
Lung Ultrasound Patterns in Multisystem Inflammatory Syndrome in Children (MIS-C)-Characteristics and Prognostic Value

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
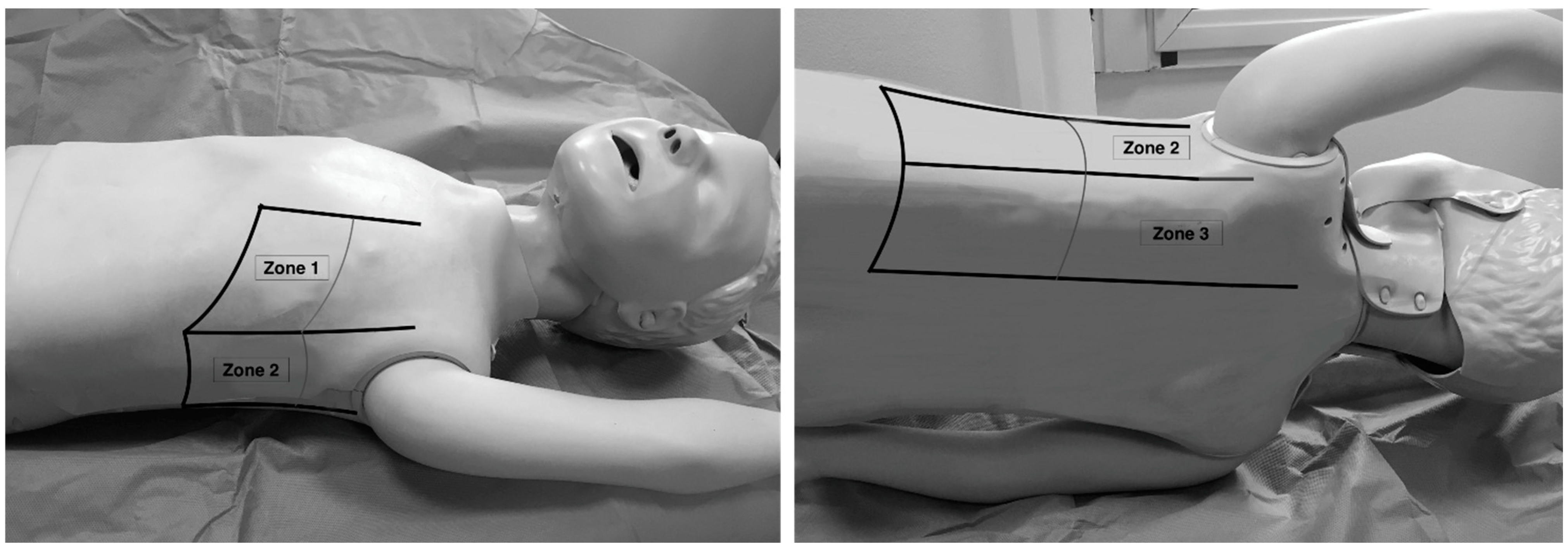
3. Lung and Cardiac Ultrasound Examination
- ▪
- A-lines: normal appearance of horizontal, equidistant, parallel artefacts originating at regular intervals from the pleural line (visceral and parietal pleura)
- ▪
- B-lines: laser-like signals arising from the hyper-echoic pleural line, extending to the bottom of the screen without fading and moving synchronously with respiration
- ▪
- Subpleural consolidation: Small, triangular, or oval shaped, echo-poor region adjacent to the pleura without a tissue-like pattern (AB)
- ▪
- Lobar consolidation: Large, hypoechogenic region adjacent to the pleura with a tissue-like pattern (AB) and an irregular pleural border
- ▪
- Pleural effusion: Anechoic or hypoechoic collection external to lung parenchyma, typically in a dependent lung region with or without respiratory movement of the lung within the effusion (flapping lung)
- (1)
- Normal lung sliding, regular pleural line, and A lines
- (2)
- Vertical artifacts, pleural line indented with several B-lines per field in the posterior regions
- (3)
- Vertical artifacts, pleural line indented with several B-lines per field in all regions
- (4)
- Broken pleural line with subpleural consolidations < 1 cm
- (5)
- Consolidations > 1 cm with or without pleural effusion (Table 1).
