
Orthorexia and Eating Disorders in Adolescents and Young Adults: A Systematic Review

 ,
, 
 and
and 
Abstract
:1. Introduction
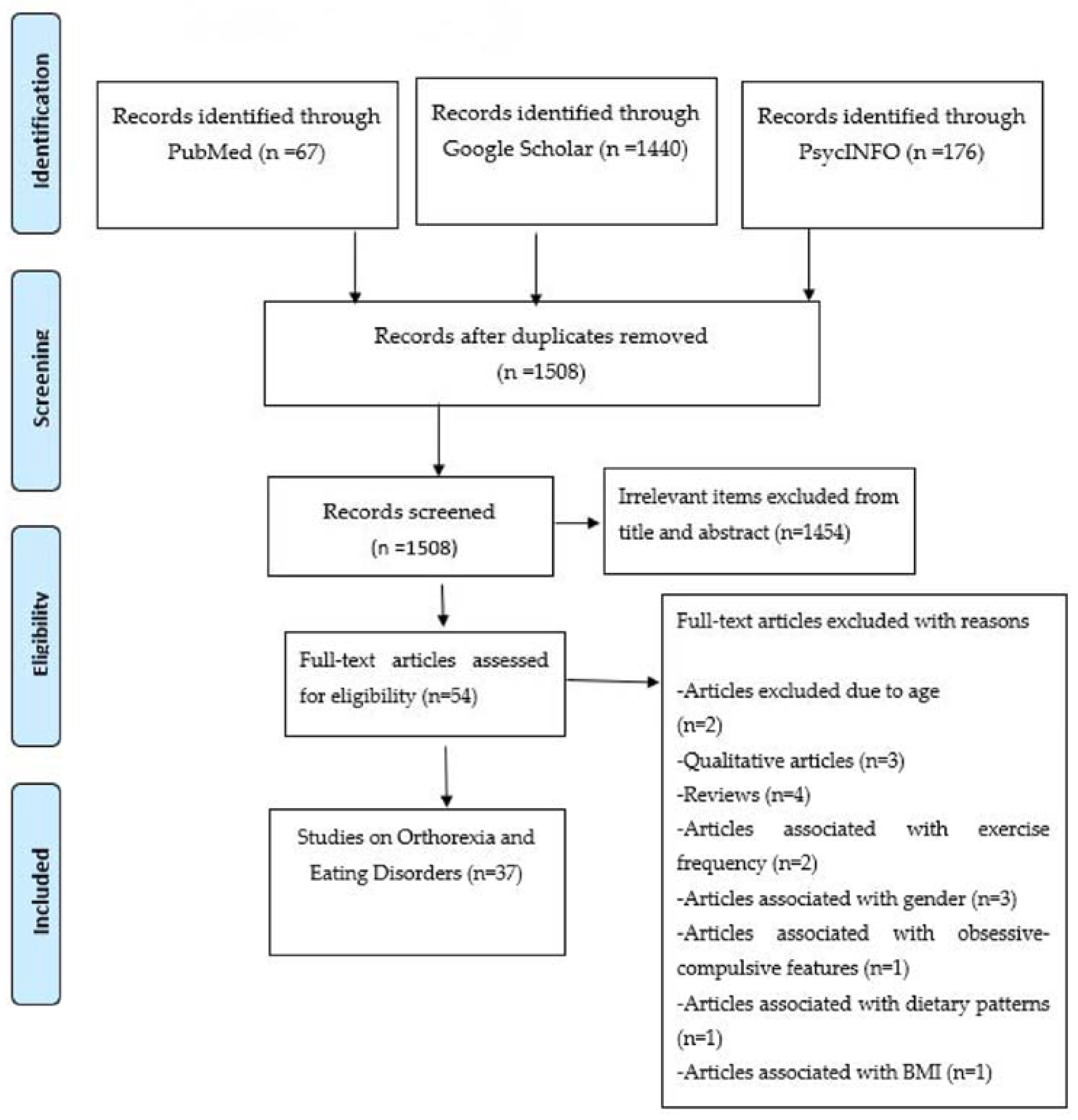
2. Materials and Methods
2.1. Literature Search Strategy
2.2. Inclusion Criteria
- Reports on young adults up to 30 years old and adolescents of any age. Studies which were based on adolescents/young adults were separately presented in our systematic review from those including a subgroup of admixture between young adults and older individuals.
- Presentation of data about possible correlations between orthorexia and eating disorders (AN and BN); the latter defined according to DSM 5 and ICD 10.
- No restrictions were posed considering diagnostic tools of eating disorders.
- Considering study design, prospective cohorts, case-control and cross-sectional studies were included.
- Only articles written in English were included.
