
The Effect of Sound in the Dental Office: Practices and Recommendations for Quality Assurance—A Narrative Review



Abstract
:1. Introduction
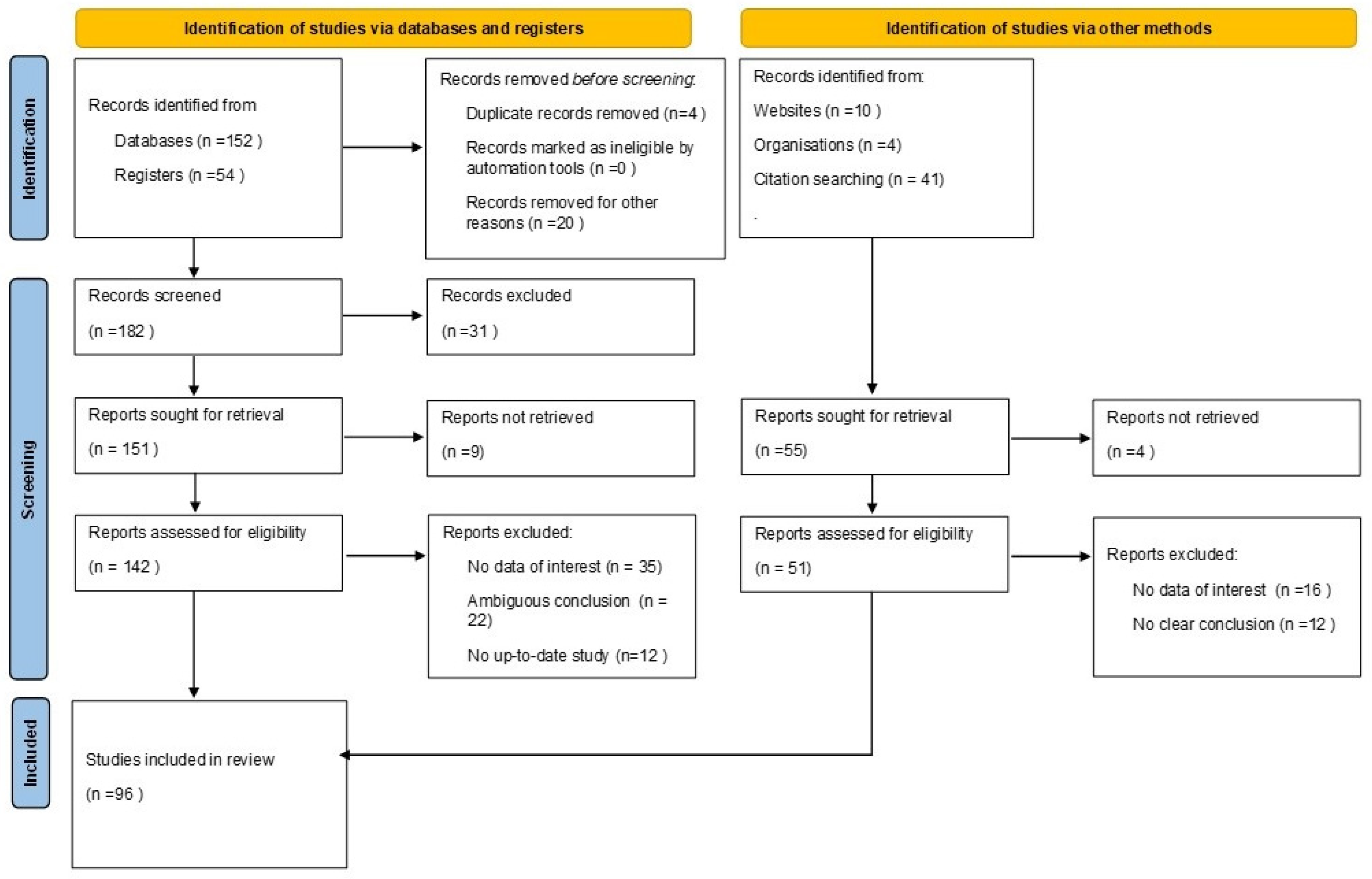
2. Materials and Methods
3. Sound Types and Levels in the Dental Office
4. Effect of Noise in the Dental Office
5. Positive Aspects of Sound in the Dental Office
6. Mechanism of Healing Effect of Sound and Music in the Dental Office
7. Options of Sound Control Design in the Dental Office
8. Discussion
9. Limitations of the Study
10. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hodge, B.; Thompson, J.F. Noise pollution in the operating theatre. Lancet 1990, 335, 891–894. [Google Scholar] [CrossRef] [PubMed]
- Hasfeldt, D.; Laerkner, E.; Birkelund, R. Noise in the operating room—What do we know? A review of the literature. J. Perianesthesia Nurs. 2010, 25, 380–386. [Google Scholar] [CrossRef] [PubMed]
- Kühlmann, A.Y.R. The Sound of Medicine: Evidence-Based Music Interventions in Healthcare Practice; Erasmus University Rotterdam: Rotterdam, The Netherlands, 2019. [Google Scholar]
- Antoniadou, M. Application of Humanities and Basic Principles of Coaching in Health Studies; Tsiotras Publications: Athens, Greece, 2021. [Google Scholar]
- McGeoch, P.D.; Rouw, R. How everyday sounds can trigger strong emotions: ASMR, misophonia and the feeling of wellbeing. Bioessays 2020, 42, e2000099. [Google Scholar] [CrossRef]
- Packyanathan, J.S.; Lakshmanan, R.; Jayashri, P. Effect of music therapy on anxiety levels on patient undergoing dental extractions. J. Fam. Med. Prim. Care 2019, 8, 3854–3860. [Google Scholar] [CrossRef]
- Ainscough, S.L.; Windsor, L.; Tahmassebi, J.F. A review of the effect of music on dental anxiety in children. Eur. Arch. Paediatr. Dent. 2019, 20, 23–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, A.; Ahmed, B. Experience of listening to music on patient anxiety during minor oral surgery procedures: A pilot study. Br. Dent. J. 2020, 228, 89–92. [Google Scholar] [CrossRef]
- Navit, S.; Johri, N.; Khan, S.A.; Singh, R.K.; Chadha, D.; Navit, P.; Sharma, A.; Bahuguna, R. Effectiveness and Comparison of Various Audio Distraction Aids in Management of Anxious Dental Paediatric Patients. J. Clin. Diagn. Res. 2015, 9, ZC05-9. [Google Scholar] [CrossRef]
- Chen, Y.; Hawkins, J. Effects of music listening to reduce preprocedural dental anxiety in special needs patients. Complement. Ther. Clin. Pract. 2021, 42, 101279. [Google Scholar] [CrossRef]
- Moola, S.; Pearson, A.; Hagger, C. Effectiveness of music interventions on dental anxiety in paediatric and adult patients: A systematic review. JBI Libr. Syst. Rev. 2011, 9, 588–630. [Google Scholar] [CrossRef]
- Potgieter, I.; MacDonald, C.; Partridge, L.; Cima, R.; Sheldrake, J.; Hoare, D.J. Misophonia: A scoping review of research. J. Clin. Psychol. 2019, 75, 1203–1218. [Google Scholar] [CrossRef]
