
Immune Fitness and the Psychosocial and Health Consequences of the COVID-19 Pandemic Lockdown in The Netherlands: Methodology and Design of the CLOFIT Study

 , , , , , , and
, , , , , , and 
Abstract
:1. Introduction
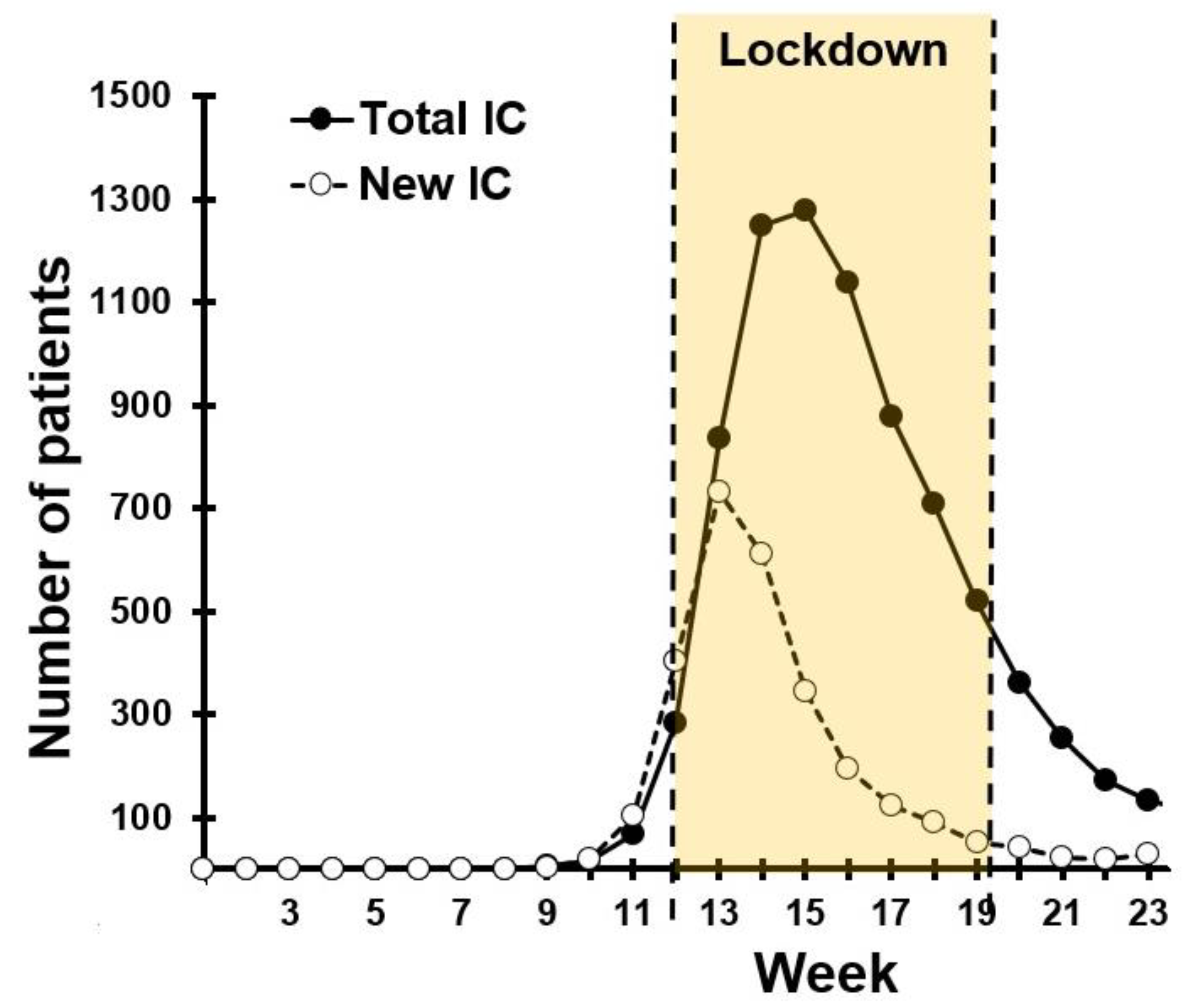
1.1. The Dutch “Intelligent Lockdown”
1.2. Psychological and Health Consequences of a Lockdown
1.3. Chronic Stress, Immune Fitness, and Susceptibility to Viral Infection
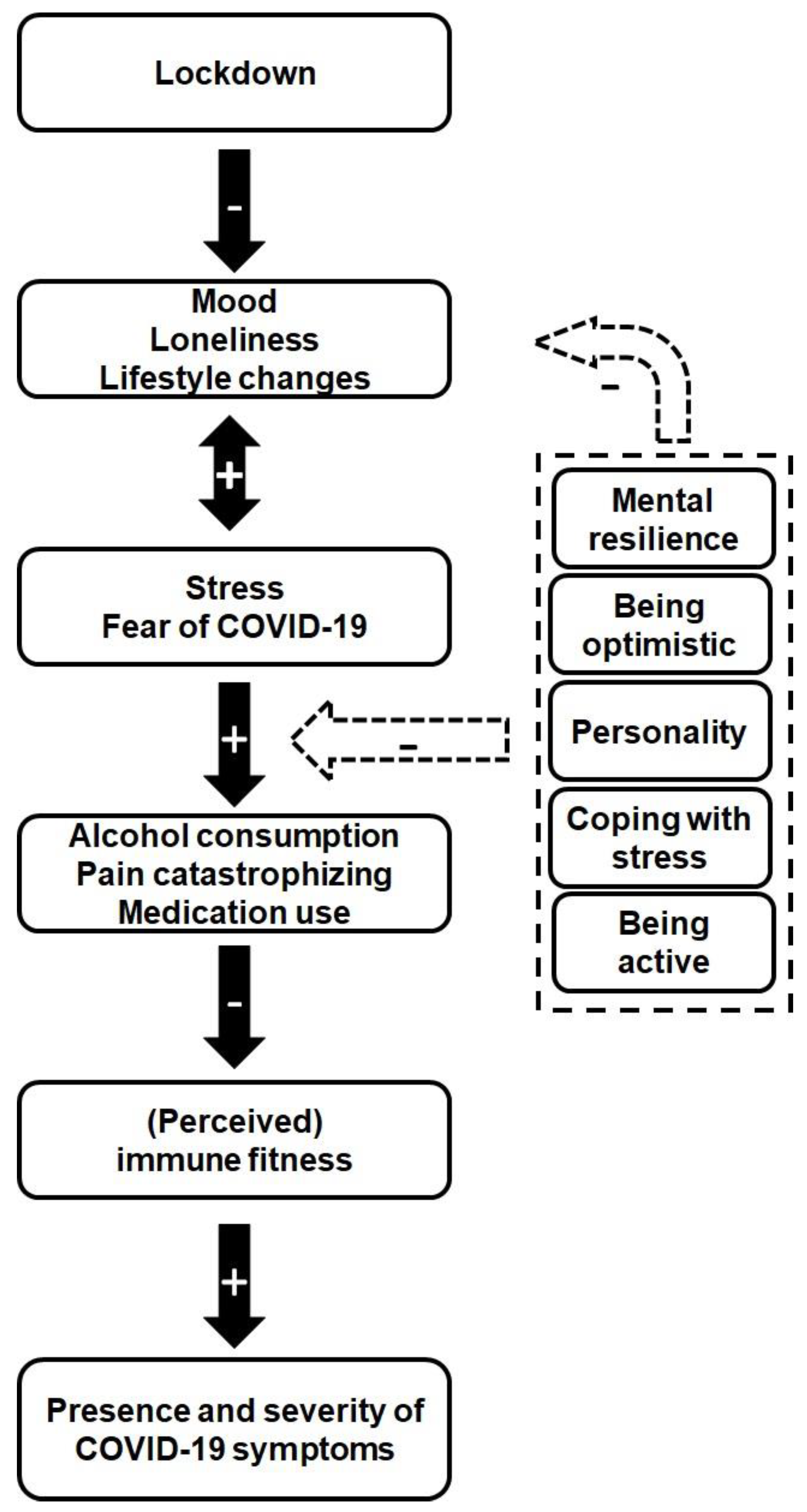
1.4. Aim of the CLOFIT Study
2. Materials and Methods
2.1. Design, Population, and Recruitment
2.2. Survey Content and Outcomes
2.2.1. Demographics
2.2.2. Education and Work
2.2.3. Underlying Diseases
2.2.4. The Use of Medicines
2.2.5. Mood and Quality of Life
2.2.6. Fear of COVID-19 (FCV-19S)
2.2.7. Immune Status Questionnaire (ISQ)
2.2.8. Perceived Immune Fitness
2.2.9. The Jackson Symptoms Scale—Common Cold
2.2.10. COVID-19 Symptoms Scale (C-19SS)
2.2.11. COVID-19 Test
2.2.12. Alcohol Consumption
2.2.13. Pain Sensitivity Questionnaire (PSQ)
2.2.14. Pain Catastrophizing Scale (PCS)
2.2.15. Graded Chronic Pain Scale—Revised (GCPS-R)
2.2.16. Use of Pain Medication
2.2.17. The FANTASTIC Lifestyle Checklist
2.2.18. Mental Resilience
2.2.19. Personality
2.2.20. Concluding Questions and Remarks
2.3. Data Handling and Statistical Analysis
3. Results
4. Discussion
4.1. Limitations
4.2. Future Research Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Virtual Press Conference on COVID-19. Available online: https://www.who.int/docs/default-source/coronaviruse/transcripts/who-audio-emergencies-coronavirus-press-conference-full-and-final-11mar2020.pdf?sfvrsn=cb432bb3_2 (accessed on 1 November 2020).