2.3. Exclusion Criteria
2.4. Quality Assessment of Included Studies
2.5. Data Collection Process and Data Extraction
2.6. Compliance with Ethics Guidelines
3. Results
3.1. Study Characteristics
3.2. Assessment Tools—Observed Correlations
3.3. Influence of Age/Gender
3.4. Prognosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Bratman, S. The health food eating disorder. Yoga J. 1997, 42, 50. [Google Scholar]
- Koven, N.S.; Senbonmatsu, R. A neuropsychological evaluation of orthorexia nervosa. Open J. Psychiatry 2013, 3, 214–222. [Google Scholar] [CrossRef] [Green Version]
- Łucka, I.; Domarecki, P.; Janikowska-Hołoweńko, D.; Plenikowska-Ślusarz, T.; Domarecka, M. The prevalence and risk factors of orthorexia nervosa among school-age youth of Pomeranian and Warmian-Masurian voivodeships. Psychiatr. Pol. 2019, 53, 383–398. [Google Scholar] [CrossRef] [PubMed]
- Donini, L.M.; Marsili, D.; Graziani, M.P.; Imbriale, M.; Cannella, C. Orthorexia nervosa: Validation of a diagnosis questionnaire. Eat. Weight Disord.-Stud. Anorex. Bulim. Obes. 2005, 10, 28–32. [Google Scholar] [CrossRef]
- Bağci Bosi, A.T.; Camur, D.; Güler, C.B. Prevalence of orthorexia nervosa in resident medical doctors in the faculty of medicine (Ankara, Turkey). Appetite 2007, 49, 661–666. [Google Scholar] [CrossRef]
- Mathieu, J. What is orthorexia? J. Am. Diet. Assoc. 2005, 105, 1510–1512. [Google Scholar] [CrossRef]
- American Psychiatric Association. DSM-IV-TR: Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, TX, USA, 2013. [Google Scholar]
- Ramacciotti, C.E.; Perrone, P.; Coli, E.; Burgalassi, A.; Conversano, C.; Massimetti, G.; Dell’Osso, L. Orthorexia nervosa in the general population: A preliminary screening using a self-administered questionnaire (ORTO-15). Eat. Weight Disord. 2011, 16, e127–e130. [Google Scholar] [CrossRef]
- Brytek-Matera, A. Orthorexia nervosa—An eating disorder, obsessive-compulsive disorder or disturbed eating habit? Arch. Psychiatry Psychother. 2012, 1, 55–60. [Google Scholar]
- Segura-Garcia, C.; Ramacciotti, C.; Rania, M.; Aloi, M.; Caroleo, M.; Bruni, A.; De Fazio, P. The prevalence of orthorexia nervosa among eating disorder patients after treatment. Eat. Weight Disord.-Stud. Anorex. Bulim. Obes. 2015, 20, 161–166. [Google Scholar] [CrossRef]
- Heaner, M.K.; Walsh, B.T. A history of the identification of the characteristic eating disturbances of bulimia nervosa, binge eating disorder and anorexia nervosa. Appetite 2013, 65, 185–188. [Google Scholar] [CrossRef]
- Koven, N.S.; Abry, A.W. The clinical basis of orthorexia nervosa: Emerging perspectives. Neuropsychiatr. Dis. Treat. 2015, 11, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Modesti, P.A.; Reboldi, G.; Cappuccio, F.P. Panethnic Differences in Blood Pressure in Europe: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 25, e0147601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Agopyan, A.; Kenger, E.B.; Kermen, S.; Ulker, M.T.; Uzsoy, M.A.; Yetgin, M.K. The relationship between orthorexia nervosa and body composition in female students of the nutrition and dietetics department. Eat. Weight Disord.-Stud. Anorex. Bulim. Obes. 2019, 24, 257–266. [Google Scholar] [CrossRef]
- Arslantaş, H.; Adana, F.; Öğüt, S.; Ayakdaş, D.; Korkmaz, A. Relationship between eating behaviors of nursing students and orthorexia nervosa (obsession with healthy eating): A cross-sectional study. J. Psychiatr. Nurs. 2017, 8, 137–144. [Google Scholar]
- Haddad, C.; Obeid, S.; Akel, M.; Honein, K.; Akiki, M.; Azar, J.; Hallit, S. Correlates of orthorexia nervosa among a representative sample of the Lebanese population. Eat. Weight Disord.-Stud. Anorex. Bulim. Obes. 2019, 24, 481–493. [Google Scholar] [CrossRef]
- Shah, S.M. Orthorexia Nervosa: Healthy Eating or Eating Disorder? Master’s Thesis, Eastern Illinois University, Charleston, IL, USA, 2012. [Google Scholar]
- Okumuşoğlu, S. The relationship of orthorexic tendencies with eating disorder tendencies and gender in a group of university students. Curr. Res. Educ. 2017, 3, 105–115. [Google Scholar]
- McInerney-Ernst, E.M. Orthorexia Nervosa: Real Construct or Newest Social Trend? University of Missouri: Kansas City, MO, USA, 2011. [Google Scholar]
- Bóna, E.; Szél, Z.; Kiss, D.; Gyarmathy, V.A. An unhealthy health behavior: Analysis of orthorexic tendencies among Hungarian gym attendees. Eat. Weight Disord.-Stud. Anorex. Bulim. Obes. 2019, 24, 13–20. [Google Scholar] [CrossRef]
- Parra-Fernández, M.L.; Rodríguez-Cano, T.; Onieva-Zafra, M.D.; Perez-Haro, M.J.; Casero-Alonso, V.; Fernández-Martinez, E.; Notario-Pacheco, B. Prevalence of orthorexia nervosa in university students and its relationship with psychopathological aspects of eating behaviour disorders. BMC Psychiatry 2018, 18, 364. [Google Scholar] [CrossRef]