Statistical Analysis
4. Results
4.1. Demographic
4.2. Agreement with CXR
5. Discussion
6. Limitations and Strengths
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Kaushik, A.; Gupta, S.; Sood, M.; Sharma, S.; Verma, S. A Systematic Review of Multisystem Inflammatory Syndrome in Children Associated With SARS-CoV-2 Infection. Pediatr. Infect. Dis. J. 2020, 39, 340–346. [Google Scholar] [CrossRef]
- Feldstein, L.R.; Rose, E.B.; Horwitz, S.M. Multisystem Inflammatory Syndrome in U.S. Children and Adolescents. N. Engl. J. Med. 2020, 383, 334–346. [Google Scholar] [CrossRef]
- Radia, T.; Williams, N.; Agrawal, P.; Harman, K.; Weale, J.; Cook, J.; Gupta, A. Multi-system inflammatory syndrome in children & adolescents (MIS-C): A systematic review of clinical features and presentation. Paediatr. Respir. Rev. 2021, 38, 51–57. [Google Scholar] [CrossRef]
- Lichtenstein, D.A.; Mezière, G.A. Relevance of lung ultrasound in the diagnosis of acute respiratory failure: The BLUE protocol. Chest 2008, 134, 117–125. [Google Scholar] [CrossRef] [Green Version]
- Berant, R.; Kwan, C.; Fischer, J. Emergency Point-of-Care Ultrasound Assessment of Whiteout Lung in the Pediatric Emergency Department. Pediatr. Emerg. Care 2015, 31, 872–875. [Google Scholar] [CrossRef]
- Bobillo-Perez, S.; Girona-Alarcon, M.; Rodriguez-Fanjul, J.; Jordan, I.; Balaguer Gargallo, M. Lung ultrasound in children: What does it give us? Paediatr. Respir. Rev. 2020, 36, 136–141. [Google Scholar] [CrossRef]
- Buonsenso, D.; De Rose, C.; Ferro, V.; Morello, R.; Musolino, A.; Valentini, P. Lung Ultrasound to detect cardiopulmonary interactions in acutely ill children. Pediatr. Pulmonol. 2022, 57, 483–497. [Google Scholar] [CrossRef]
- Musolino, A.M.; Supino, M.C.; Buonsenso, D.; Ferro, V.; Valentini, P.; Magistrelli, A.; Lombardi, M.H.; Romani, L.; D’Argenio, P.; Campana, A.; et al. Lung Ultrasound in Children with COVID-19: Preliminary Findings. Ultrasound Med. Biol. 2020, 46, 2094–2098. [Google Scholar] [CrossRef]
- Nino, G.; Zember, J.; Sanchez-Jacob, R.; Gutierrez, M.J.; Sharma, K.; Linguraru, M.G. Pediatric lung imaging features of COVID-19: A systematic review and meta-analysis. Pediatr. Pulmonol. 2021, 56, 252–263. [Google Scholar] [CrossRef]
- Caro-Dominguez, P.; Shelmerdine, S.C.; Toso, S.; Secinaro, A.; Toma, P.; Damasio, M.B. Collaborators of the European Society of Paediatric Radiology Cardiothoracic Task Force. Thoracic imaging of coronavirus disease 2019 (COVID-19) in children: A series of 91 cases. Pediatr. Radiol. 2020, 50, 1354–1368. [Google Scholar] [CrossRef]
