
Role of Ultrasound Evaluation of Temporomandibular Joint in Juvenile Idiopathic Arthritis: A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
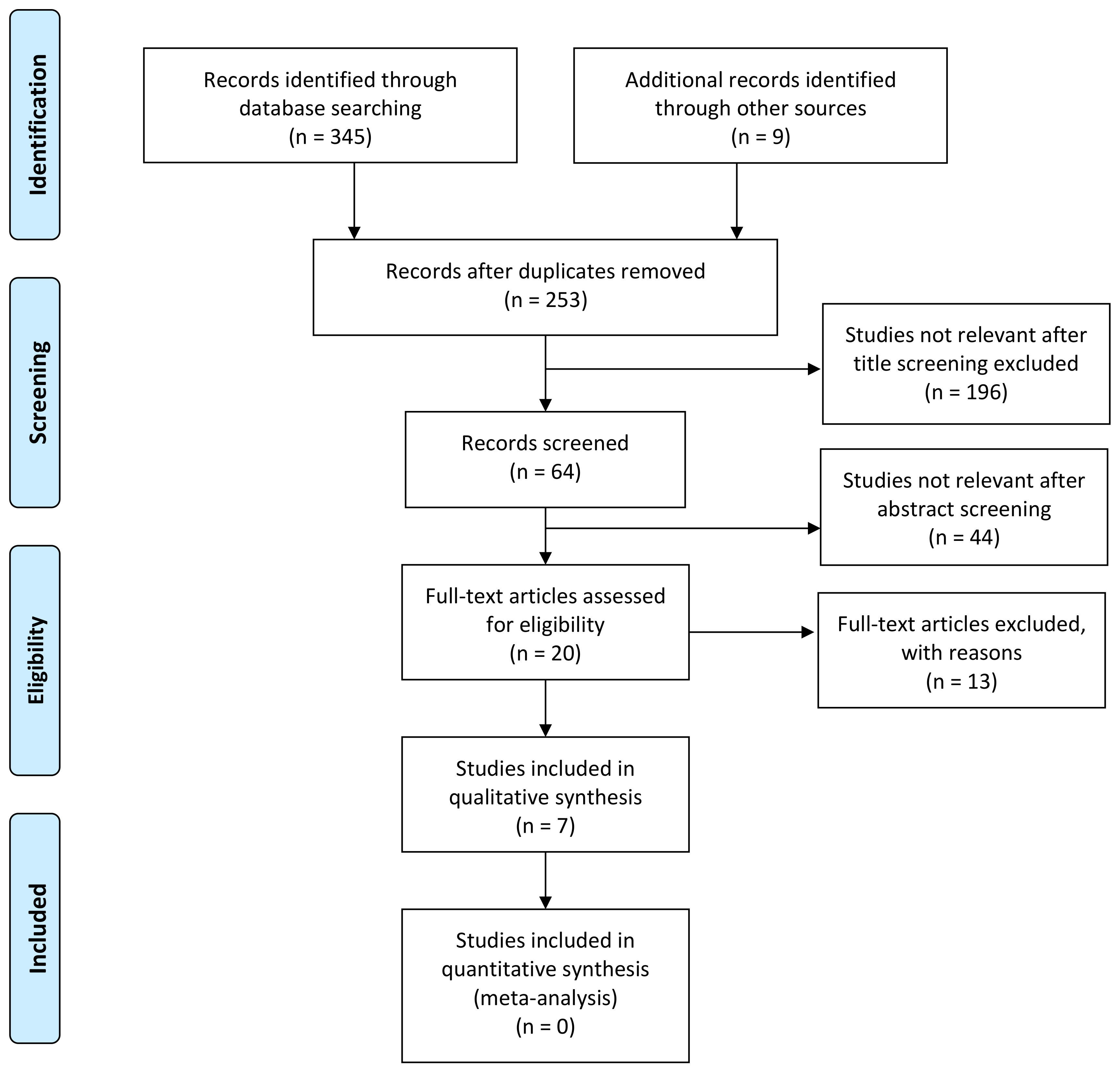
2.1. Search Strategy
2.2. Inclusion/Exclusion Criteria
2.3. Study Selection and Quality Assessment
3. Results
3.1. Joint Effusion
3.2. Condylar Changes
3.3. Synovial Thickening
3.4. Power Doppler Signal
3.5. Comparison Indicators
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| JIA | Juvenile idiopathic arthritis |
| ILAR | International League of Associations for Rheumatology |
| RF | Rheumatoid factor |
| TMJ | Temporomandibular joint |
| US | Ultrasound |
| MRI | Magnetic resonance imaging |
| Gd-MRI | Gadolinium-enhanced MRI |
| TMD | Temporomandibular disorder |
| PWD | Power Doppler |
| LPAS | Lateral periarticular joint space |
References
- Ravelli, A.; Martini, A. Juvenile idiopathic arthritis. Lancet 2007, 369, 767–778. [Google Scholar] [CrossRef]
- Cimaz, R.; Marino, A.; Martini, A. How I treat juvenile idiopathic arthritis: A state of the art review. Autoimmun. Rev. 2017, 16, 1008–1015. [Google Scholar] [CrossRef] [PubMed]
- Petty, R.E.; Southwood, T.R.; Manners, P.; Baum, J.; Glass, D.N.; Goldenberg, J.; He, X.; Maldonado-Cocco, J.; Orozco-Alcala, J.; Prieur, A.-M.; et al. International league of associations for rheumatology classification of juvenile idiopathic arthritis: Second revision, Edmonton, 2001. J. Rheumatol. 2004, 31, 390–392. [Google Scholar] [PubMed]
- Nigrovic, P.A.; Colbert, R.A.; Holers, V.M.; Ozen, S.; Ruperto, N.; Thompson, S.D.; Wedderburn, L.R.; Yeung, R.S.M.; Martini, A. Biological classification of childhood arthritis: Roadmap to a molecular nomenclature. Nat. Rev. Rheumatol. 2021, 17, 257–269. [Google Scholar] [CrossRef]
- Twilt, M.; Mobers, S.M.L.M.; Arends, L.R.; Cate, R.T.; Van Suijlekom-Smit, L. Temporomandibular involvement in juvenile idiopathic arthritis. J. Rheumatol. 2004, 31, 1418–1422. [Google Scholar] [CrossRef]
- Küseler, A.; Pedersen, T.K.; Gelineck, J.; Herlin, T. A 2 year followup study of enhanced magnetic resonance imaging and clinical examination of the temporomandibular joint in children with juvenile idiopathic arthritis. J. Rheumatol. 2005, 32, 162–169. [Google Scholar]
- Pedersen, T.K.; Küseler, A.; Gelineck, J.; Herlin, T. A prospective study of magnetic resonance and radiographic imaging in relation to symptoms and clinical findings of the temporomandibular joint in children with juvenile idiopathic arthritis. J. Rheumatol. 2008, 35, 1668–1675. [Google Scholar]