- Łucka, I.; Janikowska-Hołoweńko, D.; Domarecki, P.; Plenikowska-Ślusarz, T.; Domarecka, M. Orthorexia nervosa—A separate clinical entity, a part of eating disorder spectrum or another manifestation of obsessive-compulsive disorder? Psychiatr. Pol. 2019, 53, 371–382. [Google Scholar] [CrossRef]
- Plichta, M.; Jezewska-Zychowicz, M. Orthorexic tendency and eating disorders symptoms in Polish students: Examining differences in eating behaviors. Nutrients 2020, 12, 218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Segura-García, C.; Papaianni, M.C.; Caglioti, F.; Procopio, L.; Nisticò, C.G.; Bombardiere, L.; Capranica, L. Orthorexia nervosa: A frequent eating disordered behavior in athletes. Eat. Weight Disord.-Stud. Anorex. Bulim. Obes. 2012, 17, e226–e233. [Google Scholar]
- Brytek-Matera, A.; Fonte, M.L.; Poggiogalle, E.; Donini, L.M.; Cena, H. Orthorexia nervosa: Relationship with obsessive-compulsive symptoms, disordered eating patterns and body uneasiness among Italian university students. Eat. Weight Disord.-Stud. Anorex. Bulim. Obes. 2017, 22, 609–617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fidan, T.; Ertekin, V.; Işikay, S.; Kırpınar, I. Prevalence of orthorexia among medical students in Erzurum, Turkey. Compr. Psychiatry 2010, 51, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Barthels, F.; Meyer, F.; Huber, T.; Pietrowsky, R. Orthorexic eating behaviour as a coping strategy in patients with anorexia nervosa. Eat. Weight Disord.-Stud. Anorex. Bulim. Obes. 2017, 22, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Brytek-Matera, A.; Staniszewska, A.; Hallit, S. Identifying the profile of orthorexic behavior and “normal” eating behavior with cluster analysis: A cross-sectional study among polish adults. Nutrients 2020, 12, 3490. [Google Scholar] [CrossRef]
- Bundros, J.; Clifford, D.; Silliman, K.; Morris, M.N. Prevalence of Orthorexia nervosa among college students based on Bratman’s test and associated tendencies. Appetite 2016, 101, 86–94. [Google Scholar] [CrossRef]
- Dunn, T.M.; Hawkins, N.; Gagliano, S.; Stoddard, K. Individuals who self-identify as having “orthorexia nervosa” score in the clinical range on the Eating Attitudes Test-26. Eat. Weight Disord.-Stud. Anorex. Bulim. Obes. 2019, 24, 1025–1030. [Google Scholar] [CrossRef]
- Farchakh, Y.; Hallit, S.; Soufia, M. Association between orthorexia nervosa, eating attitudes and anxiety among medical students in Lebanese universities: Results of a cross-sectional study. Eat. Weight Disord.-Stud. Anorex. Bulim. Obes. 2019, 24, 683–691. [Google Scholar] [CrossRef]
- Hayes, O.; Wu, M.S.; De Nadai, A.S.; Storch, E.A. Orthorexia nervosa: An examination of the prevalence, correlates, and associated impairment in a university sample. J. Cogn. Psychother. 2017, 31, 124–135. [Google Scholar] [CrossRef]
- White, M.; Berry, R.; Rodgers, R.F. Body image and body change behaviors associated with orthorexia symptoms in males. Body Image 2020, 34, 46–50. [Google Scholar] [CrossRef]
- Asil, E.; Sürücüoğlu, M.S. Orthorexia nervosa in Turkish dietitians. Ecol. Food Nutr. 2015, 54, 303–313. [Google Scholar] [CrossRef] [PubMed]
- Barnes, M.A.; Caltabiano, M.L. The interrelationship between orthorexia nervosa, perfectionism, body image and attachment style. Eat. Weight Disord.-Stud. Anorex. Bulim. Obes. 2017, 22, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Brytek-Matera, A.; Onieva-Zafra, M.D.; Parra-Fernández, M.L.; Staniszewska, A.; Modrzejewska, J.; Fernández-Martínez, E. Evaluation of orthorexia nervosa and symptomatology associated with eating disorders among European University students: A multicentre cross-sectional study. Nutrients 2020, 12, 3716. [Google Scholar] [CrossRef] [PubMed]
- Gramaglia, C.; Gambaro, E.; Delicato, C.; Marchetti, M.; Sarchiapone, M.; Ferrante, D.; Zeppegno, P. Orthorexia nervosa, eating patterns and personality traits: A cross-cultural comparison of Italian, Polish and Spanish university students. BMC Psychiatry 2019, 19, 235. [Google Scholar] [CrossRef] [Green Version]
- Kyle, A. Orthorexia Nervosa in Undergraduate Health Majors: Using Yoga as an Intervention; Northern Illinois University: DeKalb, IL, USA, 2018. [Google Scholar]
- Obeid, S.; Hallit, S.; Akel, M.; Brytek-Matera, A. Orthorexia nervosa and its association with alexithymia, emotion dysregulation and disordered eating attitudes among Lebanese adults. Eat. Weight Disord.-Stud. Anorex. Bulim. Obes. 2021, 26, 2607–2616. [Google Scholar] [CrossRef]
- Parra-Fernández, M.L.; Onieva-Zafra, M.D.; Fernández-Martínez, E.; Abreu-Sánchez, A.; Fernández-Muñoz, J.J. Assessing the prevalence of orthorexia nervosa in a sample of university students using two different self-report measures. Int. J. Environ. Res. Public Health 2019, 16, 2459. [Google Scholar] [CrossRef] [Green Version]