- Rijksoverheid. Coronavirus COVID-19. Available online: https://www.rijksoverheid.nl/onderwerpen/coronavirus-covid-19 (accessed on 25 January 2021).
- Stichting NICE (National Intensive Care Evaluation). Available online: https://experience.arcgis.com/experience/e58fd5e1779b4cdd9d81e44b9b1032d0 (accessed on 1 November 2020).
- Statistics Netherlands. Available online: https://opendata.cbs.nl/statline/#/CBS/nl/dataset/70895ned/table?fromstatweb (accessed on 1 November 2020).
- National Institute for Public Health and the Environment (RIVM). Available online: https://www.rivm.nl/en/node/154271 (accessed on 1 November 2020).
- Pak, A.; Adegboye, O.A.; Adekunle, A.I.; Rahman, K.M.; McBryde, E.S.; Eisen, D.P. Economic Consequences of the COVID-19 Outbreak: The Need for Epidemic Preparedness. Front. Public Health 2020, 8, 241. [Google Scholar] [CrossRef]
- Kumar, A.; Nayar, K.R. COVID-19 and mass fatality management: A public health challenge. Disaster Med. Public Health Prep. 2020, 14, e38–e39. [Google Scholar] [CrossRef] [PubMed]
- Khan, K.S.; Mamun, M.A.; Griffiths, M.D.; Ulla, I. The mental health impact of the COVID-19 pandemic across different cohorts. Int. J. Ment. Health Addict. 2020, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Rossi, R.; Socci, V.; Talevi, D.; Mensi, S.; Niolu, C.; Pacitti, F.; Di Marco, A.; Rossi, A.; Siracusano, A.; Di Lorenzo, G. COVID-19 pandemic and lockdown measures impact on mental health among the general population in Italy. Front. Psychiatry 2020, 11, 790. [Google Scholar] [CrossRef]
- Wu, K.K.; Chan, S.K.; Ma, T.M. Posttraumatic stress, anxiety, and depression in survivors of severe acute respiratory syndrome (SARS). J. Trauma. Stress 2005, 18, 39–42. [Google Scholar] [CrossRef]
- Hawryluck, L.; Gold, W.L.; Robinson, S.; Pogorski, S.; Galea, S.; Styra, R. SARS control and psychological effects of quarantine, Toronto, Canada. Emerg. Infect. Dis. 2004, 10, 1206–1212. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Deater-Deckard, K.D.; Panneton, R. Parental Stress and Early Child Development. Adaptive and Maladaptive Outcomes; Springer International Publishing: Cham, Switzerland, 2017. [Google Scholar]
- Gualano, M.R.; Lo Moro, G.; Voglino, G.; Bert, F.; Siliquini, R. Effects of COVID-19 lockdown on mental health and sleep disturbances in Italy. Int. J. Environ. Res. Public Health 2020, 17, 4779. [Google Scholar] [CrossRef]
- Ahmed, M.Z.; Ahmed, O.; Aibao, Z.; Hanbin, S.; Siyu, L.; Ahmad, A. Epidemic of COVID-19 in China and associated Psychological Problems. Asian J. Psychiatry 2020, 51, 102092. [Google Scholar] [CrossRef]
- Cinelli, M.; Quattrociocchi, W.; Galeazzi, A.; Valensise, C.M.; Brugnoli, E.; Schmidt, A.L.; Zola, P.; Zollo, F.; Scala, A. The COVID-19 social media infodemic. Sci. Rep. 2020, 10, 16598. [Google Scholar] [CrossRef]
- Kocevska, D.; Blanken, T.F.; Van Someren, E.J.W.; Rösler, L. Sleep quality during the COVID-19 pandemic: Not one size fits all. Sleep Med. 2020, 76, 86–88. [Google Scholar] [CrossRef] [PubMed]
- De Haas, M.; Faber, R.; Hamersma, M. How COVID-19 and the Dutch ‘intelligent lockdown’ change activities, work and travel behaviour: Evidence from longitudinal data in the Netherlands. Transp. Res. Interdiscip. Perspect. 2020, 6, 100150. [Google Scholar] [CrossRef]
- Janssen, L.H.C.; Kullberg, M.J.; Verkuil, B.; van Zwieten, N.; Wever, M.C.M.; van Houtum, L.A.E.M.; Wentholt, W.G.M.; Elzinga, B.M. Does the COVID-19 pandemic impact parents’ and adolescents’ well-being? An EMA-study on daily affect and parenting. PLoS ONE 2020, 15, e0240962. [Google Scholar] [CrossRef]
- Elling, J.M.; Crutzen, R.; Talhout, R.; de Vries, H. Tobacco smoking and smoking cessation in times of COVID-19. Tob. Prev. Cessat. 2020, 6, 39. [Google Scholar] [CrossRef] [PubMed]
