
Small Area Estimation of Zone-Level Malnutrition among Children under Five in Ethiopia


Abstract
:1. Introduction
2. Methods and Materials
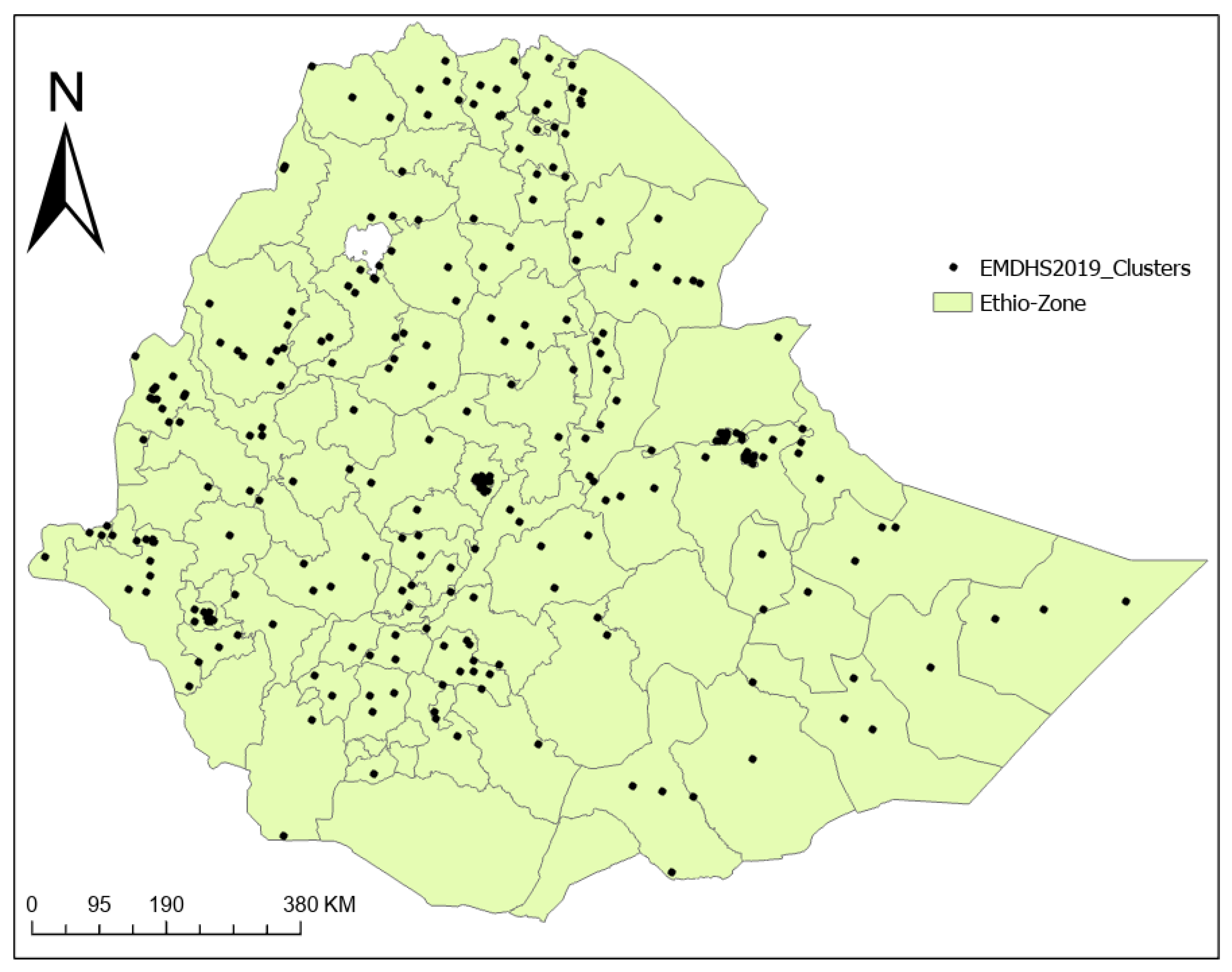
2.1. Study Setting and Design
2.2. Data Sources and Procedures