- Nilsson, U. The anxiety and pain reducing effects of music interventions: A systematic review. AORN J. 2008, 87, 780–807. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Montague, K.; Blietz, C.; Kachur, M.; Cert, B. Ensuring Quieter Hospital Environments. Am. J. Nurs. 2009, 109, 65–67. [Google Scholar] [CrossRef] [Green Version]
- Birardi, V.; Pasini, F. Study about the effects of dental noises on the emotional experiences of children aged 6 to 10 years. A pilot study. Eur. J. Paediatr. Dent. 2011, 12, 236–238. [Google Scholar]
- Shapiro, M.; Melmed, R.N.; Sgan-Cohen, H.D.; Eli, I.; Parush, S. Behavioural and physiological effect of dental environment sensory adaptation on children’s dental anxiety. Eur. J. Oral Sci. 2007, 115, 479–483. [Google Scholar] [CrossRef]
- Muppa, R.; Bhupatiraju, P.; Duddu, M.; Penumatsa, N.V.; Dandempally, A.; Panthula, P. Comparison of anxiety levels associated with noise in the dental clinic among children of age group 6–15 years. Noise Health 2013, 15, 190–193. [Google Scholar] [CrossRef] [PubMed]
- Ai, Z.T.; Mak, C.M.; Wong, H.M. Noise level and its influences on dental professionals in a dental hospital in Hong Kong. Build. Serv. Eng. Res. Technol. 2017, 38, 522–535. [Google Scholar] [CrossRef]
- Yu, J.F.; Lee, K.C.; Hong, H.H.; Kuo, S.B.; Wu, C.D.; Wai, Y.Y. Human amygdala activation by the sound produced during dental treatment: A fMRI study. Noise Health 2015, 17, 337–342. [Google Scholar] [CrossRef]
- Brusis, T.; Hilger, R.; Niggeloh, R.; Huedepohl, J.; Thiesen, K.W. Bestehtbeimzahnarztoderbeimzahntechniker die gefahreinerlärmbedingtengehörschädigung? [Are professional dental health care workers (dentists, dental technicians, assistants) in danger of noise induced hearing loss?]. Laryngorhinootologie 2008, 87, 335–340. (In German) [Google Scholar] [CrossRef]
- Dierickx, M.; Verschraegen, S.; Wierinck, E.; Willems, G.; van Wieringen, A. Noise Disturbance and Potential Hearing Loss Due to Exposure of Dental Equipment in Flemish Dentists. Int. J. Environ. Res. Public Health 2021, 18, 5617. [Google Scholar] [CrossRef]
- Setcos, J.C.; Mahyuddin, A. Noise levels encountered in dental clinical and laboratory practice. Int. J. Prosthodont. 1998, 11, 150–157. [Google Scholar] [PubMed]
- Amine, M.; Aljalil, Z.; Redwane, A.; Delfag, I.; Lahby, I.; Bennani, A. Assessment of Noise Levels of Equipment Used in the Practical Dental Teaching Activities. Int. J. Dent. 2021, 2021, 6642560. [Google Scholar] [CrossRef] [PubMed]
- Shields, W. Noise Hazards in the Practice of Dentistry; Report No. AD-A078-221; Army Inst of Dental Research: Washington, DC, USA, 1979. [Google Scholar]
- Kilpatrick, H.C. Decibel ratings of dental office sounds. J. Prosthet. Dent. 1981, 45, 175–178. [Google Scholar] [CrossRef] [PubMed]
- Sampaio Fernandes, J.C.; Carvalho, A.P.; Gallas, M.; Vaz, P.; Matos, P.A. Noise levels in dental schools. Eur. J. Dent. Educ. 2006, 10, 32–37. [Google Scholar] [CrossRef]
- Kadanakuppe, S.; Bhat, P.K.; Jyothi, C.; Ramegowda, C. Assessment of noise levels of the equipments used in the dental teaching institution, Bangalore. Indian J. Dent. Res. 2011, 22, 424–431. [Google Scholar] [CrossRef]
