

Long-Term Skin Safety Effect of Chlorine-Rich Water Treatment on C57BL/6 Mice

 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animal Groupings and Water Supplementation
2.2. Water Preparation and Their Properties
2.3. Serum and Skin Sample Preparation
2.4. Histological Examination by Hematoxylin and Eosin (H&E) Staining
2.5. Skin Parameters Measurement
2.6. Total Reactive Oxygen Species (ROS) Detection
2.7. Nitric Oxide (NO) Assay
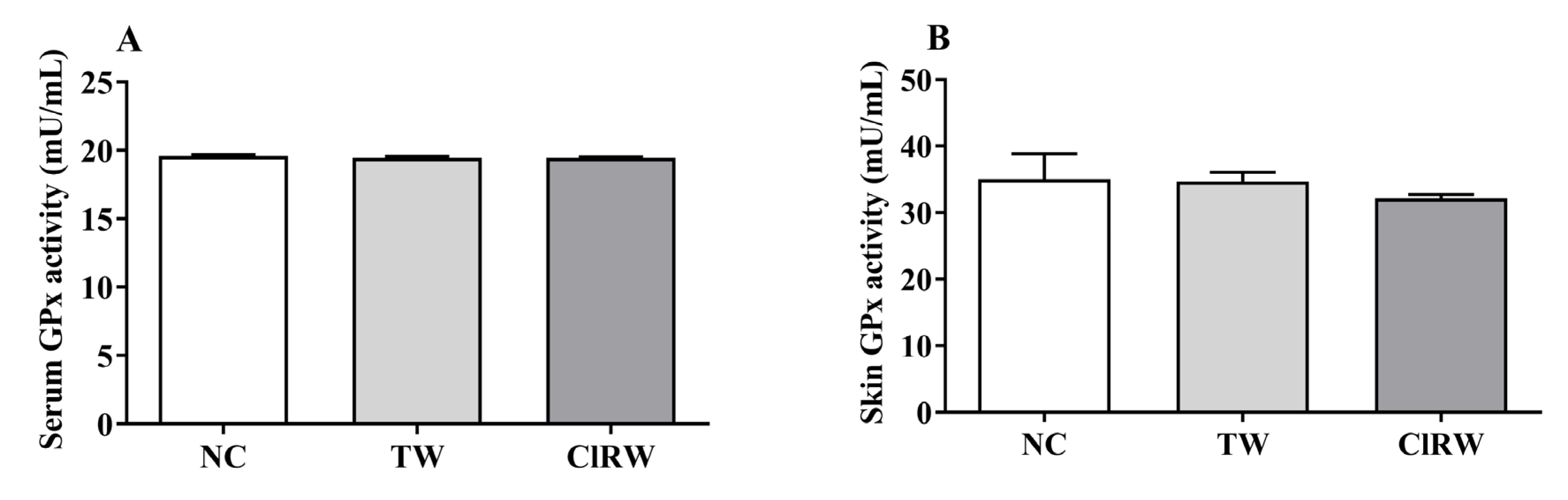
2.8. Measurement of Antioxidant Enzyme Activities
2.9. Cytokine Analysis
2.10. White Blood Cell (WBC) and its Differential Count Analysis
2.11. Statistical Analysis
3. Results
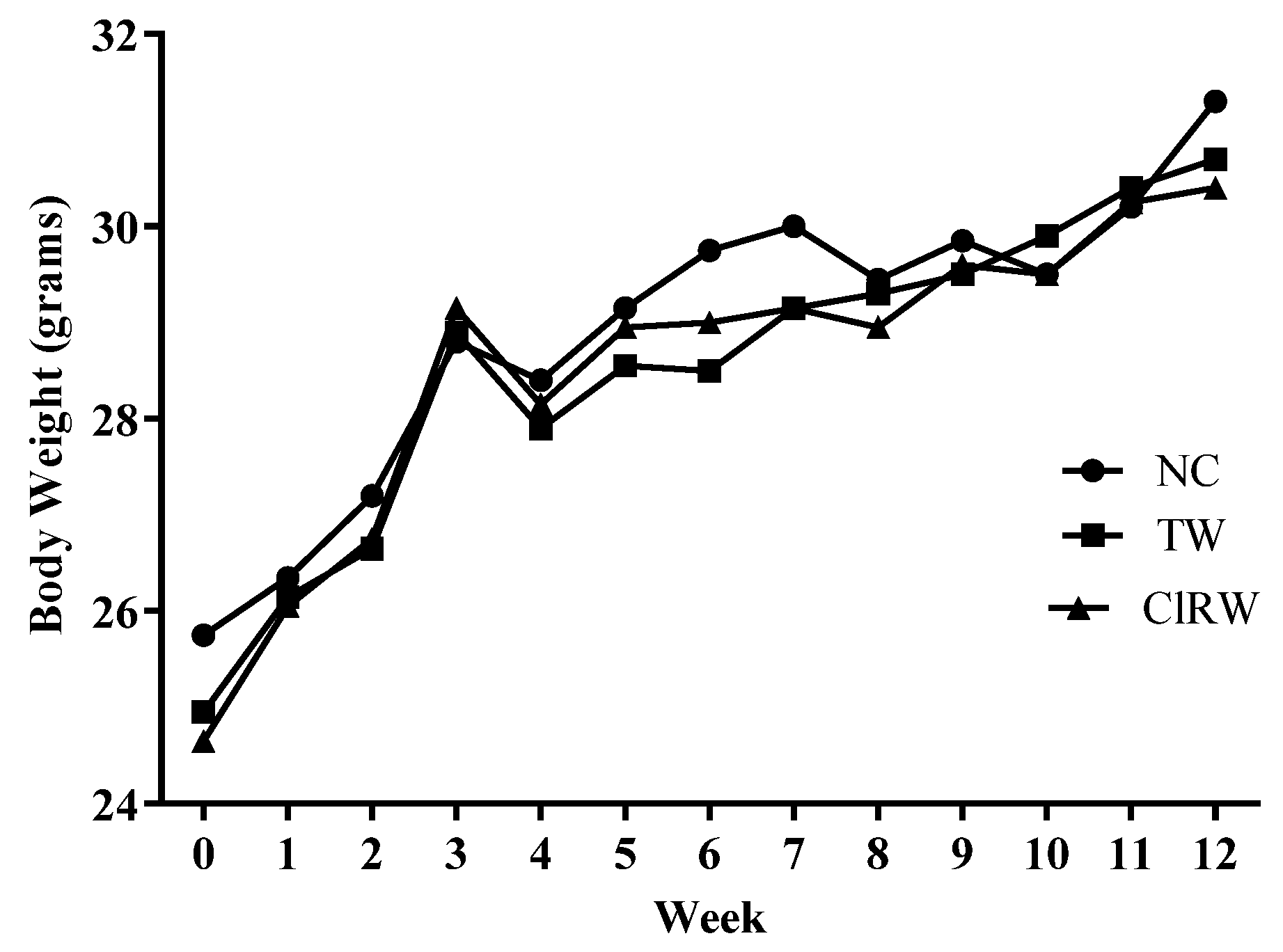
3.1. Effects of Chlorine-Rich Sterilized Water (ClRW) on Body Weight Measurements
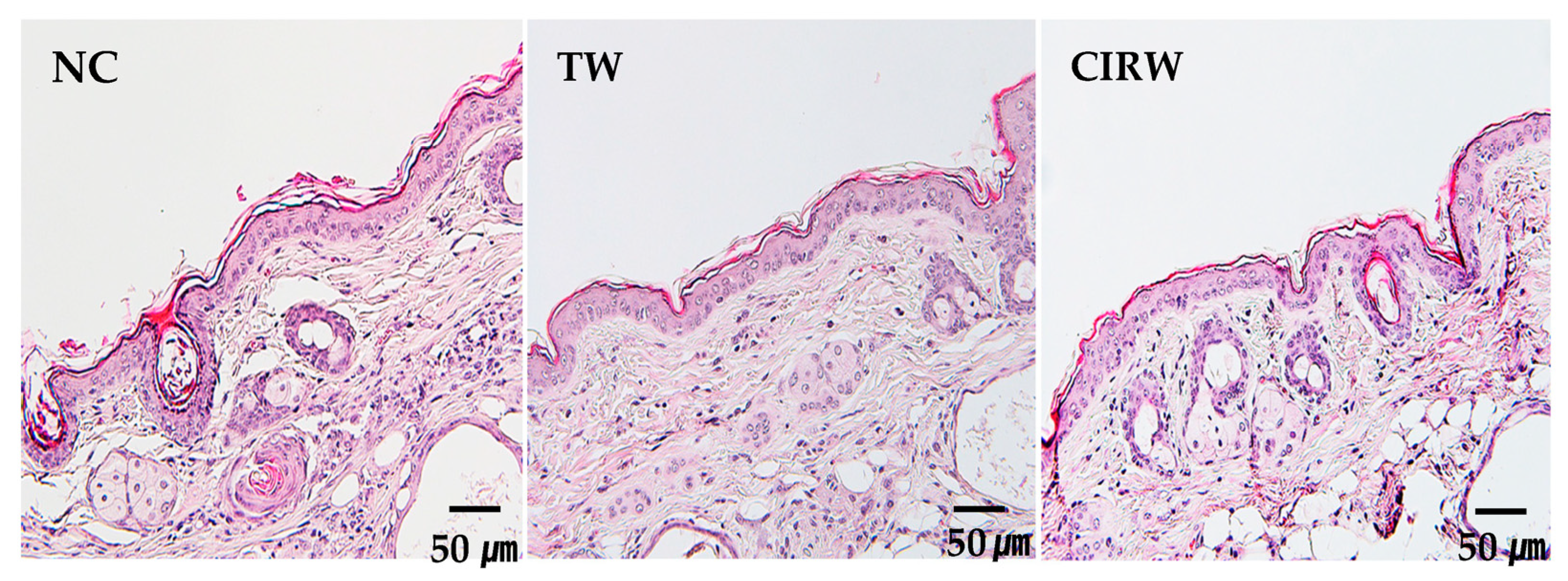
3.2. Effects of ClRW on Skin Histological Analysis
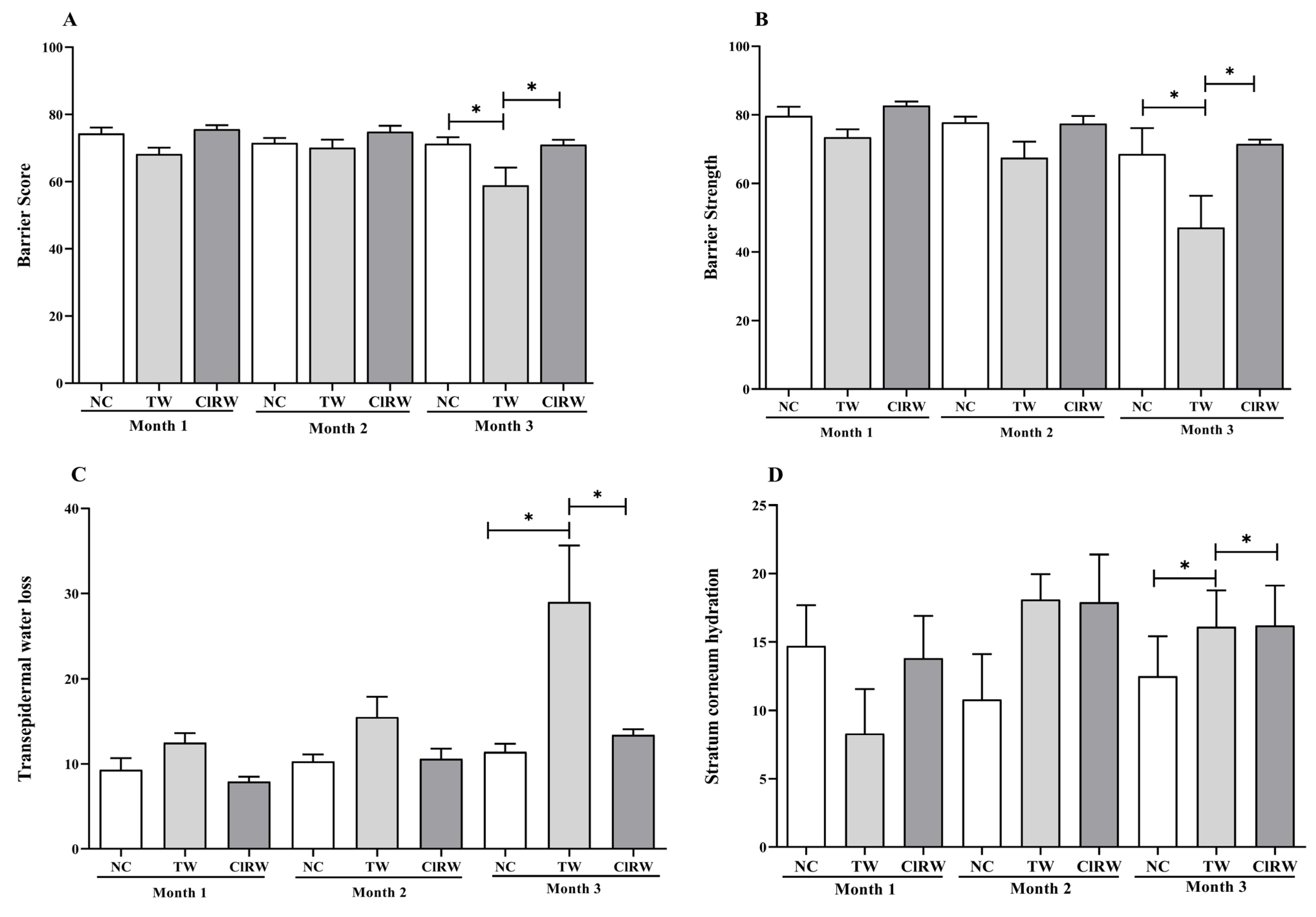
3.3. Effect of ClRW on Skin Parameters
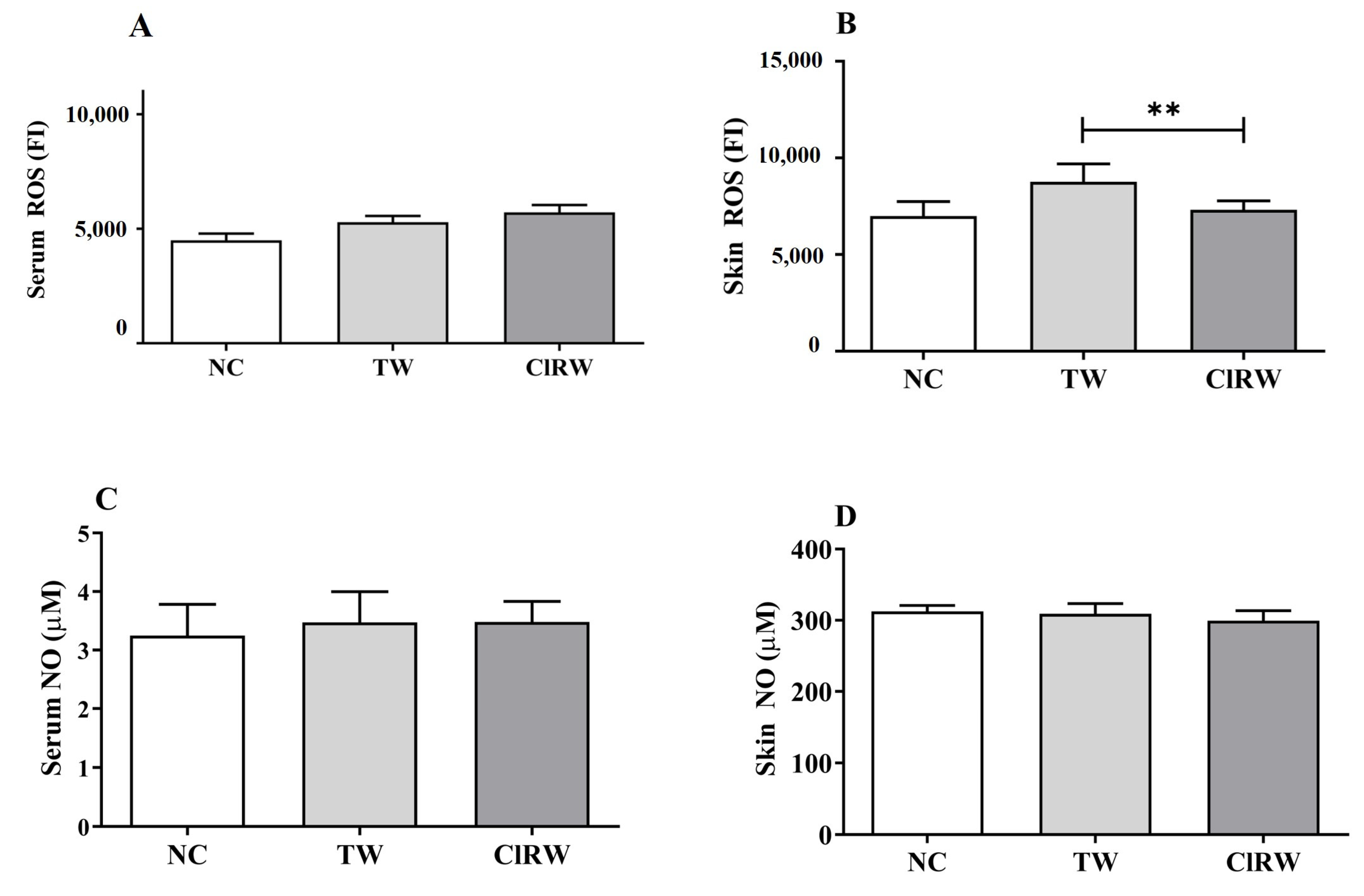
3.4. Effects of Chlorine-Rich Sterilized Water on Oxidative Stress Response
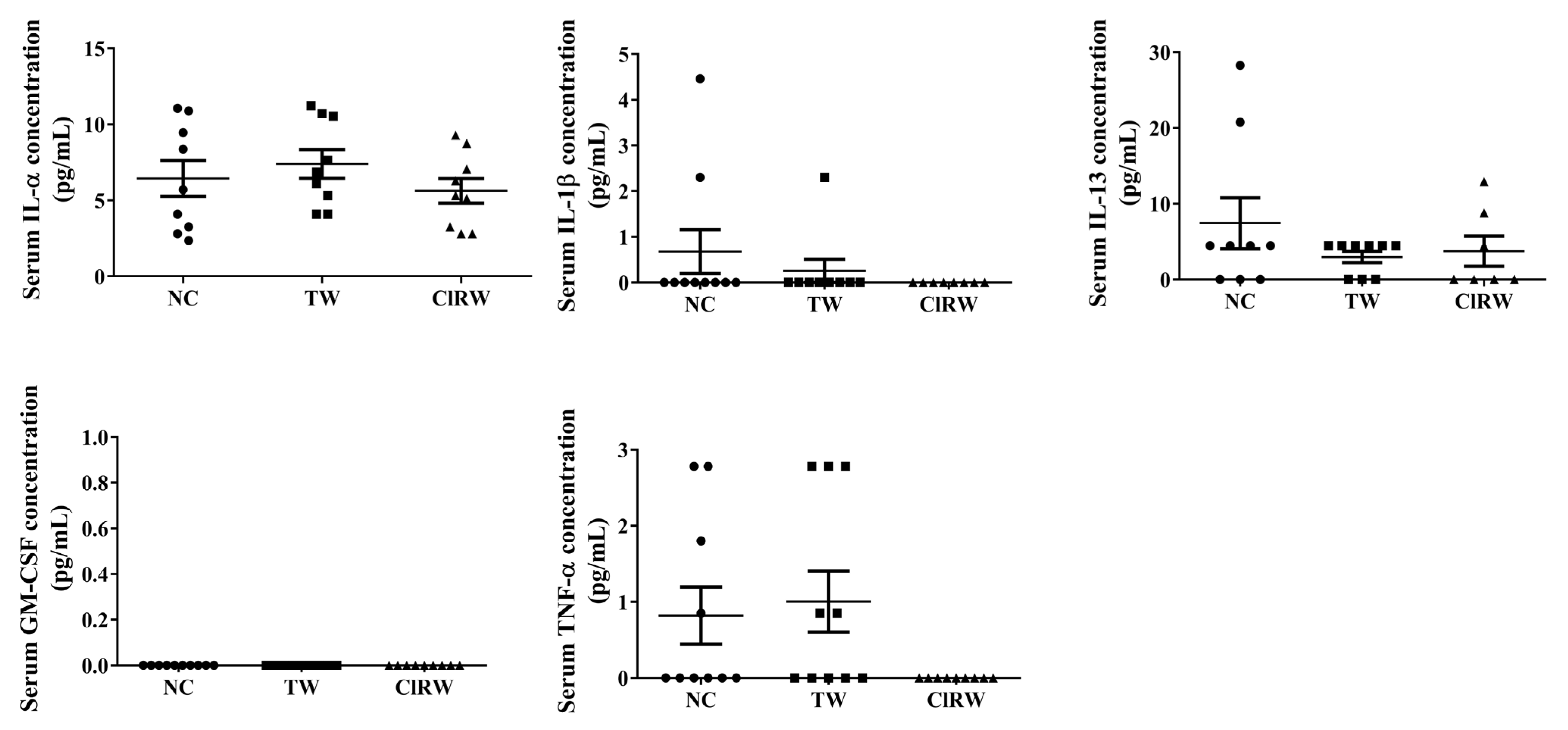
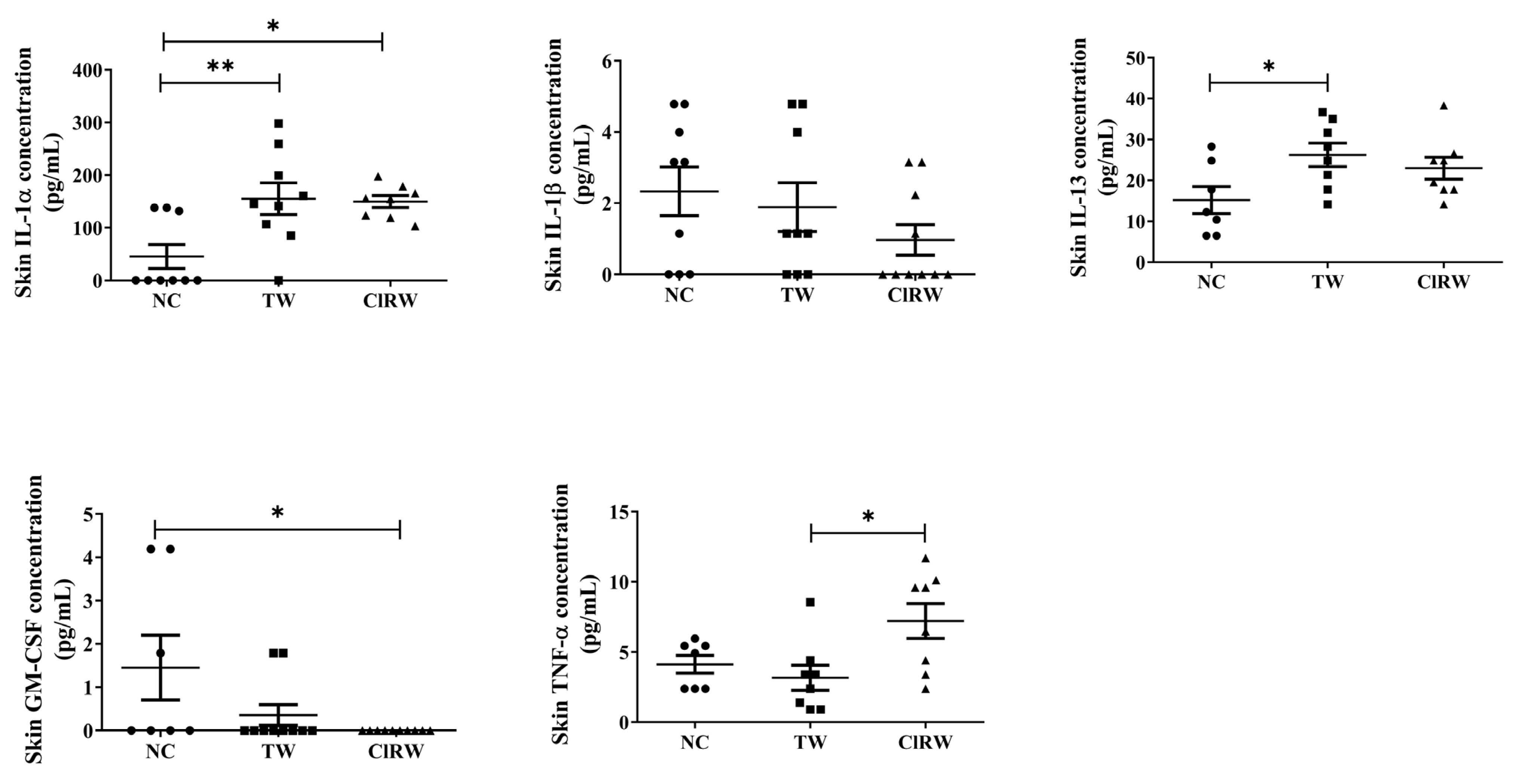
3.5. Effects of Chlorine-Rich Sterilized Water (ClRW) on Inflammatory Response
3.6. Effects of Chlorine-Rich Sterilized Water (ClRW) on Allergic Response
3.7. Effects of Chlorine Rich Sterilized Water (ClRW) on WBC Count
