
Histological Patterns of Skin Lesions in Tuberous Sclerosis Complex: A Panorama


Abstract
:1. Introduction
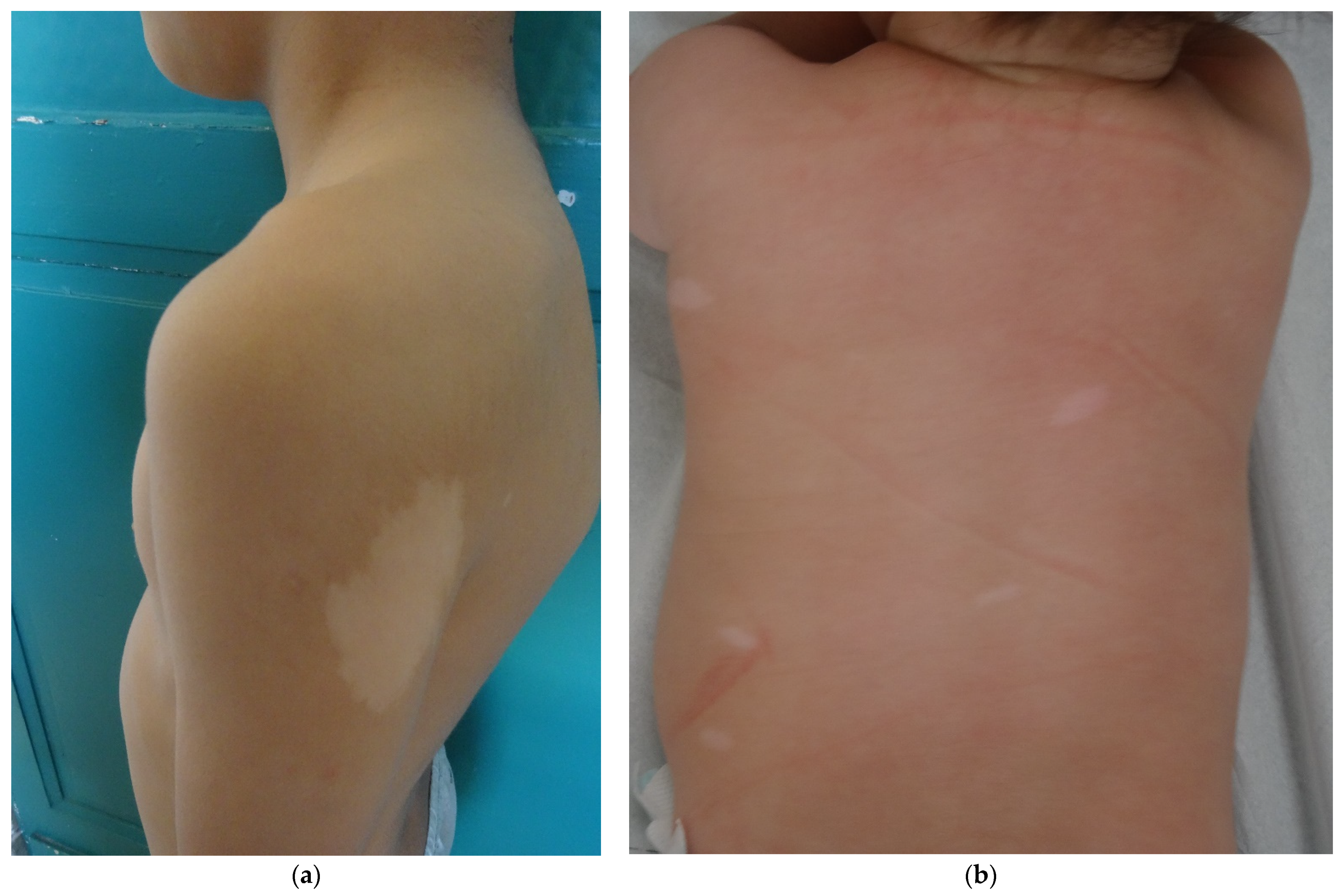
- Hypomelanotic lesions:
- -
- hypomelanotic macules
- -
- confetti skin lesions
- Connective tissue nevi (cutaneous hamartomas):
- -
- periungual fibromas (PF),
- -
- angiofibromas (AF),
- -
- shagreen patches (SP),
- -
- forehead fibrous plaques (FFP),
- -
- folliculocystic and collagen hamartomas (FCCH).
