
Novel Lung Growth Strategy with Biological Therapy Targeting Airway Remodeling in Childhood Bronchial Asthma


Abstract
:1. Introduction
1.1. Childhood Asthma
1.2. Natural Prognosis of Lung Function in Childhood Asthma
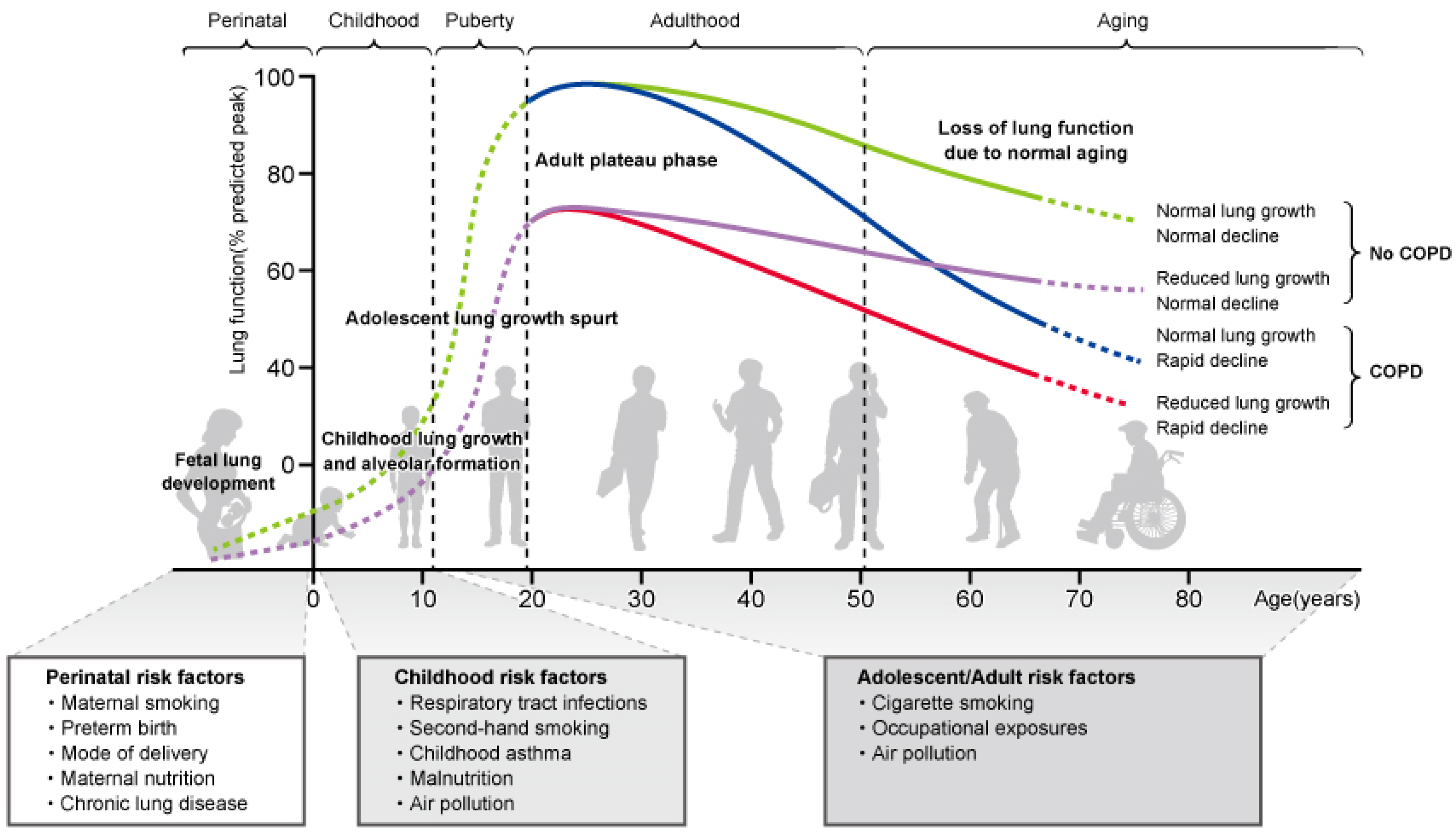
1.3. Decreased Respiratory Function in Childhood and Onset of COPD in Adulthood
1.4. Lung Development in Childhood
1.5. Impaired Lung Growth, and Increased Risk of Developing COPD, Due to Childhood Asthma
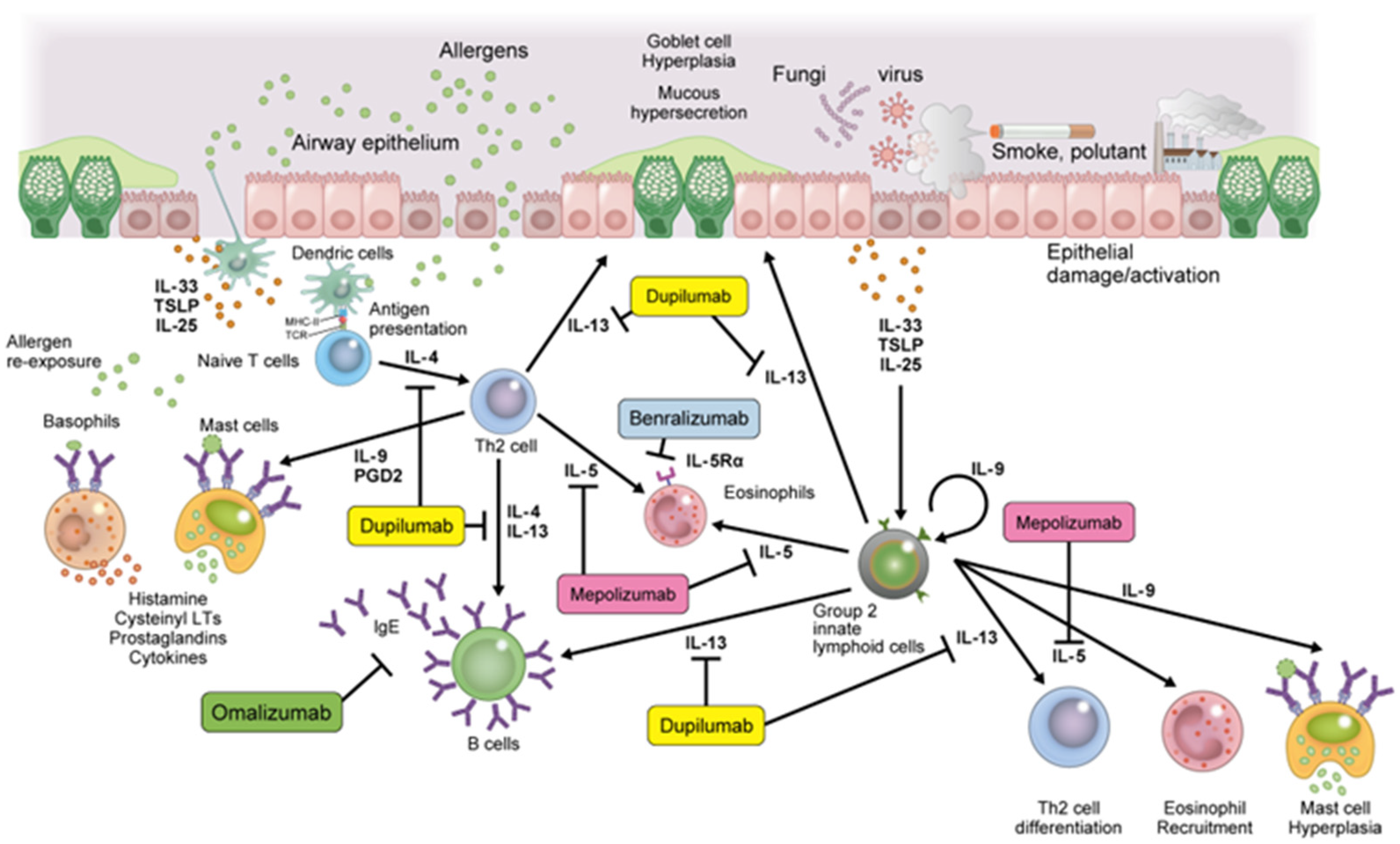
2. Airway Inflammation and Remodeling with T2-High Asthma in Children
2.1. T2-High Asthma in Childhood Asthma
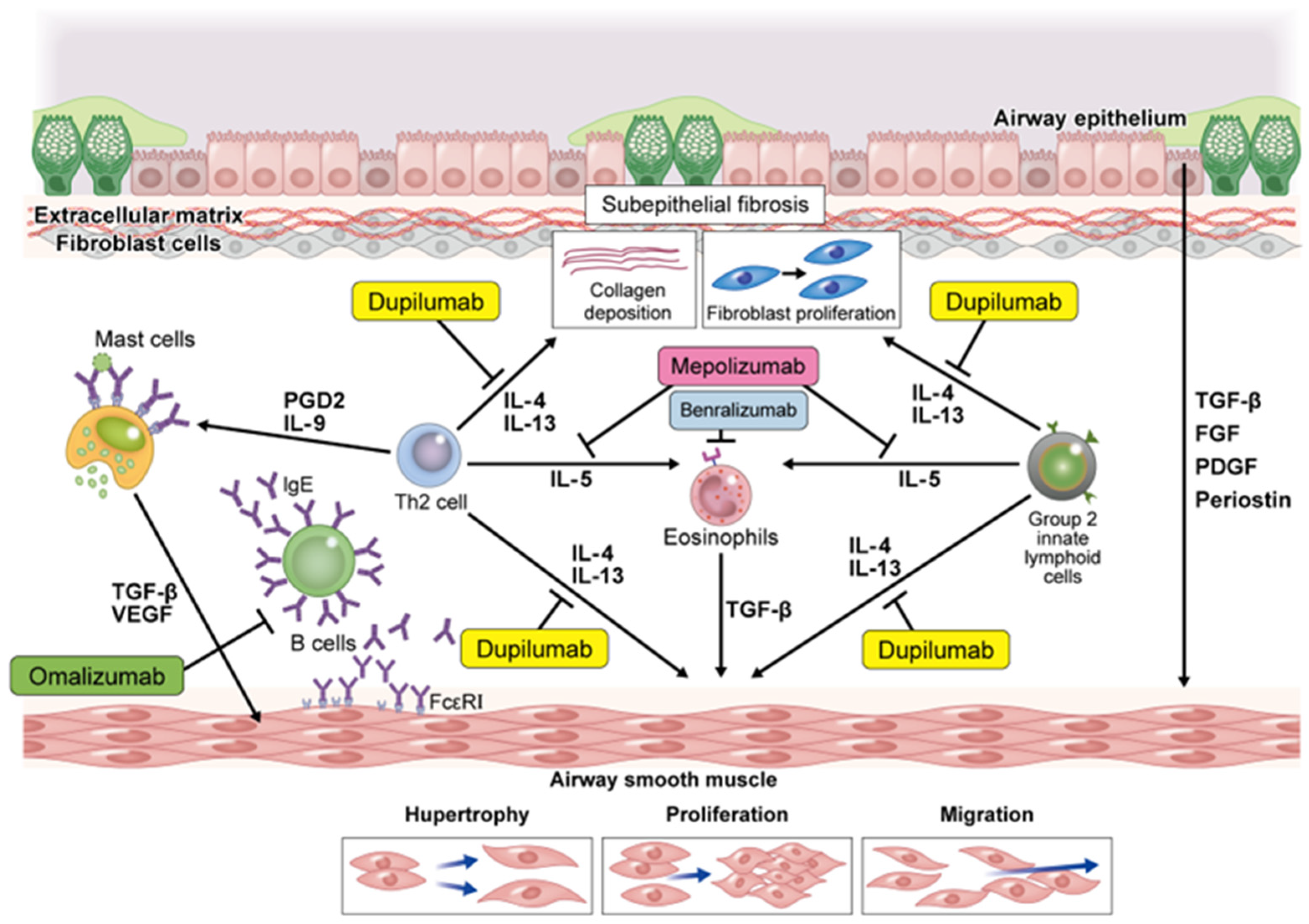
2.2. Th2 Cytokines and Airway Remodeling
3. Efficacy of Biological Drugs in Childhood Asthma and Effects on Airway Remodeling
3.1. Omalizumab
3.2. Mepolizumab
3.3. Benralizumab
3.4. Dupilumab
4. Inhibitory Effect of Airway Remodeling by Biological Drugs
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Papi, A.; Brightling, C.; Pedersen, S.E.; Reddel, H.K. Asthma. Lancet 2018, 391, 783–800. [Google Scholar] [CrossRef]
- Dharmage, S.C.; Perret, J.L.; Custovic, A. Epidemiology of Asthma in Children and Adults. Front. Pediatr. 2019, 7, 246. [Google Scholar] [CrossRef]
- Zahran, H.S.; Bailey, C.M.; Damon, S.A.; Garbe, P.L.; Breysse, P.N. Vital Signs: Asthma in Children—United States, 2001–2016. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 149–155. [Google Scholar] [CrossRef]
- Gibson, G.J.; Loddenkemper, R.; Lundbäck, B.; Sibille, Y. Respiratory health and disease in Europe: The new European Lung White Book. Eur. Respir. J. 2013, 42, 559–563. [Google Scholar] [CrossRef]
- Guilbert, T.W.; Bacharier, L.B.; Fitzpatrick, A.M. Severe asthma in children. J. Allergy Clin. Immunol. Pract. 2014, 2, 489–500. [Google Scholar] [CrossRef]
- Fleming, L.; Murray, C.; Bansal, A.T.; Hashimoto, S.; Bisgaard, H.; Bush, A.; Frey, U.; Hedlin, G.; Singer, F.; van Aalderen, W.M.; et al. The burden of severe asthma in childhood and adolescence: Results from the paediatric U-BIOPRED cohorts. Eur. Respir. J. 2015, 46, 1322–1333. [Google Scholar] [CrossRef]
- Pijnenburg, M.W.; Fleming, L. Advances in understanding and reducing the burden of severe asthma in children. Lancet Respir. Med. 2020, 8, 1032–1044. [Google Scholar] [CrossRef]
- Bui, D.S.; Lodge, C.J.; Burgess, J.A.; Lowe, A.J.; Perret, J.; Bui, M.Q.; Bowatte, G.; Gurrin, L.; Johns, D.P.; Thompson, B.R.; et al. Childhood predictors of lung function trajectories and future COPD risk: A prospective cohort study from the first to the sixth decade of life. Lancet Respir. Med. 2018, 6, 535–544. [Google Scholar] [CrossRef]
- Tsuge, M.; Ikeda, M.; Matsumoto, N.; Yorifuji, T.; Tsukahara, H. Current Insights into Atopic March. Children 2021, 8, 1067. [Google Scholar] [CrossRef]
- Tantisira, K.G.; Colvin, R.; Tonascia, J.; Strunk, R.C.; Weiss, S.T.; Fuhlbrigge, A.L. Airway responsiveness in mild to moderate childhood asthma: Sex influences on the natural history. Am. J. Respir. Crit. Care Med. 2008, 178, 325–331. [Google Scholar] [CrossRef]
- Vonk, J.M.; Postma, D.S.; Boezen, H.M.; Grol, M.H.; Schouten, J.P.; Koëter, G.H.; Gerritsen, J. Childhood factors associated with asthma remission after 30 year follow up. Thorax 2004, 59, 925–929. [Google Scholar] [CrossRef]
- Limb, S.L.; Brown, K.C.; Wood, R.A.; Wise, R.A.; Eggleston, P.A.; Tonascia, J.; Hamilton, R.G.; Adkinson, N.F., Jr. Adult asthma severity in individuals with a history of childhood asthma. J. Allergy Clin. Immunol. 2005, 115, 61–66. [Google Scholar] [CrossRef]
- Tai, A.; Tran, H.; Roberts, M.; Clarke, N.; Gibson, A.M.; Vidmar, S.; Wilson, J.; Robertson, C.F. Outcomes of childhood asthma to the age of 50 years. J. Allergy Clin. Immunol. 2014, 133, 1572–1578.e1573. [Google Scholar] [CrossRef]
- Belgrave, D.C.; Buchan, I.; Bishop, C.; Lowe, L.; Simpson, A.; Custovic, A. Trajectories of lung function during childhood. Am. J. Respir. Crit. Care Med. 2014, 189, 1101–1109. [Google Scholar] [CrossRef]
- Lodge, C.J.; Lowe, A.J.; Allen, K.J.; Zaloumis, S.; Gurrin, L.C.; Matheson, M.C.; Axelrad, C.; Welsh, L.; Bennett, C.M.; Hopper, J.; et al. Childhood wheeze phenotypes show less than expected growth in FEV1 across adolescence. Am. J. Respir. Crit. Care Med. 2014, 189, 1351–1358. [Google Scholar] [CrossRef]
- Hallberg, J.; Thunqvist, P.; Schultz, E.S.; Kull, I.; Bottai, M.; Merritt, A.S.; Chiesa, F.; Gustafsson, P.M.; Melén, E. Asthma phenotypes and lung function up to 16 years of age-the BAMSE cohort. Allergy 2015, 70, 667–673. [Google Scholar] [CrossRef]
- Sears, M.R.; Greene, J.M.; Willan, A.R.; Wiecek, E.M.; Taylor, D.R.; Flannery, E.M.; Cowan, J.O.; Herbison, G.P.; Silva, P.A.; Poulton, R. A longitudinal, population-based, cohort study of childhood asthma followed to adulthood. N. Engl. J. Med. 2003, 349, 1414–1422. [Google Scholar] [CrossRef]