- Bender, M.E.; Lipin, R.B.; Goudy, S.L. Development of the pediatric temporomandibular joint. Oral Maxillofac. Surg. Clin. N. Am. 2018, 30, 1–9. [Google Scholar] [CrossRef]
- Nahhas, R.W.; Valiathan, M.; Sherwood, R.J. Variation in timing, duration, intensity, and direction of adolescent growth in the mandible, maxilla, and cranial base: The Fels longitudinal study. Anat. Rec. 2014, 297, 1195–1207. [Google Scholar] [CrossRef]
- Von Bremen, J.; Ruf, S. Juvenile idiopathic arthritis and now?: A systematic Literature review of changes in craniofacial morphology. J. Orofac. Orthop. 2012, 73, 265–276. [Google Scholar] [CrossRef]
- Minervini, G.; Fiorillo, L.; Russo, D.; Lanza, A.; D’Amico, C.; Cervino, G.; Meto, A.; Di Francesco, F. Prosthodontic Treatment in Patients with Temporomandibular Disorders and Orofacial Pain and/or Bruxism: A Review of the Literature. Prosthesis 2022, 4, 253–262. [Google Scholar] [CrossRef]
- Stoustrup, P.; Resnick, C.M.; Pedersen, T.K.; Abramowicz, S.; Michelotti, A.; Küseler, A.; Verna, C.; Kellenberger, C.J.; Nordal, E.B.; Caserta, G.; et al. TMJ Juvenile Arthritis Working Group. Standardizing Terminology and Assessment for Orofacial Conditions in Juvenile Idiopathic Arthritis: International, Multidisciplinary Consensus-based Recommendations. J. Rheumatol. 2019, 46, 518–522. [Google Scholar] [CrossRef]
- Chatzigianni, A.; Kyprianou, C.; Papadopoulos, M.A.; Sidiropoulou, S. Dentoalveolar characteristics in children with juvenile idiopathic arthritis. Organ./Off. J. Dtsch. Ges. Kieferorthopadie 2018, 79, 133–139. [Google Scholar] [CrossRef]
- Stoustrup, P.; Glerup, M.; Bilgrau, A.E.; Küseler, A.; Verna, C.; Christensen, A.E.; Kristensen, K.D.; Nørholt, S.E.; Twilt, M.; Herlin, T.; et al. Cumulative Incidence of Orofacial Manifestations in Early Juvenile Idiopathic Arthritis: A Regional, Three-Year Cohort Study. Arthritis Care Res. 2019, 72, 907–916. [Google Scholar] [CrossRef]
- De Sonnaville, W.; Speksnijder, C.M.; Zuithoff, N.; Verkouteren, D.; Wulffraat, N.W.; Steenks, M.H.; Rosenberg, A. Mandibular range of motion in children with juvenile idiopathic arthritis with and without clinically established temporomandibular joint involvement and in healthy children; a cross-sectional study. Pediatr. Rheumatol. Online J. 2021, 19, 106. [Google Scholar] [CrossRef]