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Gorzelanny, C.; Mess, C.; Schneider, S.W.; Huck, V.; Brandner, J.M. Skin barriers in dermal drug delivery: Which barriers have to be overcome and how can we measure them? Pharmaceutics 2020, 12, 684. [Google Scholar] [CrossRef]
- Johansson, B. Functional water-in promotion of health beneficial effects and prevention of disease. Intern. Med. Rev. 2016, 3. [Google Scholar] [CrossRef]
- Iram, A.; Wang, X.; Demirci, A. Electrolyzed oxidizing water and its applications as sanitation and cleaning agent. Food Eng. Rev. 2021, 13, 411–427. [Google Scholar] [CrossRef]
- Kawada, J.; Yamada, H.; Matsuba, Y.; Ogawa, H. Effectiveness of Hand-washing Using Acidic Electrolyzed Water-A Comparative Study of Weak Acidic Electrolyzed Water, Strong Acidic Electrolyzed Water and Tap Water. Ski. Res. 2000, 42, 137–142. [Google Scholar]
- Vorobjeva, N.V.; Vorobjeva, L.I.; Khodjaev, E.Y. The bactericidal effects of electrolyzed oxidizing water on bacterial strains involved in hospital infections. Artif. Organs 2004, 28, 590–592. [Google Scholar] [CrossRef]
- Lee, J.H.; Rhee, P.L.; Kim, J.H.; Kim, J.J.; Paik, S.W.; Rhee, J.C.; SONG, J.H.; Yeom, J.S.; Lee, N.Y. Efficacy of electrolyzed acid water in reprocessing patient-used flexible upper endoscopes: Comparison with 2% alkaline glutaraldehyde. J. Gastroenterol. Hepatol. 2004, 19, 897–903. [Google Scholar] [CrossRef]