- Covar, R.A.; Spahn, J.D.; Murphy, J.R.; Szefler, S.J. Progression of asthma measured by lung function in the childhood asthma management program. Am. J. Respir. Crit. Care Med. 2004, 170, 234–241. [Google Scholar] [CrossRef]
- Postma, D.S.; Bush, A.; van den Berge, M. Risk factors and early origins of chronic obstructive pulmonary disease. Lancet 2015, 385, 899–909. [Google Scholar] [CrossRef]
- Halpin, D.M.G.; Criner, G.J.; Papi, A.; Singh, D.; Anzueto, A.; Martinez, F.J.; Agusti, A.A.; Vogelmeier, C.F. Global Initiative for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease. The 2020 GOLD Science Committee Report on COVID-19 and Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2021, 203, 24–36. [Google Scholar] [CrossRef]
- Taniguchi, A.; Tsuge, M.; Miyahara, N.; Tsukahara, H. Reactive Oxygen Species and Antioxidative Defense in Chronic Obstructive Pulmonary Disease. Antioxidants 2021, 10, 1537. [Google Scholar] [CrossRef] [PubMed]
- Lamprecht, B.; McBurnie, M.A.; Vollmer, W.M.; Gudmundsson, G.; Welte, T.; Nizankowska-Mogilnicka, E.; Studnicka, M.; Bateman, E.; Anto, J.M.; Burney, P.; et al. COPD in never smokers: Results from the population-based burden of obstructive lung disease study. Chest 2011, 139, 752–763. [Google Scholar] [CrossRef] [PubMed]
- Salvi, S.S.; Barnes, P.J. Chronic obstructive pulmonary disease in non-smokers. Lancet 2009, 374, 733–743. [Google Scholar] [CrossRef]
- Lange, P.; Celli, B.; Agustí, A.; Boje Jensen, G.; Divo, M.; Faner, R.; Guerra, S.; Marott, J.L.; Martinez, F.D.; Martinez-Camblor, P.; et al. Lung-Function Trajectories Leading to Chronic Obstructive Pulmonary Disease. N. Engl. J. Med. 2015, 373, 111–122. [Google Scholar] [CrossRef]
- Vasquez, M.M.; Zhou, M.; Hu, C.; Martinez, F.D.; Guerra, S. Low Lung Function in Young Adult Life Is Associated with Early Mortality. Am. J. Respir. Crit. Care Med. 2017, 195, 1399–1401. [Google Scholar] [CrossRef] [PubMed]
- Bui, D.S.; Burgess, J.A.; Lowe, A.J.; Perret, J.L.; Lodge, C.J.; Bui, M.; Morrison, S.; Thompson, B.R.; Thomas, P.S.; Giles, G.G.; et al. Childhood Lung Function Predicts Adult Chronic Obstructive Pulmonary Disease and Asthma-Chronic Obstructive Pulmonary Disease Overlap Syndrome. Am. J. Respir. Crit. Care Med. 2017, 196, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Belgrave, D.C.M.; Granell, R.; Turner, S.W.; Curtin, J.A.; Buchan, I.E.; Le Souëf, P.N.; Simpson, A.; Henderson, A.J.; Custovic, A. Lung function trajectories from pre-school age to adulthood and their associations with early life factors: A retrospective analysis of three population-based birth cohort studies. Lancet Respir. Med. 2018, 6, 526–534. [Google Scholar] [CrossRef]
- Berry, C.E.; Billheimer, D.; Jenkins, I.C.; Lu, Z.J.; Stern, D.A.; Gerald, L.B.; Carr, T.F.; Guerra, S.; Morgan, W.J.; Wright, A.L.; et al. A Distinct Low Lung Function Trajectory from Childhood to the Fourth Decade of Life. Am. J. Respir. Crit. Care Med. 2016, 194, 607–612. [Google Scholar] [CrossRef]
- Johannessen, A.; Bakke, P.S.; Hardie, J.A.; Eagan, T.M. Association of exposure to environmental tobacco smoke in childhood with chronic obstructive pulmonary disease and respiratory symptoms in adults. Respirology 2012, 17, 499–505. [Google Scholar] [CrossRef]
- Tai, A.; Tran, H.; Roberts, M.; Clarke, N.; Wilson, J.; Robertson, C.F. The association between childhood asthma and adult chronic obstructive pulmonary disease. Thorax 2014, 69, 805–810. [Google Scholar] [CrossRef]
- Martinez, F.D. Early-Life Origins of Chronic Obstructive Pulmonary Disease. N. Engl. J. Med. 2016, 375, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Narayanan, M.; Owers-Bradley, J.; Beardsmore, C.S.; Mada, M.; Ball, I.; Garipov, R.; Panesar, K.S.; Kuehni, C.E.; Spycher, B.D.; Williams, S.E.; et al. Alveolarization continues during childhood and adolescence: New evidence from helium-3 magnetic resonance. Am. J. Respir. Crit. Care Med. 2012, 185, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Mullassery, D.; Smith, N.P. Lung development. Semin. Pediatr. Surg. 2015, 24, 152–155. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Mensinga, T.T.; Schouten, J.P.; Rijcken, B.; Weiss, S.T. Determinants of maximally attained level of pulmonary function. Am. J. Respir. Crit. Care Med. 2004, 169, 941–949. [Google Scholar] [CrossRef]
- Allinson, J.P.; Hardy, R.; Donaldson, G.C.; Shaheen, S.O.; Kuh, D.; Wedzicha, J.A. Combined Impact of Smoking and Early-Life Exposures on Adult Lung Function Trajectories. Am. J. Respir. Crit. Care Med. 2017, 196, 1021–1030. [Google Scholar] [CrossRef]
- Perret, J.L.; Walters, H.; Johns, D.; Gurrin, L.; Burgess, J.; Lowe, A.; Thompson, B.; Markos, J.; Morrison, S.; Thomas, P.; et al. Mother’s smoking and complex lung function of offspring in middle age: A cohort study from childhood. Respirology 2016, 21, 911–919. [Google Scholar] [CrossRef]
- Hayden, L.P.; Hobbs, B.D.; Cohen, R.T.; Wise, R.A.; Checkley, W.; Crapo, J.D.; Hersh, C.P. Childhood pneumonia increases risk for chronic obstructive pulmonary disease: The COPDGene study. Respir. Res. 2015, 16, 115. [Google Scholar] [CrossRef]