- Cedströmer, A.L.; Andlin-Sobocki, A.; Abbu, N.; Hedenberg-Magnusson, B.; Dahlström, L.; Berntson, L. Condylar alterations and facial growth in children with juvenile idiopathic arthritis. J. Orofac. Orthop. Fortschr. Kieferorthopadie Organ/Off. J. Dtsch. Ges. Kieferorthopadie 2020, 81, 163–171. [Google Scholar] [CrossRef]
- Keller, H.; Müller, L.M.; Markic, G.; Schraner, T.; Kellenberger, C.J.; Saurenmann, R.K. Is early TMJ involvement in children with juvenile idiopathic arthritis clinically detectable? Clinical examination of the TMJ in comparison with contrast enhanced MRI in patients with juvenile idiopathic arthritis. Pediatr. Rheumatol. 2015, 13, 56. [Google Scholar] [CrossRef]
- Koos, B.; Twilt, M.; Kyank, U.; Fischer-Brandies, H.; Gaßling, V.; Tzaribachev, N. Reliability of clinical symptoms in diagnosing temporomandibular joint arthritis in juvenile idiopathic arthritis. J. Rheumatol. 2014, 41, 1871–1877. [Google Scholar] [CrossRef]
- Tolend, M.; Doria, A.S.; Meyers, A.B.; Larheim, T.A.; Abramowicz, S.; Aguet, J.; Appenzeller, S.; Arvidsson, L.Z.; Averill, L.W.; Feldman, B.M.; et al. Assessing the Reliability of the OMERACT Juvenile Idiopathic Arthritis Magnetic Resonance Scoring System for Temporomandibular Joints (JAMRIS-TMJ). J. Clin. Med. 2021, 10, 4047. [Google Scholar] [CrossRef]
- Tolend, M.A.; Twilt, M.; Cron, R.Q.; Tzaribachev, N.; Guleria, S.; von Kalle, T.; Koos, B.; Miller, E.; Stimec, J.; Vaid, Y.; et al. Toward establishing a standardized magnetic resonance imaging scoring system for temporomandibular joints in juvenile idiopathic arthritis. Arthritis Care Res. 2018, 70, 758–767. [Google Scholar] [CrossRef]
- Stoll, M.L.; Guleria, S.; Mannion, M.L.; Young, D.W.; Royal, S.A.; Cron, R.Q.; Vaid, Y.N. Defining the normal appearance of the temporomandibular joints by magnetic resonance imaging with contrast: A comparative study of children with and without juvenile idiopathic arthritis. Pediatr. Rheumatol. 2018, 16, 8. [Google Scholar] [CrossRef]
- Jank, S.; Haase, S.; Strobl, H.; Michels, H.; Häfner, R.; Missmann, M.; Bodner, G.; Mur, E.; Schroeder, D. Sonographic investigation of the temporomandibular joint in patients with juvenile idiopathic arthritis: A pilot study. Arthritis Rheum. 2007, 57, 213–218. [Google Scholar] [CrossRef]