- Shelmerdine, S.C.; Lovrenski, J.; Caro-Domínguez, P.; Toso, S. Coronavirus disease 2019 (COVID-19) in children: A systematic review of imaging findings. Pediatr. Radiol. 2020, 50, 1217–1230. [Google Scholar] [CrossRef]
- Hameed, S.; Elbaaly, H.; Reid, C.E.L.; Santos, R.M.F.; Shivamurthy, V.; Wong, J.; Jogeesvaran, K.H. Spectrum of Imaging Findings at Chest Radiography, US, CT, and MRI in Multisystem Inflammatory Syndrome in Children Associated with COVID-19. Radiology 2021, 298, E1. [Google Scholar] [CrossRef]
- Lopez, L.; Colan, S.D.; Frommelt, P.C.; Ensing, G.J.; Kendall, K.; Younoszai, A.K.; Lai, W.W.; Geva, T. Recommendations for quantification methods during the performance of a pediatric echocardiogram: A report from the Pediatric Measurements Writing Group of the American Society of Echocardiography Pediatric and Congenital Heart Disease Council. J. Am. Soc. Echocardiogr. 2010, 23, 465–495, quiz 576–577. [Google Scholar] [CrossRef]
- Ciofi degli Atti, M.L.; Cuttini, M.; Ravà, L.; Rinaldi, S.; Brusco, C.; Cogo, P.; Pirozzi, N.; Picardo, S.; Schiavi, F.; Raponi, M. Performance of the pediatric index of mortality 2 (PIM-2) in cardiac and mixed intensive care units in a tertiary children’s referral hospital in Italy. BMC Pediatr. 2013, 13, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Volpicelli, G.; Elbarbary, M.; Blaivas, M.; Lichtenstein, D.A.; Mathis, G.; Kirkpatrick, A.W. International Liaison Committee on Lung Ultrasound (ILC-LUS) for International Consensus Conference on Lung Ultrasound (ICC-LUS). International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med. 2012, 38, 577–591. [Google Scholar] [CrossRef] [Green Version]
- Skopljanac, I.; Ivelja, M.P.; Barcot, O.; Brdar, I.; Dolic, K.; Polasek, O.; Radic, M. Role of Lung Ultrasound in Predicting Clinical Severity and Fatality in COVID-19 Pneumonia. J. Pers. Med. 2021, 11, 757. [Google Scholar] [CrossRef]
- Yin, W.; Li, Y.; Zeng, X.; Qin, Y.; Wang, D.; Zou, T.; Su, L.; Kang, Y. The utilization of critical care ultrasound to assess hemodynamics and lung pathology on ICU admission and the potential for predicting outcome. PLoS ONE 2017, 12, e0182881. [Google Scholar] [CrossRef] [Green Version]
- Picano, E.; Pellikka, P.A. Ultrasound of extravascular lung water: A new standard for pulmonary congestion. Eur. Heart J. 2016, 37, 2097–2104. [Google Scholar] [CrossRef] [Green Version]
- Al Deeb, M.; Barbic, S.; Featherstone, R.; Dankoff, J.; Barbic, D. Point-of-care ultrasonography for the diagnosis of acute cardiogenic pulmonary edema in patients presenting with acute dyspnea: A systematic review and meta-analysis. Acad. Emerg. Med. 2014, 21, 843–852. [Google Scholar] [CrossRef]