- Savran, O.; Ulrik, C.S. Early life insults as determinants of chronic obstructive pulmonary disease in adult life. Int. J. Chron. Obstruct. Pulmon. Dis. 2018, 13, 683–693. [Google Scholar] [CrossRef]
- Duan, P.; Wang, Y.; Lin, R.; Zeng, Y.; Chen, C.; Yang, L.; Yue, M.; Zhong, S.; Wang, Y.; Zhang, Q. Impact of early life exposures on COPD in adulthood: A systematic review and meta-analysis. Respirology 2021, 26, 1131–1151. [Google Scholar] [CrossRef]
- Tagiyeva, N.; Devereux, G.; Fielding, S.; Turner, S.; Douglas, G. Outcomes of Childhood Asthma and Wheezy Bronchitis. A 50-Year Cohort Study. Am. J. Respir. Crit. Care Med. 2016, 193, 23–30. [Google Scholar] [CrossRef]
- Ali, K.M. Childhood asthma as a risk factor for adult chronic obstructive pulmonary disease: A systematic review and meta-analysis. Expert Rev. Respir. Med. 2022, 16, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Shirtcliffe, P.; Marsh, S.; Travers, J.; Weatherall, M.; Beasley, R. Childhood asthma and GOLD-defined chronic obstructive pulmonary disease. Intern. Med. J. 2012, 42, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Agusti, A.; Faner, R. Lung function trajectories in health and disease. Lancet Respir. Med. 2019, 7, 358–364. [Google Scholar] [CrossRef]
- Bisgaard, H.; Nørgaard, S.; Sevelsted, A.; Chawes, B.L.; Stokholm, J.; Mortensen, E.L.; Ulrik, C.S.; Bønnelykke, K. Asthma-like symptoms in young children increase the risk of COPD. J. Allergy Clin. Immunol. 2021, 147, 569–576.e569. [Google Scholar] [CrossRef]
- McGeachie, M.J.; Yates, K.P.; Zhou, X.; Guo, F.; Sternberg, A.L.; Van Natta, M.L.; Wise, R.A.; Szefler, S.J.; Sharma, S.; Kho, A.T.; et al. Patterns of Growth and Decline in Lung Function in Persistent Childhood Asthma. N. Engl. J. Med. 2016, 374, 1842–1852. [Google Scholar] [CrossRef]
- Phelan, P.D.; Robertson, C.F.; Olinsky, A. The Melbourne Asthma Study: 1964–1999. J. Allergy Clin. Immunol. 2002, 109, 189–194. [Google Scholar] [CrossRef]
- James, A.L.; Palmer, L.J.; Kicic, E.; Maxwell, P.S.; Lagan, S.E.; Ryan, G.F.; Musk, A.W. Decline in lung function in the Busselton Health Study: The effects of asthma and cigarette smoking. Am. J. Respir. Crit. Care Med. 2005, 171, 109–114. [Google Scholar] [CrossRef]
- Stern, D.A.; Morgan, W.J.; Wright, A.L.; Guerra, S.; Martinez, F.D. Poor airway function in early infancy and lung function by age 22 years: A non-selective longitudinal cohort study. Lancet 2007, 370, 758–764. [Google Scholar] [CrossRef]
- Marossy, A.E.; Strachan, D.P.; Rudnicka, A.R.; Anderson, H.R. Childhood chest illness and the rate of decline of adult lung function between ages 35 and 45 years. Am. J. Respir. Crit. Care Med. 2007, 175, 355–359. [Google Scholar] [CrossRef]
- Marcon, A.; Locatelli, F.; Keidel, D.; Beckmeyer-Borowko, A.B.; Cerveri, I.; Dharmage, S.C.; Fuertes, E.; Garcia-Aymerich, J.; Heinrich, J.; Imboden, M.; et al. Airway responsiveness to methacholine and incidence of COPD: An international prospective cohort study. Thorax 2018, 73, 825–832. [Google Scholar] [CrossRef]
- Bui, D.S.; Walters, H.E.; Burgess, J.A.; Perret, J.L.; Bui, M.Q.; Bowatte, G.; Lowe, A.J.; Russell, M.A.; Thompson, B.R.; Hamilton, G.S.; et al. Childhood Respiratory Risk Factor Profiles and Middle-Age Lung Function: A Prospective Cohort Study from the First to Sixth Decade. Ann. Am. Thorac. Soc. 2018, 15, 1057–1066. [Google Scholar] [CrossRef] [PubMed]
- Licari, A.; Castagnoli, R.; Brambilla, I.; Marseglia, A.; Tosca, M.A.; Marseglia, G.L.; Ciprandi, G. Asthma Endotyping and Biomarkers in Childhood Asthma. Pediatr. Allergy Immunol. Pulmonol. 2018, 31, 44–55. [Google Scholar] [CrossRef] [PubMed]
- Diamant, Z.; Vijverberg, S.; Alving, K.; Bakirtas, A.; Bjermer, L.; Custovic, A.; Dahlen, S.E.; Gaga, M.; Gerth van Wijk, R.; Giacco, S.D.; et al. Toward clinically applicable biomarkers for asthma: An EAACI position paper. Allergy 2019, 74, 1835–1851. [Google Scholar] [CrossRef] [PubMed]
- Cevhertas, L.; Ogulur, I.; Maurer, D.J.; Burla, D.; Ding, M.; Jansen, K.; Koch, J.; Liu, C.; Ma, S.; Mitamura, Y.; et al. Advances and recent developments in asthma in 2020. Allergy 2020, 75, 3124–3146. [Google Scholar] [CrossRef]
- Pepper, A.N.; Renz, H.; Casale, T.B.; Garn, H. Biologic Therapy and Novel Molecular Targets of Severe Asthma. J. Allergy Clin. Immunol. Pract. 2017, 5, 909–916. [Google Scholar] [CrossRef]
- Stokes, J.R.; Casale, T.B. Characterization of asthma endotypes: Implications for therapy. Ann. Allergy Asthma Immunol. 2016, 117, 121–125. [Google Scholar] [CrossRef]
- Saglani, S.; Lloyd, C.M. Eosinophils in the pathogenesis of paediatric severe asthma. Curr. Opin. Allergy Clin. Immunol. 2014, 14, 143–148. [Google Scholar] [CrossRef]
- LaPorte, S.L.; Juo, Z.S.; Vaclavikova, J.; Colf, L.A.; Qi, X.; Heller, N.M.; Keegan, A.D.; Garcia, K.C. Molecular and structural basis of cytokine receptor pleiotropy in the interleukin-4/13 system. Cell 2008, 132, 259–272. [Google Scholar] [CrossRef]