- Chen, W.L.; Chen, C.J.; Yeh, C.Y.; Lin, C.T.; Cheng, H.C.; Chen, R.Y. Workplace noise exposure and its consequent annoyance to dentists. J. Exp. Clin. Med. 2013, 5, 177–180. [Google Scholar] [CrossRef]
- Arenas, J.P.; Suter, A.H. Comparison of occupational noise legislation in the Americas: An overview and analysis. Noise Health 2014, 16, 306–319. [Google Scholar] [CrossRef]
- Qsaibati, M.L.; Ibrahim, O. Noise levels of dental equipment used in dental college of Damascus University. Dent. Res. J. (Isfahan) 2014, 11, 624–630. [Google Scholar]
- Burk, A.; Neitzel, R.L. An exploratory study of noise exposures in educational and private dental clinics. J. Occup. Environ. Hyg. 2016, 13, 741–749. [Google Scholar] [CrossRef] [Green Version]
- Dutta, A.; Mala, K.; Acharya, S.R. Sound levels in conservative dentistry and endodontics clinic. J. Conserv. Dent. 2013, 16, 121–125. [Google Scholar] [CrossRef] [Green Version]
- Baseer, M.A.; Al Saffan, A.; AlMasoud, S.M.; Dahy, W.T.; Aldali, H.W.; Walid Bachat, A.M.; Walid Bachat, R.M.; AlMugeiren, O.M. Noise levels encountered in university dental clinics during different specialty treatments. J. Fam. Med. Prim. Care 2021, 10, 2987–2992. [Google Scholar] [CrossRef]
- Fu, V.X.; Oomens, P.; Merkus, N.; Jeekel, J. The Perception and Attitude Toward Noise and Music in the Operating Room: A Systematic Review. J. Surg. Res. 2021, 263, 193–206. [Google Scholar] [CrossRef] [PubMed]
- Hill, J.N.; LaVela, S.L. Noise Levels in Patient Rooms and at Nursing Stations at Three VA Medical Centers. HERD 2015, 9, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Nissan, S.; Yochman, A.; Blumer, S.; Kharouba, J.; Peretz, B. Children’s responses to sensory stimuli and their behavior in the dental office. J. Clin. Pediatric Dent. 2017, 41, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Basner, M.; Babisch, W.; Davis, A.; Brink, M.; Clark, C.; Janssen, S.; Stansfeld, S. Auditory and non-auditory effects of noise on health. Lancet 2014, 383, 1325–1332. [Google Scholar] [CrossRef] [Green Version]
- Cabrera, I.N.; Lee, M.H. Reducing noise pollution in the hospital setting by establishing a department of sound: A survey of recent research on the effects of noise and music in health care. Prev. Med. 2000, 30, 339–345. [Google Scholar] [CrossRef]
- Ma, K.W.; Wong, H.M.; Mak, C.M. Dental Environmental Noise Evaluation and Health Risk Model Construction to Dental Professionals. Int. J. Environ. Res. Public Health 2017, 14, 1084. [Google Scholar] [CrossRef] [Green Version]
- Khaimook, W.; Suksamae, P.; Choosong, T.; Chayarpham, S.; Tantisarasart, R. The prevalence of noise-induced occupational hearing loss in dentistry personnel. Workplace Health Saf. 2014, 62, 357–360. [Google Scholar] [CrossRef]
- Engelmann, C.R.; Neis, J.P.; Kirschbaum, C.; Grote, G.; Ure, B.M. A noise-reduction program in a pediatric operation theatre is associated with surgeon’s benefits and a reduced rate of complications: A prospective controlled clinical trial. Ann. Surg. 2014, 259, 1025–1033. [Google Scholar] [CrossRef]
