

Transdermal Patches Containing Opioids in the Treatment of Patients with Chronic Pain


Abstract
:1. Introduction
- Mild pain can be treated with non-steroidal anti-inflammatory drugs (NSAIDs) or non-opioid analgesics such as acetaminophen or paracetamol and/or adjuvants such as antidepressants or anticonvulsants;
- Moderate pain requires the use of weak opioid analgesics, such as codeine, dihydrocodeine, tramadol, and/or adjuvants;
2. Transdermal Drug Delivery
2.1. Fentanyl
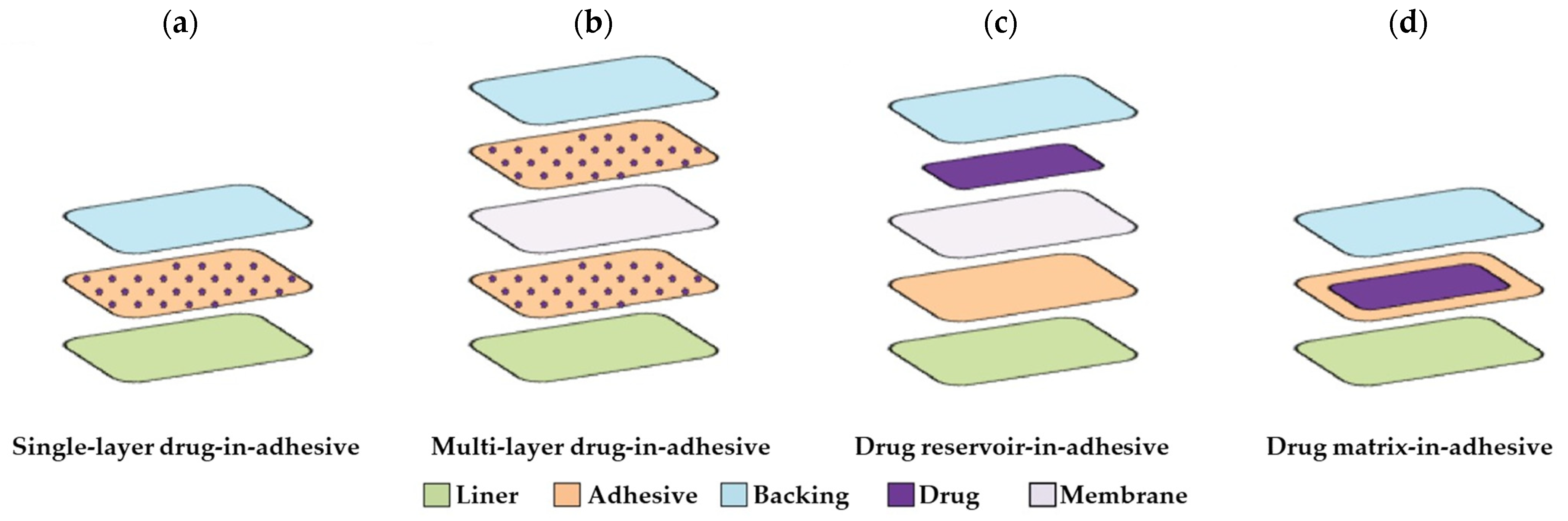
- In the case of reservoir formulations, the drug release rate from the reservoir layer is dependent on the choice of polymer and membrane layer thickness;
- In drug-in-adhesive systems and matrix patches, the control of the drug administered is diffusive, and the amount dispensed is directly proportional to the surface of the patch in contact with the skin.