- Poelman, M.P.; Gillebaart, M.; Schlinkert, C.; Dijkstra, S.C.; Derksen, E.; Mensink, F.; Hermans, R.C.J.; Aardening, P.; de Ridder, D.; de Vet, E. Eating behavior and food purchases during the COVID-19 lockdown: A cross-sectional study among adults in the Netherlands. Appetite 2020, 157, 105002. [Google Scholar] [CrossRef]
- Morey, J.N.; Boggero, I.A.; Scott, A.B.; Segerstrom, S.C. Current directions in stress and human immune function. Curr. Opin. Psychol. 2015, 5, 13–17. [Google Scholar] [CrossRef] [Green Version]
- Pawelec, G.; Akbar, A.; Caruso, C.; Solana, R.; Grubeck-Loebenstein, B.; Wikby, A. Human immunosenescence: Is it infectious? Immunol. Rev. 2005, 205, 257–268. [Google Scholar] [CrossRef]
- Gouin, J.P. Chronic stress, immune dysregulation, and health. Am. J. Lifestyle Med. 2011, 5, 476–485. [Google Scholar] [CrossRef]
- Cohen, S.; Tyrrell, D.A.; Smith, A.P. Psychological stress and susceptibility to the common cold. NEJM 1991, 325, 606–612. [Google Scholar] [CrossRef]
- Cohen, S.; Frank, E.; Doyle, W.J.; Skoner, D.P.; Rabin, B.S.; Gwaltney, J.M. Types of stressors that increase susceptibility to the common cold in healthy adults. Health Psychol. 1998, 17, 214–223. [Google Scholar] [CrossRef]
- Hogarth, L.; Hardy, L.; Mathew, A.R.; Hitsman, B. Negative mood-induced alcohol-seeking is greater in young adults who report depression symptoms, drinking to cope, and subjective reactivity. Exp. Clin. Psychopharmacol. 2018, 26, 138–146. [Google Scholar] [CrossRef] [Green Version]
- Widyadharma, I.P.E.; Dewi, P.R.; Wijayanti, I.A.S.; Utami, D.K.I. Pain related viral infections: A literature review. Egypt. J. Neurol. Psychiatry Neurosurg. 2020, 56, 105. [Google Scholar] [CrossRef]
- Kersebaum, D.; Fabig, S.C.; Sendel, M.; Sachau, J.; Lassen, J.; Rehm, S.; Hüllemann, P.; Baron, R.; Gierthmühlen, J. The early influence of COVID-19 pandemic-associated restrictions on pain, mood, and everyday life of patients with painful polyneuropathy. Pain Rep. 2020, 5, e858. [Google Scholar] [CrossRef]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef]
- Herbert, C.; Gilg, V.; Sander, M.; Kobel, S.; Jerg, A.; Steinacker, J.M. Preventing mental health, well-being and physical activity during the corona pandemic—Recommendations from psychology and sports medicine. Dtsch. Z. Sportmed. 2020, 71, 249–257. [Google Scholar] [CrossRef]
- Fuller, H.R.; Huseth-Zosel, A. Lessons in Resilience: Initial Coping among Older Adults during the COVID-19 Pandemic. Gerontologist 2021, 61, 114–125. [Google Scholar] [CrossRef]
- Ahmed, I.; Hasan, M.; Akter, R.; Sarkar, B.K.; Rahman, M.; Sarker, S.; Samad, M.A. Behavioral preventive measures and the use of medicines and herbal products among the public in response to Covid-19 in Bangladesh: A cross-sectional study. PLoS ONE 2020, 15, e0243706. [Google Scholar] [CrossRef]
- Van Schrojenstein Lantman, M.; Mackus, M.; van de Loo, A.J.A.E.; Verster, J.C. The impact of alcohol hangover symptoms on cognitive and physical functioning, and mood. Hum. Psychopharmacol. 2017, 32, e2623. [Google Scholar] [CrossRef]
- Huls, H.; Abdulahad, S.; van de Loo, A.J.A.E.; Mackus, M.; Roehrs, T.; Roth, T.; Verster, J.C. Inclusion and exclusion criteria of clinical trials for insomnia. J. Clin. Med. 2018, 7, 206. [Google Scholar] [CrossRef] [Green Version]
- Sulzer, T.A.; Kraneveld, A.D.; Garssen, J.; Verster, J.C. Early life exposome pressure on later life immune fitness: A layman’s perspective. Eur. Neuropsychopharmacol. 2019, 29, S204–S205. [Google Scholar] [CrossRef]
- World Health Organization. The World Health Organization BMI Classification. Available online: https://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 1 November 2020).
