


Psychological Predictors of COVID-19-Related Anxiety in Vulnerable Groups

Abstract
:1. Introduction
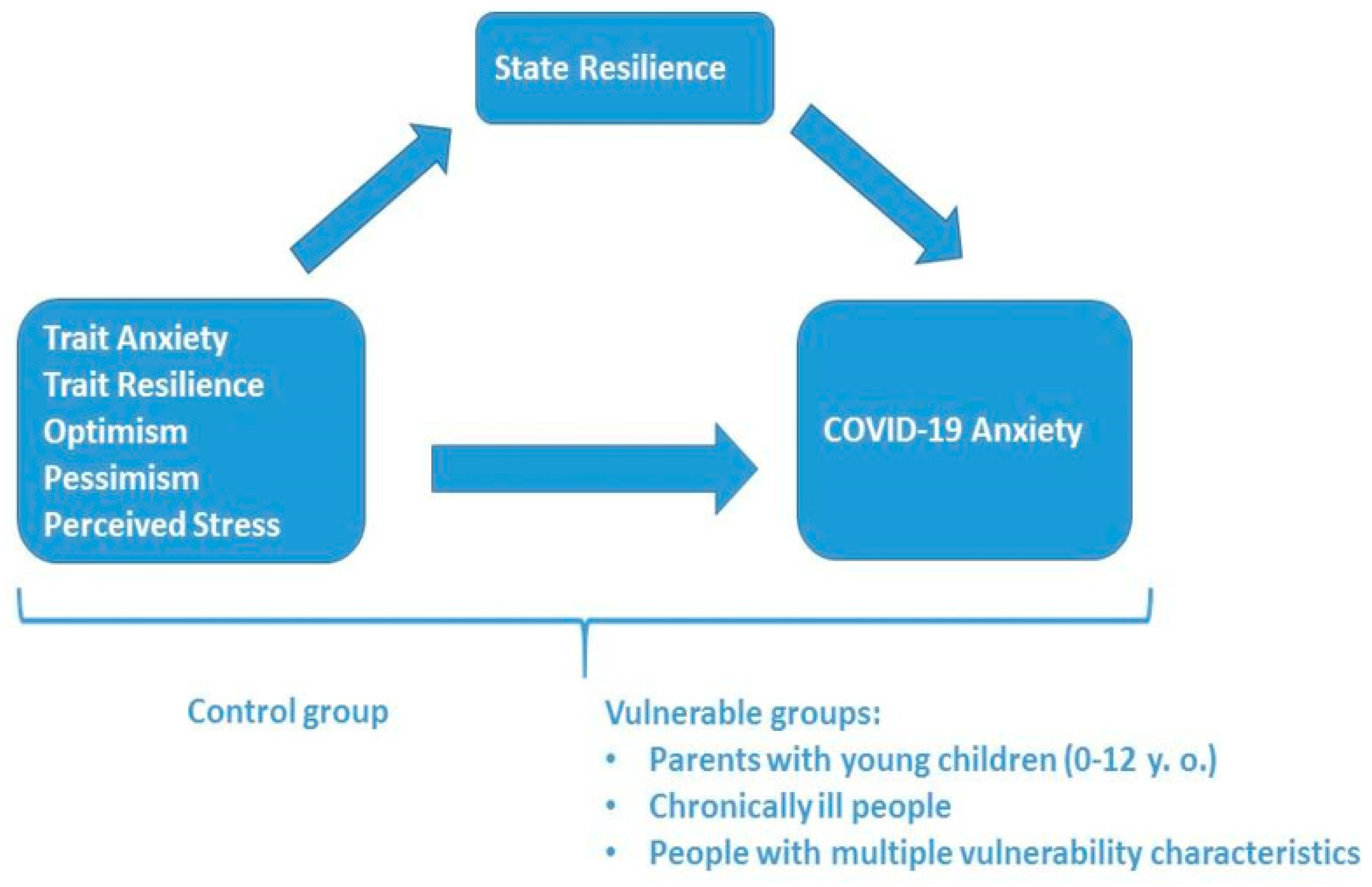
Research Hypotheses
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measures and Scales
- A short 3-item version of the Perceived Stress Scale (PSS) of Cohen, Kamarck and Mermelstein [70], a Bulgarian adaptation [14,71] that measured the degree to which people perceived their experiences “in the last 2 weeks” as stressful, unpredictable and uncontrollable on a 5-point Likert scale (1—It did not happen at all; 5—It happened very often, nearly every day). The following items were included: “In the last two weeks, how often have you felt that you were unable to control the important things in your life?”, “In the last two weeks, how often have you felt that things were going your way?” and “In the last two weeks, how often have you felt difficulties were piling up so high that you could not overcome them?”. Cronbach’s Alpha for the 3-item PSS was 0.70. The single-component structure was confirmed using PCA with 63.3% of the variance explained, as well as moderate inter-item correlations (0.61 > r > 0.34).