2.2. Buprenorphine
3. Conclusions and Perspectives
Funding
Data Availability Statement
Conflicts of Interest
References
- Raja, S.N.; Carr, D.B.; Cohen, M.; Finnerup, N.B.; Flor, H.; Gibson, S.; Keefe, F.J.; Mogil, J.S.; Ringkamp, M.; Sluka, K.A.; et al. The revised International Association for the Study of Pain definition of pain: Concepts, challenges, and compromises. Pain 2020, 161, 1976–1982. [Google Scholar] [CrossRef] [PubMed]
- Leppert, W.; Malec-Milewska, M.; Zajaczkowska, R.; Wordliczek, J. Transdermal and Topical Drug Administration in the Treatment of Pain. Molecules 2018, 23, 681. [Google Scholar] [PubMed]
- Bussières, A.E.; Stewart, G.; Al-Zoubi, F.; Decina, P.; Descarreaux, M.; Hayden, J.; Hendrickson, B.; Hincapié, C.; Pagé, I.; Passmore, S.; et al. The Treatment of Neck Pain-Associated Disorders and Whiplash-Associated Disorders: A Clinical Practice Guideline. J. Manip. Physiol. Ther. 2016, 39, 523–564.e527. [Google Scholar] [CrossRef]
- Banerjee, S.; Argáez, C. Multidisciplinary Treatment Programs for Patients with Acute or Subacute Pain: A Review of Clinical Effectiveness, Cost-Effectiveness, and Guidelines. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health. Available online: https://www.ncbi.nlm.nih.gov/books/NBK546002/ (accessed on 7 May 2023).
- Fitzcharles, M.A.; Cohen, S.P.; Clauw, D.J.; Littlejohn, G.; Usui, C.; Häuser, W. Nociplastic pain: Towards an understanding of prevalent pain conditions. Lancet 2021, 397, 2098–2110. [Google Scholar] [CrossRef] [PubMed]
- Devers, A.; Galer, B.S. Topical Lidocaine Patch Relieves a Variety of Neuropathic Pain Conditions: An Open-Label Study. Clin. J. Pain 2000, 16, 205–208. [Google Scholar] [CrossRef]
- Cohen, S.P.; Vase, L.; Hooten, W.M. Chronic pain: An update on burden, best practices, and new advances. Lancet 2021, 397, 2082–2097. [Google Scholar] [CrossRef]
- Ripamonti, C.I.; Bandieri, E.; Roila, F. Management of cancer pain: ESMO clinical practice guidelines. Ann. Oncol. 2011, 22, vi69–vi77. [Google Scholar] [CrossRef]
- Ventafridda, V.; Saita, L.; Ripamonti, C.; De Conno, F. WHO guidelines for the use of analgesics in cancer pain. Int. J. Tissue React. 1985, 7, 93–96. [Google Scholar]
- Carr, D.B.; Goudas, L.C. Acute pain. Lancet 1999, 353, 2051–2058. [Google Scholar] [CrossRef]
- Franco, P.; De Marco, I. Supercritical CO2 adsorption of non-steroidal anti-inflammatory drugs into biopolymer aerogels. J. CO2 Util. 2020, 36, 40–53. [Google Scholar] [CrossRef]
- Upton, R.N.; Semple, T.J.; Macintyre, P.E. Pharmacokinetic Optimisation of Opioid Treatment in Acute Pain Therapy. Clin. Pharmacokinet. 1997, 33, 225–244. [Google Scholar] [CrossRef] [PubMed]
- Gordon, D.B.; Dahl, J.; Phillips, P.; Frandsen, J.; Cowley, C.; Foster, R.L.; Fine, P.G.; Miaskowski, C.; Fishman, S.; Finley, R.S. The use of “as-needed” range orders for opioid analgesics in the management of acute pain: A consensus statement of the American Society for Pain Management Nursing and the American Pain Society. Pain Manag. Nurs. 2004, 5, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Walder, B.; Schafer, M.; Henzi, I.; Tramer, M. Efficacy and safety of patient-controlled opioid analgesia for acute postoperative pain: A quantitative systematic review. Acta Anaesthesiol. Scand. 2001, 45, 795–804. [Google Scholar] [CrossRef] [PubMed]