2. Hypomelanotic Lesions
3. TSC-Associated Cutaneous Hamartomas (Connective Tissue Nevi)
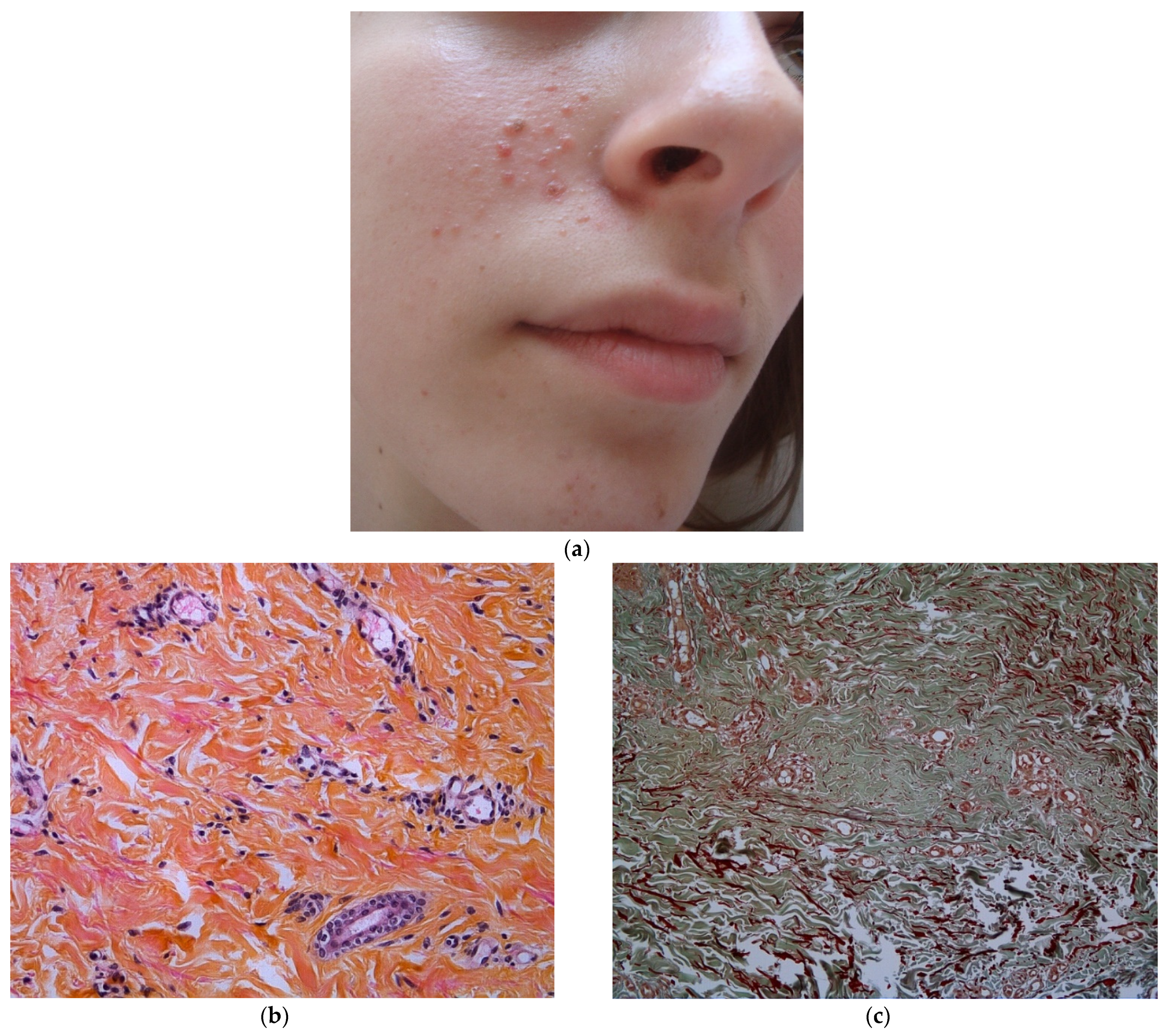
3.1. Angiofibromas (AF)
3.2. Periungual Fibroma (PF)
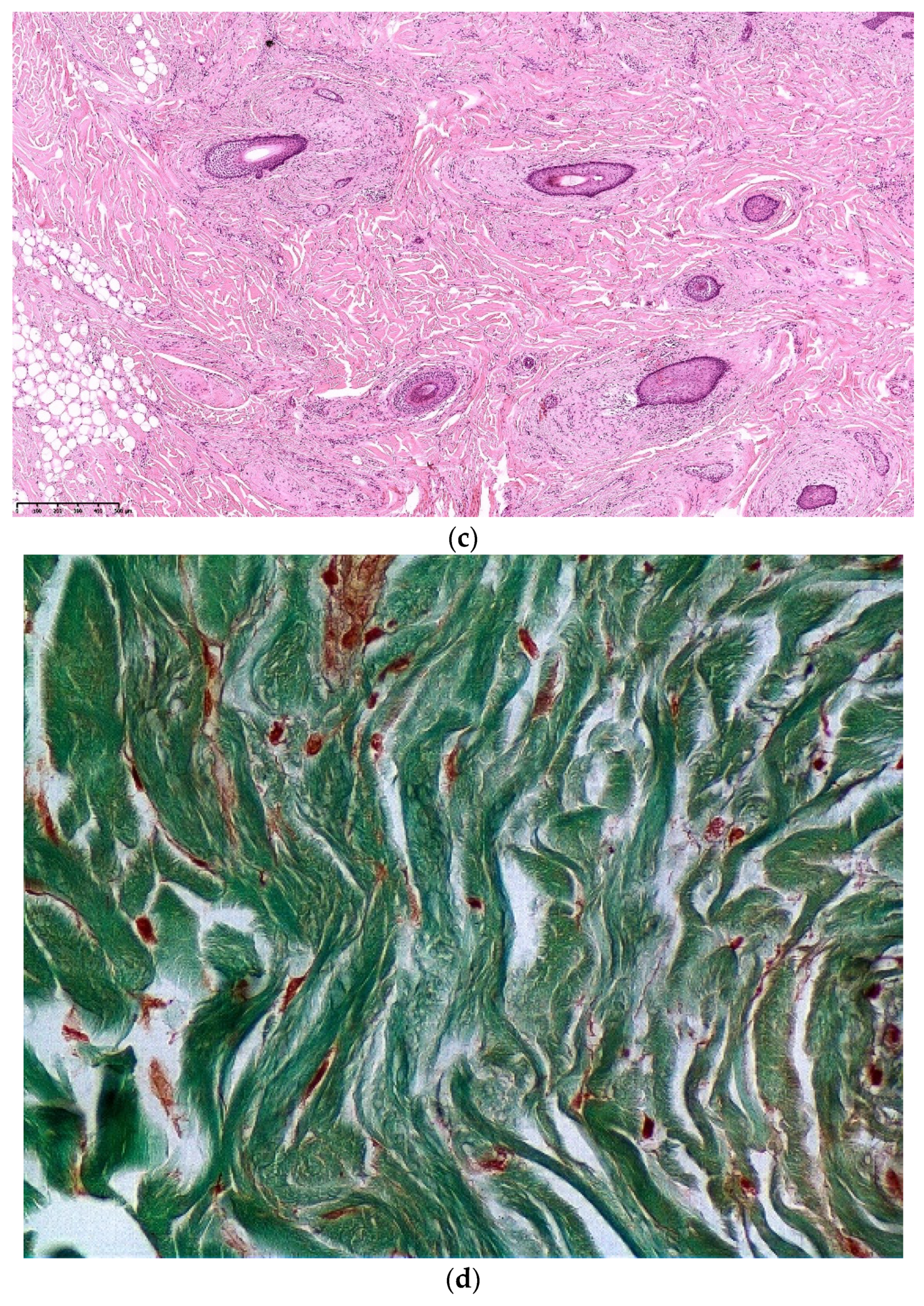
3.3. Fibrous Cephalic Plaque (FCP)
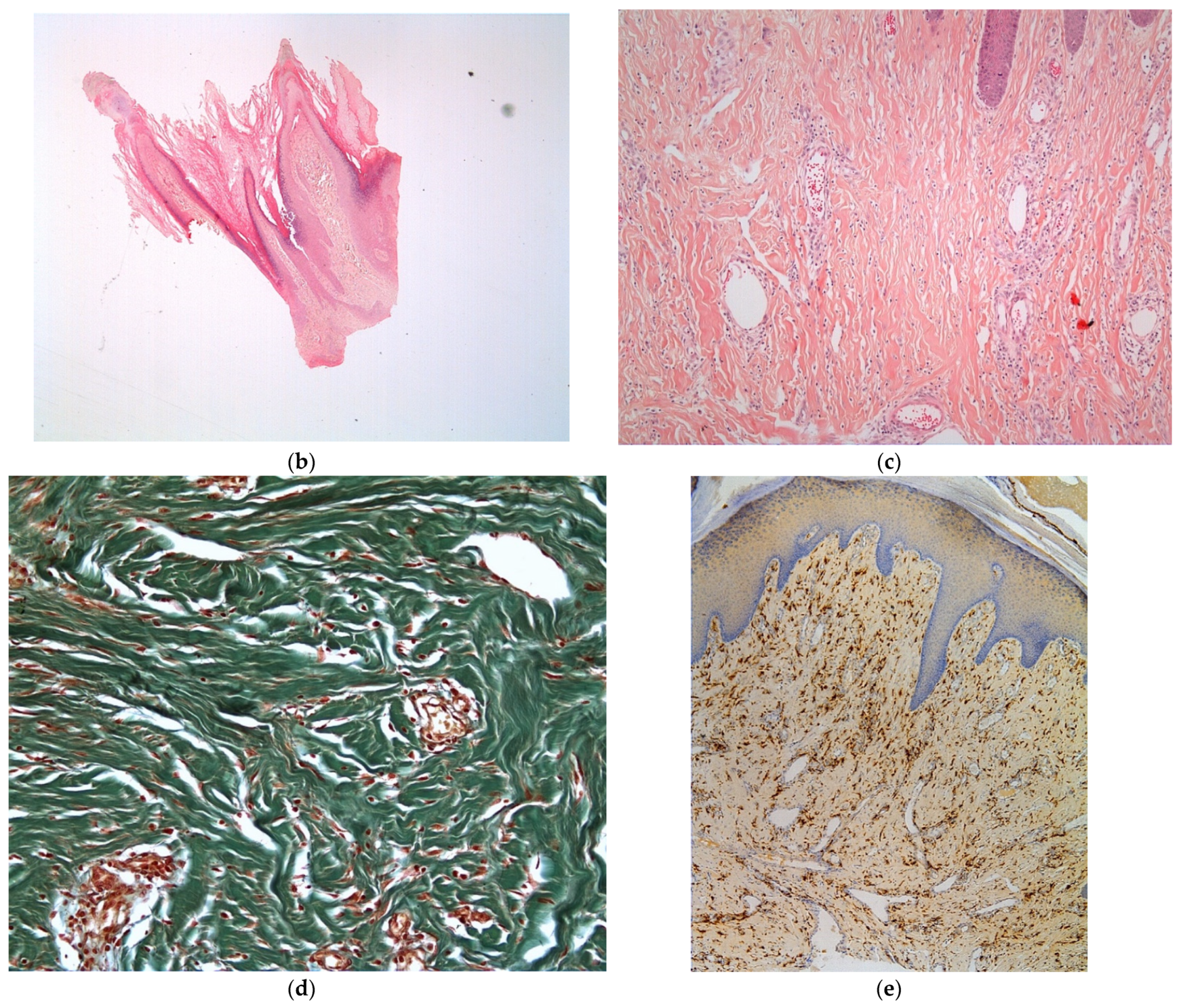
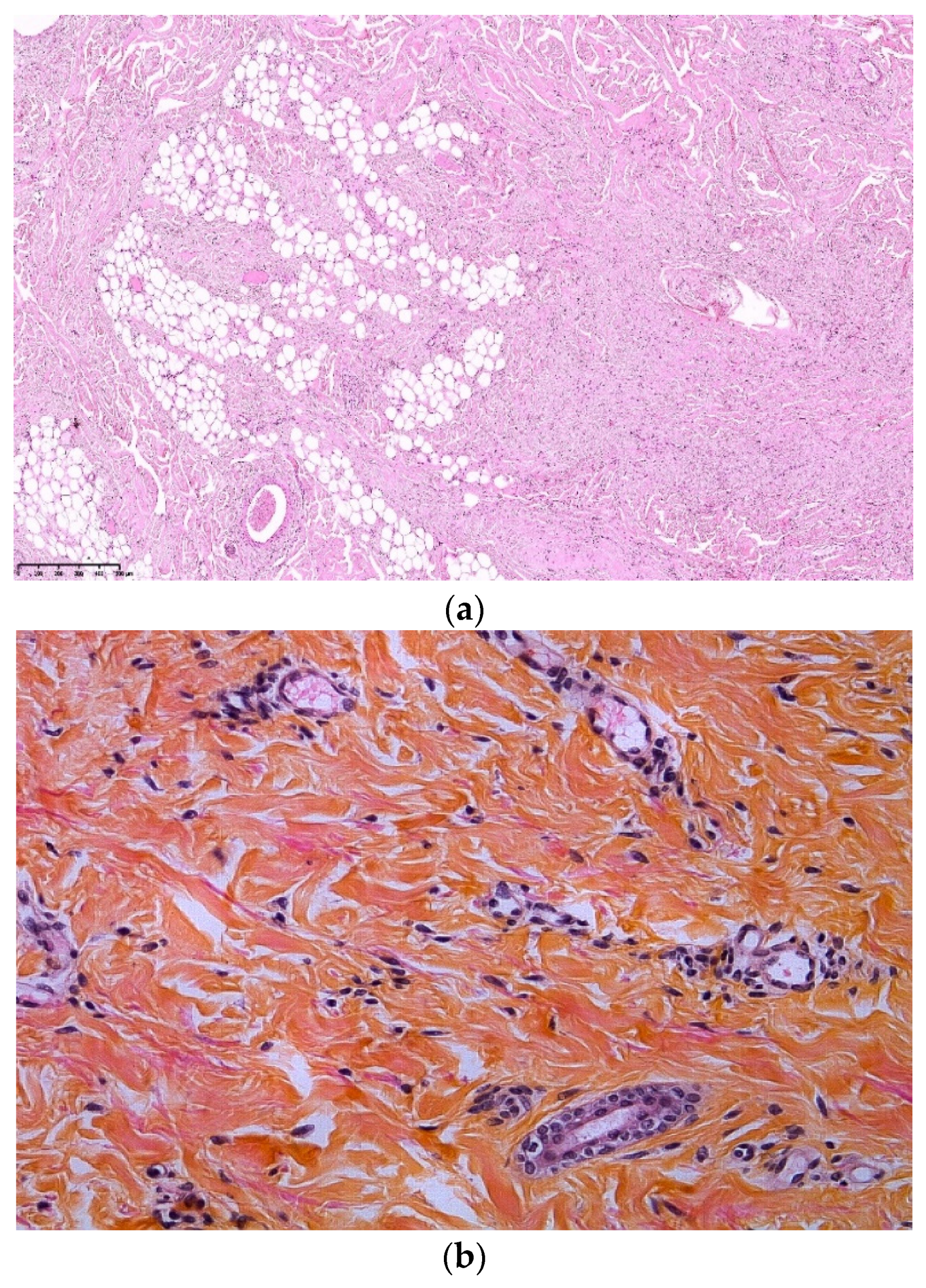
3.4. Shagreen Patches (SP)
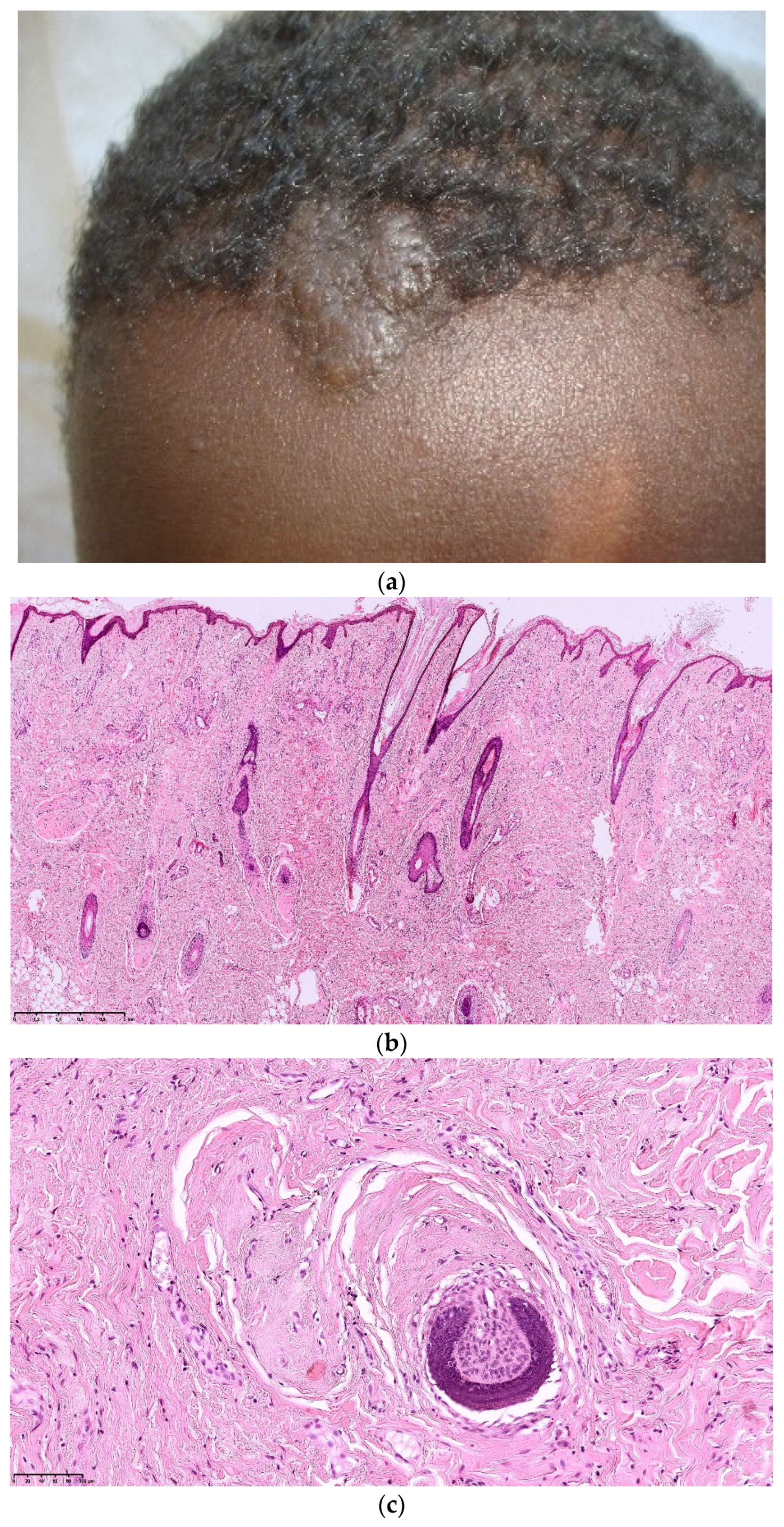
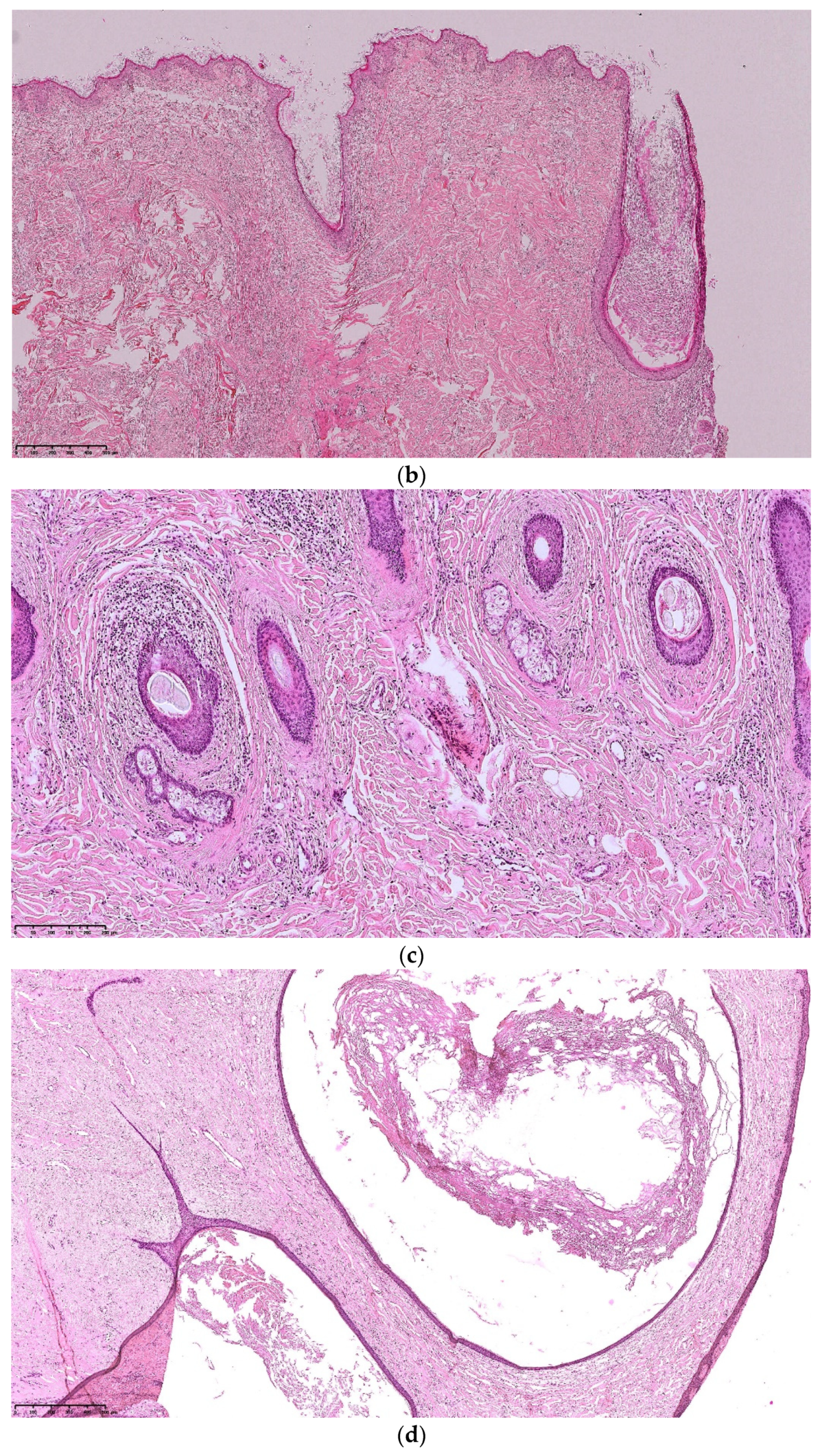
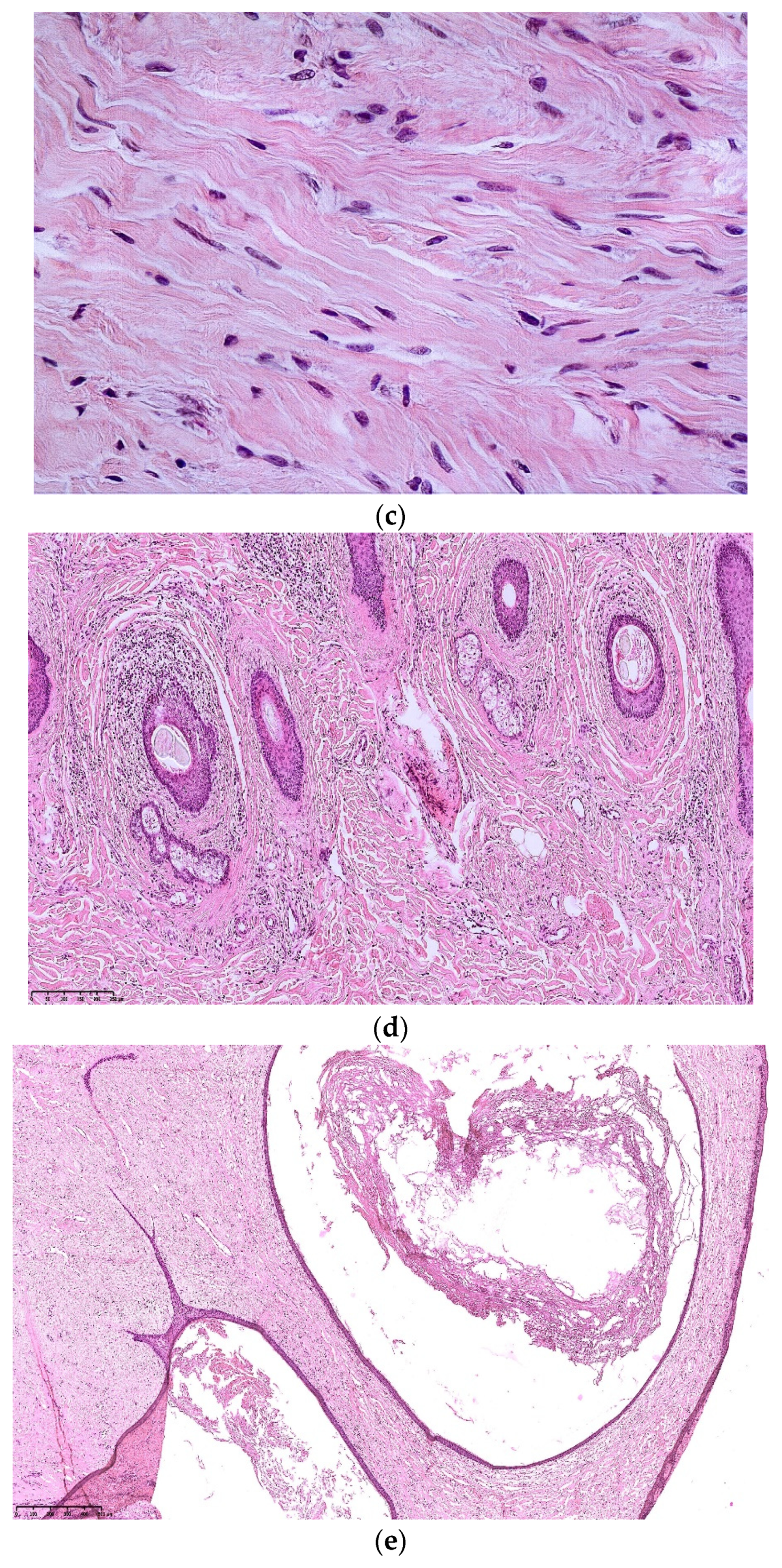
3.5. Folliculocystic and Collagen Hamartoma (FCCH)
4. Other TSC-Associated Cutaneous Lesions
5. Does TSC Cutaneous Hamartoma Belong to the Same Lesional Spectrum?
- -
- abundant thickened collagen, associated with adnexal involvement (concentric fibrosis)
- -
- vascular hyperplasia,
- -
- cellular proliferation of fibroblasts.
6. In Conclusion, Is Histopathological Examination Useful in TSC Diagnosis?
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Northrup, H.; Krueger, D.A. International Tuberous Sclerosis Complex Consensus Group. Tuberous sclerosis complex diagnostic criteria update: Recommendations of the 2012 Iinternational Tuberous Sclerosis Complex Consensus Conference. Pediatr. Neurol. 2013, 49, 243–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wataya-Kaneda, M.; Tanaka, M.; Hamasaki, T.; Katayama, I. Trends in the prevalence of tuberous sclerosis complex manifestations: An epidemiological study of 166 Japanese patients. PLoS ONE 2013, 8, e63910. [Google Scholar] [CrossRef]
- Lam, H.C.; Nijmeh, J.; Henske, E.P. New developments in the genetics and pathogenesis of tumours in tuberous sclerosis complex. J. Pathol. 2017, 241, 219–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jimbow, K. Tuberous sclerosis and guttate leukodermas. Semin. Cutan. Med. Surg. 1997, 16, 30–35. [Google Scholar] [CrossRef]
