
Barriers and Enablers for Continuous Improvement Methodologies within the Irish Pharmaceutical Industry




Abstract
:1. Introduction
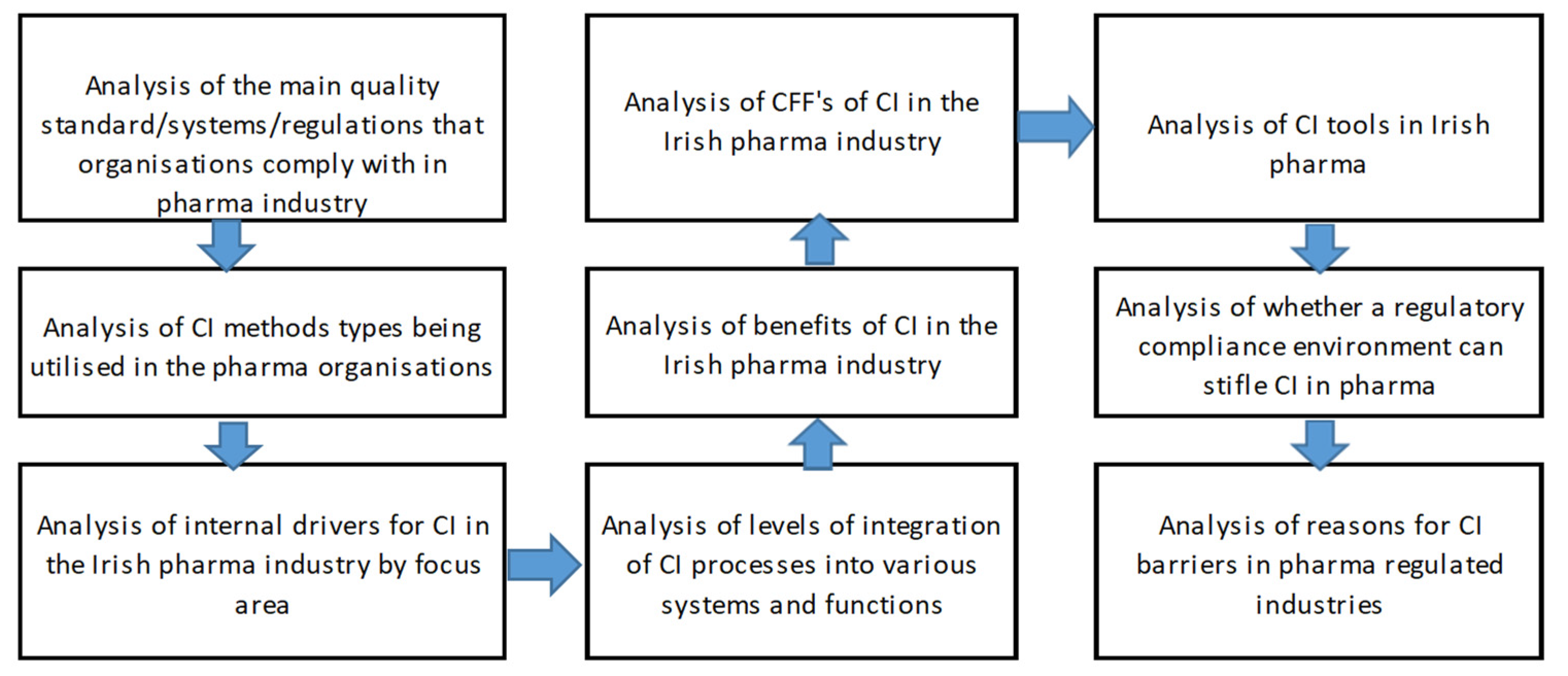
- What are the CI methods and tools utilised for CI in the Irish Pharmaceutical industry?
- What are the drivers and benefits for use of CI within the Pharma industry?
- What are the CFF’s for deployment of CI in the Irish Pharma industry?
- Does the highly regulated nature of the Irish Pharmaceutical industry pose a unique and significant barrier to CI methodology deployment and culture?