- Kau, A.L.; Korenblat, P.E. Anti-interleukin 4 and 13 for asthma treatment in the era of endotypes. Curr. Opin. Allergy Clin. Immunol. 2014, 14, 570–575. [Google Scholar] [CrossRef]
- Saco, T.V.; Pepper, A.; Casale, T.B. Uses of biologics in allergic diseases: What to choose and when. Ann. Allergy Asthma Immunol. 2018, 120, 357–366. [Google Scholar] [CrossRef]
- Halwani, R.; Al-Muhsen, S.; Hamid, Q. Airway remodeling in asthma. Curr. Opin. Pharmacol. 2010, 10, 236–245. [Google Scholar] [CrossRef]
- Boulet, L.P. Airway remodeling in asthma: Update on mechanisms and therapeutic approaches. Curr. Opin. Pulm. Med. 2018, 24, 56–62. [Google Scholar] [CrossRef]
- Wilson, S.J.; Rigden, H.M.; Ward, J.A.; Laviolette, M.; Jarjour, N.N.; Djukanović, R. The relationship between eosinophilia and airway remodelling in mild asthma. Clin. Exp. Allergy 2013, 43, 1342–1350. [Google Scholar] [CrossRef]
- O’Reilly, R.; Ullmann, N.; Irving, S.; Bossley, C.J.; Sonnappa, S.; Zhu, J.; Oates, T.; Banya, W.; Jeffery, P.K.; Bush, A.; et al. Increased airway smooth muscle in preschool wheezers who have asthma at school age. J. Allergy Clin. Immunol. 2013, 131, 1024–1032, 1032.e1001-1016. [Google Scholar] [CrossRef]
- Lezmi, G.; Gosset, P.; Deschildre, A.; Abou-Taam, R.; Mahut, B.; Beydon, N.; de Blic, J. Airway Remodeling in Preschool Children with Severe Recurrent Wheeze. Am. J. Respir. Crit. Care Med. 2015, 192, 164–171. [Google Scholar] [CrossRef]
- Grainge, C.L.; Lau, L.C.; Ward, J.A.; Dulay, V.; Lahiff, G.; Wilson, S.; Holgate, S.; Davies, D.E.; Howarth, P.H. Effect of bronchoconstriction on airway remodeling in asthma. N. Engl. J. Med. 2011, 364, 2006–2015. [Google Scholar] [CrossRef]
- Holgate, S.T. Epithelium dysfunction in asthma. J. Allergy Clin. Immunol. 2007, 120, 1233–1244, quiz 1245-1236. [Google Scholar] [CrossRef]
- Doherty, T.; Broide, D. Cytokines and growth factors in airway remodeling in asthma. Curr. Opin. Immunol. 2007, 19, 676–680. [Google Scholar] [CrossRef]
- Batra, V.; Musani, A.I.; Hastie, A.T.; Khurana, S.; Carpenter, K.A.; Zangrilli, J.G.; Peters, S.P. Bronchoalveolar lavage fluid concentrations of transforming growth factor (TGF)-beta1, TGF-beta2, interleukin (IL)-4 and IL-13 after segmental allergen challenge and their effects on alpha-smooth muscle actin and collagen III synthesis by primary human lung fibroblasts. Clin. Exp. Allergy 2004, 34, 437–444. [Google Scholar] [CrossRef]
- Tanaka, H.; Komai, M.; Nagao, K.; Ishizaki, M.; Kajiwara, D.; Takatsu, K.; Delespesse, G.; Nagai, H. Role of interleukin-5 and eosinophils in allergen-induced airway remodeling in mice. Am. J. Respir. Cell Mol. Biol. 2004, 31, 62–68. [Google Scholar] [CrossRef]
- Malavia, N.K.; Mih, J.D.; Raub, C.B.; Dinh, B.T.; George, S.C. IL-13 induces a bronchial epithelial phenotype that is profibrotic. Respir. Res. 2008, 9, 27. [Google Scholar] [CrossRef]
- Redhu, N.S.; Shan, L.; Al-Subait, D.; Ashdown, H.L.; Movassagh, H.; Lamkhioued, B.; Gounni, A.S. IgE induces proliferation in human airway smooth muscle cells: Role of MAPK and STAT3 pathways. Allergy Asthma Clin. Immunol. 2013, 9, 41. [Google Scholar] [CrossRef]
- Cao, L.; Liu, F.; Liu, Y.; Liu, T.; Wu, J.; Zhao, J.; Wang, J.; Li, S.; Xu, J.; Dong, L. TSLP promotes asthmatic airway remodeling via p38-STAT3 signaling pathway in human lung fibroblast. Exp. Lung Res. 2018, 44, 288–301. [Google Scholar] [CrossRef]
- Halwani, R.; Al-Muhsen, S.; Al-Jahdali, H.; Hamid, Q. Role of transforming growth factor-β in airway remodeling in asthma. Am. J. Respir. Cell Mol. Biol. 2011, 44, 127–133. [Google Scholar] [CrossRef]
- Kardas, G.; Daszyńska-Kardas, A.; Marynowski, M.; Brząkalska, O.; Kuna, P.; Panek, M. Role of Platelet-Derived Growth Factor (PDGF) in Asthma as an Immunoregulatory Factor Mediating Airway Remodeling and Possible Pharmacological Target. Front. Pharmacol. 2020, 11, 47. [Google Scholar] [CrossRef]
- Johnson, P.R.; Burgess, J.K.; Underwood, P.A.; Au, W.; Poniris, M.H.; Tamm, M.; Ge, Q.; Roth, M.; Black, J.L. Extracellular matrix proteins modulate asthmatic airway smooth muscle cell proliferation via an autocrine mechanism. J. Allergy Clin. Immunol. 2004, 113, 690–696. [Google Scholar] [CrossRef]
- Tatler, A.L.; John, A.E.; Jolly, L.; Habgood, A.; Porte, J.; Brightling, C.; Knox, A.J.; Pang, L.; Sheppard, D.; Huang, X.; et al. Integrin αvβ5-mediated TGF-β activation by airway smooth muscle cells in asthma. J. Immunol. 2011, 187, 6094–6107. [Google Scholar] [CrossRef]
- Pain, M.; Bermudez, O.; Lacoste, P.; Royer, P.J.; Botturi, K.; Tissot, A.; Brouard, S.; Eickelberg, O.; Magnan, A. Tissue remodelling in chronic bronchial diseases: From the epithelial to mesenchymal phenotype. Eur. Respir. Rev. 2014, 23, 118–130. [Google Scholar] [CrossRef]
- Sohal, S.S.; Ward, C.; Walters, E.H. Importance of epithelial mesenchymal transition (EMT) in COPD and asthma. Thorax 2014, 69, 768. [Google Scholar] [CrossRef]