- Williams, J.; Rasmussen, E.; Robins, L.; Nguyen, U. Hypochlorous Acid: Harnessing an Innate Response. Infect. Prev. Strategy (TIPS) 2017, 1–9. [Google Scholar]
- Rahman, M.H.; Bajgai, J.; Cho, Y.; Fadriquela, A.; Sharma, S.; Thuy, T.T.; Cho, S.H.; Jeong, Y.J.; Goh, S.H.; Kim, Y. Immune Redox Modulation Effects of Non-Electrolyzed Hypochlorous Acid Water on Helicobacter pylori-Infected C57BL/6 Mouse Model. Processes 2023, 11, 1474. [Google Scholar] [CrossRef]
- Pan, G.J.; Rayner, B.S.; Zhang, Y.; van Reyk, D.M.; Hawkins, C.L. A pivotal role for NF-κB in the macrophage inflammatory response to the myeloperoxidase oxidant hypothiocyanous acid. Arch. Biochem. Biophys. 2018, 642, 23–30. [Google Scholar] [CrossRef] [Green Version]
- Leung, T.H.; Zhang, L.F.; Wang, J.; Ning, S.; Knox, S.J.; Kim, S.K. Topical hypochlorite ameliorates NF-κB–mediated skin diseases in mice. J. Clin. Investig. 2013, 123, 5361–5370. [Google Scholar] [CrossRef] [Green Version]
- Andrés, C.M.C.; Pérez de la Lastra, J.M.; Juan, C.A.; Plou, F.J.; Pérez-Lebeña, E. Hypochlorous Acid Chemistry in Mammalian Cells—Influence on Infection and Role in Various Pathologies. Int. J. Mol. Sci. 2022, 23, 10735. [Google Scholar] [CrossRef]
- Bauer, G. HOCl and the control of oncogenesis. J. Inorg. Biochem. 2018, 179, 10–23. [Google Scholar] [CrossRef] [PubMed]