2. Literature Review
2.1. Pharmaceutical Industry & Regulatory Background
2.2. Regulatory Environments a Specific CFF to CI Deployment
3. Methodology
4. Results
5. Discussion and Implications
6. Conclusions, Limitations, and Directions for Further Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| Q1. What country/continent are you based in? |
| Q2. What industry are you in? |
| Q3. What function or department do you work in? Please tick as appropriate. |
| Q4. How many years of experience do you have in continuous improvement methodologies? |
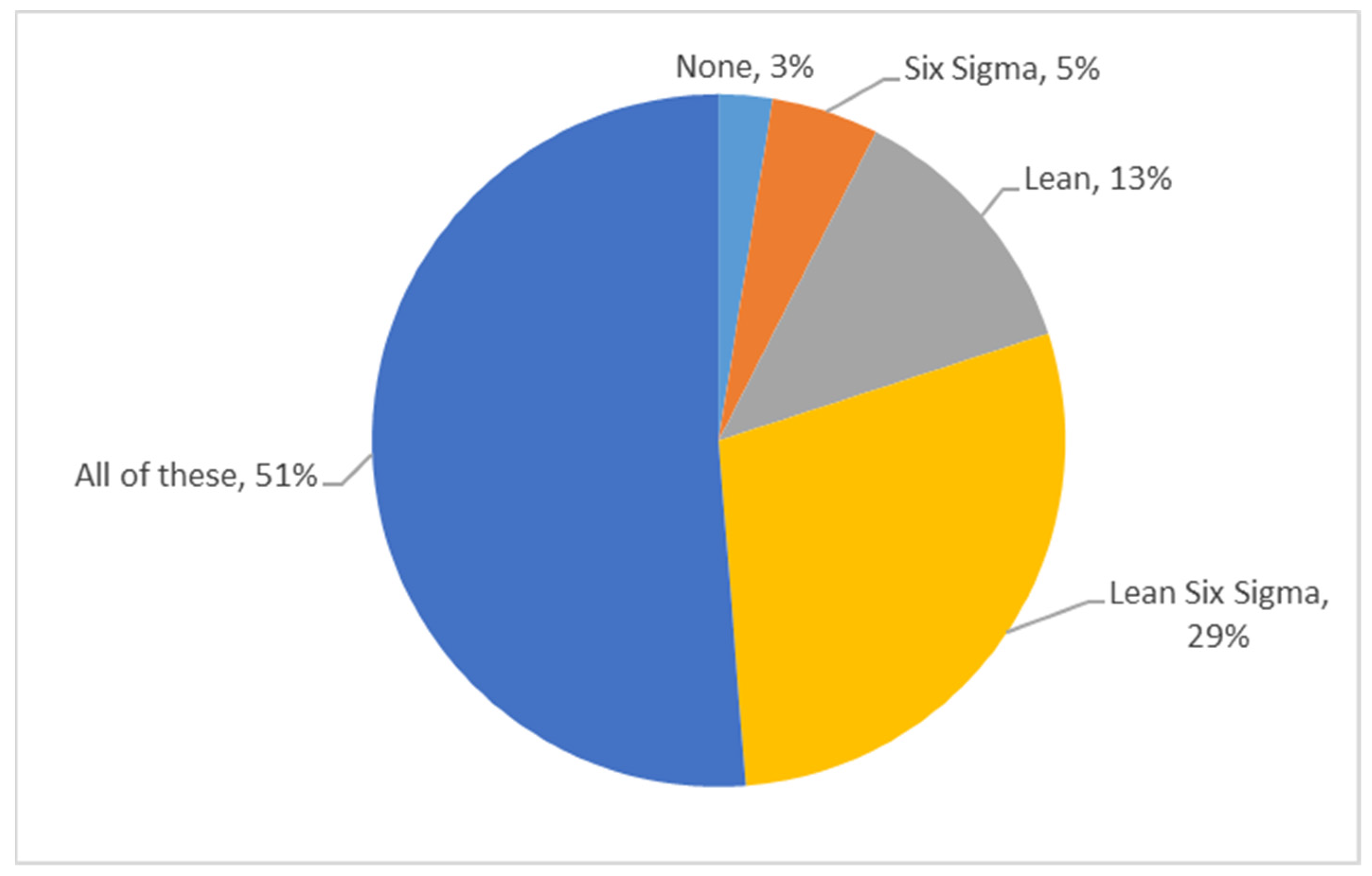
Q5. Which of the following methodologies and systems have you worked with or are aware of as being applied in your organization?