- Jimbow, K.; Fitzpatrick, T.B.; Szabo, G.; Hori, Y. Congenital circumscribed hypomelanosis: A characterization based on electron microscopic study of tuberous sclerosis, nevus depigmentosus, and piebaldism. J. Investig. Dermatol. 1975, 64, 50–62. [Google Scholar] [CrossRef] [Green Version]
- Wataya-Kaneda, M.; Tanaka, M.; Yang, L.; Yang, F.; Tsuruta, D.; Nakamura, A.; Matsumoto, S.; Hamasaki, T.; Tanemura, A.; Katayama, I. Clinical and Histologic Analysis of the Efficacy of Topical Rapamycin Therapy Against Hypomelanotic Macules in Tuberous Sclerosis Complex. JAMA Dermatol. 2015, 151, 722–730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacks, S.K.; Witman, P.M. Tuberous Sclerosis Complex: An Update for Dermatologists. Pediatr. Dermatol. 2015, 32, 563–570. [Google Scholar] [CrossRef]
- Jóźwiak, S.; Schwartz, R.A.; Janniger, C.K.; Michałowicz, R.; Chmielik, J. Skin lesions in children with tuberous sclerosis complex: Their prevalence, natural course, and diagnostic significance. Int. J. Dermatol. 1998, 37, 911–917. [Google Scholar] [CrossRef] [PubMed]
- Nickel, W.R.; Reed, W.B. Tuberous Sclerosis: Special Reference to the Microscopic Alterations in the Cutaneous Hamartomas. Arch. Dermatol. 1962, 85, 209–226. [Google Scholar] [CrossRef]
- Reed, R.J.; Ackerman, A.B. Pathology of the adventitial dermis. Hum. Pathol. 1973, 4, 207–217. [Google Scholar] [CrossRef]
- Benjamin, D.R. Cellular composition of the angiofibromas in tuberous sclerosis. Pediatr. Pathol. Lab. Med. J. Soc. Pediatr. Pathol. Affil. Int. Paediatr. Pathol. Assoc. 1996, 16, 893–899. [Google Scholar]
- de Cambourg, G.; Cribier, B. Fibrous papules of the face: A retrospective anatomoclinical study of 283 cases. Ann. Dermatol. Venereol. 2013, 140, 763–770. [Google Scholar] [CrossRef] [PubMed]