- Centraal Bureau Voor de Statistiek (CBS). Wat is Het Verschil Tussen Een Westerse en Niet-Westerse Allochtoon? Available online: https://www.cbs.nl/nl-nl/faq/specifiek/wat-is-het-verschil-tussen-een-westerse-en-niet-westerse-allochtoon (accessed on 5 October 2020).
- Centraal Bureau Voor de Statistiek (CBS). Opleidingsniveau. Available online: https://www.cbs.nl/nl-nl/nieuws/2019/33/verschil-levensverwachting-hoog-en-laagopgeleid-groeit/opleidingsniveau (accessed on 5 October 2020).
- Centraal Bureau voor de Statistiek (CBS). Uurlonen van Werknemers Naar Beroepsgroep. Available online: https://www.cbs.nl/nl-nl/maatwerk/2017/48/uurlonen-van-werknemers-naar-beroepsgroep-2016 (accessed on 5 October 2020).
- Bhattacharya, A. Financial Headache. The Cost of Workplace Hangovers and Intoxication to the UK Economy; IAS: London, UK, 2019; Available online: http://www.ias.org.uk/uploads/pdf/IAS%20reports/rp35062019.pdf (accessed on 5 October 2020).
- National Institute for Public Health and the Environment (RIVM). Aandoeningen. Welke Aandoeningen Hebben We in De Toekomst? Available online: https://www.vtv2018.nl/aandoeningen (accessed on 5 October 2020).
- McNair, D.M.; Lorr, M.; Droppleman, L.F. Manual for the Profile of Mood States; Educational and Industrial Testing Service: San Diego, CA, USA, 1971. [Google Scholar]
- De Boer, A.G.; van Lanschot, J.J.; Stalmeier, P.F.; van Sandick, J.W.; Hulscher, J.B.; de Haes, J.C.; Sprangers, M.A. Is a single-item visual analogue scale as valid, reliable and responsive as multi-item scales in measuring quality of life? Qual. Life Res. 2004, 13, 311–320. [Google Scholar] [CrossRef]
- Killgore, W.D. The visual analogue mood scale: Can a single-item scale accurately classify depressive mood state? Psychol. Rep. 1999, 85, 1238–1243. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, F. Fatigue assessments in rheumatoid arthritis: Comparative performance of visual analog scales and longer fatigue questionnaires in 7760 patients. J. Rheumatol. 2004, 31, 1896–1902. [Google Scholar]
- Verster, J.C.; van de Loo, A.J.A.E.; Benson, S.; Scholey, A.; Stock, A.-K. The assessment of overall hangover severity. J. Clin. Med. 2020, 9, 786. [Google Scholar] [CrossRef] [Green Version]
- Baars, T.; Berge, C.; Garssen, J.; Verster, J.C. Effect of raw milk consumption on perceived health, mood and immune functioning among US adults with a poor and normal health: A retrospective questionnaire based study. Complement. Ther. Med. 2019, 47, 102196. [Google Scholar] [CrossRef]
- Baars, T.; Berge, C.; Garssen, J.; Verster, J.C. The impact of raw fermented milk products on perceived health and mood among Dutch adults. Nutr. Food Sci. 2019, 49, 1195–1206. [Google Scholar] [CrossRef]
- Verster, J.C.; Arnoldy, L.; van de Loo, A.J.A.E.; Benson, S.; Scholey, A.; Stock, A.-K. The impact of mood and subjective intoxication on hangover severity. J. Clin. Med. 2020, 9, 2462. [Google Scholar] [CrossRef]
- Ahorsu, D.K.; Lin, C.-Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The fear of COVID-19 scale: Development and initial validation. Int. J. Ment. Health Addict. 2020, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Wilod Versprille, L.J.F.; van de Loo, A.J.A.E.; Mackus, M.; Arnoldy, L.; Sulzer, T.A.L.; Vermeulen, S.A.; Abdulahad, S.; Huls, H.; Baars, T.; Kraneveld, A.D.; et al. Development and validation of the Immune Status Questionnaire (ISQ). Int. J. Environ. Res. Public Health 2019, 16, 4743. [Google Scholar] [CrossRef] [Green Version]
- Van Schrojenstein Lantman, M.; Otten, L.S.; Mackus, M.; de Kruijff, D.; van de Loo, A.J.A.E.; Kraneveld, A.D.; Garssen, J.; Verster, J.C. Mental resilience, perceived immune functioning, and health. J. Multidiscip. Healthc. 2017, 10, 107–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, G.G.; Dowling, H.F.; Spiesman, I.G.; Boand, A.V. Transmission of the common cold to volunteers under controlled conditions. I. The common cold as a clinical entity. Arch. Int. Med. 1958, 101, 267–278. [Google Scholar] [CrossRef]