- Furlan, A.D.; Sandoval, J.A.; Mailis-Gagnon, A.; Tunks, E. Opioids for chronic noncancer pain: A meta-analysis of effectiveness and side effects. CMAJ 2006, 174, 1589–1594. [Google Scholar] [CrossRef]
- Sarzi-Puttini, P.; Vellucci, R.; Zuccaro, S.M.; Cherubino, P.; Labianca, R.; Fornasari, D. The appropriate treatment of chronic pain. Clin. Drug Investig. 2012, 32, 21–33. [Google Scholar] [CrossRef]
- McCleane, G.J. Pain Management: Expanding the Pharmacological Options; Wiley-Blackwell: Hoboken, NJ, USA, 2009; pp. 1–192. ISBN 978140517823. [Google Scholar] [CrossRef]
- Manchikanti, L.; Singh, V.; Caraway, D.L.; Benyamin, R.M. Breakthrough pain in chronic non-cancer pain: Fact, fiction, or abuse. Pain Phys. 2011, 14, E103–E117. [Google Scholar] [CrossRef]
- Leonardi, C.; Vellucci, R.; Mammucari, M.; Fanelli, G. Opioid risk addiction in the management of chronic pain in primary care: The addition risk questionnaire. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 4898–4905. [Google Scholar]
- Fallon, M.; Giusti, R.; Aielli, F.; Hoskin, P.; Rolke, R.; Sharma, M.; Ripamonti, C.I. Management of cancer pain in adult patients: ESMO Clinical Practice Guidelines. Ann. Oncol. 2018, 29, iv166–iv191. [Google Scholar] [CrossRef]
- Volkow, N.; Benveniste, H.; McLellan, A.T. Use and Misuse of Opioids in Chronic Pain. In Annual Review of Medicine; Annual Reviews Inc.: San Mateo, CA, USA, 2018; Volume 69, pp. 451–465. [Google Scholar]
- Latina, R.; Varrassi, G.; Di Biagio, E.; Giannarelli, D.; Gravante, F.; Paladini, A.; D’Angelo, D.; Iacorossi, L.; Martella, C.; Alvaro, R.; et al. Chronic Non-cancer Pain Management in a Tertiary Pain Clinic Network: A Retrospective Study. Pain Ther. 2023, 12, 151–164. [Google Scholar] [CrossRef]
- Alkilani, A.Z.; McCrudden, M.T.; Donnelly, R.F. Transdermal Drug Delivery: Innovative Pharmaceutical Developments Based on Disruption of the Barrier Properties of the stratum corneum. Pharmaceutics 2015, 7, 438–470. [Google Scholar] [CrossRef]
- Schoellhammer, C.M.; Blankschtein, D.; Langer, R. Skin permeabilization for transdermal drug delivery: Recent advances and future prospects. Expert Opin. Drug Deliv. 2014, 11, 393–407. [Google Scholar] [CrossRef] [PubMed]
- Mathews, L.M.; Roy, A. Management of pain using transdermal patches—A review. Asian J. Pharm. Clin. Res. 2016, 9, 32–35. [Google Scholar] [CrossRef]
- Ciurba, A.; Antonoaea, P.; Todoran, N.; Rédai, E.; Vlad, R.A.; Tătaru, A.; Muntean, D.L.; Bîrsan, M. Polymeric films containing tenoxicam as prospective transdermal drug delivery systems: Design and characterization. Processes 2021, 9, 136. [Google Scholar] [CrossRef]
- Tsai, J.H.; Liu, I.T.; Su, P.F.; Huang, Y.T.; Chiu, G.L.; Chen, Y.Y.; Lai, W.S.; Lin, P.C. Lidocaine transdermal patches reduced pain intensity in neuropathic cancer patients already receiving opioid treatment. BMC Palliat. Care 2023, 22, 4. [Google Scholar] [CrossRef] [PubMed]
- Franco, P.; Pessolano, E.; Belvedere, R.; Petrella, A.; De Marco, I. Supercritical impregnation of mesoglycan into calcium alginate aerogel for wound healing. J. Supercrit. Fluids 2020, 157, 104711. [Google Scholar] [CrossRef]