- Tyburczy, M.E.; Wang, J.-A.; Li, S.; Thangapazham, R.; Chekaluk, Y.; Moss, J.; Kwiatkowski, D.J.; Darling, T.N. Sun exposure causes somatic second-hit mutations and angiofibroma development in tuberous sclerosis complex. Hum. Mol. Genet. 2014, 23, 2023–2029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Webb, D.W.; Clarke, A.; Fryer, A.; Osborne, J.P. The cutaneous features of tuberous sclerosis: A population study. Br. J. Dermatol. 1996, 135, 1–5. [Google Scholar] [CrossRef]
- Treichel, A.M.; Pithadia, D.J.; Lee, C.-C.R.; Oyerinde, O.; Moss, J.; Darling, T.N. Histopathological Features of Fibrous Cephalic Plaques in Tuberous Sclerosis Complex. Histopathology 2021. [Google Scholar] [CrossRef]
- Bongiorno, M.A.; Nathan, N.; Oyerinde, O.; Wang, J.-A.; Lee, C.-C.R.; Brown, G.T.; Moss, J.; Darling, T.N. Clinical Characteristics of Connective Tissue Nevi in Tuberous Sclerosis Complex with Special Emphasis on Shagreen Patches. JAMA Dermatol. 2017, 153, 660–665. [Google Scholar] [CrossRef]
- Torrelo, A.; Hadj-Rabia, S.; Colmenero, I.; Piston, R.; Sybert, V.P.; Hilari-Carbonell, H.; Hernández-Martín, A.; Ferreres, J.C.; Vañó-Galván, S.; Azorín, D.; et al. Folliculocystic and collagen hamartoma of tuberous sclerosis complex. J. Am. Acad. Dermatol. 2012, 66, 617–621. [Google Scholar] [CrossRef] [PubMed]
- An, J.M.; Kim, Y.S.; Park, Y.L.; Lee, S. Folliculocystic and Collagen Hamartoma: A New Entity? Ann. Dermatol. 2015, 27, 593–596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaplan, L.; Kazlouskaya, V.; Ugorji, R.; Heilman, E.; Siegel, D.M.; Glick, S.A. Folliculocystic and collagen hamartoma of tuberous sclerosis: A new case in a female patient and review of literature. J. Cutan. Pathol. 2018, 45, 67–70. [Google Scholar] [CrossRef]