- Water, S.; Organization, W.H. Guidelines for Safe Recreational Water Environments. In Swimming Pools and Similar Environments; World Health Organization: Geneva, Switzerland, 2006; Volume 2. [Google Scholar]
- Prest, E.I.; Hammes, F.; Van Loosdrecht, M.C.; Vrouwenvelder, J.S. Biological stability of drinking water: Controlling factors, methods, and challenges. Front. Microbiol. 2016, 7, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeong, E.-S.; Bajgai, J.; You, I.-S.; Rahman, M.; Fadriquela, A.; Sharma, S.; Kwon, H.-U.; Lee, S.-Y.; Kim, C.-S.; Lee, K.-J. Therapeutic effects of hydrogen gas inhalation on trimethyltin-induced neurotoxicity and cognitive impairment in the C57BL/6 mice model. Int. J. Mol. Sci. 2021, 22, 13313. [Google Scholar] [CrossRef] [PubMed]
- Oyinloye, B.; Adenowo, A.; Kappo, A. Reactive oxygen species, apoptosis, antimicrobial peptides and human inflammatory diseases. Pharmaceuticals 2015, 8, 151–175. [Google Scholar] [CrossRef] [Green Version]
- Fukuyama, T.; Martel, B.; Linder, K.; Ehling, S.; Ganchingco, J.; Bäumer, W. Hypochlorous acid is antipruritic and anti-inflammatory in a mouse model of atopic dermatitis. Clin. Exp. Allergy 2018, 48, 78–88. [Google Scholar] [CrossRef]
- Sam, C.-H.; Lu, H.-K. The role of hypochlorous acid as one of the reactive oxygen species in periodontal disease. J. Dent. Sci. 2009, 4, 45–54. [Google Scholar] [CrossRef] [Green Version]