- Weiss, P.F.; Arabshahi, B.; Johnson, A.; Bilaniuk, L.T.; Zarnow, D.; Cahill, A.M.; Feudtner, C.; Cron, R.Q. High prevalence of temporomandibular joint arthritis at disease onset in children with juvenile idiopathic arthritis, as detected by magnetic resonance imaging but not by ultrasound. Arthritis Rheum. 2008, 58, 1189–1196. [Google Scholar] [CrossRef]
- Müller, L.; Kellenberger, C.J.; Cannizzaro, E.; Ettlin, D.; Schraner, T.; Bolt, I.B.; Peltomäki, T.; Saurenmann, R.K. Early diagnosis of temporomandibular joint involvement in juvenile idiopathic arthritis: A pilot study comparing clinical examination and ultrasound to magnetic resonance imaging. Rheumatology 2009, 48, 680–685. [Google Scholar] [CrossRef]
- Melchiorre, D.; Falcini, F.; Kaloudi, O.; Bandinelli, F.; Nacci, F.; Matucci Cerinic, M. Sonographic evaluation of the temporomandibular joints in juvenile idiopathic arthritis. J. Ultrasound 2010, 13, 34–37. [Google Scholar] [CrossRef]
- Assaf, A.T.; Kahl-Nieke, B.; Feddersen, J.; Habermann, C.R. Is high-resolution ultrasonography suitable for the detection of temporomandibular joint involvement in children with juvenile idiopathic arthritis? Dentomaxillofacial Radiol. 2013, 42, 20110379. [Google Scholar] [CrossRef]
- Kirkhus, E.; Gunderson, R.B.; Smith, H.-J.; Flatø, B.; Hetlevik, S.O.; Larheim, T.A.; Arvidsson, L.Z. Temporomandibular joint involvement in childhood arthritis: Comparison of ultrasonography-assessed capsular width and MRI-assessed synovitis. Dentomaxillofacial Radiol. 2016, 45, 20160195. [Google Scholar] [CrossRef]
- Zwir, L.F.; Terreri, M.T.; do Amaral E Castro, A.; Rodrigues, W.D.R.; Fernandes, A.R.C. Is power Doppler ultrasound useful to evaluate temporomandibular joint inflammatory activity in juvenile idiopathic arthritis? Clin. Rheumatol. 2020, 39, 1237–1240. [Google Scholar] [CrossRef]
- Tonni, I.; Borghesi, A.; Tonesi, S.; Fossati, G.; Ricci, F.; Visconti, L. An ultrasound protocol for temporomandibular joint in juvenile idiopathic arthritis: A pilot study. Dentomaxillofacial Radiol. 2021, 50, 20200399. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef]
- Available online: http://www.cebm.net/oxford-centre-evidence-based-medicine-levels-evidence-march-2009/ (accessed on 3 May 2022).
- Higgins, J.P.T.; Green, S. (Eds.) The Cochrane Collaboration. In Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0; Chichester (UK): John Wiley & Son, 2011; Available online: http://www.cochrane-handbook.org (accessed on 3 May 2022).