- Strahler, J.; Hermann, A.; Walter, B.; Stark, R. Orthorexia nervosa: A behavioral complex or a psychological condition? J. Behav. Addict. 2018, 7, 1143–1156. [Google Scholar] [CrossRef]
- Zickgraf, H.F.; Ellis, J.M.; Essayli, J.H. Disentangling orthorexia nervosa from healthy eating and other eating disorder symptoms: Relationships with clinical impairment, comorbidity, and self-reported food choices. Appetite 2019, 134, 40–49. [Google Scholar] [CrossRef]
- Brytek-Matera, A.; Rogoza, R.; Gramaglia, C.; Zeppegno, P. Predictors of orthorexic behaviours in patients with eating disorders: A preliminary study. BMC Psychiatry 2015, 15, 252. [Google Scholar] [CrossRef] [Green Version]
- Gramaglia, C.; Brytek-Matera, A.; Rogoza, R.; Zeppegno, P. Orthorexia and anorexia nervosa: Two distinct phenomena? A cross-cultural comparison of orthorexic behaviours in clinical and non-clinical samples. BMC Psychiatry 2017, 17, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiss-Leizer, M.; Rigó, A. People behind unhealthy obsession to healthy food: The personality profile of tendency to orthorexia nervosa. Eat. Weight Disord.-Stud. Anorex. Bulim. Obes. 2019, 24, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Sanlier, N.; Yassibas, E.; Bilici, S.; Sahin, G.; Celik, B. Does the rise in eating disorders lead to increasing risk of orthorexia nervosa? Correlations with gender, education, and body mass index. Ecol. Food Nutr. 2016, 55, 266–278. [Google Scholar] [CrossRef] [PubMed]
- Yakın, E.; Raynal, P.; Chabrol, H. Distinguishing orthorexic behaviors from eating disordered and obsessive–compulsive behaviors: A typological study. Eat. Weight Disord.-Stud. Anorex. Bulim. Obes. 2020, 26, 2011–2019. [Google Scholar] [CrossRef]
- Ambwani, S.; Shippe, M.; Gao, Z.; Austin, S.B. Is# cleaneating a healthy or harmful dietary strategy? Perceptions of clean eating and associations with disordered eating among young adults. J. Eat. Disord. 2019, 7, 17. [Google Scholar]
- Dell’Osso, L.; Carpita, B.; Muti, D. Prevalence and characteristics of orthorexia nervosa in a sample of university students in Italy. Eat. Weight Disord. 2018, 23, 55–65. [Google Scholar] [CrossRef]
- Steinglass, J.E.; Walsh, B.; Stern, Y. Set shifting deficit in anorexia nervosa. J. Int. Neuropsychol. Soc. 2006, 12, 43. [Google Scholar] [CrossRef]
- Duran, S. The risk of orthorexia nervosa (healthy eating obsession) symptoms for health high school students and affecting factors. Pamukkale Med. J. 2016, 9, 220–226. [Google Scholar] [CrossRef] [Green Version]
- Alvarenga, M.S.; Martins, M.C.; Sato, K.S.; Vargas, S.V. Orthorexia nervosa behavior in a sample of Brazilian dietitians assessed by the Portuguese version of ORTO-15. Eat. Weight Disord. 2012, 17, 29–35. [Google Scholar] [CrossRef]
- Aksoydan, E.; Camci, N. Prevalence of orthorexia nervosa among Turkish performance artists. Eat. Weight Disord. 2009, 14, 33–37. [Google Scholar] [CrossRef]
- Ergin, G. Investigation of Orthorexia Nervosa Frequency in Individuals with and without Health Care Personnel. Master Thesis, Baskent University Health Sciences Institute, Department of Nutrition and Dietetics, Ankara, Turkey, 2014. [Google Scholar]
- Korinth, A.; Schiess, S.; Westenhoefer, J. Eating behaviour and eating disorders in students of nutrition sciences. Public Health Nutr. 2010, 13, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunn, T.M.; Bratman, S. On orthorexia nervosa: A review of the literature and proposed diagnostic criteria. Eat. Behav. 2015, 21, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Bratman, S.; Knight, D. Health Food Junkies: Overcoming the Obsession with Healthful Eating; Broadway Books: New York, NY, USA, 2000. [Google Scholar]
- Bianciardi, E. Body image dissatisfaction in individuals with obesity seeking bariatric surgery: Exploring the burden of new mediating factors. Riv. Psichiatr. 2019, 54, 8–17. [Google Scholar] [PubMed]
- Stewart, C.S.; Baudinet, J.; Munuve, A.; Bell, A.; Konstantellou, A.; Eisler, I.; Simic, M. From efficacy to effectiveness: Child and adolescent eating disorder treatments in the real world (Part 2): 7-year follow-up. J. Eat. Disord. 2022, 10, 14. [Google Scholar] [CrossRef] [PubMed]
- Lombardo, M.; Bellia, A.; Mattiuzzo, F. Frequent follow-up visits reduce weight regain in long-term management after bariatric surgery. Bariatr. Surg. Pract. Patient Care 2015, 10, 119–125. [Google Scholar] [CrossRef]


{kind=link}
| Author (Year) | Region, Country | Study Period | Study Design | Sample Size | Percentage of Males | Mean Age (SD) | Age Range | Study Population | Associations Studied in Relation to Orthorexia | Definition of Orthorexia | Definition of Eating Disorders | Main Findings of the Study | Potential Cofounding Factors Assessed | Nos Quality Rating |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Studies exclusively on adolescents and young adults | ||||||||||||||