- Scales for Optimistic and Pessimistic Expectations—short versions of Scales for Generalized Expectations [72] were used based on previous publications [73]. Each scale consists of three items: “I’m a person who believes that there is a good way out of difficulties“, “I’m a person who looks at life optimistically“ and “I’m convinced that bad situations don’t last long“ (optimistic expectations, Cronbach’s α = 0.83) and “I’m more prepared for the worst because I think that it happens more often“, “There are very few pleasant things in life“ and “I think that one unpleasant thing usually leads to another” (pessimistic expectations, Cronbach’s α = 0.73). The statements were evaluated on a 5-point Likert scale (1—strongly disagree; 5—strongly agree). The two-factor structure was confirmed using PCA with 69.9% of the variance explained. Moderate-to-strong inter-item correlations (0.65 > r > 0.58 for the optimistic expectations scale; 0.57 > r > 0.38 for the pessimistic expectations scale) were found.
- A short 9-item version of the State–Trait Assessment of Resilience Scale (STARS) [74]. The original STARS is a 13-item scale with a 5-point Likert scale (1—disagree; 5—strongly agree) where state resilience refers to a person’s experience in a given situation, whilst trait resilience is a stable personality characteristic. Cronbach’s Alpha for the nine items was 0.89, for resilience state—α = 0.87 and for resilience trait—α = 0.77. The two-component structure was confirmed using PCA with 65.2% of the variance explained. Moderate-to-strong inter-item correlations (0.55 > r > 0.38 for the trait resilience scale; 0.78 > r > 0.47 for the state resilience scale) were found.
- A short version of the Spielberger state–trait anxiety inventory: Anxiety (Trait) [75]—the trait anxiety measures how one generally feels with 5 items on a 4-point Likert scale (1—not at all; 4—very much so). Cronbach’s Alpha for this study was 0.88. The single-factor structure was confirmed using PCA with 67.9% of the variance explained, as well as moderate-to-strong inter-item correlations (0.77 > r > 0.50).
- An 8-item version of the COVID-19 Anxiety Syndrome Scale (C-19ASS) by Ana V. Nikčević and Marcantonio M. Spada [76]—the original scale consists of nine items with 5-point Likert scale (0—not at all; 4—nearly every day). C-19ASS measures the way people cope with the COVID-19 threat. Cronbach’s Alpha for the eight-item version was 0.90. The single-component structure was confirmed using PCA with 58.2% of the variance explained, as well as moderate-to-strong inter-item correlations (0.68 > r > 0.39).
2.3. Statistical Methods and Procedure
3. Results
- For chronic sufferers, only trait anxiety was found to be a weak positive predictor—R2 = 0.079, F(1, 145) = 12.36, p = 0.001—which explained 7.9% of the variance in COVID-19-related anxiety.
- For working parents with young children, only perceived stress turned out a weak positive predictor—R2 = 0.049, F(1, 133) = 6.78, p = 0.010—which explained 4.9% of the variance in COVID-19-related anxiety.
- For the group of respondents with multiple vulnerability characteristics, both trait anxiety and perceived stress were found to be moderate positive predictors—R2 = 0.234, F(2, 138) = 20.74, p = 0.000— which together explained 23.4% of the construct variance.
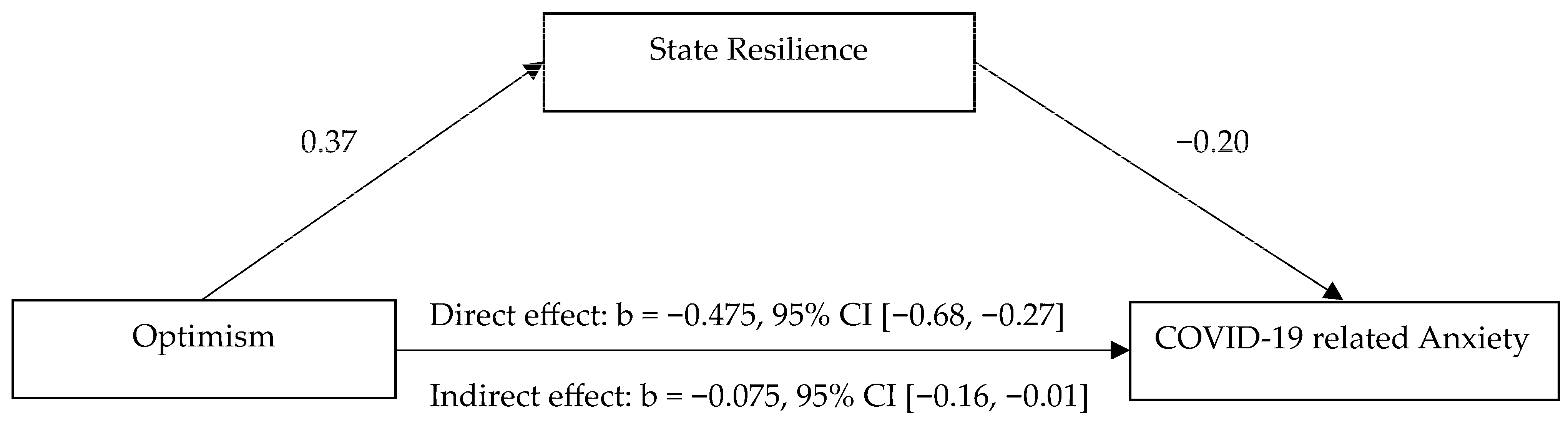
- For the control group, trait resilience turned out to be a moderate negative predictor—R2 = 0.269, F(1, 99) = 36.12, p = 0.000—which explained 26.9% of the variance. At the same time, optimism and perceived stress together explained 32.8% of the variance in COVID-19 anxiety—R2 = 0.328, F(2, 99) = 23.68, p = 0.000. It is important to note that the main effect of trait resilience was studied separately from the other factors due to multicollinearity (condition index > 30).