2.3. Response Variable
2.4. Auxiliary Covariates
2.5. Data Processing and Analysis
3. Results
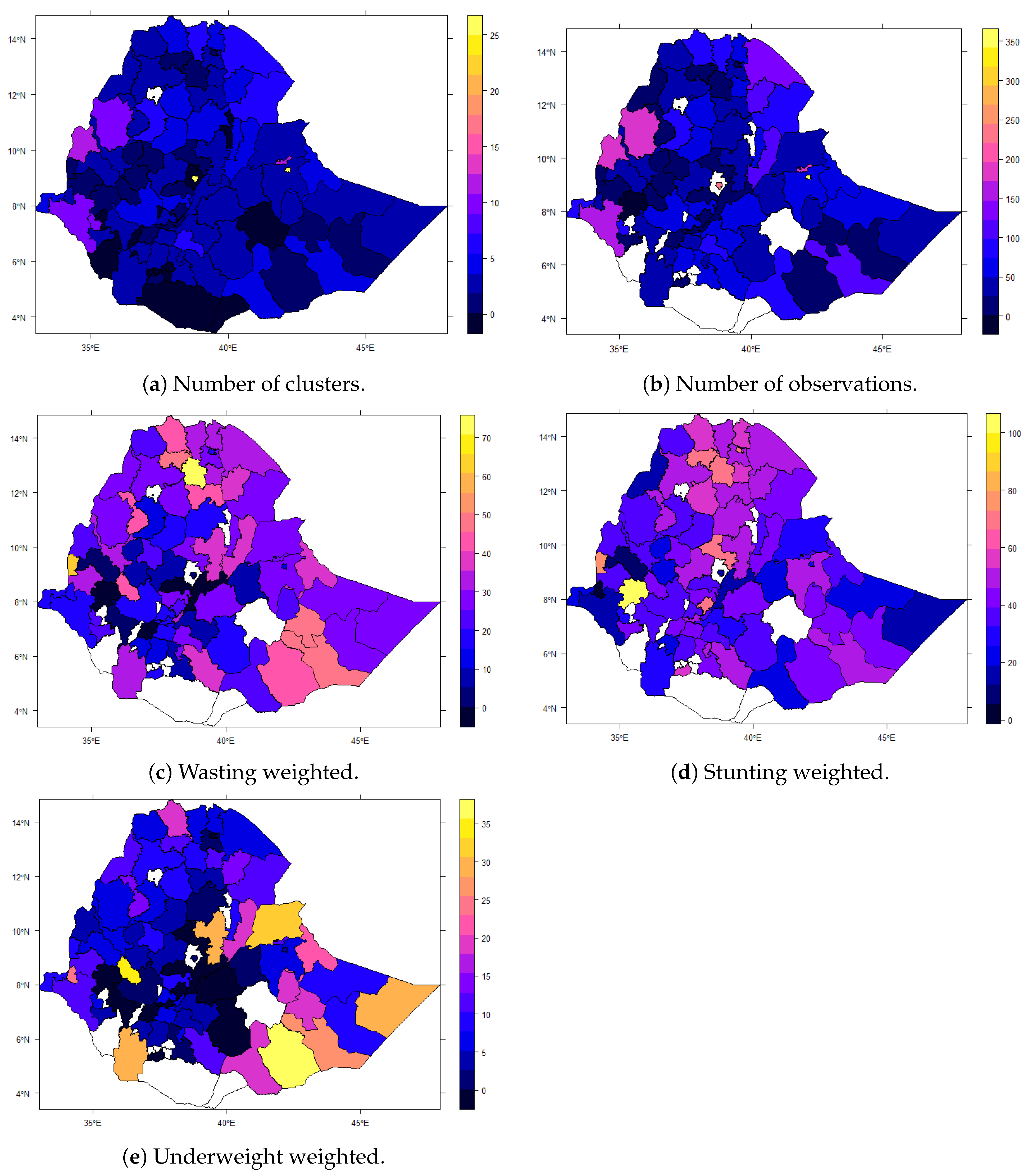
3.1. Data Description
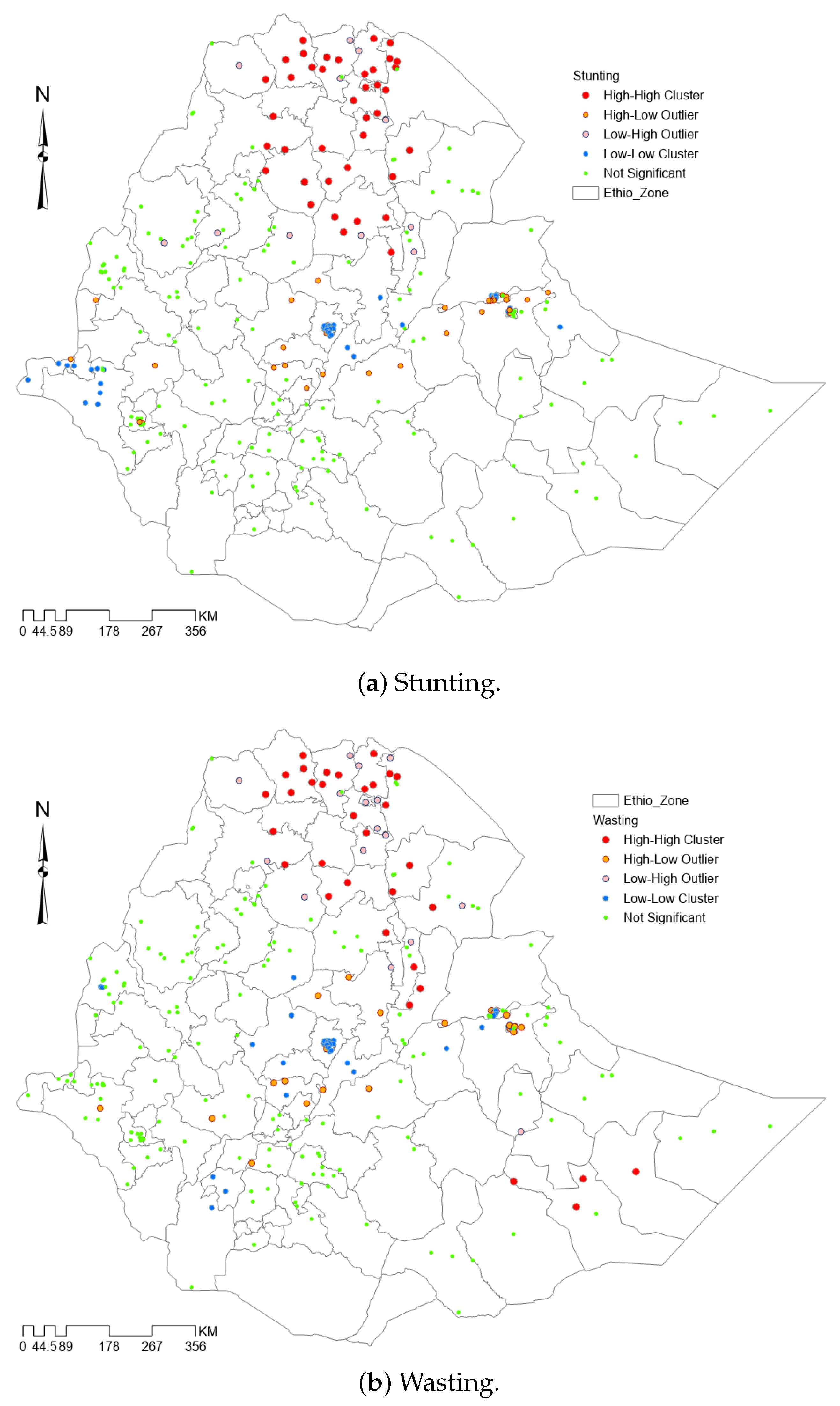
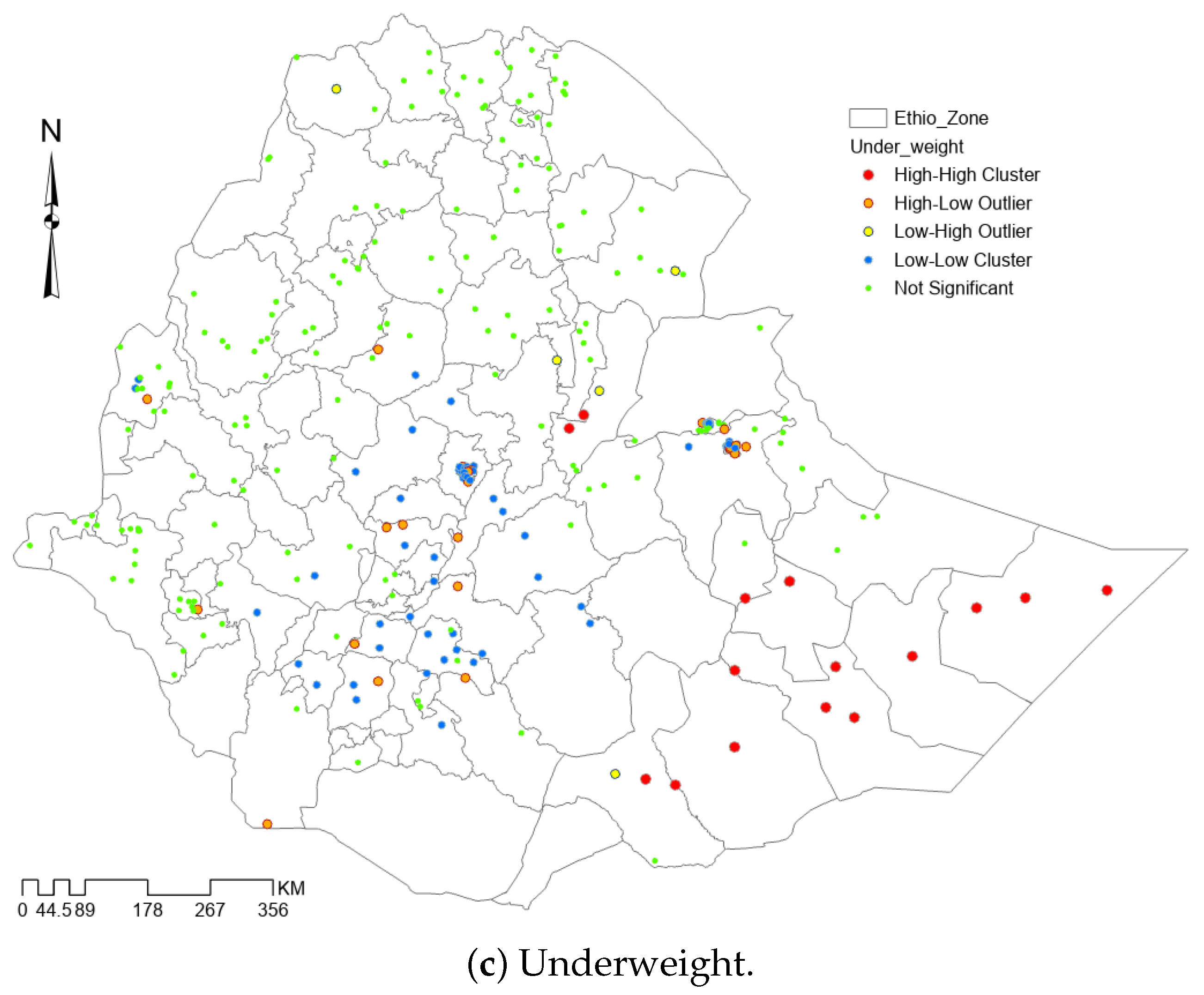