- Shkumatov, A.; Thompson, M.; Choi, K.M.; Sicard, D.; Baek, K.; Kim, D.H.; Tschumperlin, D.J.; Prakash, Y.S.; Kong, H. Matrix stiffness-modulated proliferation and secretory function of the airway smooth muscle cells. Am. J. Physiol. Lung Cell Mol. Physiol. 2015, 308, L1125–L1135. [Google Scholar] [CrossRef]
- Licari, A.; Manti, S.; Marseglia, A.; De Filippo, M.; De Sando, E.; Foiadelli, T.; Marseglia, G.L. Biologics in Children with Allergic Diseases. Curr. Pediatr. Rev. 2020, 16, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Abrams, E.M.; Becker, A.B.; Szefler, S.J. Current State and Future of Biologic Therapies in the Treatment of Asthma in Children. Pediatr. Allergy Immunol. Pulmonol. 2018, 31, 119–131. [Google Scholar] [CrossRef] [PubMed]
- Porcaro, F.; Cutrera, R.; Pajno, G.B. Options of immunotherapeutic treatments for children with asthma. Expert Rev. Respir. Med. 2019, 13, 937–949. [Google Scholar] [CrossRef] [PubMed]
- Kawakami, T.; Blank, U. From IgE to Omalizumab. J. Immunol 2016, 197, 4187–4192. [Google Scholar] [CrossRef]
- Walsh, G.M. An update on biologic-based therapy in asthma. Immunotherapy 2013, 5, 1255–1264. [Google Scholar] [CrossRef]
- Licari, A.; Castagnoli, R.; Panfili, E.; Marseglia, A.; Brambilla, I.; Marseglia, G.L. An Update on Anti-IgE Therapy in Pediatric Respiratory Diseases. Curr. Respir. Med. Rev. 2017, 13, 22–29. [Google Scholar] [CrossRef]
- Berger, W.; Gupta, N.; McAlary, M.; Fowler-Taylor, A. Evaluation of long-term safety of the anti-IgE antibody, omalizumab, in children with allergic asthma. Ann. Allergy Asthma Immunol. 2003, 91, 182–188. [Google Scholar] [CrossRef]
- Chipps, B.E.; Lanier, B.; Milgrom, H.; Deschildre, A.; Hedlin, G.; Szefler, S.J.; Kattan, M.; Kianifard, F.; Ortiz, B.; Haselkorn, T.; et al. Omalizumab in children with uncontrolled allergic asthma: Review of clinical trial and real-world experience. J. Allergy Clin. Immunol. 2017, 139, 1431–1444. [Google Scholar] [CrossRef]
- Brodlie, M.; McKean, M.C.; Moss, S.; Spencer, D.A. The oral corticosteroid-sparing effect of omalizumab in children with severe asthma. Arch. Dis. Child. 2012, 97, 604–609. [Google Scholar] [CrossRef]
- Deschildre, A.; Marguet, C.; Salleron, J.; Pin, I.; Rittié, J.L.; Derelle, J.; Taam, R.A.; Fayon, M.; Brouard, J.; Dubus, J.C.; et al. Add-on omalizumab in children with severe allergic asthma: A 1-year real life survey. Eur. Respir. J. 2013, 42, 1224–1233. [Google Scholar] [CrossRef]
- Busse, W.W.; Humbert, M.; Haselkorn, T.; Ortiz, B.; Trzaskoma, B.L.; Stephenson, P.; Garcia Conde, L.; Kianifard, F.; Holgate, S.T. Effect of omalizumab on lung function and eosinophil levels in adolescents with moderate-to-severe allergic asthma. Ann. Allergy Asthma Immunol. 2020, 124, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Busse, W.W.; Morgan, W.J.; Gergen, P.J.; Mitchell, H.E.; Gern, J.E.; Liu, A.H.; Gruchalla, R.S.; Kattan, M.; Teach, S.J.; Pongracic, J.A.; et al. Randomized trial of omalizumab (anti-IgE) for asthma in inner-city children. N. Engl. J. Med. 2011, 364, 1005–1015. [Google Scholar] [CrossRef] [PubMed]
- Teach, S.J.; Gill, M.A.; Togias, A.; Sorkness, C.A.; Arbes, S.J., Jr.; Calatroni, A.; Wildfire, J.J.; Gergen, P.J.; Cohen, R.T.; Pongracic, J.A.; et al. Preseasonal treatment with either omalizumab or an inhaled corticosteroid boost to prevent fall asthma exacerbations. J. Allergy Clin. Immunol. 2015, 136, 1476–1485. [Google Scholar] [CrossRef] [PubMed]
- Esquivel, A.; Busse, W.W.; Calatroni, A.; Togias, A.G.; Grindle, K.G.; Bochkov, Y.A.; Gruchalla, R.S.; Kattan, M.; Kercsmar, C.M.; Khurana Hershey, G.; et al. Effects of Omalizumab on Rhinovirus Infections, Illnesses, and Exacerbations of Asthma. Am. J. Respir. Crit. Care Med. 2017, 196, 985–992. [Google Scholar] [CrossRef]
- Emma, R.; Morjaria, J.B.; Fuochi, V.; Polosa, R.; Caruso, M. Mepolizumab in the management of severe eosinophilic asthma in adults: Current evidence and practical experience. Ther. Adv. Respir. Dis. 2018, 12, 1753466618808490. [Google Scholar] [CrossRef]
- Licari, A.; Manti, S.; Castagnoli, R.; Parisi, G.F.; Salpietro, C.; Leonardi, S.; Marseglia, G.L. Targeted Therapy for Severe Asthma in Children and Adolescents: Current and Future Perspectives. Paediatr. Drugs 2019, 21, 215–237. [Google Scholar] [CrossRef]
- Pavord, I.D.; Korn, S.; Howarth, P.; Bleecker, E.R.; Buhl, R.; Keene, O.N.; Ortega, H.; Chanez, P. Mepolizumab for severe eosinophilic asthma (DREAM): A multicentre, double-blind, placebo-controlled trial. Lancet 2012, 380, 651–659. [Google Scholar] [CrossRef]
- Ortega, H.G.; Liu, M.C.; Pavord, I.D.; Brusselle, G.G.; FitzGerald, J.M.; Chetta, A.; Humbert, M.; Katz, L.E.; Keene, O.N.; Yancey, S.W.; et al. Mepolizumab treatment in patients with severe eosinophilic asthma. N. Engl. J. Med. 2014, 371, 1198–1207. [Google Scholar] [CrossRef]