4. Discussion
5. Conclusions
- State resilience mediated the negative effect of optimism on COVID-19 anxiety and helped to alleviate it in the group with no self-reported vulnerabilities.
- Trait anxiety and perceived stress had a more significant role in the group with multiple vulnerabilities, compared to the other vulnerable groups—chronic sufferers and working parents with young children.
- Significant between-group differences were observed for pessimism. Chronic sufferers had higher pessimism compared to the group of working parents with young children.
- Trait resilience and optimistic expectations for the studied vulnerable groups did not have a direct relieving effect on their COVID-19 anxiety, while pessimism did not directly exacerbate the COVID-19 anxiety in the group of people with no indicated vulnerability.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fiorillo, A.; Gorwood, P. The consequences of the COVID-19 pandemic on mental health and implications for clinical practice. Eur. Psychiatry 2020, 63, E32. [Google Scholar] [CrossRef]
- Costanza, A.; Macheret, L.; Folliet, A.; Amerio, A.; Aguglia, A.; Serafini, G.; Prada, P.; Bondolfi, G.; Sarasin, F.; Ambrosetti, J. COVID-19 related fears of patients admitted to a psychiatric emergency department during and post-lockdown in Switzerland: Preliminary findings to look ahead for tailored preventive mental health strategies. Medicina 2021, 57, 1360. [Google Scholar] [CrossRef]
- Misheva, V.; Hristova, A.; Palm, F.; Nacheva, I.; Hopstadius, M.; Blasko, A. Framing the “Exceptions to the Rule” in Analyses of Responses to the First Wave of the COVID-19 Pandemic. In Crisis and the Culture of Fear and Anxiety in Contemporary Europe; Llena, C.Z., Stier, J., Gray, B., Eds.; Routledge: Abingdon, UK; New York, NY, USA, 2023; pp. 203–223. [Google Scholar] [CrossRef]
- Eurostat—Purchasing Power Parities and GDP per Capita—Flash Estimate. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Purchasing_power_parities_and_GDP_per_capita_-_flash_estimate&oldid=559318 (accessed on 1 August 2023).
- Rangachev, A.; Marinov, G.K.; Mladenov, M. The impact and progression of the COVID-19 pandemic in Bulgaria in its first two years. Vaccines 2022, 10(11), 1901. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Overview of the Implementation of COVID-19 Vaccination Strategies and Deployment Plans in the EU/EEA. 11 November 2021; Technical Report; ECDC: Stockholm, Sweden, 2021; Available online: https://www.ecdc.europa.eu/sites/default/files/documents/COVID-19-vaccination-strategies-and-deployment-plans-Nov-2021.pdf (accessed on 2 August 2023).
- Steinert, J.I.; Sternberg, H.; Prince, H.; Fasolo, B.; Galizzi, M.M.; Büthe, T.; Veltri, G.A. COVID-19 vaccine hesitancy in eight European countries: Prevalence, determinants, and heterogeneity. Sci. Adv. 2022, 8, eabm9825. [Google Scholar] [CrossRef]
- Toshkov, D. What accounts for the variation in COVID-19 vaccine hesitancy in Eastern, Southern and Western Europe? Vaccine 2023, 41, 3178–3188. [Google Scholar] [CrossRef]
- Džakula, A.; Banadinović, M.; Lovrenčić, I.L.; Vajagić, M.; Dimova, A.; Rohova, M.; Minev, M.; Scintee, S.G.; Vladescu, C.; Farcasanu, D.; et al. A comparison of health system responses to COVID-19 in Bulgaria, Croatia and Romania in 2020. Health Policy 2022, 126, 456–464. [Google Scholar] [CrossRef]
- Ten Have, H.; Gordijn, B. Vulnerability in light of the COVID-19 crisis. Med. Health Care Philos. 2021, 24, 153–154. [Google Scholar] [CrossRef]
- Gray, D.M.; Anyane-Yeboa, A.; Balzora, S.; Issaka, R.B.; May, F.P. COVID-19 and the other pandemic: Populations made vulnerable by systemic inequity. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 520–522. [Google Scholar] [CrossRef]
- Wirkner, J.; Christiansen, H.; Knaevelsrud, C.; Lüken, U.; Wurm, S.; Schneider, S.; Brakemeier, E.L. Mental health in times of the COVID-19 pandemic: Current knowledge and implications from a European perspective. Eur. Psychol. 2021, 26, 310–322. [Google Scholar] [CrossRef]
- Rudert, S.C.; Gleibs, I.H.; Gollwitzer, M.; Häfner, M.; Hajek, K.V.; Harth, N.S.; Schneider, D. Us and the virus: Understanding the COVID-19 pandemic through a social psychological lens. Eur. Psychol. 2021, 26, 259–271. [Google Scholar] [CrossRef]