- Belvedere, R.; Novizio, N.; Morello, S.; Petrella, A. The combination of mesoglycan and VEGF promotes skin wound repair by enhancing the activation of endothelial cells and fibroblasts and their cross-talk. Sci. Rep. 2022, 12, 11041. [Google Scholar] [CrossRef]
- Khandaker, M.; Alkadhem, N.; Progri, H.; Nikfarjam, S.; Jeon, J.; Kotturi, H.; Vaughan, M.B. Glutathione Immobilized Polycaprolactone Nanofiber Mesh as a Dermal Drug Delivery Mechanism for Wound Healing in a Diabetic Patient. Processes 2022, 10, 512. [Google Scholar] [CrossRef]
- Tyeb, S.; Verma, V.; Kumar, N. Polysaccharide based transdermal patches for chronic wound healing: Recent advances and clinical perspective. Carbohydr. Polym. 2023, 316, 121038. [Google Scholar] [CrossRef]
- Jeong, W.Y.; Kwon, M.; Choi, H.E.; Kim, K.S. Recent advances in transdermal drug delivery systems: A review. Biomater. Res. 2021, 25, 24. [Google Scholar] [CrossRef]
- Kaestli, L.Z.; Wasilewski-Rasca, A.F.; Bonnabry, P.; Vogt-Ferrier, N. Use of transdermal drug formulations in the elderly. Drugs Aging 2008, 25, 269–280. [Google Scholar] [CrossRef]
- Tanner, T.; Marks, R. Delivering drugs by the transdermal route: Review and comment. Ski Res. Technol. 2008, 14, 249–260. [Google Scholar] [CrossRef] [PubMed]
- Bird, D.; Ravindra, N.M. Transdermal drug delivery and patches—An overview. Med. Devices Sens. 2020, 3, e10069. [Google Scholar] [CrossRef]
- Sozio, P.; Cerasa, L.S.; Marinelli, L.; Di Stefano, A. Transdermal donepezil on the treatment of Alzheimer’s disease. Neuropsychiatr. Dis. Treat. 2012, 8, 361–368. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Zhang, Y.; Yu, X.; Xu, C. Wearable patches for transdermal drug delivery. Acta Pharm. Sin. B 2023, 13, 2298–2309. [Google Scholar] [CrossRef] [PubMed]
- McKenna, P.E.; Abbate, M.T.A.; Vora, L.K.; Sabri, A.H.; Peng, K.; Volpe-Zanutto, F.; Tekko, I.A.; Permana, A.D.; Maguire, C.; Dineen, D.; et al. Polymeric Microarray Patches for Enhanced Transdermal Delivery of the Poorly Soluble Drug Olanzapine. ACS Appl. Mater. Interfaces 2023, 15, 31300–31319. [Google Scholar] [CrossRef]
- Naser, Y.A.; Tekko, I.A.; Vora, L.K.; Peng, K.; Anjani, Q.K.; Greer, B.; Elliott, C.; McCarthy, H.O.; Donnelly, R.F. Hydrogel-forming microarray patches with solid dispersion reservoirs for transdermal long-acting microdepot delivery of a hydrophobic drug. J. Control. Release 2023, 356, 416–433. [Google Scholar] [CrossRef]
- Wermeling, D.P.; Banks, S.L.; Hudson, D.A.; Gill, H.S.; Gupta, J.; Prausnitz, M.R.; Stinchcomb, A.L. Microneedles permit transdermal delivery of a skin-impermeant medication to humans. Proc. Natl. Acad. Sci. USA 2008, 105, 2058–2063. [Google Scholar] [CrossRef]
- Kochhar, J.S.; Lim, W.X.S.; Zou, S.; Foo, W.Y.; Pan, J.; Kang, L. Microneedle integrated transdermal patch for fast onset and sustained delivery of lidocaine. Mol. Pharm. 2013, 10, 4272–4280. [Google Scholar] [CrossRef]
- Gupta, J.; Felner, E.I.; Prausnitz, M.R. Rapid pharmacokinetics of intradermal insulin administered using microneedles in type 1 diabetes subjects. Diabetes Technol. Ther. 2011, 13, 451–456. [Google Scholar] [CrossRef]
- Freynhagen, R.; Von Giesen, H.J.; Busche, P.; Sabatowski, R.; Konrad, C.; Grond, S. Switching from reservoir to matrix systems for the transdermal delivery of fentanyl: A prospective, multicenter pilot study in outpatients with chronic pain. J. Pain Symptom Manag. 2005, 30, 289–297. [Google Scholar] [CrossRef]