- Lugogo, N.; Domingo, C.; Chanez, P.; Leigh, R.; Gilson, M.J.; Price, R.G.; Yancey, S.W.; Ortega, H.G. Long-term Efficacy and Safety of Mepolizumab in Patients With Severe Eosinophilic Asthma: A Multi-center, Open-label, Phase IIIb Study. Clin. Ther. 2016, 38, 2058–2070.e1. [Google Scholar] [CrossRef]
- Khatri, S.; Moore, W.; Gibson, P.G.; Leigh, R.; Bourdin, A.; Maspero, J.; Barros, M.; Buhl, R.; Howarth, P.; Albers, F.C.; et al. Assessment of the long-term safety of mepolizumab and durability of clinical response in patients with severe eosinophilic asthma. J. Allergy Clin. Immunol. 2019, 143, 1742–1751.e1747. [Google Scholar] [CrossRef]
- Gupta, A.; Ikeda, M.; Geng, B.; Azmi, J.; Price, R.G.; Bradford, E.S.; Yancey, S.W.; Steinfeld, J. Long-term safety and pharmacodynamics of mepolizumab in children with severe asthma with an eosinophilic phenotype. J. Allergy Clin. Immunol. 2019, 144, 1336–1342.e1337. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Pouliquen, I.; Austin, D.; Price, R.G.; Kempsford, R.; Steinfeld, J.; Bradford, E.S.; Yancey, S.W. Subcutaneous mepolizumab in children aged 6 to 11 years with severe eosinophilic asthma. Pediatr. Pulmonol. 2019, 54, 1957–1967. [Google Scholar] [CrossRef] [PubMed]
- Harrison, T.; Canonica, G.W.; Chupp, G.; Lee, J.; Schleich, F.; Welte, T.; Valero, A.; Gemzoe, K.; Maxwell, A.; Joksaite, S.; et al. Real-world mepolizumab in the prospective severe asthma REALITI-A study: Initial analysis. Eur. Respir. J. 2020, 56. [Google Scholar] [CrossRef] [PubMed]
- Sposato, B.; Camiciottoli, G.; Bacci, E.; Scalese, M.; Carpagnano, G.E.; Pelaia, C.; Santus, P.; Maniscalco, M.; Masieri, S.; Corsico, A.; et al. Mepolizumab effectiveness on small airway obstruction, corticosteroid sparing and maintenance therapy step-down in real life. Pulm. Pharmacol. Ther. 2020, 61, 101899. [Google Scholar] [CrossRef] [PubMed]
- Kolbeck, R.; Kozhich, A.; Koike, M.; Peng, L.; Andersson, C.K.; Damschroder, M.M.; Reed, J.L.; Woods, R.; Dall’acqua, W.W.; Stephens, G.L.; et al. MEDI-563, a humanized anti-IL-5 receptor alpha mAb with enhanced antibody-dependent cell-mediated cytotoxicity function. J. Allergy Clin. Immunol. 2010, 125, 1344–1353.e1342. [Google Scholar] [CrossRef]
- Bleecker, E.R.; FitzGerald, J.M.; Chanez, P.; Papi, A.; Weinstein, S.F.; Barker, P.; Sproule, S.; Gilmartin, G.; Aurivillius, M.; Werkström, V.; et al. Efficacy and safety of benralizumab for patients with severe asthma uncontrolled with high-dosage inhaled corticosteroids and long-acting β(2)-agonists (SIROCCO): A randomised, multicentre, placebo-controlled phase 3 trial. Lancet 2016, 388, 2115–2127. [Google Scholar] [CrossRef]
- FitzGerald, J.M.; Bleecker, E.R.; Nair, P.; Korn, S.; Ohta, K.; Lommatzsch, M.; Ferguson, G.T.; Busse, W.W.; Barker, P.; Sproule, S.; et al. Benralizumab, an anti-interleukin-5 receptor α monoclonal antibody, as add-on treatment for patients with severe, uncontrolled, eosinophilic asthma (CALIMA): A randomised, double-blind, placebo-controlled phase 3 trial. Lancet 2016, 388, 2128–2141. [Google Scholar] [CrossRef]
- Nair, P.; Wenzel, S.; Rabe, K.F.; Bourdin, A.; Lugogo, N.L.; Kuna, P.; Barker, P.; Sproule, S.; Ponnarambil, S.; Goldman, M. Oral Glucocorticoid-Sparing Effect of Benralizumab in Severe Asthma. N. Engl. J. Med. 2017, 376, 2448–2458. [Google Scholar] [CrossRef]
- Le Floc’h, A.; Allinne, J.; Nagashima, K.; Scott, G.; Birchard, D.; Asrat, S.; Bai, Y.; Lim, W.K.; Martin, J.; Huang, T.; et al. Dual blockade of IL-4 and IL-13 with dupilumab, an IL-4Rα antibody, is required to broadly inhibit type 2 inflammation. Allergy 2020, 75, 1188–1204. [Google Scholar] [CrossRef]
- Wenzel, S.; Castro, M.; Corren, J.; Maspero, J.; Wang, L.; Zhang, B.; Pirozzi, G.; Sutherland, E.R.; Evans, R.R.; Joish, V.N.; et al. Dupilumab efficacy and safety in adults with uncontrolled persistent asthma despite use of medium-to-high-dose inhaled corticosteroids plus a long-acting β2 agonist: A randomised double-blind placebo-controlled pivotal phase 2b dose-ranging trial. Lancet 2016, 388, 31–44. [Google Scholar] [CrossRef]
- Castro, M.; Corren, J.; Pavord, I.D.; Maspero, J.; Wenzel, S.; Rabe, K.F.; Busse, W.W.; Ford, L.; Sher, L.; FitzGerald, J.M.; et al. Dupilumab Efficacy and Safety in Moderate-to-Severe Uncontrolled Asthma. N. Engl. J. Med. 2018, 378, 2486–2496. [Google Scholar] [CrossRef] [PubMed]
- Castro, M.; Rabe, K.F.; Corren, J.; Pavord, I.D.; Katelaris, C.H.; Tohda, Y.; Zhang, B.; Rice, M.S.; Maroni, J.; Rowe, P.; et al. Dupilumab improves lung function in patients with uncontrolled, moderate-to-severe asthma. ERJ Open Res. 2020, 6. [Google Scholar] [CrossRef] [PubMed]
- Busse, W.W.; Maspero, J.F.; Rabe, K.F.; Papi, A.; Wenzel, S.E.; Ford, L.B.; Pavord, I.D.; Zhang, B.; Staudinger, H.; Pirozzi, G.; et al. Liberty Asthma QUEST: Phase 3 Randomized, Double-Blind, Placebo-Controlled, Parallel-Group Study to Evaluate Dupilumab Efficacy/Safety in Patients with Uncontrolled, Moderate-to-Severe Asthma. Adv. Ther. 2018, 35, 737–748. [Google Scholar] [CrossRef]