- Brown, M.M.; Walsh, E.J.; Yu, L.; Smidt, A.C. Progressive Scalp Plaque in a Girl with Tuberous Sclerosis. Pediatr. Dermatol. 2014, 31, 249–250. [Google Scholar] [CrossRef]
- Cardona, R.; Cancel-Artau, K.J.; Carrasquillo, O.Y.; Martin-Garcia, R.F. Folliculocystic and Collagen Hamartoma: A Distinct Hamartoma Associated with Tuberous Sclerosis Complex. Am. J. Dermatopathol. 2021, 43, 67–70. [Google Scholar] [CrossRef] [PubMed]
- Bishnoi, A.; Tripathy, S.; Vinay, K.; De, D.; Parsad, D.; Chatterjee, D.; Saikia, U.N. Image Gallery: Folliculocystic and collagen hamartoma: A lesser-known presentation of tuberous sclerosis. Br. J. Dermatol. 2018, 178, e276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reolid, A.; Navarro, R.; Daudén, E.; Alonso-Cerezo, M.C.; Fraga, J.; Llamas-Velasco, M. Facial folliculocystic and collagen hamartoma: A variant of fibrous cephalic plaque with prominent cyst formation? J. Dtsch. Dermatol. Ges. J. Ger. Soc. Dermatol. JDDG 2019, 17, 738–741. [Google Scholar] [CrossRef]
- Santos, A.C.E.D.; Heck, B.; Camargo, B.D.; Vargas, F.R. Prevalence of Café-au-Lait Spots in children with solid tumors. Genet. Mol. Biol. 2016, 39, 232–238. [Google Scholar] [CrossRef] [Green Version]
- Bell, S.D.; MacDonald, D.M. The prevalence of café-au-lait patches in tuberous sclerosis. Clin. Exp. Dermatol. 1985, 10, 562–565. [Google Scholar] [CrossRef]
- Sachs, C.; Lipsker, D. The molluscum pendulum necklace sign in tuberous sclerosis complex: A case series A pathognomonic finding? J. Eur. Acad. Dermatol. Venereol. JEADV 2017. [Google Scholar] [CrossRef] [PubMed]
- Sachs, C.; Lipsker, D. Nevus Anemicus and Bier Spots in Tuberous Sclerosis Complex. JAMA Dermatol. 2016, 152, 217–218. [Google Scholar] [CrossRef] [Green Version]