- Sobell, L.C.; Agrawal, S.; Sobell, M.B.; Leo, G.I.; Young, L.Y.; Cunningham, J.A.; Simco, E.R. Comparison of a quick drinking screen with the timeline followback for individuals with alcohol problems. J. Stud. Alcohol 2003, 64, 858–861. [Google Scholar] [CrossRef] [Green Version]
- Watson, P.E.; Watson, I.D.; Batt, R.D. Prediction of blood alcohol concentrations in human subjects. Updating the Widmark Equation. J. Stud. Alcohol Drugs 1981, 42, 547–556. [Google Scholar] [CrossRef] [PubMed]
- Van de Loo, A.J.A.E.; van Andel, N.; van Gelder, C.A.G.H.; Janssen, B.S.G.; Titulaer, J.; Jansen, J.; Verster, J.C. The effects of alcohol mixed with energy drink (AMED) on subjective intoxication and alertness: Results from a double-blind placebo-controlled clinical trial. Hum. Psychopharmacol. 2016, 31, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Ruscheweyh, R.; Marziniak, M.; Stumpenhorst, F.; Reinholz, J.; Knecht, S. Pain sensitivity can be assessed by self-rating: Development and validation of the pain sensitivity questionnaire. Pain 2009, 146, 65–74. [Google Scholar] [CrossRef]
- Ruscheweyh, R.; Verneuer, B.; Dany, K.; Marziniak, M.; Wolowski, A.; Çolak-Ekici, R.; Schulte, T.L.; Bullmann, V.; Grewe, S.; Gralow, I.; et al. Validation of the pain sensitivity questionnaire in chronic pain patients. Pain 2012, 153, 1210–1218. [Google Scholar] [CrossRef] [PubMed]
- Melotti, R.; Ruscheweyh, R.; Pramstaler, P.P.; Hicks, A.A.; Pattaro, C. Structural consistency of the Pain Sensitivity Questionnaire in the Cooperative Health Research in South Tyrol (CHRIS) population-based study. J. Pain 2018, 19, 1424–1434. [Google Scholar] [CrossRef] [Green Version]
- Gebhart, G.F.; Schmidt, R.F. Pain Catastrophizing. In Encyclopedia of Pain; Springer: Berlin/Heidelberg, Germany, 2013. [Google Scholar] [CrossRef]
- Darnall, B.D.; Sturgeon, J.A.; Cook, K.F.; Taub, C.J.; Roy, A.; Burns, J.W.; Sullivan, M.; Mackey, S.C. Development and validation of a daily pain catastrophizing scale. J. Pain 2017, 18, 1139–1149. [Google Scholar] [CrossRef] [PubMed]
- Crombez, G.; Vlaeyen, J.W.S.; Heuts, P.H.T.G.; Lysens, R. Pain-Related fear is more disabling than pain itself: Evidence on the role of pain-related fear in chronic low back pain disability. Pain 1999, 80, 329–339. [Google Scholar] [CrossRef]
- Von Korff, M.; Ormel, J.; Keefe, F.J.; Dworkin, S.F. Grading the severity of chronic pain. Pain 1992, 50, 133–149. [Google Scholar] [CrossRef]
- Von Korff, M.; DeBar, L.L.; Krebs, E.E.; Kerns, R.D.; Deyo, R.A.; Keefe, F.J. Graded chronic pain scale revised: Mild, bothersome, and high-impact chronic pain. Pain 2020, 161, 651–661. [Google Scholar] [CrossRef] [PubMed]
- Zorginstituut Nederland. Farmacotherapeutisch Kompas. Available online: https://www.farmacotherapeutischkompas.nl/ (accessed on 5 October 2020).
- Nederlands Huisartsen Genootschap (NHG). Pijn. Available online: https://richtlijnen.nhg.org/standaarden/pijn (accessed on 5 October 2020).
- Wilson, D.M.C.; Ciliska, D. Development and use of the FANTASTIC checklist. Can. Fam. Physician 1984, 30, 1527–1532. [Google Scholar]
- Sharratt, J.K.; Sharratt, M.T.; Smith, D.M.; Howell, N.J.; Davenport, L. FANTASTIC Lifestyle survey of University of Waterloo employees. Can. Fam. Physician 1984, 30, 1869–1872. [Google Scholar]
- Wilson, D.M.C.; Nielsen, E.; Ciliska, D. Lifestyle assessment: Testing the FANTASTIC Instrument. Can. Fam. Physician 1984, 30, 1863–1866. [Google Scholar]
- Canadian Society for Exercise Physiology. Fantastic Lifestyle Checklist. Available online: https://rowingbc.ca/wp-content/uploads/2016/12/Fantastic-Lifestyle-Checklist.pdf (accessed on 10 October 2020).