- Hristova, A.; Karastoyanov, G. Stress and coping strategies during the first wave of COVID-19 in Bulgaria. Psychol. Res. (Balkans) 2022, 24, 5–22. [Google Scholar]
- Paunova-Markova, E. Perceived threats and difficulties of mothers of young children during a state of emergency in a COVID-19 pandemic. Psychol. Res. 2020, 23, 84–108. [Google Scholar]
- Paunova-Markova, E. Perceived threats and difficulties of mothers of young children after 9 months in a COVID-19 pandemic. Psychol. Res. 2022, 25, 109–127. [Google Scholar] [CrossRef]
- Maeva, M. Family Well-Being during the COVID-19 Pandemic in Bulgaria. Psychol. Res. 2022, 25, 128–137. [Google Scholar] [CrossRef]
- Panchelieva, T.; Nacheva, I.; Bakalova, D. Socio-economic Aspects of the Crisis Caused by COVID-19: Effects of the Change in the Work Regime. Econ. Altern. 2023, accepted. [Google Scholar]
- Nacheva, I.; Panchelieva, T.; Bakalova, D. Emotional Experiences of Vulnerable Groups during COVID-19. Eur. J. Psychol. Open 2023. [CrossRef]
- Babore, A.; Trumello, C.; Lombardi, L.; Candelori, C.; Chirumbolo, A.; Cattelino, E.; Baiocco, R.; Bramanti, S.M.; Viceconti, M.L.; Pignataro, S.; et al. Mothers’ and Children’s Mental Health during the COVID-19 Pandemic Lockdown: The Mediating Role of Parenting Stress. Child Psychiatry Hum. Dev. 2023, 54, 134–146. [Google Scholar] [CrossRef]
- Wu, M.; Xu, W.; Yao, Y.; Zhang, L.; Guo, L.; Fan, J.; Chen, J. Mental health status of students’ parents during COVID-19 pandemic and its influence factors. Gen. Psychiatry 2020, 33, e100250. [Google Scholar] [CrossRef]
- Schieman, S.; Badawy, P.J.; Milkie, M.A.; Bierman, A. Work-life conflict during the COVID-19 pandemic. Socius 2021, 7, 2378023120982856. [Google Scholar] [CrossRef]
- World Health Organization—Disability Considerations during the COVID-19 Outbreak. Available online: https://www.who.int/who-documents-detail/disability-considerations-during-the-covid-19-outbreak (accessed on 5 August 2023).
- Saqib, M.; Siddiqui, S.; Qasim, M.; Jamil, M.; Rafique, J.; Awan, U.; Ahmad, H.; Afzal, M. Effect of COVID-19 lockdown on patients with chronic diseases. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 1621–1623. [Google Scholar] [CrossRef]
- Budu, M.O.; Rugel, E.J.; Nocos, R.; Teo, K.; Rangarajan, S.; Lear, S.A. Psychological Impact of COVID-19 on People with Pre-Existing Chronic Disease. Int. J. Environ. Res. Public Health 2021, 18, 5972. [Google Scholar] [CrossRef]
- Mihashi, M.; Otsubo, Y.; Yinjuan, X.; Nagatomi, K.; Hoshiko, M.; Ishitake, T. Predictive factors of psychological disorder development during recovery following SARS outbreak. Health Psychol. 2009, 28, 91–100. [Google Scholar] [CrossRef]
- Blustein, D.L.; Guarino, P.A. Work and unemployment in the time of COVID-19: The existential experience of loss and fear. J. Humanist. Psychol. 2020, 60, 702–709. [Google Scholar] [CrossRef]
- Rodríguez, S.; Valle, A.; Piñeiro, I.; Rodríguez-Llorente, C.; Guerrero, E.; Martins, L. Sociodemographic characteristics and stress of people from Spain confined by COVID-19. Eur. J. Investig. Health Psychol. Educ. 2020, 10, 1095–1105. [Google Scholar] [CrossRef] [PubMed]
- Kučera, D.; Stuchlíková, I.; Mrhálek, T. Impacts of COVID-19 pandemic on the mental health of working adults in the Czech Republic: Analysis of self-report psychological data in a one year perspective. Eur. J. Investig. Health Psychol. Educ. 2021, 11, 1061–1072. [Google Scholar] [CrossRef]
- Pettinicchio, D.; Maroto, M.; Chai, L.; Lukk, M. Findings from an online survey on the mental health effects of COVID-19 on Canadians with disabilities and chronic health conditions. Disabil. Health J. 2021, 14, 101085. [Google Scholar] [CrossRef] [PubMed]
- Gruchoła, M.; Sławek-Czochra, M. “The culture of fear” of inhabitants of EU countries in their reaction to the COVID-19 pandemic—A study based on the reports of the Eurobarometer. Saf. Sci. 2021, 135, 105140. [Google Scholar] [CrossRef]
- American Psychology Association (n.d.). Anxiety. Available online: https://www.apa.org/topics/anxiety (accessed on 3 August 2023).