- Soldati, G.; Demi, M. The use of lung ultrasound images for the differential diagnosis of pulmonary and cardiac interstitial pathology. J. Ultrasound 2017, 20, 91–96. [Google Scholar] [CrossRef]
- Enghard, P.; Rademacher, S.; Nee, J.; Hasper, D.; Engert, U.; Jorres, A.; Kruse, J.M. Simplified lung ultrasound protocol shows excellent prediction of extravascular lung water in ventilated intensive care patients. Crit. Care 2015, 19, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Agricola, E.; Bove, T.; Oppizzi, M.; Marino, G.; Zangrillo, A.; Margonato, A.; Picano, E. “Ultrasound comet-tail images”: A marker of pulmonary edema: A comparative study with wedge pressure and extravascular lung water. Chest 2005, 127, 1690–1695. [Google Scholar] [CrossRef]
- Soldati, G.; Copetti, R.; Sher, S. Sonographic interstitial syndrome: The sound of lung water. J. Ultrasound Med. 2009, 28, 163–174. [Google Scholar] [CrossRef]
- Tripathi, S.; Ganatra, H.; Martinez, E.; Mannaa, M.; Peters, J. Accuracy and reliability of bedside thoracic ultrasound in detecting pulmonary pathology in a heterogeneous pediatric intensive care unit population. J. Clin. Ultrasound 2019, 47, 63–70. [Google Scholar] [CrossRef]
- Balk, D.S.; Lee, C.; Schafer, J.; Welwarth, J.; Hardin, J.; Novack, V. Lung ultrasound compared to chest X-ray for diagnosis of pediatric pneumonia: A meta-analysis. Pediatr. Pulmonol. 2018, 53, 1130–1139. [Google Scholar] [CrossRef]
- Buonsenso, D.; Musolino, A.; Ferro, V.; De Rose, C.; Morello, R.; Ventola, C. Role of lung ultrasound for the etiological diagnosis of acute lower respiratory tract infection (ALRTI) in children: A prospective study. J. Ultrasound 2022, 25, 185–197. [Google Scholar] [CrossRef]
- Copetti, R.; Cominotto, F.; Meduri, S.; Orso, D. The “Survived Lung:” An Ultrasound Sign of “Bubbly Consolidation” Pulmonary Infarction. Ultrasound Med. Biol. 2020, 46, 2546–2550. [Google Scholar] [CrossRef]
- Manolis, A.S.; Manolis, T.A.; Manolis, A.A.; Papatheou, D.; Melita, H. COVID-19 Infection: Viral Macro- and Micro-Vascular Coagulopathy and Thromboembolism/Prophylactic and Therapeutic Management. J. Cardiovasc. Pharm. Ther. 2021, 26, 12–24. [Google Scholar] [CrossRef]
- Lu, X.; Zhang, L.; Du, H.; Zhang, J.; Li, Y.Y.; Qu, J.; Zhang, W. Chinese Pediatric Novel Coronavirus Study Team. SARS-CoV-2 Infection in Children. N. Engl. J. Med. 2020, 382, 1663–1665. [Google Scholar] [CrossRef] [Green Version]
- Dong, Y.; Mo, X.; Hu, Y.; Qi, X.; Jiang, F.; Jiang, Z. Epidemiology of COVID-19 Among Children in China. Pediatrics 2020, 145, e20200702. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.; Yin, L.; Patel, J.; Tang, L.; Huang, Y. The inflammatory markers of multisystem inflammatory syndrome in children (MIS-C) and adolescents associated with COVID-19: A meta-analysis. J. Med. Virol. 2021, 93, 4358–4369. [Google Scholar] [CrossRef]