- Grape, S.; Schug, S.A.; Lauer, S.; Schug, B.S. Formulations of fentanyl for the management of pain. Drugs 2010, 70, 57–72. [Google Scholar] [CrossRef] [PubMed]
- Jeal, W.; Benfield, P. Transdermal fentanyl—A review of its pharmacological properties and therapeutic efficacy in pain control. Drugs 1997, 53, 109–138. [Google Scholar] [CrossRef]
- Roy, S.D.; Flynn, G.L. Transdermal Delivery of Narcotic Analgesics: pH, Anatomical, and Subject Influences on Cutaneous Permeability of Fentanyl and Sufentanil. Pharm. Res. Off. J. Am. Assoc. Pharm. Sci. 1990, 7, 842–847. [Google Scholar] [CrossRef]
- Gupta, S.K.; Southam, M.; Gale, R.; Hwang, S.S. System functionality and physicochemical model of fentanyl transdermal system. J. Pain Symptom Manag. 1992, 7, S17–S26. [Google Scholar] [CrossRef] [PubMed]
- Takashina, Y.; Naito, T.; Mino, Y.; Yagi, T.; Ohnishi, K.; Kawakami, J. Impact of CYP3A5 and ABCB1 gene polymorphisms on fentanyl pharmacokinetics and clinical responses in cancer patients undergoing conversion to a transdermal system. Drug Metab. Pharmacokinet. 2012, 27, 414–421. [Google Scholar] [CrossRef]
- Prodduturi, S.; Smith, G.J.; Wokovich, A.M.; Doub, W.H.; Westenberger, B.J.; Buhse, L. Reservoir based fentanyl transdermal drug delivery systems: Effect of patch age on drug release and skin permeation. Pharm. Res. 2009, 26, 1344–1352. [Google Scholar] [CrossRef]
- Kim, T.S.; Jin, S.E.; Sun, B.; Kim, M.S.; Hwang, S.J. Comparison of adhesion and dissolution of fentanyl patches: Fentadur® and Durogesic DTrans®. J. Pharm. Investig. 2015, 45, 475–480. [Google Scholar] [CrossRef]
- Miyazaki, T.; Hanaoka, K.; Namiki, A.; Ogawa, S.; Kitajima, T.; Hosokawa, T.; Ishida, T.; Nogami, S.; Mashimo, S. Efficacy, safety and pharmacokinetic study of a novel fentanyl-containing matrix transdermal patch system in Japanese patients with cancer pain. Clin. Drug Investig. 2008, 28, 313–325. [Google Scholar] [CrossRef]
- Prodduturi, S.; Sadrieh, N.; Wokovich, A.M.; Doub, W.H.; Westenberger, B.J.; Buhse, L. Transdermal delivery of fentanyl from matrix and reservoir systems: Effect of heat and compromised skin. J. Pharm. Sci. 2010, 99, 2357–2366. [Google Scholar] [CrossRef]
- Marier, J.F.; Lor, M.; Morin, J.; Roux, L.; Di Marco, M.; Morelli, G.; Sædder, E.A. Comparative bioequivalence study between a novel matrix transdermal delivery system of fentanyl and a commercially available reservoir formulation. Br. J. Clin. Pharmacol. 2007, 63, 121–124. [Google Scholar] [CrossRef]
- Marier, J.F.; Lor, M.; Potvin, D.; DiMarco, M.; Morelli, G.; Sædder, E.A. Pharmacokinetics, tolerability, and performance of a novel matrix transdermal delivery system of fentanyl relative to the commercially available reservoir formulation in healthy subjects. J. Clin. Pharmacol. 2006, 46, 642–653. [Google Scholar] [CrossRef] [PubMed]
- Hoy, S.M.; Keating, G.M. Fentanyl Transdermal Matrix Patch (Durotep® MT Patch; Durogesic® DTrans®; Durogesic® SMAT). Drugs 2008, 68, 1711–1721. [Google Scholar] [CrossRef] [PubMed]
- Hair, P.I.; Keating, G.M.; McKeage, K. Transdermal matrix fentanyl membrane patch (Matrifen®): In severe cancer-related chronic pain. Drugs 2008, 68, 2001–2009. [Google Scholar] [CrossRef] [PubMed]
