 |
| Invasive ventilation, (n, %) | 8/14 (57%) | 9/17 (52%) | 1.000 |
| IMV, n | 2 | 8 | |
| NAVA, n | 0 | 1 | |
| HFOV, n | 6 | 0 | |
| Non-invasive ventilation, (n, %) | 6/14 (43%) | 8/17 (48%) | |
| CPAP, n | 4 | 3 | |
| NIPPV, n | 2 | 3 | |
| NIV NAVA, n | 0 | 2 | |
| Medications before procedure | |||
| Methylxanthines, n | 8 | 12 | |
| Diuretics, n | 3 | 3 | |
| Postnatal steroids, n | 3 | 2 | |
| Pre-procedural pulmonary score | 0.66 (0.55–0.88) | 0.63 (0.50–1.00) | 0.705 |
| Transcatheter Occlusion n = 14 | Surgical Ligation n = 17 | p-Value | |
|---|---|---|---|
| Duration on invasive ventilator after procedure, days | 4 (1.5–6.5) | 4 (3–6) | 0.654 |
| Duration on positive pressure ventilator after procedure, days | 31 (24–45.5) | 67 (52.5–86) | 0.033 |
| Oxygen dependent days after procedure | 38 (9–66) | 59 (25.5–163) | 0.083 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wei, Y.-J.; Chen, Y.-J.; Lin, Y.-C.; Kan, C.-D.; Hsieh, M.-L.; Lin, Y.-J.; Wu, J.-M.; Wang, J.-N. Respiratory Trajectory after Invasive Interventions for Patent Ductus Arteriosus of Preterm Infants. Children 2021, 8, 398. https://doi.org/10.3390/children8050398
Wei Y-J, Chen Y-J, Lin Y-C, Kan C-D, Hsieh M-L, Lin Y-J, Wu J-M, Wang J-N. Respiratory Trajectory after Invasive Interventions for Patent Ductus Arteriosus of Preterm Infants. Children. 2021; 8(5):398. https://doi.org/10.3390/children8050398
Chicago/Turabian StyleWei, Yu-Jen, Yen-Ju Chen, Yung-Chieh Lin, Chung-Dann Kan, Min-Ling Hsieh, Yuh-Jyh Lin, Jing-Ming Wu, and Jieh-Neng Wang. 2021. "Respiratory Trajectory after Invasive Interventions for Patent Ductus Arteriosus of Preterm Infants" Children 8, no. 5: 398. https://doi.org/10.3390/children8050398
APA StyleWei, Y. -J., Chen, Y. -J., Lin, Y. -C., Kan, C. -D., Hsieh, M. -L., Lin, Y. -J., Wu, J. -M., & Wang, J. -N. (2021). Respiratory Trajectory after Invasive Interventions for Patent Ductus Arteriosus of Preterm Infants. Children, 8(5), 398. https://doi.org/10.3390/children8050398