|
Q6. How integrated are CI into the following quality subsystem or subsystems (Likert scale):
|
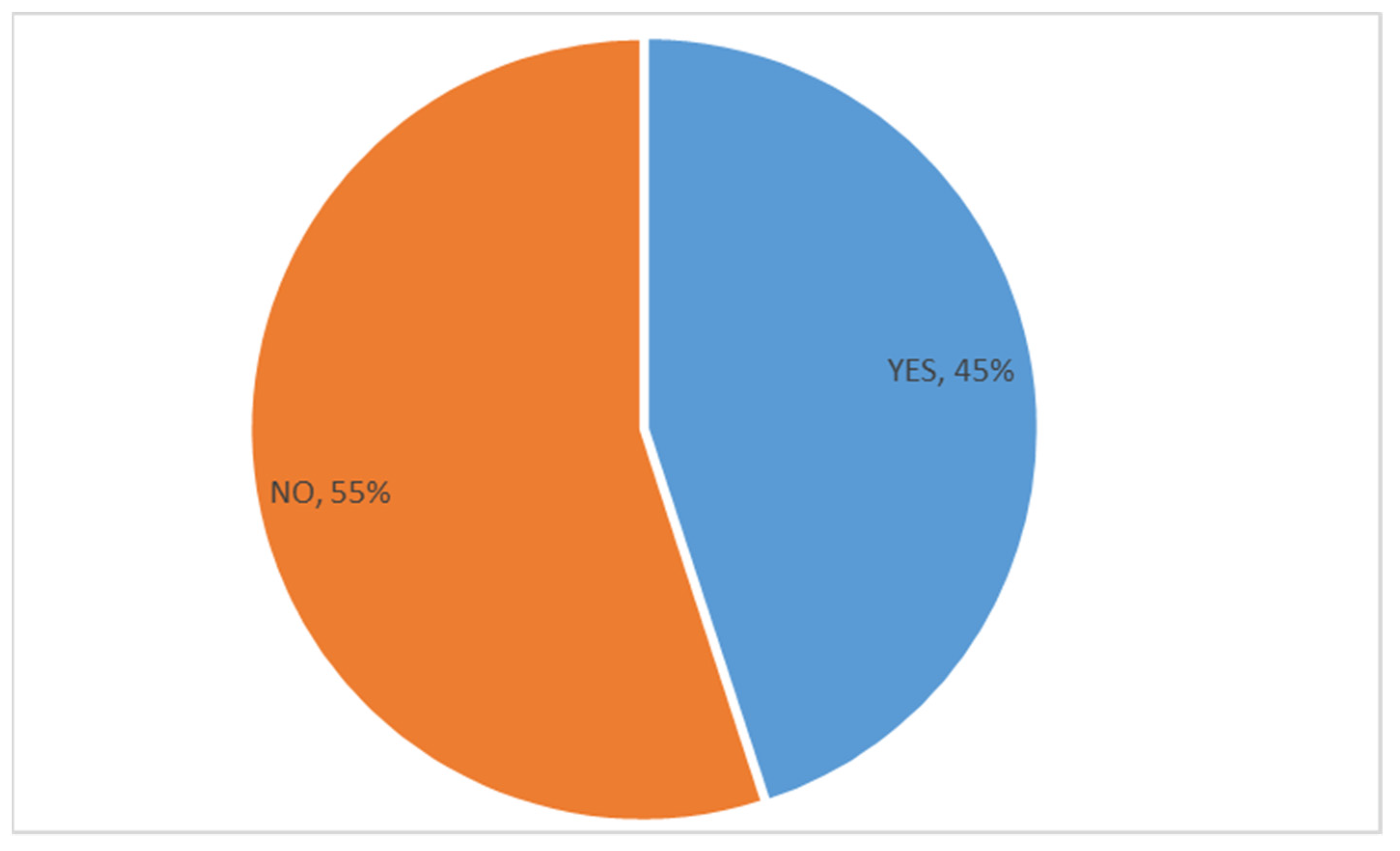
| Q7. Do you feel that a regulatory compliance or regulated environment/culture stifles continuous improvement programs in your organization? Yes or No. |
| Q8. Why do you feel that a regulatory environment can stifle CI? Tick all that apply. |
|
|
|
|
|
|
|
|
|
|
|
|
| Q9. What are the internal drivers of CI in your organisation? (Likert scale) |
|
|
|
|
|
|
| Q10. Please tick what you think are the top 5 benefits of CI to your organization? Tick 5 of the benefits listed. |
| Q11. Please tick what you think are the top 5 Critical Failure Factors (CFFs) to the use of CI methodologies in your organization? (pick from list) |
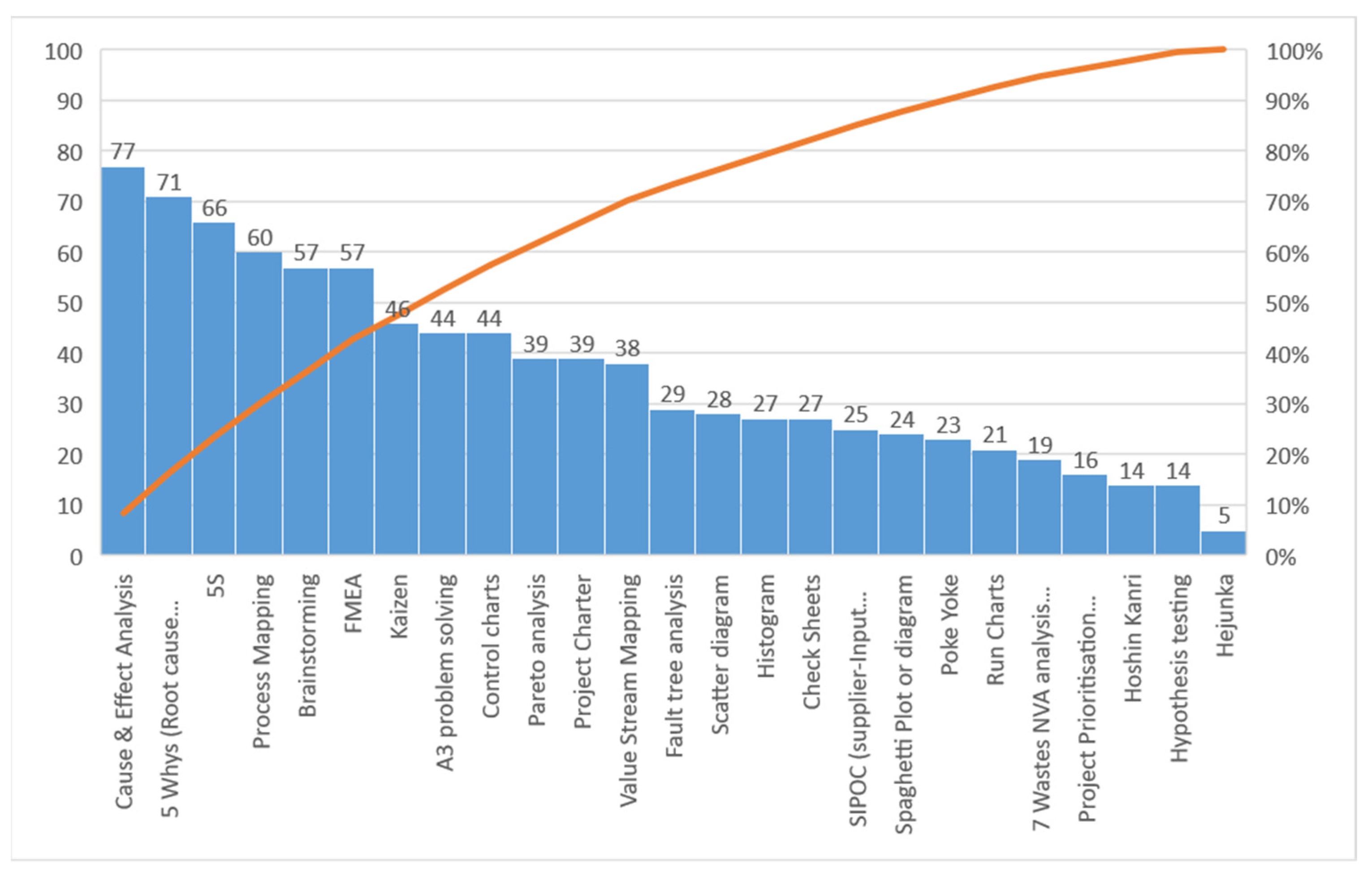
| Q12. Which of the following tools have you utilised in your current organization as part of CI initiatives or are you aware of as being utilised? (Please tick all from the list that applies to your organisation) |
| Q13. Which quality system or quality standard do you adhere to in your organization? Tick all that apply if known. |
References
- IDA Bio-Pharmaceuticals & Biotechnology Ireland. Available online: https://www.idaireland.com/doing-business-here/industry-sectors/bio-pharmaceuticals (accessed on 14 November 2021).
- Irish Pharmaceutical Heathcare Association Contribution to the Irish Economy. Available online: https://www.ipha.ie/about-the-industry/contribution-to-the-irish-economy/ (accessed on 14 November 2021).
- BioPharmaChem Ireland A Strategy for BioPharmaChem Manufacturing in Ireland 2019–2023. Available online: https://www.ibec.ie/influencing-for-business?ppc_keyword=ibec&gclid=Cj0KCQiAhMOMBhDhARIsAPVml-Et-psaCH1IzFpt3Hu8At3XK4HeMiK-t3RvTH55HzZbE-XbfRNShY4aApciEALw_wcB (accessed on 14 November 2021).
- Draguet, V. A Pharmaceutical Strategy for Europe. Available online: https://ec.europa.eu/health/human-use/strategy_en (accessed on 17 November 2021).