- Lecic-Tosevski, D.; Vukovic, O.; Stepanovic, J. Stress and personality. Psychiatriki 2011, 22, 20–29. [Google Scholar]
- Cohen, S. Perceived Stress in a Probability Sample of the United States; Sage: New York, NY, USA, 1988. [Google Scholar]
- Maunder, R.G.; Leszcz, M.; Savage, D.; Adam, M.A.; Peladeau, N.; Romano, D.; Rose, M.; Schulman, R.B. Applying the lessons of SARS to pandemic influenza: An evidence-based approach to mitigating the stress experienced by healthcare workers. Can. J. Public Health 2008, 99, 486–488. [Google Scholar] [CrossRef] [PubMed]
- Walker, B.H.; Anderies, J.M.; Kinzig, A.P.; Ryan, P. Exploring resilience in social-ecological systems through comparative studies and theory development: Introduction to the special issue. Ecol. Soc. 2006, 11, 12. Available online: https://www.jstor.org/stable/26267774 (accessed on 13 August 2023). [CrossRef]
- Sheerin, C.M.; Lind, M.J.; Brown, E.A.; Gardner, C.O.; Kendler, K.S.; Amstadter, A.B. The impact of resilience and subsequent stressful life events on MDD and GAD. Depress. Anxiety 2018, 35, 140–147. [Google Scholar] [CrossRef]
- Barzilay, R.; Moore, T.M.; Greenberg, D.M.; DiDomenico, G.E.; Brown, L.A.; White, L.K.; Gur, R.C.; Gur, R.E. Resilience, COVID-19-related stress, anxiety and depression during the pandemic in a large population enriched for healthcare providers. Transl. Psychiatry 2020, 10, 291. [Google Scholar] [CrossRef] [PubMed]
- Yıldırım, M.; Solmaz, F. COVID-19 burnout, COVID-19 stress and resilience: Initial psychometric properties of COVID-19 Burnout Scale. Death Stud. 2022, 46, 524–532. [Google Scholar] [CrossRef] [PubMed]
- Conversano, C.; Rotondo, A.; Lensi, E.; Vista, O.; Arpone, V.; Reda, M. Optimism and Its Impact on Mental and Physical Well-Being. Clin. Pract. Epidemiol. Ment. Health 2010, 6, 25–29. [Google Scholar] [CrossRef]
- Tiger, L. Optimism: The Biology of Hope; Simon & Schuster: New York, NY, USA, 1979. [Google Scholar]
- Argyle, M. Causes and Correlates of Happiness. In Well-Being: The Foundations of Hedonic Psychology; Kahneman, D., Diener, E., Schwarz, N., Eds.; Russell Sage Foundation: New York, NY, USA, 1999; pp. 353–373. [Google Scholar]
- Peterson, C. The future of optimism. Am. Psychol. 2000, 55, 44–55. [Google Scholar] [CrossRef] [PubMed]
- Scheier, M.F.; Carver, C.S. Optimism, coping, and health: Assessment and implications of generalized outcome expectancies. Health Psychol. 1985, 4, 219–247. [Google Scholar] [CrossRef] [PubMed]
- Lench, H. Personality and health outcomes: Making positive expectations a reality. J. Happiness Stud. 2011, 12, 493–507. [Google Scholar] [CrossRef]
- Biber, D.D.; Melton, B.; Czech, D.R. The impact of COVID-19 on college anxiety, optimism, gratitude, and course satisfaction. J. Am. Coll. Health 2022, 70, 1947–1952. [Google Scholar] [CrossRef]
- Carver, C.S.; Scheier, M.F.; Segerstrom, S.C. Optimism. Clin. Psychol. Rev. 2010, 30, 879–889. [Google Scholar] [CrossRef]
- Yıldırım, M. Optimism as a predictor of flourishing over and above the big five among youth. In Proceedings of the 4th International Academic Studies Conference, Istanbul, Turkey, 10–12 October 2019. [Google Scholar]
- Hanssen, M.M.; Vancleef, L.M.G.; Vlaeyen, J.W.S.; Peters, M.L. More optimism, less pain! The influence of generalized and pain-specific expectations on experienced cold-pressor pain. J. Behav. Med. 2014, 37, 47–58. [Google Scholar] [CrossRef]
- Alves, M.P.; Costa, V.; Cunha, A.I.; Carvalho, P.; Loureiro, M.J. Optimism and fear of COVID-19 in higher education students: The mediating role of general anxiety. Psychol. Health Med. 2023, 28, 241–252. [Google Scholar] [CrossRef]
- Shevlin, M.; McBride, O.; Murphy, J.; Miller, J.G.; Hartman, T.K.; Levita, L.; Mason, L.; Martinez, A.P.; McKay, R.; Stocks, T.V.A.; et al. Anxiety, depression, traumatic stress and COVID-19-related anxiety in the UK general population during the COVID-19 pandemic. BJPsych Open 2020, 6, e125. [Google Scholar] [CrossRef] [PubMed]