- Lu, Q.; Shi, X.-Y.; Wang, Y.-Y.; Zhang, M.-N.; Wang, W.-Z.; Wang, J.; Wang, Q.-H.; Chen, H.-M.; Chen, H.-M.; Zou, L.-P. Juvenile xanthogranuloma as a new type of skin lesions in tuberous sclerosis complex. Orphanet J. Rare Dis. 2020, 15, 147. [Google Scholar] [CrossRef] [PubMed]
- Parker, W.E.; Orlova, K.A.; Heuer, G.G.; Baybis, M.; Aronica, E.; Frost, M.; Wong, M.; Crino, P.B. Enhanced epidermal growth factor, hepatocyte growth factor, and vascular endothelial growth factor expression in tuberous sclerosis complex. Am. J. Pathol. 2011, 178, 296–305. [Google Scholar] [CrossRef] [PubMed]
- Uitto, J.; Santa Cruz, D.J.; Eisen, A.Z. Connective tissue nevi of the skin. Clinical, genetic, and histopathologic classification of hamartomas of the collagen, elastin, and proteoglycan type. J. Am. Acad. Dermatol. 1980, 3, 441–461. [Google Scholar] [CrossRef]
- Arora, H.; Falto-Aizpurua, L.; Cortés-Fernandez, A.; Choudhary, S.; Romanelli, P. Connective Tissue Nevi: A Review of the Literature. Am. J. Dermatopathol. 2017, 39, 325–341. [Google Scholar] [CrossRef] [PubMed]
- McCuaig, C.C.; Vera, C.; Kokta, V.; Marcoux, D.; Hatami, A.; Thuraisingam, T.; Marton, D.; Fortier-Riberdy, G.; Powell, J. Connective tissue nevi in children: Institutional experience and review. J. Am. Acad. Dermatol. 2012, 67, 890–897. [Google Scholar] [CrossRef]
- Amato, L.; Mei, S.; Gallerani, I.; Moretti, S.; Cipollini, E.M.; Palleschi, G.M.; Fabbri, P. Familial cutaneous collagenoma: Report of an affected family. Int. J. Dermatol. 2005, 44, 315–317. [Google Scholar] [CrossRef] [PubMed]
- Gurel, M.S.; Mulayim, M.K.; Ozardali, I.; Bitiren, M. Familial cutaneous collagenoma: New affected family with prepubertal onset. J. Dermatol. 2007, 34, 477–481. [Google Scholar] [CrossRef]
- Stocchero, G.F. Storiform collagenoma: Case report. Einstein Sao Paulo Braz. 2015, 13, 103–105. [Google Scholar] [CrossRef] [PubMed]