- Lane, M.E. The transdermal delivery of fentanyl. Eur. J. Pharm. Biopharm. 2013, 84, 449–455. [Google Scholar] [CrossRef]
- Marquardt, K.A.; Tharratt, R.S.; Musallam, N.A. Fentanyl remaining in a transdermal system following three days of continuous use. Ann. Pharmacother. 1995, 29, 969–971. [Google Scholar] [CrossRef]
- Oliveira, G.; Hadgraft, J.; Lane, M.E. Toxicological implications of the delivery of fentanyl from gel extracted from a commercial transdermal reservoir patch. Toxicol. In Vitro 2012, 26, 645–648. [Google Scholar] [CrossRef]
- Kuhlman, J.J., Jr.; McCaulley, R.; Valouch, T.J.; Behonick, G.S. Fentanyl use, misuse, and abuse: A summary of 23 postmortem cases. J. Anal. Toxicol. 2003, 27, 499–504. [Google Scholar] [CrossRef] [PubMed]
- Moore, K.T.; Sathyan, G.; Richarz, U.; Natarajan, J.; Vandenbossche, J. Randomized 5-treatment crossover study to assess the effects of external heat on serum fentanyl concentrations during treatment with transdermal fentanyl systems. J. Clin. Pharmacol. 2012, 52, 1174–1185. [Google Scholar] [CrossRef]
- Zecca, E.; Manzoni, A.; Centurioni, F.; Farina, A.; Bonizzoni, E.; Seiler, D.; Perrone, T.; Caraceni, A. Pharmacokinetic study between a bilayer matrix fentalyl patch and a monolayer matrix fentanyl patch: Single dose administration in healthy volunteers. Br. J. Clin. Pharmacol. 2015, 80, 110–115. [Google Scholar] [CrossRef]
- Defraeye, T.; Bahrami, F.; Ding, L.; Malini, R.I.; Terrier, A.; Rossi, R.M. Predicting Transdermal Fentanyl Delivery Using Mechanistic Simulations for Tailored Therapy. Front. Pharmacol. 2020, 11, 585393. [Google Scholar] [CrossRef]
- Shomaker, T.S.; Zhang, J.; Ashburn, M.A. Assessing the impact of heat on the systemic delivery of fentanyl through the transdermal fentanyl delivery system. Pain Med. 2000, 1, 225–230. [Google Scholar] [CrossRef]
- Luckenbill, K.; Thompson, J.; Middleton, O.; Kloss, J.; Apple, F. Fentanyl postmortem redistribution: Preliminary findings regarding the relationship among femoral blood and liver and heart tissue concentrations. J. Anal. Toxicol. 2008, 32, 639–643. [Google Scholar] [CrossRef] [PubMed]
- Gudin, J.; Fudin, J. A Narrative Pharmacological Review of Buprenorphine: A Unique Opioid for the Treatment of Chronic Pain. Pain Ther. 2020, 9, 41–54. [Google Scholar] [CrossRef] [PubMed]
- Al-Tawil, N.; Odar-Cederlöf, I.; Berggren, A.C.; Johnson, H.E.; Persson, J. Pharmacokinetics of transdermal buprenorphine patch in the elderly. Eur. J. Clin. Pharmacol. 2013, 69, 143–149. [Google Scholar] [CrossRef]
- Plosker, G.L. Buprenorphine 5, 10 and 20 μg/h Transdermal Patch. Drugs 2011, 71, 2491–2509. [Google Scholar] [CrossRef]
- Böhme, K. Buprenorphine in a transdermal therapeutic system—A new option. Clin. Rheumatol. 2002, 21, S13–S16. [Google Scholar] [CrossRef] [PubMed]
- Ehrlich, A.T.; Darcq, E. Recommending buprenorphine for pain management. Pain Manag. 2019, 9, 13–16. [Google Scholar] [CrossRef]
- Wilding, I.R.; Davis, S.S.; Rimoy, G.H.; Rubin, P.; Kurihara-Bergstrom, T.; Tipnis, V.; Berner, B.; Nightingale, J. Pharmacokinetic evaluation of transdermal buprenorphine in man. Int. J. Pharm. 1996, 132, 81–87. [Google Scholar] [CrossRef]