- Rabe, K.F.; Nair, P.; Brusselle, G.; Maspero, J.F.; Castro, M.; Sher, L.; Zhu, H.; Hamilton, J.D.; Swanson, B.N.; Khan, A.; et al. Efficacy and Safety of Dupilumab in Glucocorticoid-Dependent Severe Asthma. N. Engl. J. Med. 2018, 378, 2475–2485. [Google Scholar] [CrossRef]
- Bacharier, L.B.; Maspero, J.F.; Katelaris, C.H.; Fiocchi, A.G.; Gagnon, R.; de Mir, I.; Jain, N.; Sher, L.D.; Mao, X.; Liu, D.; et al. Dupilumab in Children with Uncontrolled Moderate-to-Severe Asthma. N. Engl. J. Med. 2021, 385, 2230–2240. [Google Scholar] [CrossRef] [PubMed]
- Saglani, S.; Lloyd, C.M. Novel concepts in airway inflammation and remodelling in asthma. Eur. Respir. J. 2015, 46, 1796–1804. [Google Scholar] [CrossRef]
- Fuso, L.; Macis, G.; Condoluci, C.; Sbarra, M.; Contu, C.; Conte, E.G.; Angeletti, G.; Montuschi, P. Impulse oscillometry and nitrogen washout test in the assessment of small airway dysfunction in asthma: Correlation with quantitative computed tomography. J. Asthma 2019, 56, 323–331. [Google Scholar] [CrossRef]
- Mostaço-Guidolin, L.B.; Osei, E.T.; Ullah, J.; Hajimohammadi, S.; Fouadi, M.; Li, X.; Li, V.; Shaheen, F.; Yang, C.X.; Chu, F.; et al. Defective Fibrillar Collagen Organization by Fibroblasts Contributes to Airway Remodeling in Asthma. Am. J. Respir. Crit. Care Med. 2019, 200, 431–443. [Google Scholar] [CrossRef]
- Zhang, X.; Xia, T.; Lai, Z.; Zhang, Q.; Guan, Y.; Zhong, N. Uncontrolled asthma phenotypes defined from parameters using quantitative CT analysis. Eur. Radiol. 2019, 29, 2848–2858. [Google Scholar] [CrossRef]
- Shimizu, K.; Hasegawa, M.; Makita, H.; Nasuhara, Y.; Konno, S.; Nishimura, M. Comparison of airway remodelling assessed by computed tomography in asthma and COPD. Respir. Med. 2011, 105, 1275–1283. [Google Scholar] [CrossRef]
- Gorska, K.; Korczynski, P.; Mierzejewski, M.; Kosciuch, J.; Zukowska, M.; Maskey-Warzechowska, M.; Krenke, R. Comparison of endobronchial ultrasound and high resolution computed tomography as tools for airway wall imaging in asthma and chronic obstructive pulmonary disease. Respir. Med. 2016, 117, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, A.; Hall, C.; Hoffman, E.A.; Woods, J.C.; Gierada, D.S.; Castro, M. Using imaging as a biomarker for asthma. J. Allergy Clin. Immunol. 2017, 139, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Gono, H.; Fujimoto, K.; Kawakami, S.; Kubo, K. Evaluation of airway wall thickness and air trapping by HRCT in asymptomatic asthma. Eur. Respir. J. 2003, 22, 965–971. [Google Scholar] [CrossRef] [PubMed]
- Hoshino, M.; Matsuoka, S.; Handa, H.; Miyazawa, T.; Yagihashi, K. Correlation between airflow limitation and airway dimensions assessed by multidetector CT in asthma. Respir. Med. 2010, 104, 794–800. [Google Scholar] [CrossRef]
- Kasahara, K.; Shiba, K.; Ozawa, T.; Okuda, K.; Adachi, M. Correlation between the bronchial subepithelial layer and whole airway wall thickness in patients with asthma. Thorax 2002, 57, 242–246. [Google Scholar] [CrossRef] [PubMed]
- Nishimoto, K.; Karayama, M.; Inui, N.; Mori, K.; Kono, M.; Hozumi, H.; Suzuki, Y.; Furuhashi, K.; Enomoto, N.; Fujisawa, T.; et al. Relationship between fraction of exhaled nitric oxide and airway morphology assessed by three-dimensional CT analysis in asthma. Sci. Rep. 2017, 7, 10187. [Google Scholar] [CrossRef] [PubMed]
- Jiang, D.; Wang, Z.; Yu, N.; Shen, C.; Deng, L.; Guo, Y. Airway Remodeling in Asthma: Evaluation in 5 Consecutive Bronchial Generations by Using High-Resolution Computed Tomography. Respir. Care 2018, 63, 1399–1406. [Google Scholar] [CrossRef]
- Jiang, D.; Wang, Z.; Shen, C.; Jin, C.; Yu, N.; Wang, J.; Yin, N.; Guo, Y. Small airway dysfunction may be an indicator of early asthma: Findings from high-resolution CT. Ann. Allergy Asthma Immunol. 2019, 122, 498–501. [Google Scholar] [CrossRef]
- Gupta, S.; Hartley, R.; Khan, U.T.; Singapuri, A.; Hargadon, B.; Monteiro, W.; Pavord, I.D.; Sousa, A.R.; Marshall, R.P.; Subramanian, D.; et al. Quantitative computed tomography-derived clusters: Redefining airway remodeling in asthmatic patients. J. Allergy Clin. Immunol. 2014, 133, 729–738.e718. [Google Scholar] [CrossRef]
- Shim, S.S.; Schiebler, M.L.; Evans, M.D.; Jarjour, N.; Sorkness, R.L.; Denlinger, L.C.; Rodriguez, A.; Wenzel, S.; Hoffman, E.A.; Lin, C.L.; et al. Lumen area change (Delta Lumen) between inspiratory and expiratory multidetector computed tomography as a measure of severe outcomes in asthmatic patients. J. Allergy Clin. Immunol. 2018, 142, 1773–1780.e1779. [Google Scholar] [CrossRef]
- Berair, R.; Hartley, R.; Mistry, V.; Sheshadri, A.; Gupta, S.; Singapuri, A.; Gonem, S.; Marshall, R.P.; Sousa, A.R.; Shikotra, A.; et al. Associations in asthma between quantitative computed tomography and bronchial biopsy-derived airway remodelling. Eur. Respir. J. 2017, 49, 1601507. [Google Scholar] [CrossRef] [PubMed]
