
A Wolf in Sheep’s Clothing: Collision of Melanoma and Keratoacanthoma

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
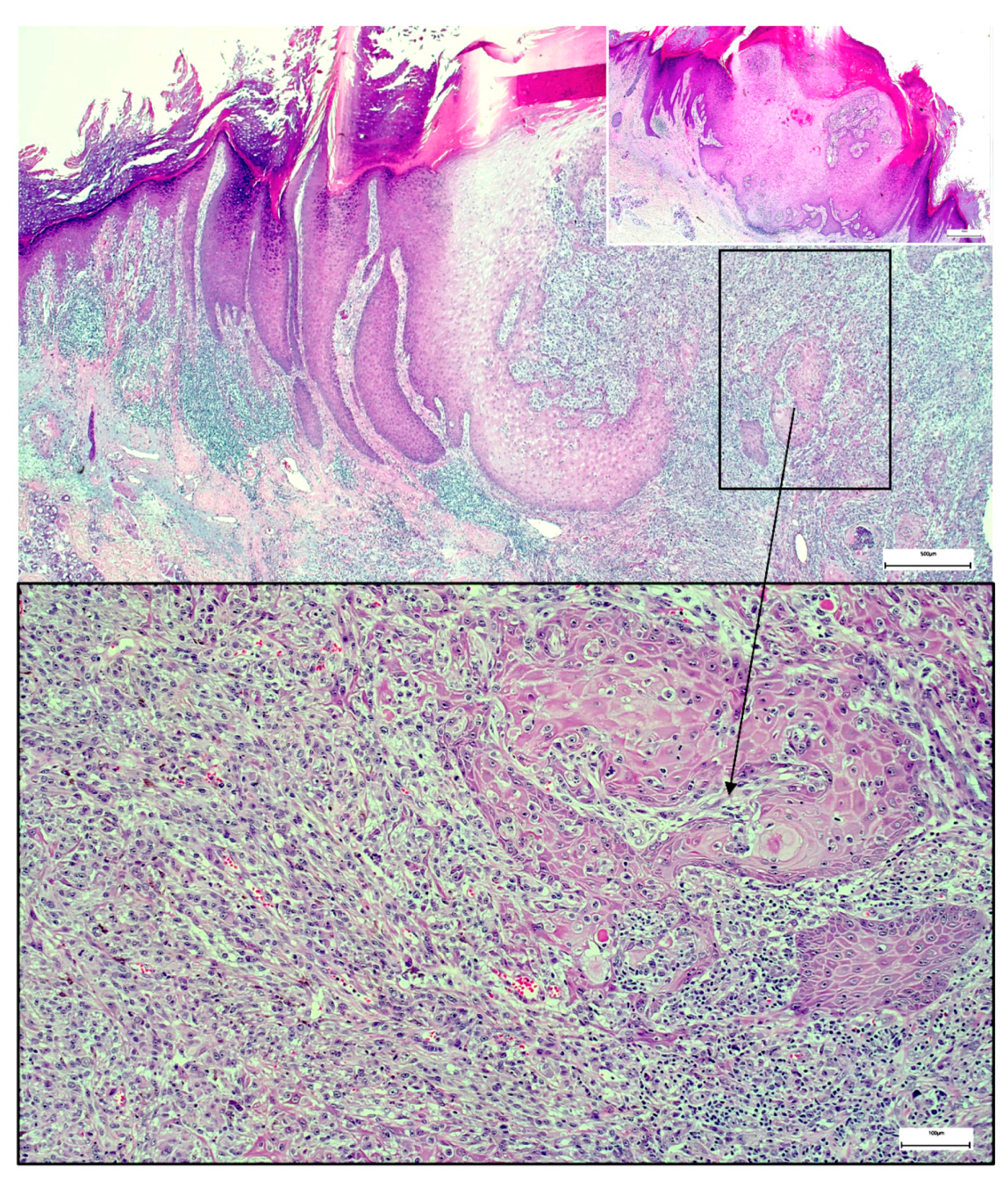
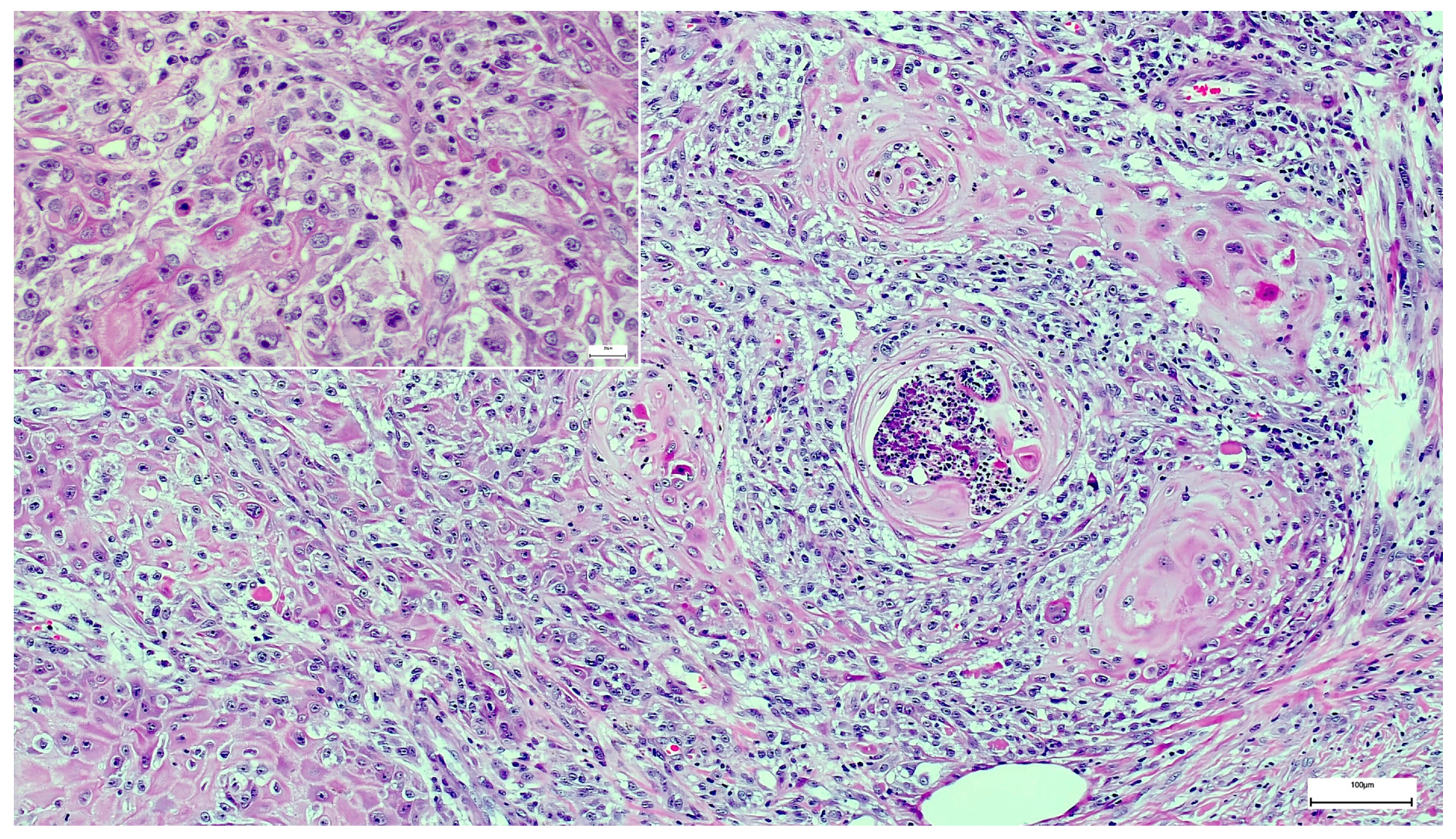
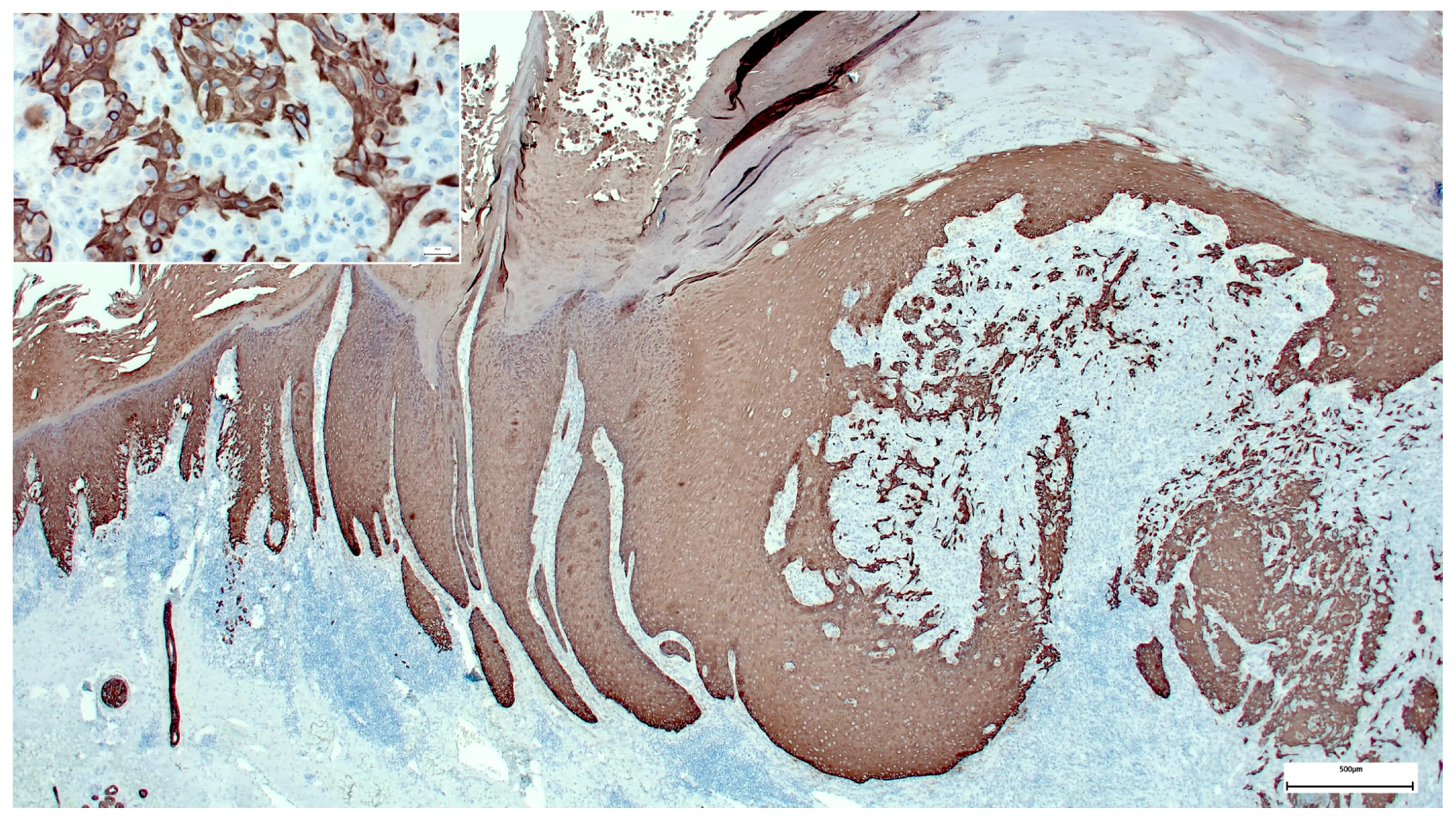
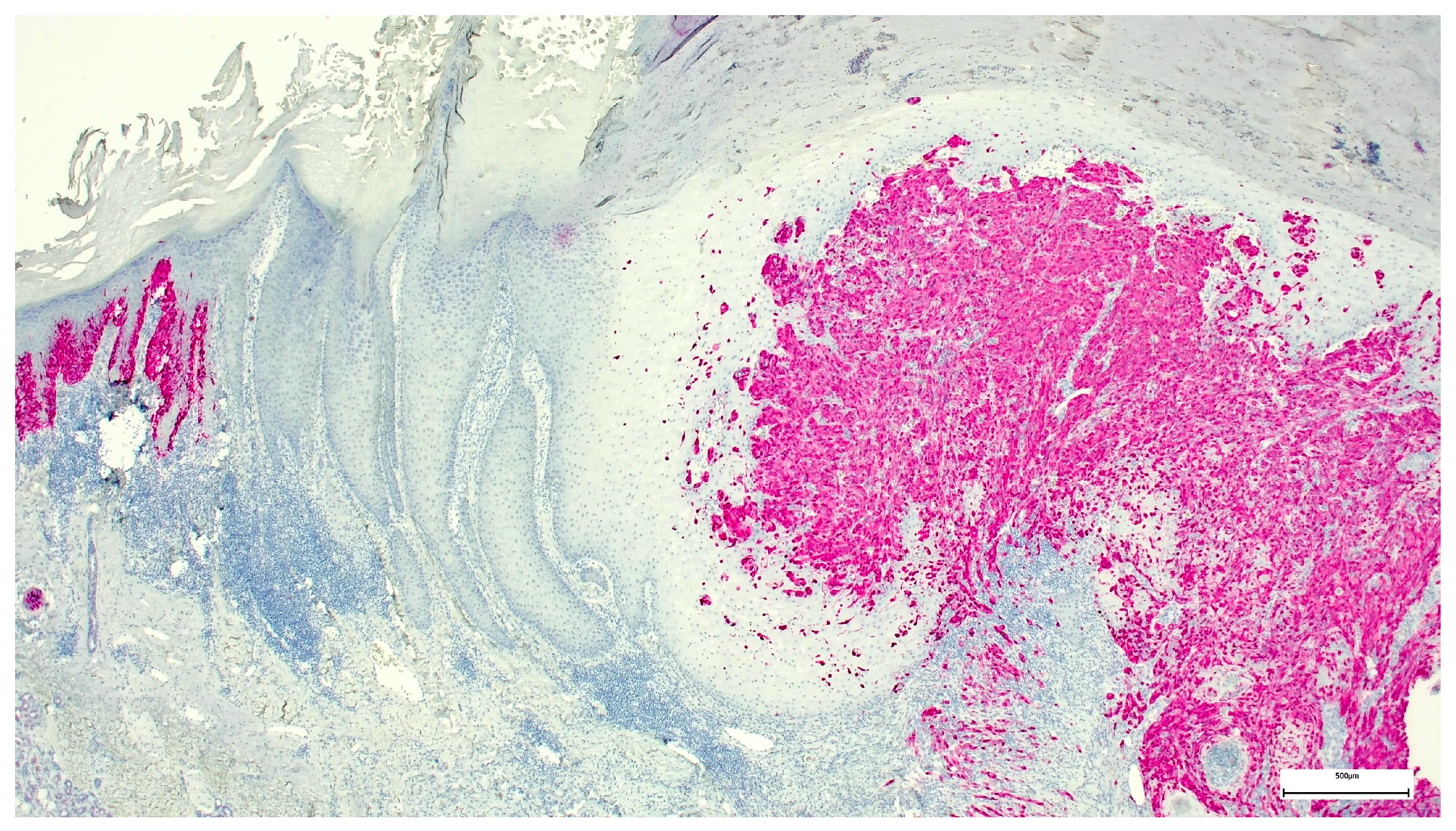
:1. Case Presentation
2. Discussion
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Kochoumian, E.; Kazlouskaya, V.; Mangold, A.; Lal, K.; Maia-Cohen, S.; Elston, D.M. Tumor with the features of both squamous cell carcinoma and melanoma (melanocarcinoma). Indian Dermatol. Online J. 2015, 6, 217–219. [Google Scholar] [PubMed]