- Sittl, R.; Nuijten, M.; Nautrup, B.P. Changes in the prescribed daily doses of transdermal fentanyl and transdermal buprenorphine during treatment of patients with cancer and noncancer pain in Germany: Results of a retrospective cohort study. Clin. Ther. 2005, 27, 1022–1031. [Google Scholar] [CrossRef]
- Ahn, J.S.; Lin, J.; Ogawa, S.; Yuan, C.; O’Brien, T.; Le, B.H.; Bothwell, A.M.; Moon, H.; Hadjiat, Y.; Ganapathi, A. Transdermal buprenorphine and fentanyl patches in cancer pain: A network systematic review. J. Pain Res. 2017, 10, 1963–1972. [Google Scholar] [CrossRef]
- Evans, H.C.; Easthope, S.E. Transdermal buprenorphine. Drugs 2003, 63, 1999–2010. [Google Scholar] [CrossRef] [PubMed]
- Likar, R.; Lorenz, V.; Korak-Leiter, M.; Kager, I.; Sittl, R. Transdermal Buprenorphine Patches Applied in a 4-Day Regimen Versus a 3-Day Regimen: A Single-Site, Phase III, Randomized, Open-Label, Crossover Comparison. Clin. Ther. 2007, 29, 1591–1606. [Google Scholar] [CrossRef] [PubMed]
- Mythili, N.; Navaneetham, R.; Sham, M.E.; Menon, S.; Kumar, V.; Archana, S. Efficacy of Transdermal Buprenorphine Patch in Postoperative Pain Management in Oral and Maxillofacial Surgery. J. Maxillofac. Oral Surg. 2022, 1–6. [Google Scholar] [CrossRef]
- Breivik, H.; Ljosaa, T.M.; Stengaard-Pedersen, K.; Persson, J.; Aro, H.; Villumsen, J.; Tvinnemose, D. A 6-months, randomised, placebo-controlled evaluation of efficacy and tolerability of a low-dose 7-day buprenorphine transdermal patch in osteoarthritis patients naïve to potent opioids. Scand. J. Pain 2010, 1, 122–141. [Google Scholar] [CrossRef] [PubMed]
- Yoon, D.H.; Bin, S.-I.; Chan, S.K.-C.; Chung, C.K.; In, Y.; Kim, H.; Lichauco, J.J.; Mok, C.C.; Moon, Y.-W.; Ng, T.K.-T.; et al. Effectiveness and tolerability of transdermal buprenorphine patches: A multicenter, prospective, open-label study in Asian patients with moderate to severe chronic musculoskeletal pain. BMC Musculoskelet. Disord. 2017, 18, 337. [Google Scholar] [CrossRef]
- Brown, L.; Langer, R. Transdermal delivery of drugs. Annu. Rev. Med. 1988, 39, 221–229. [Google Scholar] [CrossRef]
- James, I.G.; O’Brien, C.M.; McDonald, C.J. A randomized, double-blind, double-dummy comparison of the efficacy and tolerability of low-dose transdermal buprenorphine (BuTrans seven-day patches) with buprenorphine sublingual tablets (Temgesic) in patients with osteoarthritis pain. J. Pain Symptom Manag. 2010, 40, 266–278. [Google Scholar] [CrossRef]
- Karlsson, M.; Berggren, A.C. Efficacy and safety of low-dose transdermal buprenorphine patches (5, 10, and 20 microg/h) versus prolonged-release tramadol tablets (75, 100, 150, and 200 mg) in patients with chronic osteoarthritis pain: A 12-week, randomized, open-label, controlled, parallel-group noninferiority study. Clin. Ther. 2009, 31, 503–513. [Google Scholar] [CrossRef]
- Kim, H.J.; Ahn, H.S.; Nam, Y.; Chang, B.S.; Lee, C.K.; Yeom, J.S. Comparative study of the efficacy of transdermal buprenorphine patches and prolonged-release tramadol tablets for postoperative pain control after spinal fusion surgery: A prospective, randomized controlled non-inferiority trial. Eur. Spine J. 2017, 26, 2961–2968. [Google Scholar] [CrossRef]
- Plosker, G.L.; Lyseng-Williamson, K.A. Buprenorphine 5, 10 and 20 μg/h transdermal patch: A guide to its use in chronic non-malignant pain. CNS Drugs 2012, 26, 367–373. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Patch | Amount of Drug [μg/h] | Main Results | Reference |