- Luiking, Y.C.; Engelen, M.P.; Deutz, N.E. Regulation of nitric oxide production in health and disease. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masaki, H. Role of antioxidants in the skin: Anti-aging effects. J. Dermatol. Sci. 2010, 58, 85–90. [Google Scholar] [CrossRef]
- Pham-Huy, L.A.; He, H.; Pham-Huy, C. Free radicals, antioxidants in disease and health. Int. J. Biomed. Sci. 2008, 4, 89. [Google Scholar]
- Pasparakis, M.; Haase, I.; Nestle, F.O. Mechanisms regulating skin immunity and inflammation. Nat. Rev. Immunol. 2014, 14, 289. [Google Scholar] [CrossRef]
- Edmiston, C.E.; McBain, A.; Kiernan, M.; Leaper, D. A narrative review of microbial biofilm in postoperative surgical site infections: Clinical presentation and treatment. J. Wound Care 2016, 25, 693–702. [Google Scholar] [CrossRef]
- Iskandar, K.; Sartelli, M.; Tabbal, M.; Ansaloni, L.; Baiocchi, G.L.; Catena, F.; Coccolini, F.; Haque, M.; Labricciosa, F.M.; Moghabghab, A. Highlighting the gaps in quantifying the economic burden of surgical site infections associated with antimicrobial-resistant bacteria. World J. Emerg. Surg. 2019, 14, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Stevens, D.L. Treatments for skin and soft-tissue and surgical site infections due to MDR Gram-positive bacteria. J. Infect. 2009, 59, S32–S39. [Google Scholar] [CrossRef]