- Kieselova, K.; Santiago, F.; Henrique, M.; Cunha, M.F. Multiple sclerotic fibromas of the skin: An important clue for the diagnosis of Cowden syndrome. BMJ Case Rep. 2017, 2017. [Google Scholar] [CrossRef] [PubMed]
- Tong, Y.; Schneider, J.A.; Coda, A.B.; Hata, T.R.; Cohen, P.R. Birt-Hogg-Dubé Syndrome: A Review of Dermatological Manifestations and Other Symptoms. Am. J. Clin. Dermatol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Weintraub, R.; Pinkus, H. Multiple fibrofolliculomas (Birt-Hogg-Dubé) associated with a large connective tissue nevus. J. Cutan. Pathol. 1977, 4, 289–299. [Google Scholar] [CrossRef]
- Pérez, A.D.A.; Yu, S.; North, J.P. Multiple cutaneous collagenomas in the setting of multiple endocrine neoplasia type 1. J. Cutan. Pathol. 2015, 42, 791–795. [Google Scholar] [CrossRef]
- Birt, A.R.; Hogg, G.R.; Dubé, W.J. Hereditary multiple fibrofolliculomas with trichodiscomas and acrochordons. Arch. Dermatol. 1977, 113, 1674–1677. [Google Scholar] [CrossRef]
- Spring, P.; Fellmann, F.; Giraud, S.; Clayton, H.; Hohl, D. Syndrome of Birt-Hogg-Dubé, a histopathological pitfall with similarities to tuberous sclerosis: A report of three cases. Am. J. Dermatopathol. 2013, 35, 241–245. [Google Scholar] [CrossRef] [PubMed]
- Misago, N.; Narisawa, Y. Fibrofolliculoma in a patient with tuberous sclerosis complex. Clin. Exp. Dermatol. 2009, 34, 892–894. [Google Scholar] [CrossRef] [PubMed]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| A. Genetic diagnostic criteria |
| Identification of either TSC1 or TSC2 pathogenic mutation is sufficient to make a definitive diagnosis of TSC |
| B. Clinical diagnostic criteria |
| Major features: |
| 1. Hypomelanotic macules (≥3, at least 5-mm diameter) |
| 2. Angiofibromas (≥3) or fibrous cephalic plaque |
| 3. Ungueal fibromas (≥2) |