| Agopyan 2018 [16] | Turkey (Istanbul) | March to May 2017 | Cross-sectional | 136 | 0 | 20.9 ± 2.0 years | N/R | College students | Eating disorder | ORTHO-11 > 27 | EAT-40 > 30 | A significant negative correlation (p < 0.05) was observed between the EAT-40 and ORTO-11 scores. | None | 5/10 |
| Arslantas 2017 [17] | Turkey (Izmir) | May 2018 | Cross-sectional | 181 | 22 | N/R | N/R | College students | Eating disorder | ORTHO-11 * | EAT-40 > 30 | A low negative correlation was identified between EAT-40 and ORTHO-11 (r = −0.162; p = 0.027). 84.5% were at risk according to EAT40, and 45.3% were at risk of ON | None | 5/10 |
| Brytek-Matera 2017 [27] | Italy | N/R | Cross-sectional | 120 | 30.8% | 22.74 ± 7.31 years | 19 to 30 | College students | Eating disorders | ORTHO-15 < 35 | The Eating Attitudes Test-26 (EAT-26) * | In female students a statistically significant positive, but weak, correlation was found between ORTO-15 and body image discomfort (r = 0.39 and r = 0.32; p = 0.001 and p = 0.003) Concerning, male students as the scores decreased on the ORTO-15 (more pathologica), the EAT-26 scores were linked to healthier eating attitudes. No significant differences were observed between females and males | Νone | 5/10 |
| Bundros 2016 [31] | USA | Academic year of 2014 to 2015 | Cross-sectional | 448 | 27 | 22.17 ± 4.83 | N/R | College students | Eating disorders | Bratman Orthorexia Test (BOT) * | Eating Attitude Test-26 (EAT-26) * | Significant positive correlations were discovered between total BOT and EAT-26 scores (r = 0.47, p < 0.01). Higher orthorexic tendencies were associated with higher eating disorder risk | None | 5/10 |
| Dunn 2019 [32] | USA | Ν/R | Cross-sectional | 354 | 10 | 21.6 years (SD 12.9) | N/R | College students and clinical cases | Eating disorder | ORTHO-15 * | Eating Attitude Test (EAT-26) * | The mean EAT-26 score for those indicated to have ON was in the range for having possibly an eating disorder. | None | 6/10 |
| Farchakh 2019 [33] | Lebanon | Between May 2018 and January 2019 | Cross-sectional | 627 | 50 | 21.81 ± 2.00 | N/R | Medical students | Eating disorder | ORTHO-15 * | The Eating Attitude (Test-26) * | Higher EAT score (β = −0.094) was significantly associated with lower ORTO-15 scores | BMI, age, gender | 7/10 |
| Fidan 2010 [28] | Turkey | January 2008 | Cross-sectional | 878 | 53 | 21.3 ± 2.1 years | 16 to 29 | Medical students | Eating disorders | ORTHO-11 * | Eating Attitude Test-40 > 30 | Male students presented a statistically significantly higher tendency for orthorexia (p = 0.001). A statistically significant difference for tendency for orthorexia was also observed between the different age groups (p = 0.025). In logistic regression analysis, age, sex, Eating Attitude Test-40 (EAT-40), and height affected the ORTO-11 scores. The difference between mean ORTO-11 scores of the groups with EAT-40 scores of 30 or lower was statistically significant (p = 0.028) | None | 5/10 |
| Hayles 2017 [34] | USA | Ν/R | Cross-sectional | 404 | 17 | 20.71 (SD 5 4.36) | N/R | Undergraduate students | disordered eating | Bratman Orthorexia Self-Test *, ORTHO-15 * | Eating Disorder Examination Questionnaire * | Orthorexia symptoms presented small to medium correlations with disordered eating symptoms. Orthorexia nervosa symptoms demonstrated an inverse and statistically significant relationship with the total EDEQ score. | None | 6/10 |
| Koven 2013 [2] | USA | N/R | Cross-sectional | 100 | 21 | 19.3 (1.2) | 18 to 22 | College students | Neurophysiological functioning | ORTHO-15 * | Eating Disorder Inventory (EDI-2) * | Body Dissatisfaction and perfectionism symptoms, as features of AN augmented as ORTO-15 score was reduced, meaning that orthorexia severity was higher | Age, education, and estimated intellectual functioning | 7/10 |
| Lucka 2019 [24] | Poland | N/R | Cross-sectional | 864 | 30 | 13–30 (males) 18–29 (females) | 13–29 (women) 13–30 (men) | Secondary and tertiary students | Eating disorders | ORTO-15 < 40 | EAT-26 * | The highest risk of orthorexia was found in junior secondary school students, aged between 13 and 16 years old The lowest risk was observed in senior secondary school (16 to 19-years old) Individuals at risk of orthorexia scored higher in the EAT-26, (EAT-26 total score z = 9.90; p < 0.001) (EAT bulimia: r = 0.259 p < 0.001) | None | 5/10 |