- Sánchez Yus, E.; Requena, L. Keratoacanthoma within a superficial spreading malignant melanoma in situ. J. Cutan. Pathol. 1991, 18, 288–292. [Google Scholar] [PubMed]
- Cota, C.; Andrea, S.; Viviana, L.; Heinz, K.; Arno, R.; Omar, S.; Luis, R.; Lorenzo, C. Uncommon Histopathological Variants of Malignant Melanoma: Part 1. Am. J. Dermatopathol. 2019, 41, 243–263. [Google Scholar] [CrossRef] [PubMed]
- Sadlier, M.; Alani, A.; Ipadeola, O.B.; Ahmad, K. A pink and purple plaque. JAAD Case Rep. 2018, 4, 189–191. [Google Scholar] [CrossRef] [PubMed]
- Green, R.; Woody, M.; Soldano, A.C.; Madden, E. Basal cell carcinoma and malignant melanoma cutaneous collision tumor. In Baylor University Medical Center Proceedings; Taylor & Francis: Abingdon, UK, 2018; Volume 31, pp. 362–363. [Google Scholar]
- Kim, T.H.; Lee, J.H.; Roh, M.R. A case of keratoacanthoma associated with Basal cell carcinoma. Ann. Dermatol. 2015, 27, 237–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cornejo, K.M.; Deng, A.C. Malignant melanoma within squamous cell carcinoma and basal cell carcinoma: Is it a combined or collision tumor?—A case report and review of the literature. Am. J. Dermatopathol. 2013, 35, 226–234. [Google Scholar] [CrossRef] [PubMed]
- Mopuri, N.; Laitung, J.; Cardozo, C. Collision tumour of squamous cell carcinoma and invasive malignant melanoma of scalp—A case report. J. Plast. Reconstr. Aesthetic Surg. 2009, 62, e104–e105. [Google Scholar] [CrossRef] [PubMed]