- Burke-Kennedy, E. Irish Exports Hit Record €15.7bn in March as Demand for Medicines Surges. Available online: https://www.irishtimes.com/business/economy/irish-exports-hit-record-15-7bn-in-march-as-demand-for-medicines-surges-1.4254319 (accessed on 14 November 2021).
- Purnhagen, K.P. The Challenges of Globalization in Pharmaceutical Law--Is an International Drug Approval System Modeled after the European System Worth Considering? Food Drug Law J. 2008, 63, 623–645. [Google Scholar]
- Bilanin, M.; Ahern, S.; Colao, M.; Campa, C.; Geldhof, G. ICH Q12 Implementation from an Industry Perspective. La Vague 2017. Available online: https://www.a3p.org/en/ich-q12-implementation/ (accessed on 18 November 2021).
- Lee, J. What Is Past Is Prologue: The International Conference on Harmonization and Lessons Learned from European Drug Regulations Harmonization. Univ. Pa. J. Int. Law 2005, 26, 151. [Google Scholar]
- Nenni, M.E.; Giustiniano, L.; Pirolo, L. Improvement of Manufacturing Operations through a Lean Management Approach: A Case Study in the Pharmaceutical Industry. Int. J. Eng. Bus. Manag. 2014, 6, 24. [Google Scholar] [CrossRef]
- Boccardelli, P.; Grandi, A.; Magnusson, M.; Oriani, R. The Value of Managerial Learning in R&D. In Strategy in Transition; Wiley: Hoboken, NJ, USA, 2009. [Google Scholar]
- Dale, B.G. Sustaining a Process of Continuous Improvement: Definition and Key Factors. TQM Mag. 1996, 8, 49–51. [Google Scholar] [CrossRef]
- Gonzalez, R.V.D.; Martins, M.F. Capability for Continuous Improvement: Analysis of Companies from Automotive and Capital Goods Industries. TQM J. 2016, 28, 250–274. [Google Scholar] [CrossRef]
- Byrne, B.; McDermott, O.; Noonan, J. Applying Lean Six Sigma Methodology to a Pharmaceutical Manufacturing Facility: A Case Study. Processes 2021, 9, 550. [Google Scholar] [CrossRef]
- Chowdary, B.V.; George, D. Improvement of Manufacturing Operations at a Pharmaceutical Company. J. Manuf. Technol. Manag. 2012, 23, 56–75. [Google Scholar] [CrossRef]
- Nicholas, J. Line Balancing Manual Assembly Processes Using a Kaizen Blitz Approach in a Highly Regulated Industry. 2019, Volume 2. Available online: https://books.google.co.jp/books?hl=zh-CN&lr=&id=mZgEBdQhjAAC&oi=fnd&pg=PR9&dq=Line+Balancing+Manual+Assembly+Processes+Using+a+Kaizen+Blitz+Approach+in+a+Highly+Regulated+Industry&ots=91xuIamUHQ&sig=8IPDJsssJPvLy-j-VX-J_QHxkqc&redir_esc=y#v=onepage&q&f=false (accessed on 18 November 2021).
- Vetalice, J.A. Review of Study Results: FDA Impact on U.S. Medical Technology Innovation-BONEZONE. Available online: https://bonezonepub.com/2010/12/31/review-of-study-results-fda-impact-on-us-medical-technology-innovation/ (accessed on 30 June 2021).
- Sreedharan, V.R.; Sunder, M.V. Critical Success Factors of TQM, Six Sigma, Lean and Lean Six Sigma: A Literature Review and Key Findings. Benchmarking Int. J. 2018, 25, 3479–3504. [Google Scholar] [CrossRef]
- Pavlović, K.; Božanić, V. Lean and Six Sigma Concepts: Application in Pharmaceutical Industry. Int. J. Qual. Res. 2012, 6, 23–28. [Google Scholar]
- Garza-Reyes, J.A.; Betsis, I.E.; Kumar, V.; Radwan Al-Shboul, M.A. Lean Readiness – the Case of the European Pharmaceutical Manufacturing Industry. Int. J. Product. Perform. Manag. 2018, 67, 20–44. [Google Scholar] [CrossRef]
- O’Rourke, D.; Greene, A. Lean Manufacturing Practice in a CGMP Environment. Pharm. Technol. Eur. 2006, 18, 33–40. [Google Scholar]
- Cavallaro, F.; Lugg-Widger, F.; Cannings-John, R.; Harron, K. Reducing Barriers to Data Access for Research in the Public Interest—Lessons from Covid-19. Available online: https://blogs.bmj.com/bmj/2020/07/06/reducing-barriers-to-data-access-for-research-in-the-public-interest-lessons-from-covid-19/ (accessed on 18 November 2021).