- Chen, H.Y.; Wu, S.K.; Lu, C.C.; You, J.Y.; Lai, C.L. Assessing the mobility of the mandibular condyle by sonography. Patient Prefer. Adherence 2014, 8, 1419–1425. [Google Scholar] [CrossRef] [PubMed]
- Iordache, C.; Fatu, A.M.; Pomrleanu, C.; Scurtu, D.; Codrina, A. Temporomandibular joint in juvenile idiopathic arthritis: An imaging study and ergonomic considerations. Rom. J. Oral Rehabil. 2017, 9, 60–67. [Google Scholar]
- Von Schuckmann, L.; Klotsche, J.; Suling, A.; Kahl-Nieke, B.; Foeldvari, I. Temporomandibular joint involvement in patients with juvenile idiopathic arthritis: A retrospective chart review. Scand. J. Rheumatol. 2020, 49, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Alqanatish, J.T.; Alrewaithi, B.S.; Alsewairi, W.M.; Khan, A.H.; Alsalman, M.J.; Alrasheed, A.A. Temporomandibular joint involvement in children with juvenile idiopathic arthritis: A single tertiary-center experience. Saudi Med. J. 2021, 42, 399–404. [Google Scholar] [CrossRef]
- Parra, D.A.; Chan, M.; Krishnamurthy, G.; Spiegel, L.; Amaral, J.G.; Temple, M.J.; John, P.R.; Connolly, B.L. Use and accuracy of US guidance for image-guided injections of the temporomandibular joints in children with arthritis. Pediatr. Radiol. 2010, 40, 1498–1504. [Google Scholar] [CrossRef]
- Stoll, M.L.; Good, J.; Sharpe, T.; Beukelman, T.; Young, D.; Waite, P.D.; Cron, R.Q. Intra-articular corticosteroid injections to the temporomandibular joints are safe and appear to be effective therapy in children with juvenile idiopathic arthritis. J. Oral Maxillofac. Surg. 2012, 70, 1802–1807. [Google Scholar] [CrossRef]
- Habibi, S.; Ellis, J.; Strike, H.; Ramanan, A.V. Safety and efficacy of US-guided CS injection into temporomandibular joints in children with active JIA. Rheumatology 2011, 51, 874–877. [Google Scholar] [CrossRef]
- Young, C.M.; Shiels, W.E., II; Coley, B.D.; Hogan, M.J.; Murakami, J.W.; Jones, K.; Higgins, G.C.; Rennebohm, R.M. Ultrasound-guided corticosteroid injection therapy for juvenile idiopathic arthritis: 12-year care experience. Pediatr. Radiol. 2012, 42, 1481–1489. [Google Scholar] [CrossRef]
- Stoll, M.L.; Morlandt, A.B.; Teerawattanapong, S.; Young, D.; Waite, P.D.; Cron, R.Q. Safety and efficacy of intra-articular infliximab therapy for treatment-resistant temporomandibular joint arthritis in children: A retrospective study. Rheumatology 2012, 52, 554–559. [Google Scholar] [CrossRef]
- Olsen-Bergem, H.; Bjørnland, T. A cohort study of patients with juvenile idiopathic arthritis and arthritis of the temporomandibular joint: Outcome of arthrocentesis with and without the use of steroids. Int. J. Oral. Maxillofac. Surg. 2014, 43, 990–995. [Google Scholar] [CrossRef]
- Resnick, C.M.; Vakilian, P.M.; Kaban, L.B.; Peacock, Z.S. Is Intra-Articular Steroid Injection to the Temporomandibular Joint for Juvenile Idiopathic Arthritis More Effective and Efficient When Performed With Image Guidance? J. Oral. Maxillofac. Surg. 2017, 75, 694–700. [Google Scholar] [CrossRef] [PubMed]
- Frid, P.; Augdal, T.A.; Larheim, T.A.; Halbig, J.; Rypdal, V.; Songstad, N.T.; Rosén, A.; Tylleskär, K.B.; Berstad, J.R.; Flatø, B.; et al. Efficacy and safety of intraarticular corticosteroid injections in adolescents with juvenile idiopathic arthritis in the temporomandibular joint: A Norwegian 2-year prospective multicenter pilot study. Pediatr. Rheumatol. Online J. 2020, 18, 75. [Google Scholar] [CrossRef] [PubMed]
- Johnson, K. Imaging of juvenile idiopathic arthritis. Pediatr. Radiol. 2006, 36, 743–758. [Google Scholar] [CrossRef] [PubMed]
- Cimaz, R.; Giani, T.; Caporali, R. What is the real role of ultrasound in the management of juvenile idiopathic arthritis? Ann. Rheum. Dis. 2020, 79, 437–439. [Google Scholar] [CrossRef]