- Padmanabhanunni, A.; Pretorius, T.B.; Isaacs, S.A. We are Not Islands: The Role of Social Support in the Relationship between Perceived Stress during the COVID-19 Pandemic and Psychological Distress. Int. J. Environ. Res. Public Health 2023, 20, 3179. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Bao, X.; Yan, J.; Miao, H.; Guo, C. Anxiety and depression in Chinese students during the COVID-19 pandemic: A meta-analysis. Front. Public Health 2021, 9, 697642. [Google Scholar] [CrossRef] [PubMed]
- Torales, J.; O’Higgins, M.; Castaldelli-Maia, J.M.; Ventriglio, A. The outbreak of COVID-19 coronavirus and its impact on global mental health. Int. J. Soc. Psychiatry 2020, 4, 317–320. [Google Scholar] [CrossRef]
- Petzold, M.B.; Bendau, A.; Plag, J.; Pyrkosch, L.; Mascarell Maricic, L.; Betzler, F.; Rogoll, J.; Grose, J.; Ströhle, A. Risk, resilience, psychological distress, and anxiety at the beginning of the COVID-19 pandemic in Germany. Brain Behav. 2020, 10, 01745. [Google Scholar] [CrossRef]
- Özdin, S.; Bayrak Özdin, Ş. Levels and predictors of anxiety, depression and health anxiety during COVID-19 pandemic in Turkish society: The importance of gender. Int. J. Soc. Psychiatry 2020, 66, 504–511. [Google Scholar] [CrossRef]
- Fu, W.; Wang, C.; Zou, L.; Guo, Y.; Lu, Z.; Yan, S.; Mao, J. Psychological health, sleep quality, and coping styles to stress facing the COVID-19 in Wuhan, China. Transl. Psychiatry 2020, 10, 225. [Google Scholar] [CrossRef]
- Gualano, M.R.; Lo Moro, G.; Voglino, G.; Bert, F.; Siliquini, R. Effects of Covid-19 lockdown on mental health and sleep disturbances in Italy. Int. J. Environ. Res. Public Health 2020, 17, 4779. [Google Scholar] [CrossRef]
- Wang, K.; Manning, R.B., III; Bogart, K.R.; Adler, J.M.; Nario-Redmond, M.R.; Ostrove, J.M.; Lowe, S.R. Predicting depression and anxiety among adults with disabilities during the COVID-19 pandemic. Rehabil. Psychol. 2022, 67, 179. [Google Scholar] [CrossRef]
- Amerio, A.; Bertuccio, P.; Santi, F.; Bianchi, D.; Brambilla, A.; Morganti, A.; Odone, A.; Costanza, A.; Signorelli, C.; Aguglia, A.; et al. Gender differences in COVID-19 lockdown impact on mental health of undergraduate students. Front. Psychiatry 2022, 12, 813130. [Google Scholar] [CrossRef]
- Blix, I.; Birkeland, M.S.; Thoresen, S. Worry and mental health in the Covid-19 pandemic: Vulnerability factors in the general Norwegian population. BMC Public Health 2021, 21, 928. [Google Scholar] [CrossRef] [PubMed]
- Magano, J.; Vidal, D.G.; Sousa, H.F.P.e.; Dinis, M.A.P.; Leite, Â. Psychological Factors Explaining Perceived Impact of COVID-19 on Travel. Eur. J. Investig. Health Psychol. Educ. 2021, 11, 1120–1133. [Google Scholar] [CrossRef] [PubMed]
- Chandu, V.C.; Pachava, S.; Vadapalli, V.; Marella, Y. Development and initial validation of the COVID-19 anxiety scale. Indian J. Public Health 2020, 64, 201–204. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus Disease 2019 (COVID-19): Situation Report-86 World Health Organization. 2020. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200415-sitrep-86-covid-19.pdf?sfvrsn=c615ea20_2 (accessed on 1 August 2023).
- Coco, G.L.; Salerno, L.; Albano, G.; Pazzagli, C.; Lagetto, G.; Mancinelli, E.; Freda, M.F.; Bassi, G.; Giordano, C.; Gullo, S.; et al. Psychosocial predictors of trajectories of mental health distress during the COVID-19 pandemic: A four-wave panel study. Psychiatry Res. 2023, 326, 115262. [Google Scholar] [CrossRef] [PubMed]
- Shabani, M.J.; Mohsenabadi, H.; Gharraee, B.; Shayanfar, F.; Corcoran, V.P.; McKay, D. Psychological correlates of health anxiety in response to the coronavirus (COVID-19) pandemic: A cross-sectional online study in Iran. Int. J. Cogn. Ther. 2023, 16, 103–122. [Google Scholar] [CrossRef]
- Hayes, A. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 2nd ed.; Guilford Press: New York, NY, USA, 2017; p. 692. [Google Scholar]
- Solomou, I.; Constantinidou, F. Prevalence and predictors of anxiety and depression symptoms during the COVID-19 pandemic and compliance with precautionary measures: Age and sex matter. Int. J. Environ. Res. Public Health 2020, 17, 4924. [Google Scholar] [CrossRef]
- OSF. Socio-Psychological Effects of the Crisis Caused by COVID-19: Perceived Stress and Dynamics of Experiences. Available online: https://osf.io/hrw78/ (accessed on 10 August 2023).