- Gomila, A.; Carratalà, J.; Badia, J.M.; Camprubí, D.; Piriz, M.; Shaw, E.; Diaz-Brito, V.; Espejo, E.; Nicolas, C.; Brugués, M. Preoperative oral antibiotic prophylaxis reduces Pseudomonas aeruginosa surgical site infections after elective colorectal surgery: A multicenter prospective cohort study. BMC Infect. Dis. 2018, 18, 1–9. [Google Scholar] [CrossRef]
- da Cruz Nizer, W.S.; Inkovskiy, V.; Overhage, J. Surviving reactive chlorine stress: Responses of gram-negative bacteria to hypochlorous acid. Microorganisms 2020, 8, 1220. [Google Scholar] [CrossRef]
- Memar, M.Y.; Ghotaslou, R.; Samiei, M.; Adibkia, K. Antimicrobial use of reactive oxygen therapy: Current insights. Infect. Drug Resist. 2018, 11, 567. [Google Scholar] [CrossRef] [Green Version]
- Dainichi, T.; Hanakawa, S.; Kabashima, K. Classification of inflammatory skin diseases: A proposal based on the disorders of the three-layered defense systems, barrier, innate immunity and acquired immunity. J. Dermatol. Sci. 2014, 76, 81–89. [Google Scholar] [CrossRef] [Green Version]
- Enk, A.H.; Angeloni, V.; Udey, M.; Katz, S. An essential role for Langerhans cell-derived IL-1 beta in the initiation of primary immune responses in skin. J. Immunol. 1993, 150, 3698–3704. [Google Scholar] [CrossRef] [PubMed]
- Arango Duque, G.; Descoteaux, A. Macrophage cytokines: Involvement in immunity and infectious diseases. Front. Immunol. 2014, 5, 491. [Google Scholar] [CrossRef] [Green Version]