- Zollo, M.; Winter, S. Deliberate Learning and the Evolution of Dynamic Capabilities. Organ. Sci. 2002, 339–351. [Google Scholar] [CrossRef] [Green Version]
- Mauri, F.; Garetti, M.; Gandelli, A. A Structured Approach to Process Improvement in Manufacturing Systems. Prod. Plan. Control 2010, 21, 695–717. [Google Scholar] [CrossRef]
- What’s the Difference between Pharmaceutical and Biotechnology?|Morgan McKinley Recruitment. Available online: https://www.morganmckinley.com/ie/article/difference-between-pharmaceutical-and-biotechnology (accessed on 14 November 2021).
- Alqahtani, S.; Seoane-Vazquez, E.; Rodriguez-Monguio, R.; Eguale, T. Priority Review Drugs Approved by the FDA and the EMA: Time for International Regulatory Harmonization of Pharmaceuticals? Pharmacoepidemiol. Drug Saf. 2015, 24, 709–715. [Google Scholar] [CrossRef] [PubMed]
- HPRA Quality Defects. Available online: http://www.hpra.ie/homepage/medicines/quality-information/quality-defects (accessed on 17 November 2021).
- Allison, G.; Cain, Y.T.; Cooney, C.; Garcia, T.; Bizjak, T.G.; Holte, O.; Jagota, N.; Komas, B.; Korakianiti, E.; Kourti, D.; et al. Regulatory and Quality Considerations for Continuous Manufacturing. May 20–21, 2014 Continuous Manufacturing Symposium. J. Pharm. Sci. 2015, 104, 803–812. [Google Scholar] [CrossRef]
- Witcher, M. Integrating Development Tools into the Process Validation Lifecycle to Achieve Six Sigma Pharmaceutical Quality. Bioprocess. J. 2018, 17, 1–11. [Google Scholar] [CrossRef]
- FDA Guidance for Industry: CMC Postapproval Manufacturing Changes to Be Documented in Annual Reports; FDA: Silver Spring, MD, USA, 2014; Volume 16.
- Miglani, A.; Saini, C.; Musyuni, P.; Aggarwal, G. A Review and Analysis of Product Recall for Pharmaceutical Drug Product. J. Generic Med. 2021, 17411343211033887. [Google Scholar] [CrossRef]
- Bloomberg J&J Sees ‘Significant Costs’ in 2011 to Fix Recalls-Bloomberg. Available online: https://www.bloomberg.com/news/articles/2011-01-25/j-j-profit-declines-12-on-product-recalls-2011-outlook-trails-forecast (accessed on 18 November 2021).
- Hall, K.; Stewart, T.; Chang, J.; Freeman, M.K. Characteristics of FDA Drug Recalls: A 30-Month Analysis. Am. J. Health-Syst. Pharm. AJHP Off. J. Am. Soc. Health-Syst. Pharm. 2016, 73, 235–240. [Google Scholar] [CrossRef]
- Anonymous International Collaboration on GMP Inspections. Available online: https://www.ema.europa.eu/en/human-regulatory/research-development/compliance/good-manufacturing-practice/international-collaboration-gmp-inspections (accessed on 18 November 2021).
- FDA. Mutual Recognition Agreement (MRA); FDA: Silver Spring, MD, USA, 2021. [Google Scholar]
- Makuch, R.W.; Shi, R. Comparison of Drug Approvals in Europe Versus the United States: An Analysis of Discrepancies Between Drug Products Reviewed by EMA and FDA. Ther. Innov. Regul. Sci. 2014, 48, 362–366. [Google Scholar] [CrossRef] [PubMed]
- Makower, J.; Meer, A.; Denend, L. FDA Impact on US Medical Technology Innovation. 2010. Available online: http://www.medtecheurope.org/wp-content/uploads/2015/09/01112010_FDA-impact-on-US-medical-technology-innovation_Backgrounder.pdf (accessed on 18 November 2021).
- ICH ICH Official Web Site: ICH. Available online: https://ich.org/ (accessed on 18 November 2021).
- Škrnjug, I.; Uzeirbegović, S.; Romčević, M.L.; Tomić, S.; Meyer, H.; Conrad, C. Mutual Recognition in the European System: A Blueprint for Increasing Access to Medicines? Regul. Toxicol. Pharmacol. 2019, 106, 270–277. [Google Scholar] [CrossRef]
- ECA FDA Adopts ICH Q12-ECA Academy. Available online: https://www.gmp-compliance.org/gmp-news/fda-adopts-ich-q12 (accessed on 18 November 2021).