- Consiglio, C.R.; Cotugno, N.; Sardh, F.; Pou, C.; Amodio, D.; Rodriguez, L.; CACTUS Study Team; Landegren, N.; Palma, P.; Brodin, P. The Immunology of Multisystem Inflammatory Syndrome in Children with COVID-19. Cell 2020, 183, 968–981.e7. [Google Scholar] [CrossRef]
- Claes, A.S.; Clapuyt, P.; Menten, R.; Michoux, N.; Dumitriu, D. Performance of chest ultrasound in pediatric pneumonia. Eur. J. Radiol. 2017, 88, 82–87. [Google Scholar] [CrossRef] [Green Version]
- Guerra, M.; Crichiutti, G.; Pecile, P.; Romanello, C.; Busolini, E.; Valent, F. Ultrasound detection of pneumonia in febrile children with respiratory distress: A prospective study. Eur. J. Pediatr. 2016, 175, 163–170. [Google Scholar] [CrossRef]
- Demi, M.; Prediletto, R.; Soldati, G.; Demi, L. Physical Mechanisms Providing Clinical Information From Ultrasound Lung Images: Hypotheses and Early Confirmations. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2020, 67, 612–623. [Google Scholar] [CrossRef]
- Soldati, G.; Demi, M.; Inchingolo, R.; Smargiassi, A.; Demi, L. On the Physical Basis of Pulmonary Sonographic Interstitial Syndrome. J. Ultrasound Med. 2016, 35, 2075–2086. [Google Scholar] [CrossRef] [PubMed]
- Mento, F.; Soldati, G.; Prediletto, R.; Demi, M.; Demi, L. Quantitative Lung Ultrasound Spectroscopy Applied to the Diagnosis of Pulmonary Fibrosis: The First Clinical Study. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2020, 67, 2265–2273. [Google Scholar] [CrossRef]
- Mongodi, S.; Santangelo, E.; De Luca, D.; Rovida, S.; Corradi, F.; Volpicelli, G. Quantitative Lung Ultrasound: Time for a Consensus? Chest 2020, 158, 469–470. [Google Scholar] [CrossRef]
- Bagri, N.K.; Deepak, R.K.; Meena, S.; Gupta, S.K.; Prakash, S.; Setlur, K. Outcomes of multisystem inflammatory syndrome in children temporally related to COVID-19: A longitudinal study. Rheumatol. Int. 2022, 42, 477–484. [Google Scholar] [CrossRef]
- Földi, M.; Farkas, N.; Kiss, S.; Zádori, N.; Váncsa, S.; Szakó, L. KETLAK Study Group. Obesity is a risk factor for developing critical condition in COVID-19 patients: A systematic review and meta-analysis. Obes. Rev. 2020, 21, e13095. [Google Scholar] [CrossRef]
- Malik, P.; Patel, U.; Patel, K.; Martin, M.; Shah, C.; Mehta, D. Obesity a predictor of outcomes of COVID-19 hospitalized patients-A systematic review and meta-analysis. J. Med. Virol. 2021, 93, 1188–1193. [Google Scholar] [CrossRef]
- Reiff, D.D.; Mannion, M.L.; Samuy, N.; Scalici, P.; Cron, R.Q. Distinguishing active pediatric COVID-19 pneumonia from MIS-C. Pediatr. Rheumatol. Online J. 2021, 19, 21. [Google Scholar] [CrossRef]