3.2. Direct Estimates of Malnutrition
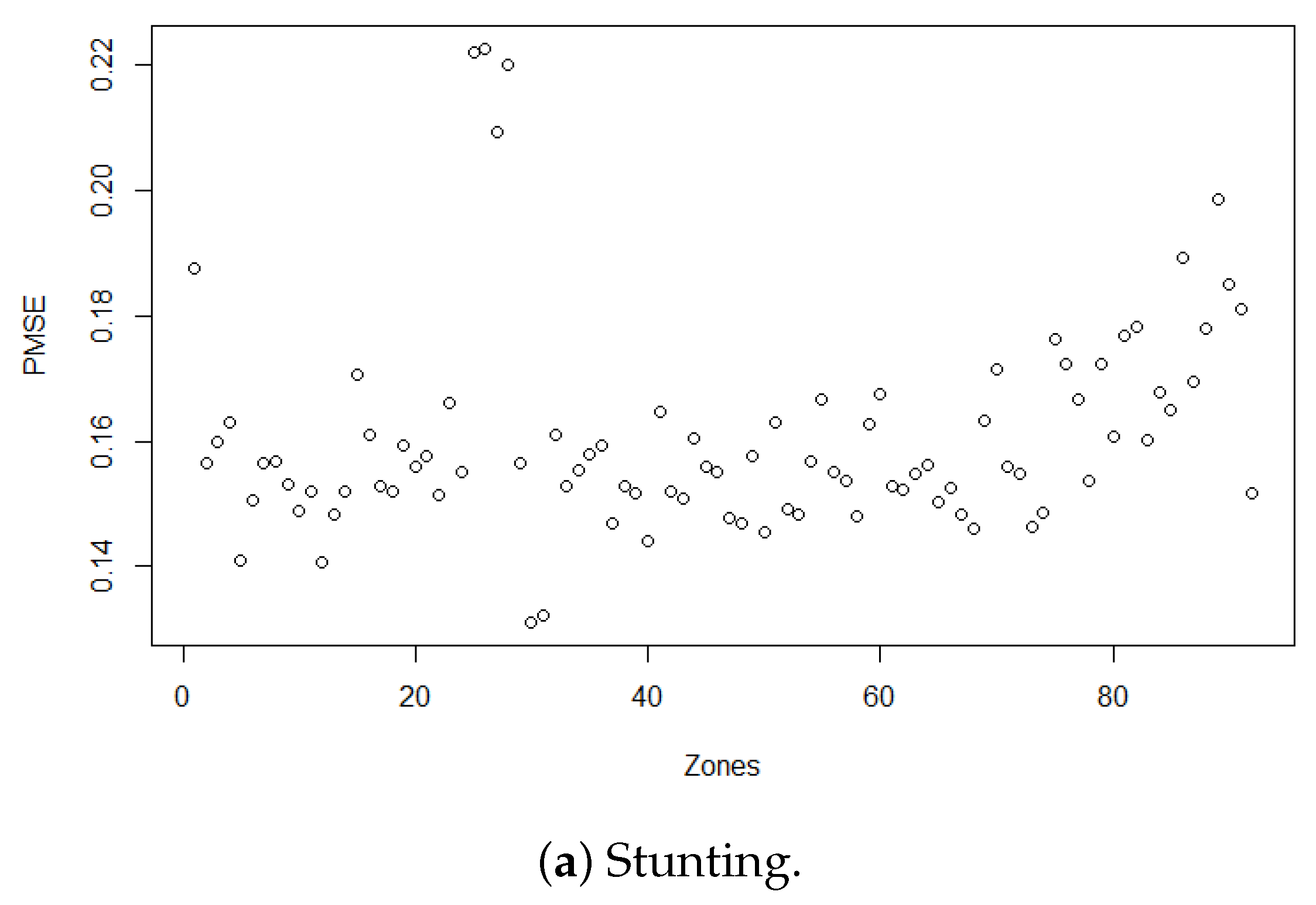
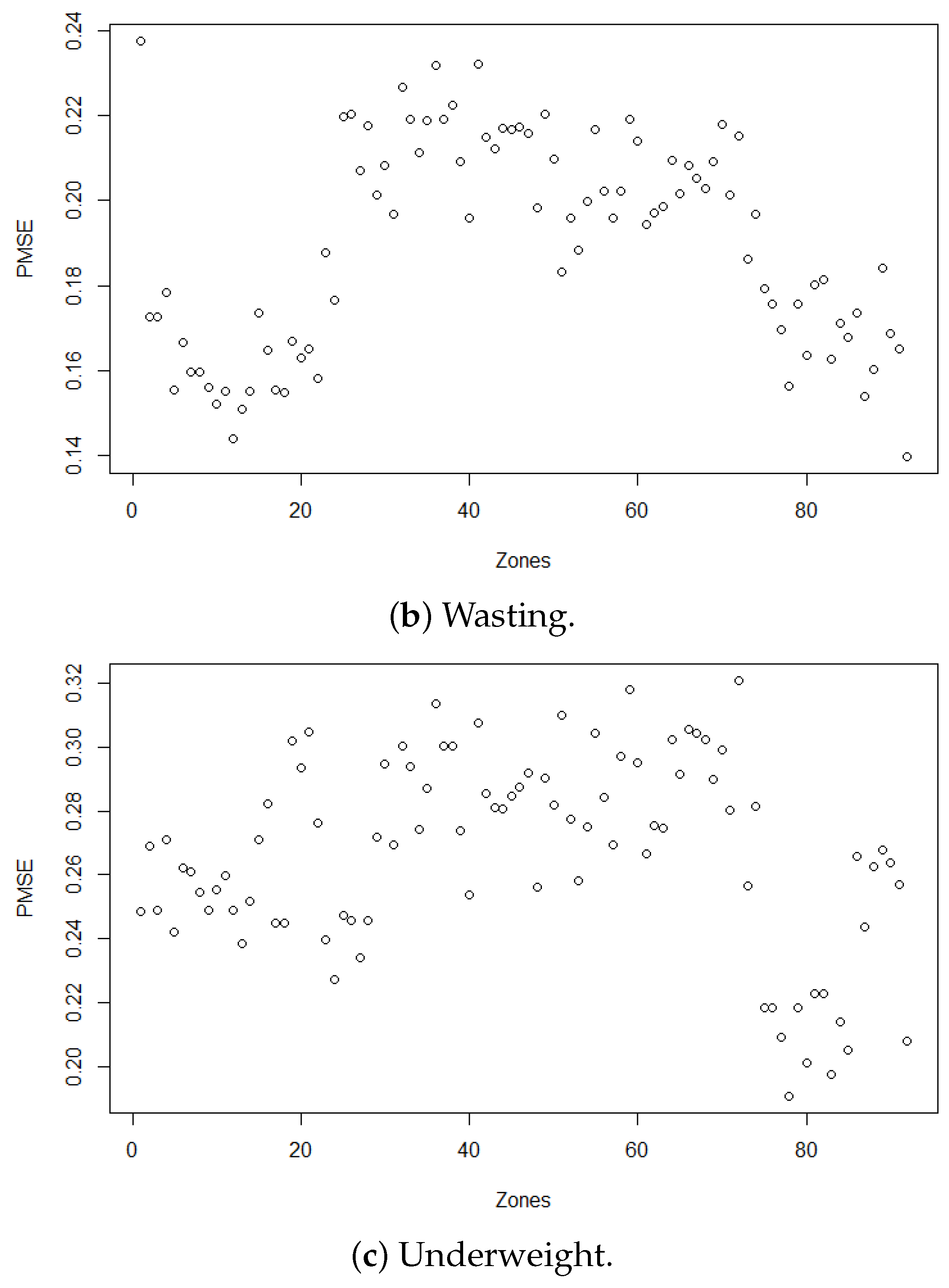
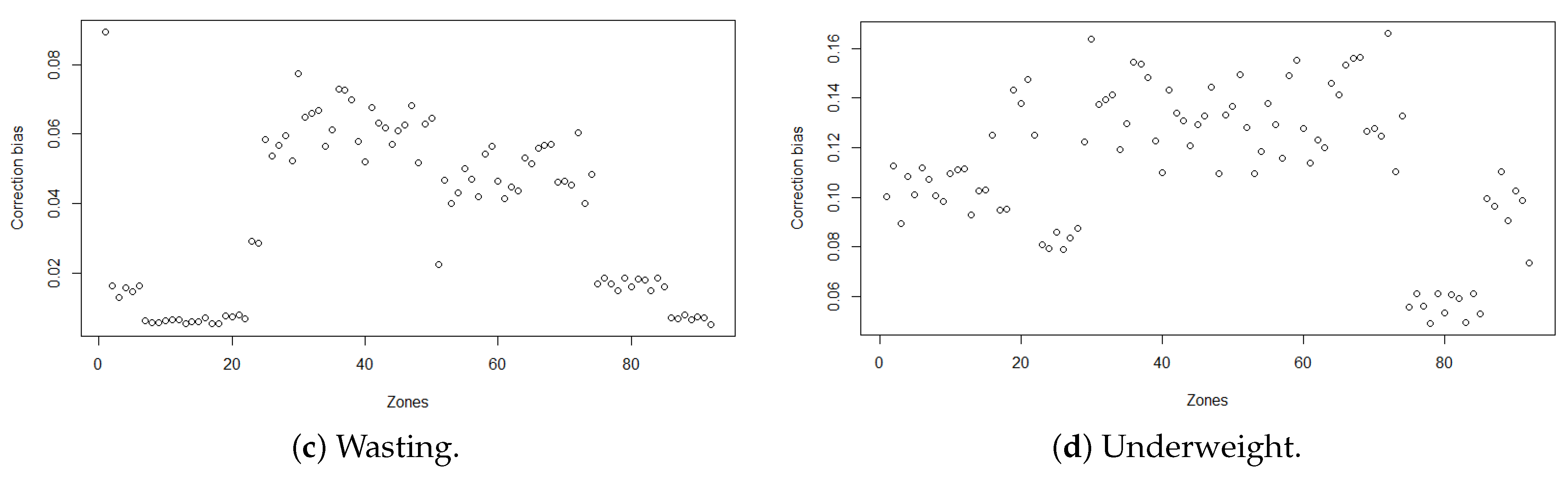
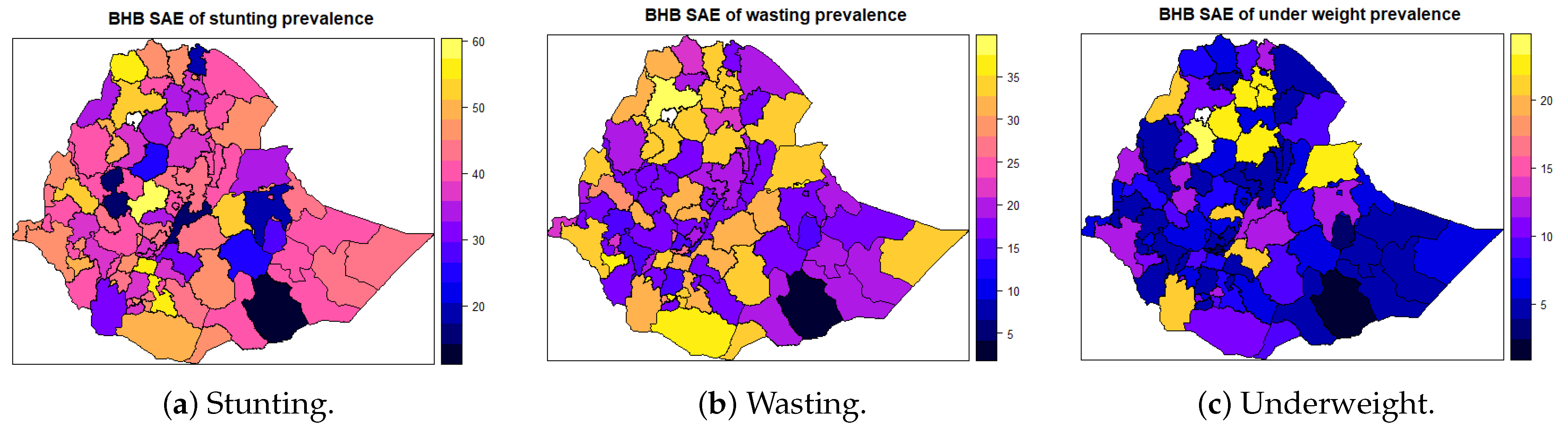
3.3. Small Area Estimates of Malnutrition
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Ethiopia Mini Demographic and Health Survey 2019. Available online: https://www.dhsprogram.com/pubs/pdf/FR363/FR363.pdf (accessed on 6 April 2022).
- Branca, F.; Grummer-Strawn, L.; Borghi, E.; Blössner, M.; Onis, M. Extension of the WHO maternal, infant and young child nutrition targets to 2030. SCN News 2015, 41, 55–58. [Google Scholar]
- Federal Democratic Republic of Ethiopia. National Nutrition Program 2016–2020; Federal Democratic Republic of Ethiopia: Addis Ababa, Ethiopia, 2016. [Google Scholar]
- WHO. Global Strategy for Women’s, Children’s and Adolescents’ Health (2016–2030); WHO: Geneva, Switzerland, 2016; Volume 20, pp. 4–103.