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Karastoyanov, G.; Rusinova-Hristova, A. Balgarska adaptacia na vaprosnik za vazpriet stress [Bulgarian adaptation of a questionnaire for perceived stress]. Psihol. Izsled. 2020, 1, 67–77. (In Bulgarian) [Google Scholar]
- Velichkov ARadoslavova, M.; Rasheva, M. Metod za izmervane na generaliziranite ochakvaniya za valentnostta na poluchenite rezultati (optimism I negativni ochakvaniya) [Method for measurement of the generalized expectations for the valency of the results obtained (optimism and negative expectations)]. Bulg. J. Psychol. 1993, 3, 85–100. (In Bulgarian) [Google Scholar]
- Hristova, A.; Nacheva, I.; Andreev, B. Optimistichni i pesimistichni naglasi v sotsialen kontekst [Optimistic and pessimistic attitudes in a social context]. Psihol. Izsled. 2017, 20, 261–285. (In Bulgarian) [Google Scholar]
- Lock, S.; Rees, C.S.; Heritage, B. Development and validation of a brief measure of psychological resilience: The state-trait assessment of resilience scale. Aust. Psychol. 2020, 55, 10–25. [Google Scholar] [CrossRef]
- Zsido, A.N.; Teleki, S.A.; Csokasi, K.; Rozsa, S.; Bandi, S.A. Development of the short version of the spielberger state—Trait anxiety inventory. Psychiatry Res. 2020, 291, 113223. [Google Scholar] [CrossRef]
- Nikčević, A.V.; Spada, M.M. The COVID-19 anxiety syndrome scale: Development and psychometric properties. Psychiatry Res. 2020, 292, 113322. [Google Scholar] [CrossRef]
- Kuran, C.H.A.; Morsut, C.; Kruke, B.I.; Krüger, M.; Segnestam, L.; Orru, K.; Nævestad, T.O.; Airola, M.; Keranen, J.; Gabel, F.; et al. Vulnerability and vulnerable groups from an intersectionality perspective. Int. J. Disaster Risk Reduct. 2020, 50, 101826. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Parents with Young Children | Chronically III People | People with Multiple Vulnerability Characteristics | Control Group | Total | |
|---|---|---|---|---|---|---|
| N of respondents | 134 | 146 | 140 | 100 | 520 | |
| % | 25.8 | 28.1 | 26.9 | 19.2 | 100.0 | |
| Age | M | 37.68 | 59.56 | 43.72 | 52.00 | 48.99 |
| SD | 6.99 | 10.27 | 11.28 | 12.42 | 13.15 | |
| Gender | Male | 14 | 14 | 14 | 16 | 58 |
| Female | 131 | 118 | 126 | 81 | 456 | |
| Missing/NA | 1 | 1 | 0 | 3 | 5 | |
| Education | Primary | 0 | 3 | 2 | 0 | 5 |
| Secondary | 19 | 46 | 35 | 25 | 125 | |
| Higher | 115 | 97 | 103 | 75 | 390 | |
| Occupation | Manager | 40 | 17 | 21 | 18 | 96 |
| Non-manager | 62 | 38 | 52 | 33 | 185 | |
| Student | 1 | 0 | 3 | 1 | 5 | |
| Retired | 1 | 63 | 11 | 20 | 95 | |
| Unemployed | 10 | 9 | 23 | 11 | 53 | |
| Other | 18 | 17 | 26 | 13 | 74 | |
| Factor | Group | M (SD) 95% CI [LL; UL] | Sk./K. | F (df 3) (Sig.) | Homogeneity of Variances-Levene (Sig.) | Pairwise Tests-Scheffé |
|---|---|---|---|---|---|---|
| Trait Anxiety | Chronic sufferers | 2.529 (0.743) [2.408; 2.651] | −0.200/−0.613 | 0.379 (0.768) | 0.384 | n/a |
| Parents of 0–12 y.o. | 2.480 (0.749) [2.352; 2.608] | 0.279/−0.441 | ||||
| People with multiple vulnerability | 2.523 (0.811) [2.388; 2.659] | 0.119/−0.869 | ||||
| Control group | 2.434 (0.786) [2.279; 2.591] | −0.040/−0.647 | ||||
| COVID-19 Anxiety | Chronic sufferers | 2.043 (0.839) [1.905; 2.180] | 0.770/−0.209 | 1.477 (0.220) | 0.086 | n/a |
| Parents of 0–12 y.o. | 1.969 (0.839) [1.826; 2.113] | 0.823/0.168 | ||||
| People with multiple vulnerability | 2.122 (0.995) [1.956; 2.289] | 1.001/0.820 | ||||
| Control group | 1.896 (0.812) [1.735; 2.057] | 0.301/0.109 | ||||
| Trait Resilience | Chronic sufferers | 3.192 (0.575) [3.098; 3.286] | −0.857/0.538 | 0.280 (0.840) | 0.084 | n/a |