- Marchac, V.; Emond, S.; Mamou-Mani, T.; Le Bihan-Benjamin, C.; Le Bourgeois, M.; De Blic, J.; Scheinmann, P.; Brunelle, F. Thoracic CT in pediatric patients with difficult-to-treat asthma. AJR Am. J. Roentgenol 2002, 179, 1245–1252. [Google Scholar] [CrossRef] [PubMed]
- Tsuge, M.; Ikeda, M.; Kondo, Y.; Tsukahara, H. Severe pediatric asthma with a poor response to omalizumab: A report of three cases and three-dimensional bronchial wall analysis. J. Int. Med. Res. 2022, 50, 3000605211070492. [Google Scholar] [CrossRef] [PubMed]
- Riccio, A.M.; Dal Negro, R.W.; Micheletto, C.; De Ferrari, L.; Folli, C.; Chiappori, A.; Canonica, G.W. Omalizumab modulates bronchial reticular basement membrane thickness and eosinophil infiltration in severe persistent allergic asthma patients. Int. J. Immunopathol. Pharmacol. 2012, 25, 475–484. [Google Scholar] [CrossRef]
- Riccio, A.M.; Mauri, P.; De Ferrari, L.; Rossi, R.; Di Silvestre, D.; Benazzi, L.; Chiappori, A.; Dal Negro, R.W.; Micheletto, C.; Canonica, G.W. Galectin-3: An early predictive biomarker of modulation of airway remodeling in patients with severe asthma treated with omalizumab for 36 months. Clin. Transl. Allergy 2017, 7, 6. [Google Scholar] [CrossRef]
- Zastrzeżyńska, W.; Przybyszowski, M.; Bazan-Socha, S.; Gawlewicz-Mroczka, A.; Sadowski, P.; Okoń, K.; Jakieła, B.; Plutecka, H.; Ćmiel, A.; Sładek, K.; et al. Omalizumab may decrease the thickness of the reticular basement membrane and fibronectin deposit in the bronchial mucosa of severe allergic asthmatics. J. Asthma 2020, 57, 468–477. [Google Scholar] [CrossRef]
- Hoshino, M.; Ohtawa, J. Effects of adding omalizumab, an anti-immunoglobulin E antibody, on airway wall thickening in asthma. Respiration 2012, 83, 520–528. [Google Scholar] [CrossRef]
- Tajiri, T.; Niimi, A.; Matsumoto, H.; Ito, I.; Oguma, T.; Otsuka, K.; Takeda, T.; Nakaji, H.; Inoue, H.; Iwata, T.; et al. Comprehensive efficacy of omalizumab for severe refractory asthma: A time-series observational study. Ann. Allergy Asthma Immunol. 2014, 113, 470–475.e2. [Google Scholar] [CrossRef]
- Przybyszowski, M.; Paciorek, K.; Zastrzeżyńska, W.; Gawlewicz-Mroczka, A.; Trojan-Królikowska, A.; Orłowska, A.; Soja, J.; Pawlik, W.; Sładek, K. Influence of omalizumab therapy on airway remodeling assessed with high-resolution computed tomography (HRCT) in severe allergic asthma patients. Adv. Respir. Med. 2018; online ahead of print. [Google Scholar] [CrossRef]
- Haldar, P.; Brightling, C.E.; Hargadon, B.; Gupta, S.; Monteiro, W.; Sousa, A.; Marshall, R.P.; Bradding, P.; Green, R.H.; Wardlaw, A.J.; et al. Mepolizumab and exacerbations of refractory eosinophilic asthma. N. Engl. J. Med. 2009, 360, 973–984. [Google Scholar] [CrossRef]
- Chachi, L.; Diver, S.; Kaul, H.; Rebelatto, M.C.; Boutrin, A.; Nisa, P.; Newbold, P.; Brightling, C. Computational modelling prediction and clinical validation of impact of benralizumab on airway smooth muscle mass in asthma. Eur. Respir. J. 2019, 54. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Drug | Year | Analysis | Study | Ref. |
|---|---|---|---|---|
| Omalizumab | 2012 | Bronchial biopsies | 11 adult severely allergic asthmatics, 12-month treatment
| [134] |
| Omalizumab | 2012 | CT airway analysis | 14 adult severely allergic asthmatics, 16-week treatment
| [137] |
| Omalizumab | 2014 | CT airway analysis | 26 adult severely allergic asthmatics, 48-week treatment
| [138] |
| Omalizumab | 2017 | Bronchial biopsies | 8 adult severely allergic asthmatics, 36-month treatment
| [135] |
| Omalizumab | 2018 | CT airway analysis | 12 adult severely allergic asthmatics, >4-month treatment
| [139] |
| Omalizumab | 2020 | Bronchial biopsies | 13 adult severely allergic asthmatics, >12-month treatment
| [136] |
| Mepolizumab | 2009 | CT airway analysis | 29 adult severely allergic asthmatics, 12-month treatment
| [140] |
| Benralizumab | 2019 | Bronchial biopsies | 15 adult severely allergic asthmatics, 12-month treatment
| [141] |
| Dupilumab | No study on in vivo effects on airway remodeling |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsuge, M.; Ikeda, M.; Tsukahara, H. Novel Lung Growth Strategy with Biological Therapy Targeting Airway Remodeling in Childhood Bronchial Asthma. Children 2022, 9, 1253. https://doi.org/10.3390/children9081253
Tsuge M, Ikeda M, Tsukahara H. Novel Lung Growth Strategy with Biological Therapy Targeting Airway Remodeling in Childhood Bronchial Asthma. Children. 2022; 9(8):1253. https://doi.org/10.3390/children9081253
Chicago/Turabian StyleTsuge, Mitsuru, Masanori Ikeda, and Hirokazu Tsukahara. 2022. "Novel Lung Growth Strategy with Biological Therapy Targeting Airway Remodeling in Childhood Bronchial Asthma" Children 9, no. 8: 1253. https://doi.org/10.3390/children9081253
APA StyleTsuge, M., Ikeda, M., & Tsukahara, H. (2022). Novel Lung Growth Strategy with Biological Therapy Targeting Airway Remodeling in Childhood Bronchial Asthma. Children, 9(8), 1253. https://doi.org/10.3390/children9081253