| White 2020 [35] | United States | N/R | Cross-sectional | 103 | 100% | 19.84, SD = 1.71 | 18–25 | Undergraduate students | Eating disorder pathology | ORTO-7 * | The Eating Disorder Diagnostic Scale (EDDS) * | Orthorexia symptoms presented a positive association with other dimensions of eating pathology (r = 0.535, p < 0.001) | None | 6/10 |
| Studies on adolescents and young adults, with admixture with older individuals | ||||||||||||||
| Asil 2015 [36] | Turkey (Ankara) | December 2012– March 2013 | Cross-sectional | 117 | 14 | 34 ± 11.2 years | N/R | Dieticians | Eating disorder | ORTHO-15 * | EAT-40 > 30 | The participants who had ORTO-15 scores less than 40 points presented significantly higher scores for EAT-40 (p < 0.05). A significant negative correlation was observed between the ORTO-15 and EAT-40 score | None | 5/10 |
| Barnes 2016 [37] | Australia | 2017 | Cross-sectional | 220 | 21 | 23.81 (8.40) | 18 to 62 | college students | History of eating disorder and personality traits | ORTHO-15 < 36 | Eating disorder (anorexia of bulimia neurosa) was self-reported | The most significant predictor of orthorexia nervosa was the presence of an eating disorder history. A significant difference was found on the ORTO-15 score between those having a positive history of eating disorder (M = 17.94, SD = 1.01) and those who did not (M = 23.37, SD = 4.20), t (159) = −5.15, p0.001. | None | 5/10 |
| Bona 2019 [22] | Hungary | March 2017–October 2017 | Cross-sectional | 207 | 32 | 31.9 (8.7) | 18 to 59 | Gym attendees | Eating disorder | Orto-11-Hu * | Eating Disorder Test (EAT-40) * | (Drive for thinness and interpersonal distrust was the two characteristics that presented significant associations with higher orthorexic tendencies. A relation to age was indicated: younger participants were more likely to have orthorexic habits. | Eating Disorder Inventory, health and exercise habits, and demographics | 8/10 |
| Brytek-Matera 2020 [38] | Spain and Poland. | N/R | Cross-sectional | 860 | 34.9% | 21.17 ± 3.38 | 18–35 | University students | ED symptoms | Düsseldorf Orthorexia Scale (DOS) * | Eating Disorder Inventory (EDI) * | DOS scores and bulimia were significantly correlated (r = 0.170; p < 0.01) | None | 5/10 |
| Gramaglia 2016 [39] | Italy, Poland and Spain | 1 January 2016 to 31 December 2017 | Cross-sectional | 664 | 28.00% | 24.02 years | 17–54 | University students | Eating patterns | ORTO-15 < 35 was used for Italy and Spain, and the cutoff of 24 for Poland | Eating Attitudes Test-26 (EAT-26) * | More than a third of the sample presented ON, F | Gender | 6/10 |
| Haddad 2019 [18] | Lebanon | Between January and May 2018 | Cross-sectional | 811 | 34 | 27.59 ± 11.76 | N/R | Lebanese governorates | Eating habits | ORTHO-15 < 40 | Eating Disorder Inventory (EDI-2), Eating attitudes test (EAT-26) > 21 | Increased EAT scores (Beta = −0.087) were related to lower ORTHO-15 scores, meaning higher level of orthorexia tendencies and behaviors | Sociodemographic Factors | 8/10 |
| Kyle 2018 [40] | USA | N/R | Cross-sectional | 124 | 12.10% | 21.3 ± 3.1 w | 18 to 34 | College students and yoga attendants | Eating patterns | ORTO-15 < 40 | Obsessive–Compulsive Inventory (OCI-R) > 21 | No significant relationship was found between a history of an eating disorder and ON [X 2 (1, N = 124) = 0.481, p = 0.488)] or possible eating disorder [X 2 (1, N = 124) = 0.393, p = 0.531 | Gender, age | 7/10 |
| Łucka [3] | Gdansk and Gdynia | N/A | Cross-sectional | 864 | N/A | 20.21 +/− 3.27 females, 18.93 +/− 3.67 males | 13–30 | Students | Eating attitude | ORTO-15 < 35 | EAT-26 > 20 | 27% of subjects were reported to have a great risk of ON. This risk was significantly higher in individuals with ED, both women (χ2 = 58.300; p < 0.001) and men (χ2 = 6.376; p = 0.012) | None | 5/10 |
| Mahesh Shah 2012 [19] | USA | Spring of 2010 | Cross-sectional | 172 | 41 | 19.83 (SD = 2.73 range: 18–39) | 18 to 39 | College students | Eating disorders | ORTHO-15 < 40 | EAT-26 > 20 | A significant negative correlation was identified between disordered eating behaviors and ON (r = −0.33, p < 0.01) | None | 6/10 |
| McInerney-Ernst 2011 [21] | USA | 2010 | Cross-sectional | 163 | 42 | (M = 19.94, SD = 3.01) | 18 to 40 | College students | Eating disorder | ORTHO-15 < 40 | Eating Disorder Examination Questionnaire (EDE-Q) * | Self-reported disordered eating patterns significantly predicted ON symptoms. Fewer ON symptoms were related to higher level of disordered eating pattern. Regression analysis results were statistically significant, F (1, 159) = 11.32, p = 0.001. Disordered eating patterns (EDE-Q; β = −0.26) was the only significant predictor of the ORTO-15 component measuring eating concern and worry. | None | 5/10 |