- Transforming Our World: The 2030 Agenda for Sustainable Development. Available online: https://sdgs.un.org/2030agenda (accessed on 6 April 2022).
- WHO. Ambition and Action in Nutrition: 2016–2025; World Health Organization: Geneva, Switzerland, 2017.
- Ainsworth, M.; Ambel, X.; Martin, G.; Sinha, S.; Huppi, M. What Can We Learn from Nutrition Impact Evaluations; Independent Evaluation Group, the World Bank: Washington, DC, USA, 2010. [Google Scholar]
- Quisumbing, A.R. Food aid and child nutrition in rural Ethiopia. World Dev. 2003, 31, 1309–1324. [Google Scholar] [CrossRef] [Green Version]
- Yamano, T.; Alderman, H.; Christiaensen, L. Child growth, shocks, and food aid in rural Ethiopia. Am. J. Agric. Econ. 2005, 87, 273–288. [Google Scholar] [CrossRef] [Green Version]
- AlemayehuAzeze, A.; Huang, W. Maternal education, linkages and child nutrition in the long and short-run: Evidence from the Ethiopia Demographic and Health Surveys. Int. J. Afr. Dev. 2014, 1, 3. [Google Scholar]
- Negash, C.; Whiting, S.J.; Henry, C.J.; Belachew, T.; Hailemariam, T.G. Association between maternal and child nutritional status in Hula, rural Southern Ethiopia: A cross sectional study. PLoS ONE 2015, 10, e0142301. [Google Scholar] [CrossRef] [PubMed]
- Dereje, N. Determinants of severe acute malnutrition among under five children in Shashogo Woreda, southern Ethiopia: A community based matched case control study. J. Nutr. Food Sci. 2014, 4, 300. [Google Scholar] [CrossRef] [Green Version]
- Ayele, D.G.; Zewotir, T.T.; Mwambi, H.G. Structured additive regression models with spatial correlation to estimate under-five mortality risk factors in Ethiopia. BMC Public Health 2015, 15, 268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mekonnen, A.; Jones, N.; Tefera, B. Tackling Child Malnutrition in Ethiopia: Do the Sustainable Development Poverty Reduction Programme’s Underlying Policy Assumptions Reflect Local Realities? Young Lives: London, UK, 2005. [Google Scholar]
- Bantamen, G.; Belaynew, W.; Dube, J. Assessment of factors associated with malnutrition among under five years age children at Machakel Woreda, Northwest Ethiopia: A case control study. J. Nutr. Food Sci. 2014, 4, 1. [Google Scholar]
- Asfaw, M.; Wondaferash, M.; Taha, M.; Dube, L. Prevalence of undernutrition and associated factors among children aged between six to fifty nine months in Bule Hora district, South Ethiopia. BMC Public Health 2015, 15, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajkumar, A.S.; Gaukler, C.; Tilahun, J. Combating Malnutrition in Ethiopia: An Evidence-Based Approach for Sustained Results; World Bank Publications: Washington, DC, USA, 2011. [Google Scholar]
- Sohnesen, T.P.; Ambel, A.A.; Fisker, P.; Andrews, C.; Khan, Q. Small area estimation of child undernutrition in Ethiopian woredas. PLoS ONE 2017, 12, e0175445. [Google Scholar] [CrossRef] [PubMed]
- Wolter, K.M.; Wolter, K.M. Taylor Series Methods. In Introduction to Variance Estimation; Springer: New York, NY, USA, 2007; pp. 226–271. Available online: https://link.springer.com/chapter/10.1007/978-0-387-35099-8_6 (accessed on 6 April 2022).