- Peng, L.; Chen, J.; Jiang, H. The impact of operating room noise levels on stress and work efficiency of the operating room team: A protocol for systematic review and meta-analysis. Medicine 2022, 101, e28572. [Google Scholar] [CrossRef]
- Friedrich, M.G.; Boos, M.; Pagel, M. New technical solution to minimise noise exposure for surgical staff: The ‘silent operating theatre optimisation system’. BMJ Innov. 2017, 3, 196e205. [Google Scholar] [CrossRef]
- Medicinanarrativa. Available online: https://www.medicinanarrativa.eu/sound-therapy-and-well-being-some-scientific-studies} (accessed on 15 September 2022).
- Soulveda. Available online: https://www.soulveda.com/wellbeing/sound-healing-in-ancient-egypt/ (accessed on 21 September 2022).
- Thaut, M.H. Music as therapy in early history. Prog. Brain Res. 2015, 217, 143–158. [Google Scholar] [CrossRef] [PubMed]
- Sheppard, A.; Broughton, M.C. Promoting wellbeing and health through active participation in music and dance: A systematic review. Int. J. Qual. Stud. Health Well-Being 2020, 15, 1732526. [Google Scholar] [CrossRef] [Green Version]
- Appukuttan, D.P. Strategies to manage patients with dental anxiety and dental phobia: Literature review. Clin. Cosmet. Investig. Dent. 2016, 8, 35–50. [Google Scholar] [CrossRef] [Green Version]
- Klassen, J.A.; Liang, Y.; Tjosvold, L.; Klassen, T.P.; Hartling, L. Music for pain and anxiety in children undergoing medical procedures: A systematic review of randomized controlled trials. Ambul. Pediatr. 2008, 8, 117–128. [Google Scholar] [CrossRef] [PubMed]
- Ullmann, Y.; Fodor, L.; Schwarzberg, I.; Carmi, N.; Ullmann, A.; Ramon, Y. The sounds of music in the operating room. Injury 2008, 39, 592–597. [Google Scholar] [CrossRef]
- Oomens, P.; Fu, V.X.; Kleinrensink, G.J.; Jeekel, J. The effect of music on simulated surgical performance: A systematic review. Surg. Endosc. 2019, 33, 2774–2784. [Google Scholar] [CrossRef] [Green Version]
- Bechtold, M.L.; Puli, S.R.; Othman, M.O.; Bartalos, C.R.; Marshall, J.B.; Roy, P.K. Effect of music on patients undergoing colonoscopy: A meta-analysis of randomized controlled trials. Dig. Dis. Sci. 2009, 54, 19–24. [Google Scholar] [CrossRef]
- Nickel, A.K.; Hillecke, T.; Argstatter, H.; Bolay, H.V. Outcome research in music therapy: A step on the long road to an evidence-based treatment. Ann. N. Y. Acad. Sci. 2005, 1060, 283–293. [Google Scholar] [CrossRef]
- Khalfa, S.; Bella, S.D.; Roy, M.; Peretz, I.; Lupien, S.J. Effects of relaxing music on salivary cortisol level after psychological stress. Ann. N. Y. Acad. Sci. 2003, 999, 374–376. [Google Scholar] [CrossRef]
- Corah, N.L.; Gale, E.N.; Pace, L.F.; Seyrek, S.K. Relaxation and musical programming as means of reducing psychological stress during dental procedures. J. Am. Dent. Assoc. 1981, 103, 232–234. [Google Scholar] [CrossRef] [PubMed]