| Obeid 2021 [41] | Lebanon | October 2020 | Cross-sectional | 787 | 22.30% | 23.87 ± 8.75 | >18 | Community dwelling participants | Eating disorders | ORTO R * | Eating Attitude Test (EAT 26) > 20 | More ON tendencies and behaviors were associated with, higher EAT scores (β = 0.15) | Difficulties in emotion regulation, alexithymia, (DERS score) | 9/10 |
| Okumuşoğlu 2017 [20] | Turkey | Ν/R | Cross-sectional | 100 | 43 | 22.35, SD: 2.194 | 18 to 60 | College students | Eating disorders | ORTHO-11 * | Eating attitude test-40 (YTT-40) > 30 and REZZY eating disorders scale (REZZY) > 2 | ED tendencies which were measured by REZZY scores presented a negative correlation with ORTO-11 scale (r = −0.328, p = 0.01) but not with YTT-40 scores | None | 5/10 |
| Parra-Fernández 2018 [23] | Spain | N/R | Cross-sectional | 454 | 35 | 21.74 ± 4.73 years (18–51) | 18 to 41 | College students | Eating disorders | ORTO-11-ES < 25 | Eating Disorder Inventory-2 questionnaire (EDI-2) * | High values of the ED subscales corresponded to low values for the ON scores. The highest (negative) correlation coefficient (−0.564, p < 0.01) was observed between drive for thinness and the ON score. Significant were the scores on the EDI-2 for the group at risk of ON regarding their drive for thinness (17.1% vs. 2.1%), bulimia (2.6% vs. 0%) and body dissatisfaction (26.3% vs. 12.4%) | None | 6/10 |
| Parra-Fernández 2019 [42] | Spain | 2017/2018 | Cross-sectional | 492 | 43.1% | 19.97 years (SD = 3.03) | 18 to 44 | College students | Compare the prevalence of ON | Düsseldorfer Orthorexie Skala (DOS-ES) > 30 ORTO-11-ES < 25 | The Eating Disorder Inventory-EDI-2-Spanish Version * | ORTHO and bulimia were significantly correlated (t (1, 489) = 4.19, p < 0.01). | None | 6/10 |
| Plichta 2017 [25] | Poland | 2017 | Cross-sectional | 1120 | 29.6% | N/R | 18–35 | students | The dietary patterns (DPs) of people showing ON tendency, ED symptoms, and both ON tendency and ED symptoms | ORTO-15 < 35 | Eating Disorder Screen for Primary Care (ESP) * | Both ON tendency and ED symptoms were reported in 13% of the sample. The use of a special diet in both past and present might lead to an increased risk of ON tendency and ED symptoms. | None | 5/10 |
| Segura-García 2012 [26] | Italy | From May 2009 to April 2010 | Cross-sectional | 577 athletes and 250 controls | 67 | 23.2 ± 5.5 (males), 21.3 ± 7.0 (females) | 16 to 45 | Athletes of judged sports, team sports and fitness activities and controls from college students | Eating disorder | ORTHO-15 < 35 | Eating Attitude Test 26 (EAT-26) > 20, and Yale-Brown-Corner Eating Disorder Scale (YBC-EDS) > 8. | Age, diet in the past positivity to YBC-EDS or to EAT-26, competition level, and number of YBC-EDS preoccupations/ rituals were considered to be independent predictors of ON | Age, gender, BMI, activity level, professional competitive level, previous dieting, actual dieting, EAT-26 positivity, YBC-EDS positivity, BUT positivity, YBC-EDS symptoms | 7/10 |
| Strahler 2018 [43] | Germany | February to April 2017 | Cross-sectional | 713 | 22 | 28.9 ± 10.6, 29.4 ± 11.2 years (range: 18–75 years, median: 25 years) = women | Women, 18–75 | Population survey | eating disorder | Duesseldorf Orthorexia Scale (DOS) > 30 | Eating Disorder Examination—Questionnaire (EDE-Q8) > 2.5 | The pathological eating explained the highest percentage of variation in ON (R2 = 0.380). In order to discriminate ON from other mental health symptoms, a substantial co-occurrence with pathological eating with about 78% of ON subjects was suggested showing above-threshold symptoms of an eating disorder. Addictive behaviors were not related to ON. | None | 5/10 |
| Zickgraf 2019 [44] | USA | N/R | Cross-sectional | 449 | 51 | 33.6 (9.5) | 20 to 69 | Internet population | Eating disorders | Eating habits questionnaire (EHQ) * | Clinical impairment assessment—Eating only (CIA-E) *, Eating attitudes test-Severe restricting for thinness/bingeing and purging (EAT-26-SRT/BP) * | ON symptoms were related more to AN/BN than to ARFID. Clinical impairment from eating was not related to overall ON symptomatology | Gender, BMI and weight | 7/10 |
| Studies on Prognosis/features of Eating Disorders | ||||||||||||||
| Barthels 2016 [29] | N/R | N/R | Cross-sectional | 72 | 0 | M = 21.17, SD = 6.88 years (anorexia patients) | N/R | 42 female patients diagnosed with anorexia nervosa and 30 female participants for control group | Analyze orthorexic eating behavior in anorexic individuals | Düsseldorf Orthorexie Skala (DOS) > 30 | Female patients diagnosed with anorexia nervosa | No significant differences were observed between the AN group, the ANO and the control group. Patients with pronounced orthorexic eating behavior tend to eat more often healthy food, regardless of calorie content | None | 5/10 |