- Buonsenso, D.; Mariani, F.; Pierri, L.; Morello, R.; Yock-Corrales, A.; Del Aguila, O. Association between Coagulation Profile and Clinical Outcome in Children with SARS-CoV-2 Infection or MIS-C: A Multicenter Cross-Sectional Study. Children 2022, 9, 279. [Google Scholar] [CrossRef]
- García-Salido, A.; de Carlos Vicente, J.C.; Belda Hofheinz, S.; Balcells Ramírez, J.; Slöcker Barrio, M.; Leóz Gordillo, I.; García-Salido, A.; de Carlos Vicente, J.C.; Belda Hofheinz, S.; Balcells Ramírez, J.; et al. Severe manifestations of SARS-CoV-2 in children and adolescents: From COVID-19 pneumonia to multisystem inflammatory syndrome: A multicentre study in pediatric intensive care units in Spain. Crit. Care 2020, 24, 1–13. [Google Scholar] [CrossRef]
- Al-Ghafry, M.; Vagrecha, A.; Malik, M.; Levine, C.; Uster, E.; Aygun, B. Multisystem inflammatory syndrome in children (MIS-C) and the prothrombotic state: Coagulation profiles and rotational thromboelastometry in a MIS-C cohort. J. Thromb. Haemost. 2021, 19, 1764–1770. [Google Scholar] [CrossRef]
- Caiulo, V.A.; Gargani, L.; Caiulo, S.; Fisicaro, A.; Moramarco, F.; Latini, G.; Picano, E. Lung ultrasound in bronchiolitis: Comparison with chest X-ray. Eur. J. Pediatr. 2011, 170, 1427–1433. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
 | PATTERN 1 Normal lung sliding, regular pleural line andA lines |
 | PATTERN 2 Vertical artifacts, pleural line indented with several B-lines per field in the posterior regions |
 | PATTERN 3 Vertical artifacts, pleural line indented with several B-lines per field in all regions |
 | PATTERN 4 Broken pleural line with subpleural consolidations <1 cm |
 | PATTERN 5 Consolidation >1 cm without pleural effusion |
 | PATTERN 5 Consolidation >1 cm with pleural effusion |
| All | LUS < 3 | LUS = 3 | LUS = 4 | LUS = 5 | |
|---|---|---|---|---|---|
| Sex, M | 71.1% | 66.7% | 83.3% | 71.1% | 83.3% |
| Age, years | 8.105 ± 4.865 [8(4–12)] | 7.571 ± 5.144 [8(3–12)] | 11.5 ± 4.764 [12.5(10.5–13.75)] | 8.105 ± 4.865 [8(4–12)] | 9.333 ± 4.179 [9.5(6.25–12.75)] |
| Comorbidities, N(%) | 12 (50%) | 6 (25%) | 1 (4%) | 4 (16%) | 2 (8%) |
| BMI, kg/m2 | 18.751 ± 3.546 [18.445(16.408–20.293)] | 17.47 ± 3.037 [16.55(16.315–18.175)] | 20.39 ± 5.216 [20.2(18.75–21.63)] | 18.751 ± 3.546 [18.445(16.408–20.293)] | 22.213 ± 5.078 [20.57(19.365–24.24)] |
| Fever before therapy, days | 5.5 ± 1.765 [5(5–6)] | 5.526 ± 2.195 [5(4–7)] | 5.333 ± 0.816 [5.5(5–6)] | 5.5 ± 1.765 [5(5–6)] | 5.833 ± 1.835 [5(5–6.5)] |
| Fever global duration, days | 7.028 ± 2.145 [7(5–9)] | 7.6 ± 2.326 [7(6.75–9)] | 6.5 ± 1.049 [6.5(6–7)] | 7.028 ± 2.145 [7(5–9)] | 7.2 ± 1.924 [7(6–8)] |