- Kidd, P. Th1/Th2 balance: The hypothesis, its limitations, and implications for health and disease. Altern. Med. Rev. 2003, 8, 223–246. [Google Scholar]
- Ren, A.; Liu, R.; Miao, Z.G.; Zhang, X.; Cao, P.F.; Chen, T.X.; Li, C.Y.; Shi, L.; Jiang, A.L.; Zhao, M.W. Hydrogen-rich water regulates effects of ROS balance on morphology, growth and secondary metabolism via glutathione peroxidase in Ganoderma lucidum. Environ. Microbiol. 2017, 19, 566–583. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Before | After | |
|---|---|---|
| Temp. | 21.4 | 21.3 |
| pH | 7.75 | 7.11 |
| ORP | 500 mV | 450 mV |
| ACC | 0.7 ppm | 5.0 ppm |
| H2 | 36 ppm | 235 ppm |
| Serum and Skin Count (pg/mL) | NC | TW | ClRW |
|---|---|---|---|
| Serum IL-2 | 2.97 ± 0.98 | 2.72 ± 0.65 | 2.82 ± 0.42 |
| Serum IL-4 | 2.12 ± 1.56 | 1.02 ± 0.59 | 0.99 ± 1.56 * |
| Serum IL-5 | 2.60 ± 0.71 | 2.09 ± 0.62 | 1.65 ± 0.53 * |
| Serum IL-6 | 2.83 ± 0.47 | 2.14 ± 0.60 | 1.83 ± 0.50 |
| Serum IL-10 | 12.27 ± 9.24 | 0.70 ± 1.73 | 0.11 ± 0.23 * |
| Serum IL-12 | 78.22 ± 21.64 | 57.06 ± 13.88 | 43.52 ± 18.69 * |
| Skin IL-2 | 1.24 ± 0.95 | 2.04 ± 1.07 | 1.95 ± 0.97 |
| Skin IL-4 | 0.00 ± 0.00 | 0.00 ± 0.00 | 0.00 ± 0.00 |
| Skin IL-5 | 0.00 ± 0.00 | 0.00 ± 0.00 | 0.10 ± 0.10 |
| Skin IL-6 | 0.70 ± 0.12 | 0.64 ± 0.16 | 0.76 ± 0.12 |
| Skin IL-10 | 0.00 ± 0.00 | 0.00 ± 0.00 | 0.00 ± 0.00 |
| Skin IL-12 | 6.20 ± 2.04 | 6.08 ± 2.03 | 7.05 ± 2.99 |
| WBC Count (K/μL) | NC | TW | ClRW |