| Brytek-Matera 2015 [45] | Poland | From May 2014 to November 2014 | Cross-sectional | 52 female patients | 0 | 22.81 years (SD = 3.80) | N/R | Outpatients at the Polish National Center for Eating Disorders. | Eating disorders | ORTHO-15 < 24 | The Eating Attitudes Test-26 (EAT-26) > 20 | ON was negatively predicted by eating pathology, weight concern, health orientation, and appearance orientation. Orthorexic behaviors were not found to be significant with pathways between other variables. Orthorexic behaviors were more frequent in the group with lower level of eating pathology and less common in the group reporting higher levels of eating pathology. | None | 5/10 |
| Brytek-Matera 2020 [30] | Poland | N/R | Cross-sectional | 230 | 23.9% | 26.52 ± 7.65 | 18–60 | Participants from universities, companies and health centers | Pathological eating behaviors | The Düsseldorf Orthorexia Scale (DOS) > 30 | The Three-Factor Eating Questionnaire (TFEQ-R18) *, The Eating Disorder Inventory (EDI) * | In the whole sample of adults, 3.0% presented traits of ON, 5.7% were at risk of ON, and 91.3% presented no risk of developing ON. A higher percentage of ON was observed in patients with high inappropriate eating behaviors, high psychological, and affective ED traits and moderate OCD features. Higher DOS scores presented significant associations with higher cognitive restraint, uncontrolled and emotional eating, drive for thinness and bulimia. | None | 6/10 |
| Gramaglia 2017 [46] | N/R | N/R | Cross-sectional | 97 | N/R | N/R | > 18 years | Patients with a diagnosis of AN | Orthorexic behaviors between clinical and non-clinical groups | ORTO-15 < 40 | AN diagnosis | No difference was recorded (Chi-square test) in the percentage of subjects scoring under the ORTO-15 cutoff between Italian AN and Italian HC (p = 0.263), and between Polish AN and Polish HC (p = 0.670). | None | 5/10 |
| Kiss Leizer 2018 [47] | N/R | N/R | Cross-sectional | 739 | N/R | M = 29.67 SD = 10.18 | 18 to 72 | Social media respondents | Personality profile | Ortho-11 * | Temperament and Character Inventory-56 (TCI-56) * | There was a difference recorded between the ON groups in harm avoidance (F (2, 736) = 16.32, p < 0.001, η2 = 0.04). A significant difference was also reported between ON groups on self-directedness factor (F (2, 736) = 19.16, p < 0.001, η2 = 0.05). High harm avoidance and low self-directedness are relevant factors of AN and BN | None | 5/10 |
| Sanlier 2016 [48] | Turkey | April and May 2014 | Cross-sectional | 900 | 42 | 20.37 ± 1.74 | 17–23 | College students | Eating disorder | ORTHO-15 * | EAT-40 * | EAT-40 and ORTO-15 scores were significantly negatively correlated. Orthorectic participants among women were more than men (p < 0.001) | Gender | 6/10 |
| Segura-Garcia 2015 [11] | Italy | Ν/R | cross-sectional | 32 patients with eating disorders and matched controls | 0 | 22.2 ± 3.4 at the follow up | N/R | Eating disorders patients | eating disorders and OCD | ORTHO-15 < 35 | Yale-Brown-Cornell Eating Disorder Scale (YBC-EDS) > 30 and EAT-26 > 20 | ON highly prevalent symptoms among patients with AN and BN which tend to increase after treatment. | Age, gender, BMI | 7/10 |
| Yakın 2020 [49] | France | N/R | Cross-sectional | 921 | 15.3% | 20.72 (SD = 2.63) | 18 to 30 | Students | ED behaviors | Eating Habits Questionnaire (EHQ) * | Eating Disorders Inventory-3rd Edition (EDI-3) * | “Orthorexic behavior” and “Eating disordered behavior” clusters displayed greater appearance orientation and overweight preoccupation compared to the “Low” cluster, could be interpreted as an important resemblance between ON and ED. | None | 5/10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skella, P.; Chelmi, M.E.; Panagouli, E.; Garoufi, A.; Psaltopoulou, T.; Mastorakos, G.; Sergentanis, T.N.; Tsitsika, A. Orthorexia and Eating Disorders in Adolescents and Young Adults: A Systematic Review. Children 2022, 9, 514. https://doi.org/10.3390/children9040514
Skella P, Chelmi ME, Panagouli E, Garoufi A, Psaltopoulou T, Mastorakos G, Sergentanis TN, Tsitsika A. Orthorexia and Eating Disorders in Adolescents and Young Adults: A Systematic Review. Children. 2022; 9(4):514. https://doi.org/10.3390/children9040514
Chicago/Turabian StyleSkella, Panagiota, Maria Eleni Chelmi, Eleni Panagouli, Anastasia Garoufi, Theodora Psaltopoulou, George Mastorakos, Theodoros N. Sergentanis, and Artemis Tsitsika. 2022. "Orthorexia and Eating Disorders in Adolescents and Young Adults: A Systematic Review" Children 9, no. 4: 514. https://doi.org/10.3390/children9040514
APA StyleSkella, P., Chelmi, M. E., Panagouli, E., Garoufi, A., Psaltopoulou, T., Mastorakos, G., Sergentanis, T. N., & Tsitsika, A. (2022). Orthorexia and Eating Disorders in Adolescents and Young Adults: A Systematic Review. Children, 9(4), 514. https://doi.org/10.3390/children9040514