- Smith, B.W.; Wiggins, K.; Dalen, J.; Bernard, J. Brief Resilience Scale: Assessing the ability to bounce back. Int. J. Behav. Med. 2008, 15, 194–200. [Google Scholar] [CrossRef]
- Sanderman, R.; Eysenck, S.B.G.; Arrindell, W.A. Crosscultural comparison of personality traits: The Netherlands and England. Psychol. Rep. 1991, 69, 1091–1096. [Google Scholar] [CrossRef]
- Sanderman, R.; Arrindell, W.A.; Ranchor, A.V.; Eysenck, H.J.; Eysenck, S.B.G. Het Meten van Persoonlijkheidskenmerken Met de Eysenck Personality Questionnaire (EPQ), Een Handleiding. Tweede Herziene Druk; UMCG/Rijksuniversiteit Groningen, Research Institute SHARE: Groningen, The Netherlands, 2012. [Google Scholar]
- Balikji, S.; Mackus, M.; Brookhuis, K.; Garssen, J.; Kraneveld, A.D.; Roth, T.; Verster, J.C. The association of sleep, perceived immune functioning, and irritable bowel syndrome. J. Clin. Med. 2018, 7, 238. [Google Scholar] [CrossRef] [Green Version]
- Mullol, J.; Alobid, I.; Mariño-Sánchez, F.; Izquierdo-Domínguez, A.; Marin, C.; Klimek, L.; Wang, D.-Y.; Liu, Z. The loss of smell and taste in the COVID-19 outbreak: A tale of many countries. Curr. Allergy Asthma Rep. 2020, 20, 61. [Google Scholar] [CrossRef]
- Zhao, Y.; Cao, Y.; Wang, S.; Cai, K.; Xu, K. COVID-19 and gastrointestinal symptoms. BJS Open 2020, 107, e382–e383. [Google Scholar] [CrossRef]
- Liu, G.; Zong, G.; Doty, R.L.; Sun, Q. Prevalence and risk factors of taste and smell impairment in a nationwide representative sample of the US population: A cross-sectional study. BMJ Open 2016, 6, e013246. [Google Scholar] [CrossRef] [Green Version]
- Verster, J.C.; Tiplady, B.; McKinney, A. Mobile technology and naturalistic study designs in addiction research. Curr. Drug Abus. Rev. 2012, 5, 169–171. [Google Scholar] [CrossRef]
- Ammar, A.; Bouaziz, B.; Trabelsi, K.; Glenn, J.; Zmijewski, P.; Müller, P.; Chtourou, H.; Jmaiel, M.; Chamari, K.; Driss, T.; et al. Applying digital technology to promote active and healthy confinement lifestyle during pandemics in the elderly. Biol. Sport 2021, 38, 391–396. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Questionnaire/Scale | 2019 | Before Lockdown | During Lockdown | Moment of Survey Completion |
|---|---|---|---|---|
| Demographics | - | - | - | √ |
| Education | - | - | - | √ |
| Employment status | √ | - | √ | - |
| Work and immune fitness | √ | - | - | - |
| Work and pain | √ | - | - | - |
| Work and alcohol hangover | √ | - | - | - |
| Underlying diseases | - | - | - | √ |
| The use of medicines | - | √ | √ | - |
| Mood and quality of life | - | √ | √ | - |
| Fear of COVID-19 (FCV-19S) | - | - | √ | √ |
| Immune Status Questionnaire (ISQ) | √ | - | - | - |
| Perceived immune fitness | √ | √ | √ | √ |
| The Jackson Symptoms scale—common cold | - | √ | √ | - |
| COVID-19 Symptoms Scale (C-19SS) | - | √ | √ | - |
| COVID-19 test | - | - | - | √ |
| Alcohol consumption | - | √ | √ | |
| Pain Sensitivity Questionnaire (PSQ) | - | - | - | √ |
| Pain catastrophizing scale (PCS) | - | - | - | √ |
| Graded Chronic Pain Scale—Revised (GCPS-R) | - | - | - | √ |
| Use of pain medication | √ | - | √ | - |
| The FANTASTIC Lifestyle Checklist | - | √ | √ | - |
| Mental resilience | - | - | - | √ |
| Personality | - | - | - | √ |
| Questionnaire/Scale | Description in Section | Number of Participants |
|---|---|---|
| Part 1 of the survey | ||
| Demographics | 2.2.1 | 1910 |
| Education | 2.2.2 | 1910 |