- FDA. International Regulatory Harmonization; FDA: Silver Spring, MD, USA, 2020. [Google Scholar]
- European Medicines Agency ICH Guideline Q10 on Pharmaceutical Quality System-Step 5. Available online: https://www.ema.europa.eu/en/ich-q10-pharmaceutical-quality-system (accessed on 18 November 2021).
- Boylan, B.; McDermott, O.; Kinahan, N.T. Manufacturing Control System Development for an In Vitro Diagnostic Product Platform. Processes 2021, 9, 975. [Google Scholar] [CrossRef]
- National Academies of Sciences, Engineering, and Medicine. Barriers to Innovations in Pharmaceutical Manufacturing: Proceedings of a Workshop–in Brief; The National Academies Press: Washington, DC, USA, 2020. [Google Scholar] [CrossRef]
- ICH ICH Q12 Technical and Regulatory Considerations for Pharmaceutical Product Lifecycle Management. Available online: https://www.ema.europa.eu/en/ich-q12-technical-regulatory-considerations-pharmaceutical-product-lifecycle-management (accessed on 18 November 2021).
- Chatterjee, B. Applying Lean Six Sigma in the Pharmaceutical Industry, 1st ed.; Routledge: London, UK, 2014. [Google Scholar]
- Antony, J.; Krishan, N.; Cullen, D.; Kumar, M. Lean Six Sigma for Higher Education Institutions (HEIs): Challenges, Barriers, Success Factors, Tools/Techniques. Int. J. Product. Perform. Manag. 2012, 61, 940–948. [Google Scholar] [CrossRef]
- Albliwi, S.; Antony, J.; Abdul Halim Lim, S.; van der Wiele, T. Critical Failure Factors of Lean Six Sigma: A Systematic Literature Review. Int. J. Qual. Reliab. Manag. 2014, 31, 1012–1030. [Google Scholar] [CrossRef]
- Full Article: Synergies between Critical Success Factors of Lean Six Sigma and Public Values. Available online: https://www-tandfonline-com.libgate.library.nuigalway.ie/doi/full/10.1080/14783363.2017.1383153 (accessed on 5 September 2021).
- Antony, J.; Snee, R.; Hoerl, R. Lean Six Sigma: Yesterday, Today and Tomorrow. Int. J. Qual. Reliab. Manag. 2017, 34, 1073–1093. [Google Scholar] [CrossRef]
- Barclay, R.C.; Cudney, E.A.; Shetty, S.; Antony, J. Determining Critical Success Factors for Lean Implementation. Total Qual. Manag. Bus. Excell. 2021, 1–15. [Google Scholar] [CrossRef]
- Ball, H.L. Conducting Online Surveys. J. Hum. Lact. Off. J. Int. Lact. Consult. Assoc. 2019, 35, 413–417. [Google Scholar] [CrossRef]
- Power, A. LinkedIn: Facebook for Professionals? Br. J. Midwifery 2015, 23, 196–198. [Google Scholar] [CrossRef]
- Easterby-Smith, M.; Thorpe, R.; Jackson, P.R. Management Research; SAGE: Newbury Park, CA, USA, 2012; ISBN 1-4462-6026-7. [Google Scholar]
- Quality Digest Magazine. Available online: https://www.qualitydigest.com/mar08/articles/05_article.shtml (accessed on 15 November 2021).
- Antony, J.; Gupta, S.; Sunder M., V.; Gijo, E.V. Ten Commandments of Lean Six Sigma: A Practitioners’ Perspective. Int. J. Product. Perform. Manag. 2018, 67, 1033–1044. [Google Scholar] [CrossRef]
- Wagner, K.; Schulze, U.; Farber, A. Lean Comes to Pharma. Pharm. Exec. 2009. Available online: www.Pharmexec.Com/Lean-Comes-Pharma-0 (accessed on 25 February 2016).