| Parents of 0–12 y.o. | 3.166 (0.483) [3.084; 3.249] | −0.193/0.238 | ||||
| People with multiple vulnerability | 3.176 (0.586) [3.078; 3.274] | −0.240/−0.682 | ||||
| Control group | 3.127 (0.553) [3.018; 3.237] | −0.327/0.360 | ||||
| State Resilience | Chronic sufferers | 2.955 (0.691) [2.843; 3.068] | −0.382/−0.096 | 1.100 (0.349) | 0.138 | n/a |
| Parents of 0–12 y.o. | 3.023 (0.604) [2.920; 3.126] | −0.645/0.783 | ||||
| People with multiple vulnerability | 2.878 (0.673) [2.766; 2.991] | −0.055/−0.620 | ||||
| Control group | 2.966 (0.692) [2.829; 3.103] | −0.255/−0.428 | ||||
| Perceived Stress | Chronic sufferers | 2.412 (0.892) [2.266; 2.558] | 0.623/0.206 | 1.571 (0.196) | 0.302 | n/a |
| Parents of 0–12 y.o. | 2.403 (0.933) [2.243; 2.563] | 0.621/−0.087 | ||||
| People with multiple vulnerability | 2.620 (0.977) [2.457; 2.784] | 0.409/−0.385 | ||||
| Control group | 2.4883 (0.998) [2.290; 2.687] | 0.415/−0.432 | ||||
| Pessimism | Chronic sufferers | 2.897 (0.910) [2.748; 3.046] | −0.171/−0.408 | 4.055 (0.007) | 0.111 | ChS > P ** |
| Parents of 0–12 y.o. | 2.531 (0.865) [2.383; 2.679] | 0.159/−0.092 | ||||
| People with multiple vulnerability | 2.801 (1.011) [2.631; 2.971] | 0.307/−0.498 | ||||
| Control group | 2.670 (0.905) [2.491; 2.850] | 0.125/−0.580 | ||||
| Optimism | Chronic sufferers | 4.043 (0.805) [3.912; 4.175] | −0.803/0.606 | 2.569 (0.054) | 0.255 | n/a |
| Parents of 0–12 y.o. | 4.109 (0.654) [3.998; 4.221] | −0.197/−0.833 | ||||
| People with multiple vulnerability | 3.896 (0.871) [3.751; 4.043] | −0.682/0.382 | ||||
| Control group | 4.161 (0.750) [4.013; 4.311] | −0.765/0.103 |
| 95% CI | |||||||
|---|---|---|---|---|---|---|---|
| Model | Beta | SE | LL | UL | β | p | |
| Chronic sufferers | |||||||
| 1. | Trait Anxiety | 0.317 | 0.090 | 0.139 | 0.496 | 0.281 * | 0.001 |
| Parents with little children | |||||||
| 1. | Perceived Stress | 0.199 | 0.076 | 0.048 | 0.349 | 0.221 * | 0.010 |
| People with multiple vulnerabilities | |||||||
| 1. | Trait Anxiety | 0.536 | 0.092 | 0.354 | 0.718 | 0.445 * | 0.000 |
| 2. | Trait Anxiety | 0.377 | 0.110 | 0.158 | 0.595 | 0.313 * | 0.001 |
| Perceived stress | 0.228 | 0.091 | 0.049 | 0.408 | 0.230 * | 0.013 | |
| Control group | |||||||
| 1. | Trait Resilience | −0.762 | 0.127 | −1.013 | −0.510 | −0.519 * | 0.000 |
| 2. | Optimism | −0.443 | 0.096 | −0.634 | −0.252 | −0.409 * | 0.000 |
| Perceived Stress | 0.229 | 0.072 | 0.086 | 0.373 | 0.282 * | 0.002 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bakalova, D.; Nacheva, I.; Panchelieva, T. Psychological Predictors of COVID-19-Related Anxiety in Vulnerable Groups. Eur. J. Investig. Health Psychol. Educ. 2023, 13, 1815-1830. https://doi.org/10.3390/ejihpe13090132
Bakalova D, Nacheva I, Panchelieva T. Psychological Predictors of COVID-19-Related Anxiety in Vulnerable Groups. European Journal of Investigation in Health, Psychology and Education. 2023; 13(9):1815-1830. https://doi.org/10.3390/ejihpe13090132
Chicago/Turabian StyleBakalova, Diana, Ilina Nacheva, and Tsvetelina Panchelieva. 2023. "Psychological Predictors of COVID-19-Related Anxiety in Vulnerable Groups" European Journal of Investigation in Health, Psychology and Education 13, no. 9: 1815-1830. https://doi.org/10.3390/ejihpe13090132
APA StyleBakalova, D., Nacheva, I., & Panchelieva, T. (2023). Psychological Predictors of COVID-19-Related Anxiety in Vulnerable Groups. European Journal of Investigation in Health, Psychology and Education, 13(9), 1815-1830. https://doi.org/10.3390/ejihpe13090132