- Collado, P.; Vojinovic, J.; Nieto, J.C.; Windschall, D.; Magni-Manzoni, S.; Bruyn, G.A.W.; Iagnocco, A.; D’Agostino, M.A.; Naredo, E.; on behalf of the Omeract Ultrasound Pediatric Group. Toward standardized musculoskeletal ultrasound in pediatric rheumatology: Normal age-related ultrasound findings. Arthritis Care Res. 2016, 68, 348–356. [Google Scholar] [CrossRef]
- Collado, P.; Windschall, D.; Vojinovic, J.; Magni-Manzoni, S.; Balint, P.; Bruyn, G.A.; Hernandez-Diaz, C.; Nieto, J.C.; Ravagnani, V.; Tzaribachev, N.; et al. Amendment of the OMERACT ultrasound definitions of joints’ features in healthy children when using the DOPPLER technique. Pediatr. Rheumatol. 2018, 16, 23. [Google Scholar] [CrossRef]
- Windschall, D.; Collado, P.; Vojinovic, J.; Magni-Manzoni, S.; Balint, P.; Bruyn, G.A.; Hernandez-Diaz, C.; Nieto, J.C.; Ravagnani, V.; Tzaribachev, N.; et al. Age-Related vascularization and ossification of joints in children: An international pilot study to test multi-observer ultrasound reliability. Arthritis Care Res. 2017, 72, 498–506. [Google Scholar] [CrossRef]
- Katzberg, R.W.; Conway, W.F.; Ackerman, S.J.; Gonzales, T.S.; Kheyfits, V.; Cronan, M.S. Pilot study to show the feasibility of high-resolution sagittal ultrasound imaging of the temporomandibular joint. J. Oral Maxillofac. Surg. 2017, 75, 1151–1162. [Google Scholar] [CrossRef]
- Tolend, M.; Junhasavasdikul, T.; Cron, R.Q.; Clemente, E.J.I.; von Kalle, T.; Kellenberger, C.J.; Koos, B.; Miller, E.; van Rossum, M.A.; Saurenmann, R.K.; et al. Discrete choice experiment on a magnetic resonance imaging scoring system for temporomandibular joints in juvenile idiopathic arthritis. Arthritis Care Res. 2021, 74, 308–316. [Google Scholar] [CrossRef]
- Kellenberger, C.J.; Junhasavasdikul, T.; Tolend, M.; Doria, A.S. Temporomandibular joint atlas for detection and grading of juvenile idiopathic arthritis involvement by magnetic resonance imaging. Pediatr. Radiol. 2017, 48, 411–426. [Google Scholar] [CrossRef]
- Jank, S.; Rudisch, A.; Bodner, G.; Brandlmaier, I.; Gerhard, S.; Emshoff, R. High-resolution ultrasonography of the TMJ: Helpful diagnostic approach for patients with TMJ disorders? J. Craniomaxillofac. Surg. 2001, 29, 366–371. [Google Scholar] [CrossRef]
- Klatkiewicz, T.; Gawriołek, K.; Pobudek Radzikowska, M.; Czajka-Jakubowska, A. Ultrasonography in the Diagnosis of Temporomandibular Disorders: A Meta-Analysis. Med. Sci. Monit. 2018, 24, 812–817. [Google Scholar] [CrossRef]
- Rossi Espagnet, M.C.; Bernardi, B.; Pasquini, L.; Talamanca, L.; Tom, P.; Napolitano, A. Signal intensity at unenhanced T1-weighted magnetic resonance in the globus pallidus and dentate nucleus after serial administrations of a macrocyclic gadolinium based contrast agent in children. Pediatr. Radiol. 2017, 47, 1345–1352. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| PICO |
|---|
| Patients: Patients with JIA evaluated for TMJ involvement Intervention: Use of US for assessment of TMJ involvement Comparison: Comparison with healthy controls and/or MRI for evaluation of TMJ involvement Outcome: Identify active synovitis of TMJ in JIA patients Database included: Medline via PubMed, EMBASE, WEB OF SCIENCE, SCOPUS |
| Study | Study Type | Level of Evidence | Uniform Inclusion Criteria | Standardized Imaging Protocol | Sufficient Outcome Variables Description | Blinded Assessor | Risk of Bias |
|---|---|---|---|---|---|---|---|
| Weiss [23] | Prospective | 3b | No | Yes | No | Unclear | High |
| Muller [24] | Prospective | 4 | Yes | Yes | Yes | Yes | Low |
| Melchiorre [25] | Prospective | 4 | No | Yes | Yes | Yes | High |
| Assaf [26] | Prospective | 3b | No | Yes | Yes | No | High |
| Kirkhus [27] | Prospective | 4 | No | Yes | No | Yes | High |
| Zwir [28] | Prospective | 4 | Yes | Yes | No | Yes | High |
| Tonni [29] | Prospective | 3b | No | Yes | Yes | Unclear | High |
| Weiss et al. (2008) [23] | Muller et al. (2009) [24] | Melchiorre et al. (2010) [25] | Assaf et al. (2015) [26] | Kirkhus et al. (2016) [27] | Zwir et al. (2020) [28] | Tonni et al. (2021) [29] | |