- Haigney, S. Responding to FDA CAPA Requests. Pharm. Technol. 2021, 45, 52–57. [Google Scholar]
- Schmitt, S. How A Team Led By Medtronic Quality Experts Plans To Stand Up To “A Monster Called CAPA”–And Make It “Cool”. Available online: https://medtech.pharmaintelligence.informa.com/MT124933/How-A-Team-Led-By-Medtronic-Quality-Experts-Plans-To-Stand-Up-To-A-Monster-Called-CAPA--And-Make-It-Cool (accessed on 15 August 2021).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Functional Areas of Respondents | % |
|---|---|
| Production/Operations | 24% |
| Manufacturing /Process Engineering | 14% |
| Operations Quality | 9% |
| Validation | 9% |
| QC Lab Role | 9% |
| Continuous Improvement | 8% |
| Supply Chain/Logistics | 8% |
| Project Management | 6% |
| Regulatory | 5% |
| Quality Systems | 5% |
| Warehouse/Shipping | 1% |
| Maintenance | 1% |
| Sales | 1% |
| R&D/Design | 0% |
| Complaints/Pharmacovigilance/Post Market surveillance | 0% |
| Supplier Quality | 0% |
| Technical Writer | 0% |
| HR | 0% |
| Quality System | % |
|---|---|
| 21 CFR 211 | 28% |
| ISO 9001:2015 | 25% |
| ICH Q10 Pharma Quality System | 25% |
| 21 CFR 210 | 10% |
| ICH Q7 (ICH GMP for API | 10% |
| Don’t know | 2% |
| High Driver | Driver | Moderate Driver | Low Driver | Does Not Drive a CI Focus Whatsoever | |
|---|---|---|---|---|---|
| Customer/Patient focus | 43% | 25% | 18% | 10% | 4% |
| Productivity | 59% | 33% | 11% | 0% | 0% |
| Quality | 55% | 28% | 16% | 1% | 3% |
| Regulatory | 28% | 35% | 28% | 11% | 14% |
| Financial | 43% | 25% | 26% | 8% | 3% |
| Safety | 43% | 31% | 15% | 6% | 4% |
| Benefits of CI | No. of Responses | % |
|---|---|---|
| Improved Productivity | 25% | |
| Improved product quality | 23% | |
| Achieving Cost Savings | 14% | |
| Enhanced Staff Efficiency | 8% | |
| Improved Speed/Timeliness | 6% | |
| Reduced defect rate in processes | 4% | |
| Increased Employee Engagement | 4% | |
| Improved Standardization of Processes/Procedures | 3% | |
| Improved Customer/Patient Safety | 3% | |
| Enhanced Customer/Patient Satisfaction | 3% | |
| Ensures Compliance | 3% | |
| Improved Employee Satisfaction and morale | 2% | |
| Improved Communication Between the Departments | 1% | |
| Increased Understanding of Customer Wants/Needs | 0.4% |
| Reasons for CI Barriers in Regulated Environments | Strongly Agree | Agree | Neither Agree Nor Disagree | Disagree | Strongly Disagree |
|---|---|---|---|---|---|
| Fear of extra validation activity | 44% | 31% | 19% | 6% | 0% |
| Compliance v’s Quality (closing issues/investigations within deadlines) | 31% | 39% | 25% | 6% | 0% |
| Regulatory Culture of being “safe.” | 42% | 47% | 6% | 6% | 0% |
| Overdependence on a Continuous Improvement owner/dept. to drive program | 22% | 36% | 22% | 17% | 3% |
| Changes seen as potentially affecting compliance to Regulations | 42% | 36% | 22% | 0% | 0% |
| Fear of extra regulatory submission workload | 42% | 31% | 19% | 6% | 3% |
| CI seen as a Quality dept initiative | 14% | 17% | 22% | 36% | 11% |
| Lack of training | 19% | 31% | 22% | 25% | 3% |
| CAPA seen as unwanted extra work | 14% | 42% | 14% | 25% | 6% |
| Regulatory department don’t see benefits. | 22% | 22% | 39% | 11% | 6% |
| Lack of management support | 19% | 25% | 28% | 22% | 6% |
| Heavy external audit schedule limits time for CI | 11% | 25% | 33% | 28% | 3% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McDermott, O.; Antony, J.; Sony, M.; Daly, S. Barriers and Enablers for Continuous Improvement Methodologies within the Irish Pharmaceutical Industry. Processes 2022, 10, 73. https://doi.org/10.3390/pr10010073
McDermott O, Antony J, Sony M, Daly S. Barriers and Enablers for Continuous Improvement Methodologies within the Irish Pharmaceutical Industry. Processes. 2022; 10(1):73. https://doi.org/10.3390/pr10010073
Chicago/Turabian StyleMcDermott, Olivia, Jiju Antony, Michael Sony, and Stephen Daly. 2022. "Barriers and Enablers for Continuous Improvement Methodologies within the Irish Pharmaceutical Industry" Processes 10, no. 1: 73. https://doi.org/10.3390/pr10010073
APA StyleMcDermott, O., Antony, J., Sony, M., & Daly, S. (2022). Barriers and Enablers for Continuous Improvement Methodologies within the Irish Pharmaceutical Industry. Processes, 10(1), 73. https://doi.org/10.3390/pr10010073