|---|---|---|---|
| Reservoir | 25–100 | Comparison with fentanyl infusion; the drug half-life after patch removal was significantly longer than the half-life after infusion | [47] |
| 25–50 | Use of Durotep® commercial patches on 60 Japanese cancer patients that previously used oral morphine or oxycodone; evaluation of the influence of two biomarkers on fentanyl pharmacokinetics | [48] | |
| 25 | Use of Duragesic® commercial patches to evaluate stability and skin permeation profiles as a function of the age of the patch | [49] | |
| Matrix | 12–100 | Comparison with a reservoir system; tests on 46 patients with CCP and CNCP; 91% of patients preferred the matrix system | [43] |
| 12–100 | Comparison between Fentadur®, a reservoir system, and Durogesic Dtrans®, a matrix system, in terms of adhesion and dissolution properties; both were acceptable for skin attachment, although higher adhesion forces were expressed by the matrix system; from the point of view of the dissolution study, the release of the reservoir system was lower than that of the matrix system. | [50] | |
| 12.5 | Comparison with Durotep®, a commercial reservoir system; tests on 87 patients of both sexes with a confirmed diagnosis of cancer; successful replacement of morphine, oral oxycodone, or fentanyl injection formulations | [51] | |
| 25 | Comparison with Duragesic® commercial patches to evaluate the effect of elevated temperatures and compromised skin on drug release and skin permeation; the patches are comparable when applied to intact skin at normal skin temperature, whereas, in the case of compromised skin, the matrix patch has a more significant permeation enhancement effect than the reservoir system | [52] | |
| 50 | Comparison with Durogesic®, a commercial reservoir system; adherence and skin irritability results were similar, but the matrix formulation is more convenient because of the smaller size | [53] | |
| 50 | Comparison with a reservoir system; tests on 24 male patients; enhanced adherence compared to the reservoir formulation; constant fentanyl delivery rate over three days | [54] | |
| 12.5–50 | Use of Durotep® MT patch, Durogesic® Dtrans®, and Durogesic® SMAT commercial patches; comparison with a reservoir system; patients preferred the transdermal matrix patch over the transdermal reservoir patch | [55] | |
| 12–300 | Equivalent to a reservoir system in terms of TDD and analgesic efficacy in patients with CCP | [56] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Marco, I. Transdermal Patches Containing Opioids in the Treatment of Patients with Chronic Pain. Processes 2023, 11, 2673. https://doi.org/10.3390/pr11092673
De Marco I. Transdermal Patches Containing Opioids in the Treatment of Patients with Chronic Pain. Processes. 2023; 11(9):2673. https://doi.org/10.3390/pr11092673
Chicago/Turabian StyleDe Marco, Iolanda. 2023. "Transdermal Patches Containing Opioids in the Treatment of Patients with Chronic Pain" Processes 11, no. 9: 2673. https://doi.org/10.3390/pr11092673
APA StyleDe Marco, I. (2023). Transdermal Patches Containing Opioids in the Treatment of Patients with Chronic Pain. Processes, 11(9), 2673. https://doi.org/10.3390/pr11092673