- Thomas, I.; Kihiczak, N.I.; Rothenberg, J.; Ahmed, S.; Schwartz, R.A. Melanoma within the seborrheic keratosis. Dermatol. Surg. 2004, 30 (Pt 1), 559–561. [Google Scholar] [PubMed]
- Pool, S.E.; Manieei, F.; Clark, W.H., Jr.; Harrist, T.J. Dermal squamo-melanocytic tumor: A unique biphenotypic neoplasm of uncertain biological potential. Hum. Pathol. 1999, 30, 525–529. [Google Scholar] [CrossRef]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Walther, M.; Falkvoll, S.; Leibl, S. A Wolf in Sheep’s Clothing: Collision of Melanoma and Keratoacanthoma. Dermatopathology 2021, 8, 253-257. https://doi.org/10.3390/dermatopathology8030030
Walther M, Falkvoll S, Leibl S. A Wolf in Sheep’s Clothing: Collision of Melanoma and Keratoacanthoma. Dermatopathology. 2021; 8(3):253-257. https://doi.org/10.3390/dermatopathology8030030
Chicago/Turabian StyleWalther, Matthias, Sandra Falkvoll, and Sebastian Leibl. 2021. "A Wolf in Sheep’s Clothing: Collision of Melanoma and Keratoacanthoma" Dermatopathology 8, no. 3: 253-257. https://doi.org/10.3390/dermatopathology8030030
APA StyleWalther, M., Falkvoll, S., & Leibl, S. (2021). A Wolf in Sheep’s Clothing: Collision of Melanoma and Keratoacanthoma. Dermatopathology, 8(3), 253-257. https://doi.org/10.3390/dermatopathology8030030