- Anselin, L. Local indicators of spatial association—LISA. Geogr. Anal. 1995, 27, 93–115. [Google Scholar] [CrossRef]
- Sahu, S.K.; Gelf, A.E.; Holl, D.M. Fusing point and areal level space–time data with application to wet deposition. J. R. Stat. Soc. Ser. Appl. Stat. 2010, 59, 77–103. [Google Scholar] [CrossRef]
- Pfeffermann, D. New Important Developments in Small Area Estimation. Stat. Sci. 2013, 28, 40–68. [Google Scholar] [CrossRef]
- Rao, J.N.; Molina, I. Small Area Estimation; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2015. [Google Scholar]
- Elbers, C.; Lanjouw, J.O.; Lanjouw, P. Micro-level estimation of poverty and inequality. Econometrica 2003, 71, 355–364. [Google Scholar] [CrossRef]
- Betti, G.; Dabalen, A.; Ferré, C.; Neri, L. Updating poverty maps between Censuses: A case study of Albania. In Poverty and Exclusion in the Western Balkans; Springer: Berlin/Heidelberg, Germany, 2013; pp. 55–70. [Google Scholar]
- Ghosh, M.; Natarajan, K.; Stroud, T.W.F.; Carlin, B.P. Generalized Linear Models for Small-Area Estimation. J. Am. Stat. Assoc. 1998, 93, 273–282. [Google Scholar] [CrossRef]
- Bakar, K.S.; Biddle, N.; Kokic, P.; Jin, H. A Bayesian spatial categorical model for prediction to overlapping geographical areas in sample surveys. J. R. Stat. Soc. Ser. Stat. Soc. 2020, 183, 535–563. [Google Scholar] [CrossRef]
- Muchie, K.F.; Wanjoya, A.K.; Mwalili, S.M. A Simulation Study of Hierarchical Bayesian Fusion Spatial Small Area Model for Binary Outcome under Spatial Misalignment. Open J. Stat. 2021, 11, 993–1009. [Google Scholar] [CrossRef]
- Orey, S. An ergodic theorem for Markov chains. Z. Wahrscheinlichkeitstheorie Verwandte Geb. 1962, 1, 174–176. [Google Scholar] [CrossRef]
- You, Y.; Rao, J.; Dick, J. Benchmarking hierarchical Bayes small area estimators with application in census undercoverage estimation. In Proceedings of the Survey Methods Section, 2002 Annual Meeting in Hamilton, Hamilton, ON, Canada, 26–29 May 2002; pp. 86–90. [Google Scholar]
- WHO. The Double Burden of Malnutrition-Policy Brief; WHO: Geneva, Switzerland, 2016.
- WHO. The State of Food Security and Nutrition in the World 2018: Building Climate Resilience for Food Security and Nutrition; Food and Agriculture Organization: Rome, Italy, 2018.
- African Union Commission; NEPAD Planning and Coordinating Agency; UN Economic Commission for Africa; UN World Food Programme. The Cost of Hunger in Africa: Social and Economic Impact of Child Undernutrition in Egypt, Ethiopia, Swaziland and Uganda; United States Agency for International Development: Washington, DC, USA, 2013. [Google Scholar]
- National Nutrition Programme June 2013–June 2015; Government of Federal Democratic Republic of Ethiopia: Addis Ababa, Ethiopia, 2013; Available online: https://www.medbox.org/pdf/5e148832db60a2044c2d2ccb (accessed on 6 April 2022).
- Swinburn, B.A.; Kraak, V.I.; Allender, S.; Atkins, V.J.; Baker, P.I.; Bogard, J.R.; Brinsden, H.; Calvillo, A.; De Schutter, O.; Devarajan, R.; et al. The global syndemic of obesity, undernutrition, and climate change: The Lancet Commission report. Lancet 2019, 393, 791–846. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Indicator | Prevalence | SE | 95% CI |
|---|---|---|---|
| Stunted | 38.9 | 1.29 | [36.38, 41.45] |
| Wasting | 22.5 | 1.36 | [19.81, 25.14] |
| Underweight | 6.9 | 0.53 | [5.82, 7.89] |
| Measure | Underweight | Stunting | Wasting |
|---|---|---|---|
| Moran’s Index | 0.218227 | 0.395968 | 0.372278 |
| Expected Index | −0.003289 | −0.003289 | −0.003289 |
| Variance | 0.002098 | 0.002122 | 0.002118 |
| z-score | 4.836414 | 8.667563 | 8.160307 |
| p-value | 0.000001 | 0.000000 | 0.000000 |
| Parameters | ||||||
|---|---|---|---|---|---|---|
| Z-value | 1.71403 | 0.32273 | 0.03037 | −0.05075 | 0.46410 | 0.19037 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muchie, K.F.; Wanjoya, A.K.; Mwalili, S.M. Small Area Estimation of Zone-Level Malnutrition among Children under Five in Ethiopia. Math. Comput. Appl. 2022, 27, 44. https://doi.org/10.3390/mca27030044
Muchie KF, Wanjoya AK, Mwalili SM. Small Area Estimation of Zone-Level Malnutrition among Children under Five in Ethiopia. Mathematical and Computational Applications. 2022; 27(3):44. https://doi.org/10.3390/mca27030044
Chicago/Turabian StyleMuchie, Kindie Fentahun, Anthony Kibira Wanjoya, and Samuel Musili Mwalili. 2022. "Small Area Estimation of Zone-Level Malnutrition among Children under Five in Ethiopia" Mathematical and Computational Applications 27, no. 3: 44. https://doi.org/10.3390/mca27030044
APA StyleMuchie, K. F., Wanjoya, A. K., & Mwalili, S. M. (2022). Small Area Estimation of Zone-Level Malnutrition among Children under Five in Ethiopia. Mathematical and Computational Applications, 27(3), 44. https://doi.org/10.3390/mca27030044