| 4. Shagreen patch |
| 5. Multiple retinal hamartomas |
| 6. Cortical dysplasia |
| 7. Subependymal nodules |
| 8. Subependymal giant cell astrocytoma |
| 9. Cardiac rhabdomyoma |
| 10. Lymphangioleiomyomatosis |
| 11. Angiomyolipomas (≥2) |
| Minor features: |
| 1. «Confetti» skin lesions |
| 2. Dental enamel pits (>3) |
| 3. Intraoral fibromas (≥2) |
| 4. Retinal achromic patch |
| 5. Multiple renal cysts |
| 6. Nonrenal hamartomas |
| Fibrosis | Cellularity | Dilated Vessels | Perifollicular Fibrosis | Decreased or Fragmented Elastic Fibers | |
|---|---|---|---|---|---|
| Angiofibroma | + | ++ | ++ | 0 | ++ |
| ++ in old AF | + in old AF | ||||
| Periungueal fibroma | + to ++ | +++ | +++ | 0 | ++ |
| Fibrous cephalic plaque | +++ | + to ++ | + | ++ | +++ |
| Shagreen patches | +++ | + to ++ | + | + | +++ |
| Folliculocystic and collagen hamartoma | +++ | + | + | +++ | +++ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cascarino, M.; Leclerc-Mercier, S. Histological Patterns of Skin Lesions in Tuberous Sclerosis Complex: A Panorama. Dermatopathology 2021, 8, 236-252. https://doi.org/10.3390/dermatopathology8030029
Cascarino M, Leclerc-Mercier S. Histological Patterns of Skin Lesions in Tuberous Sclerosis Complex: A Panorama. Dermatopathology. 2021; 8(3):236-252. https://doi.org/10.3390/dermatopathology8030029
Chicago/Turabian StyleCascarino, Marine, and Stéphanie Leclerc-Mercier. 2021. "Histological Patterns of Skin Lesions in Tuberous Sclerosis Complex: A Panorama" Dermatopathology 8, no. 3: 236-252. https://doi.org/10.3390/dermatopathology8030029
APA StyleCascarino, M., & Leclerc-Mercier, S. (2021). Histological Patterns of Skin Lesions in Tuberous Sclerosis Complex: A Panorama. Dermatopathology, 8(3), 236-252. https://doi.org/10.3390/dermatopathology8030029