| Employment status | 2.2.2 | 907 |
| Work and immune fitness | 2.2.2 | 495 |
| Work and pain | 2.2.2 | 238 |
| Work and alcohol hangover | 2.2.2 | 364 |
| Underlying diseases | 2.2.3 | 1378 |
| The use of medicines | 2.2.4 | 1415 |
| Mood and quality of life | 2.2.5 | 1415 |
| Fear of COVID-19 (FCV-19S) | 2.2.6 | 1020 |
| Immune Status Questionnaire (ISQ) | 2.2.7 | 1408 |
| Perceived immune fitness | 2.2.8 | 1020 |
| The Jackson Symptoms scale—common cold | 2.2.9 | 1020 |
| COVID-19 Symptoms Scale (C-19SS) | 2.2.10 | 1020 |
| COVID-19 test | 2.2.11 | 1009 |
| Alcohol consumption | 2.2.12 | 761 |
| Pain Sensitivity Questionnaire (PSQ) | 2.2.13 | 910 |
| Pain catastrophizing scale (PCS) | 2.2.14 | 910 |
| Graded Chronic Pain Scale—Revised (GCPS-R) | 2.2.15 | 495 |
| Use of pain medication | 2.2.16 | 495 |
| Part 2 of the survey | ||
| The FANTASTIC Lifestyle Checklist | 2.2.17 | 514 |
| Mental resilience | 2.2.18 | 511 |
| Personality | 2.2.19 | 505 |
| Variable | Study Outcome |
|---|---|
| Male/Female | 687 (36.0%)/1223 (64.0%) |
| Age (years) | 46.3 (18.5) |
| Weight (kg) | 79.2 (18.6) |
| Height (m) | 1.73 (0.1) |
| BMI (kg/m2) | 26.5 (5.8) |
| Ethnicity—Dutch | 1796 (94.0%) |
| —Migration background | 114 (6.0%) |
| Educational level—Low | 694 (36.4%) |
| —Middle | 502 (26.3%) |
| —High | 713 (37.3%) |
| Employment status—Unemployed | 146 (16.1%) |
| —Employer/employee | 262 (39.1%) |
| —Student | 86 (9.5%) |
| —Student with parttime job | 153 (16.9%) |
| —Retired | 160 (17.6%) |
| Underlying disease—Yes | 893 (64.8%) |
| —No | 485 (35.2%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kiani, P.; Merlo, A.; Saeed, H.M.; Benson, S.; Bruce, G.; Hoorn, R.; Kraneveld, A.D.; van de Loo, A.J.A.E.; Severeijns, N.R.; Sips, A.S.M.; et al. Immune Fitness and the Psychosocial and Health Consequences of the COVID-19 Pandemic Lockdown in The Netherlands: Methodology and Design of the CLOFIT Study. Eur. J. Investig. Health Psychol. Educ. 2021, 11, 199-218. https://doi.org/10.3390/ejihpe11010016
Kiani P, Merlo A, Saeed HM, Benson S, Bruce G, Hoorn R, Kraneveld AD, van de Loo AJAE, Severeijns NR, Sips ASM, et al. Immune Fitness and the Psychosocial and Health Consequences of the COVID-19 Pandemic Lockdown in The Netherlands: Methodology and Design of the CLOFIT Study. European Journal of Investigation in Health, Psychology and Education. 2021; 11(1):199-218. https://doi.org/10.3390/ejihpe11010016
Chicago/Turabian StyleKiani, Pantea, Agnese Merlo, Hama M. Saeed, Sarah Benson, Gillian Bruce, Rosalie Hoorn, Aletta D. Kraneveld, Aurora J. A. E. van de Loo, Noortje R. Severeijns, Annabel S. M. Sips, and et al. 2021. "Immune Fitness and the Psychosocial and Health Consequences of the COVID-19 Pandemic Lockdown in The Netherlands: Methodology and Design of the CLOFIT Study" European Journal of Investigation in Health, Psychology and Education 11, no. 1: 199-218. https://doi.org/10.3390/ejihpe11010016
APA StyleKiani, P., Merlo, A., Saeed, H. M., Benson, S., Bruce, G., Hoorn, R., Kraneveld, A. D., van de Loo, A. J. A. E., Severeijns, N. R., Sips, A. S. M., Scholey, A., Garssen, J., & Verster, J. C. (2021). Immune Fitness and the Psychosocial and Health Consequences of the COVID-19 Pandemic Lockdown in The Netherlands: Methodology and Design of the CLOFIT Study. European Journal of Investigation in Health, Psychology and Education, 11(1), 199-218. https://doi.org/10.3390/ejihpe11010016