| PICU (yes) | 65.8% | 38.1% | 100% | 65.8% | 100% |
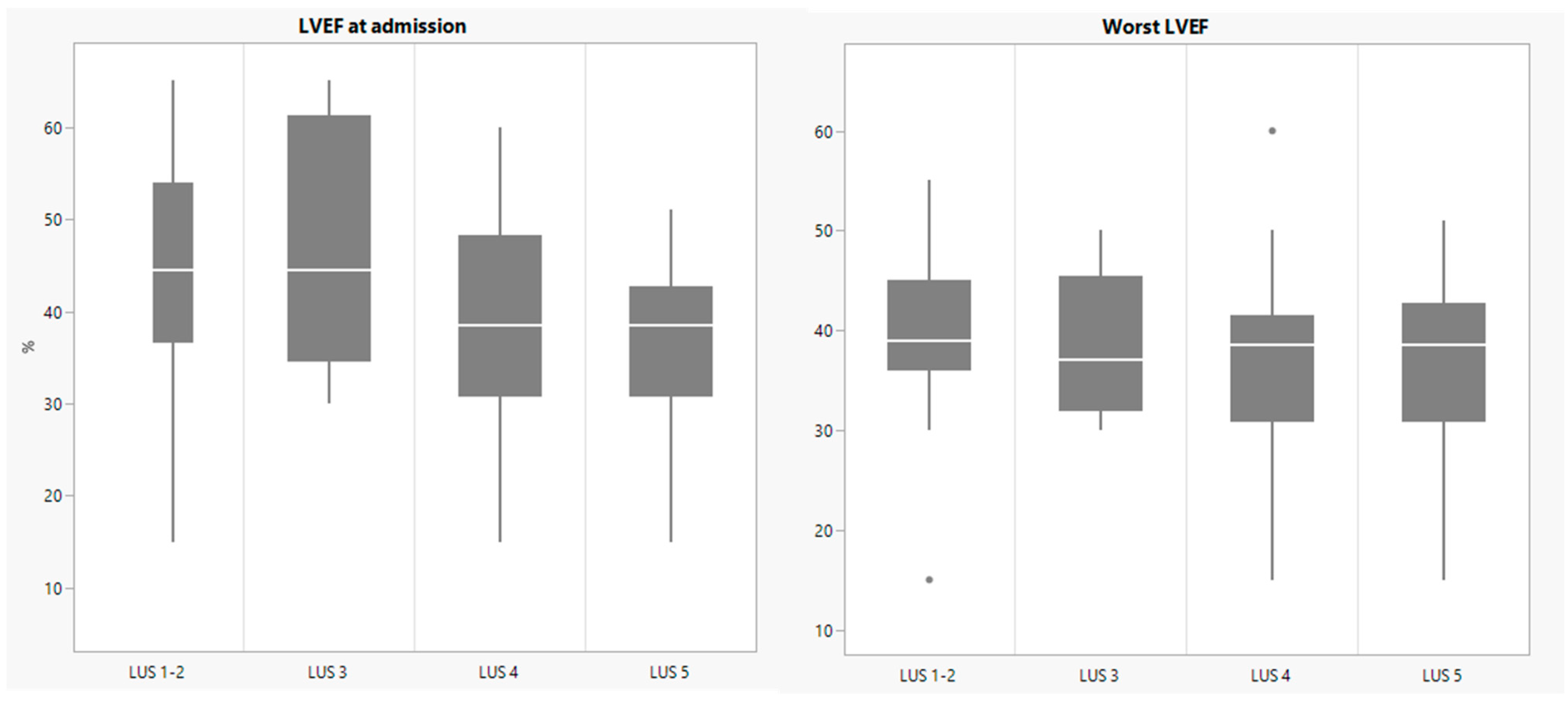
| LVEF at admission, % | 50.842 ± 13.219 [51.5(39.25–60)] | 57.286 ± 9.624 [60(52–62)] | 46.667 ± 14.137 [44.5(36.5–57.75)] | 50.842 ± 13.219 [51.5(39.25–60)] | 36.5 ± 11.777 [38.5(36.5–39.75)] |
| LVEF worst value, % | 46.843 ± 12.781 [49(38.5–55)] | 53.889 ± 10.922 [53.5(49–60)] | 38.417 ± 7.446 [37(33.375–42.5)] | 46.843 ± 12.781 [49(38.5–55)] | 36.5 ± 11.777 [38.5(36.5–39.75)] |
| Inotrope use | 41.9% | 14.3% | 50% | 41.9% | 66.7% |
| Ventilation (y) | 39.3% | 18.2% | 66.7% | 39.3% | 50% |
| Hospital stay, days | 12.081 ± 3.854 [12(10–14)] | 10.9 ± 3.905 [10(8.5–12.25)] | 14.167 ± 3.251 [14(12–16.75)] | 12.081 ± 3.854 [12(10–14)] | 13.5 ± 3.834 [13.5(11.25–16.5)] |
| PICU LOS, days | 2.789 ± 2.801 [2.5(0–4)] | 1.048 ± 1.564 [0(0–2)] | 4.333 ± 2.066 [4.5(2.5–5.75)] | 2.789 ± 2.801 [2.5(0–4)] | 4.5 ± 1.378 [4(4–4.75)] |
| Ventilation days | 2.6 ± 1.43 [2.5(1.25–3.75)] | 2 ± 1.414 [2(1.5–2.5)] | 3 ± 1.826 [3(1.75–4.25)] | 2.6 ± 1.43 [2.5(1.25–3.75)] | 2.667 ± 2.082 [2(1.5–3.5)] |
| LUS 1 | LUS 2 | LUS 3 | LUS 4 | LUS 5 | |
|---|---|---|---|---|---|
| CXR_consolidations | 0 | 6 | 6 | 8 | 4 |
| CXR_effusions | 0 | 5 | 2 | 4 | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Camporesi, A.; Gemma, M.; Buonsenso, D.; Ferrario, S.; Mandelli, A.; Pessina, M.; Diotto, V.; Rota, E.; Raso, I.; Fiori, L.; et al. Lung Ultrasound Patterns in Multisystem Inflammatory Syndrome in Children (MIS-C)-Characteristics and Prognostic Value. Children 2022, 9, 931. https://doi.org/10.3390/children9070931
Camporesi A, Gemma M, Buonsenso D, Ferrario S, Mandelli A, Pessina M, Diotto V, Rota E, Raso I, Fiori L, et al. Lung Ultrasound Patterns in Multisystem Inflammatory Syndrome in Children (MIS-C)-Characteristics and Prognostic Value. Children. 2022; 9(7):931. https://doi.org/10.3390/children9070931
Chicago/Turabian StyleCamporesi, Anna, Marco Gemma, Danilo Buonsenso, Stefania Ferrario, Anna Mandelli, Matteo Pessina, Veronica Diotto, Elena Rota, Irene Raso, Laura Fiori, and et al. 2022. "Lung Ultrasound Patterns in Multisystem Inflammatory Syndrome in Children (MIS-C)-Characteristics and Prognostic Value" Children 9, no. 7: 931. https://doi.org/10.3390/children9070931
APA StyleCamporesi, A., Gemma, M., Buonsenso, D., Ferrario, S., Mandelli, A., Pessina, M., Diotto, V., Rota, E., Raso, I., Fiori, L., Campari, A., & Izzo, F. (2022). Lung Ultrasound Patterns in Multisystem Inflammatory Syndrome in Children (MIS-C)-Characteristics and Prognostic Value. Children, 9(7), 931. https://doi.org/10.3390/children9070931