|---|---|---|---|
| Total WBC | 5.94 ± 1.24 | 6.29 ± 1.17 | 7.15 ± 1.31 * |
| Neutrophils | 1.67 ± 0.30 | 1.83 ± 0.34 | 1.93 ± 036 |
| Lymphocytes | 4.15 ±1.00 | 4.23 ± 1.02 | 5.04 ± 1.00 * |
| Monocytes | 0.11 ± 0.05 | 0.20 ± 0.15 | 0.16 ± 0.11 |
| Eosinophils | 0.02 ± 0.01 | 0.01 ± 0.01 | 0.01 ± 0.008 |
| Basophils | 0.002 ± 0.00 | 0.005 ± 0.005 | 0.006 ± 0.006 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rahman, M.H.; Fadriquela, A.; Bajgai, J.; Hoon, G.S.; Hyun, C.S.; Kim, C.-S.; Lee, K.-J. Long-Term Skin Safety Effect of Chlorine-Rich Water Treatment on C57BL/6 Mice. Processes 2023, 11, 1914. https://doi.org/10.3390/pr11071914
Rahman MH, Fadriquela A, Bajgai J, Hoon GS, Hyun CS, Kim C-S, Lee K-J. Long-Term Skin Safety Effect of Chlorine-Rich Water Treatment on C57BL/6 Mice. Processes. 2023; 11(7):1914. https://doi.org/10.3390/pr11071914
Chicago/Turabian StyleRahman, Md. Habibur, Ailyn Fadriquela, Johny Bajgai, Goh Seong Hoon, Cho Syung Hyun, Cheol-Su Kim, and Kyu-Jae Lee. 2023. "Long-Term Skin Safety Effect of Chlorine-Rich Water Treatment on C57BL/6 Mice" Processes 11, no. 7: 1914. https://doi.org/10.3390/pr11071914
APA StyleRahman, M. H., Fadriquela, A., Bajgai, J., Hoon, G. S., Hyun, C. S., Kim, C. -S., & Lee, K. -J. (2023). Long-Term Skin Safety Effect of Chlorine-Rich Water Treatment on C57BL/6 Mice. Processes, 11(7), 1914. https://doi.org/10.3390/pr11071914