|---|---|---|---|---|---|---|---|
| N of JIA pts (female)/joints | 32 (25)/64 | 30(16)/60 | 68 (57)/136; 40 healthy controls | 20 (16)/40 | 55 (42) | 92(63)/184 | 8(7)/14; 7 healthy controls |
| Age, years | 8.6 (median) | 9.8 (median) | 11 (mean) | 11.06 (mean) | 12.4 (mean) | 12.7 (mean) | 11.6 (mean) |
| Transducer frequency | 12.5 MHz | 12 MHz | 8.5 MHz | 12 MHz | 12–18 MHz | 13 and 6.7 ** MHz | 15 MHz |
| Who did the US? | Radiologist | Radiologist | Rheumatologist | Radiologist | Radiologist | Radiologist | Radiologist |
| Joint effusion | 0 pts (Defined as fluid collection in the joint) | 8/29 (28%) pts and 10/58 (17%) joints (Defined as thickening of the joint capsule (>2 mm)) | 46/68 pts (68% (bilateral in 16 (35%) cases) (Defined as thickening of the joint capsule >1.5 mm and the presence of a hypoechoic area within the joint space) | 20 positive images/160 (12.5%) (Defined as sonographically visible fluid accumulation within the articular space) | Sensitivity 72%, specificity 70% for the capsular width at the subcondylar level * (Capsular width was measured as an indirect measurement of synovitis. Capsular cut-off of 1.2 mmL) | NE | 0 pts |
| Synovial thickening | NE | NE | NE | 55 positive images/160 (34.4%) (Defined as a value greater than 1.56 mm) | NE | NE | LPAS of JIA pts 0.086 cm LPAS of controls 0.0055 cm (Evaluated as the lateral periarticular space (LPAS) Defined as the width of the synovial joint space measured from the cortical contour of the condyle to the contour of the capsule) |
| Synovial PWD | NE | NE | NE | NE | NE | 0 pts | NE |
| Condylar changes | 9 pts (28%) | 7/29 (24%) pts and 10/58 (17%) joints | 62 (91.2%) out of 68 pts | 124 positive images/160 (77.5%) | NE | NE | NE |
| TMJ-MRI assessment and/or healthy controls comparison | 23% agreement and a kappa coefficient of 0 for acute TMJ arthritis 50% agreement and a kappa coefficient of 0.12 for chronic TMJ involvement | A pathological US was statistically significantly correlated with active TMJ arthritis on MRI (chi-square p 0.008 for all joints and p 0.047 for patients) | No TMJ-MRI assessment. In all 40 healthy controls, the TMJ capsule was less than 1.4 mm thick | For every enrolled patient the involvement of the TMJ was proven by MRI | The correlation between ultrasonography-assessed capsular width and MRI-assessed amount of synovitis was moderate both at the subcondylar and at the condylar levels (Spearman’s rho (r): 0.483; p, 0.001 and 0.347; p, 0.001, respectively). | Poor sensitivity (0%), low specificity (36.4%), very low positive predictive value (0%), and high negative predictive value (100%) when compared with MR | The Spearman test applied to the values of LPAS measured in ultrasound and the corresponding MR images showed a proportional positive correlation with a p of 0.623 and a p < 0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marino, A.; De Lucia, O.; Caporali, R. Role of Ultrasound Evaluation of Temporomandibular Joint in Juvenile Idiopathic Arthritis: A Systematic Review. Children 2022, 9, 1254. https://doi.org/10.3390/children9081254
Marino A, De Lucia O, Caporali R. Role of Ultrasound Evaluation of Temporomandibular Joint in Juvenile Idiopathic Arthritis: A Systematic Review. Children. 2022; 9(8):1254. https://doi.org/10.3390/children9081254
Chicago/Turabian StyleMarino, Achille, Orazio De Lucia, and Roberto Caporali. 2022. "Role of Ultrasound Evaluation of Temporomandibular Joint in Juvenile Idiopathic Arthritis: A Systematic Review" Children 9, no. 8: 1254. https://doi.org/10.3390/children9081254
APA StyleMarino, A., De Lucia, O., & Caporali, R. (2022). Role of Ultrasound Evaluation of Temporomandibular Joint in Juvenile Idiopathic Arthritis: A Systematic Review. Children, 9(8), 1254. https://doi.org/10.3390/children9081254