- Thoma, M.V.; Zemp, M.; Kreienbühl, L.; Hofer, D.; Schmidlin, P.R.; Attin, T.; Ehlert, U.; Nater, U.M. Effects of Music Listening on Pre-treatment Anxiety and Stress Levels in a Dental Hygiene Recall Population. Int. J. Behav. Med. 2015, 22, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Bradt, J.; Dileo, C.; Shim, M. Music interventions for preoperative anxiety. Cochrane Database Syst. Rev. 2013, 6, CD006908. [Google Scholar] [CrossRef] [PubMed]
- Sound Healing Research Foundation. Available online: https://soundhealingresearchfoundation.org/research_paper%20%20Research%20Paper/effects-vibroacoustic-music-symptom-reduction-inducing-relaxation-response-good-vibrations-dr-george-patrick/ (accessed on 15 February 2022).
- Pietschnig, J.; Voracek, M.; Formann, A.K. Mozart effect-Shmozart effect: A meta-analysis. Intelligence 2010, 38, 314–323. [Google Scholar] [CrossRef]
- Wolf, L.; Wolf, T. Music and Healthcare. A Paper Commissioned by the Musical Connections Program of Carnegie Hall’s Weill Music Institute. August 2011. Available online: https://culturehive.co.uk/wp-content/uploads/2014/01/Music_and_Health_Care.pdf (accessed on 23 August 2022).
- Aitken, J.C.; Wilson, S.; Coury, D.; Moursi, A.M. The effect of music distraction on pain, anxiety and behavior in pediatric dental patients. Pediatric Dent. 2002, 24, 114–118. [Google Scholar]
- Gujjar, K.R.; van Wijk, A.; Kumar, R.; de Jongh, A. Are Technology-Based Interventions Effective in Reducing Dental Anxiety in Children and Adults? A Systematic Review. J. Evid. Based Dent. Pract. 2019, 19, 140–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frere, C.L.; Crout, R.; Yorty, J.; McNeil, D.W. Effects of audiovisual distraction during dental prophylaxis. J. Am. Dent. Assoc. 2001, 132, 1031–1038. [Google Scholar] [CrossRef] [Green Version]
- López-Valverde, N.; Muriel Fernández, J.; López-Valverde, A.; Valero Juan, L.F.; Ramírez, J.M.; Flores Fraile, J.; Herrero Payo, J.; Blanco Antona, L.A.; Macedo de Sousa, B.; Bravo, M. Use of Virtual Reality for the Management of Anxiety and Pain in Dental Treatments: Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 3086. [Google Scholar] [CrossRef]
- Birnie, K.A.; Noel, M.; Chambers, C.T.; Uman, L.S.; Parker, J.A. Psychological interventions for needle-related procedural pain and distress in children and adolescents. Cochrane Database Syst. Rev. 2018, 10, CD005179. [Google Scholar] [CrossRef]
- Music Therapy Unit, of the Royal Children’s Hospital in Melbourne. 2004. Available online: https://www.rch.org.au/uploadedFiles/Main/Content/ept/RCH_guidelines_RecordedMusic.pdf (accessed on 30 April 2022).
- Marwah, N.; Prabhakar, A.R.; Raju, O.S. Music distraction—Its efficacy in management of anxious pediatric dental patients. J. Indian Soc. Pedod. Prev. Dent. 2005, 23, 168–170. [Google Scholar] [CrossRef]
- Kühlmann, A.Y.R.; de Rooij, A.; Kroese, L.F.; van Dijk, M.; Hunink, M.G.M.; Jeekel, J. Meta-analysis evaluating music interventions for anxiety and pain in surgery. Br. J. Surg. 2018, 105, 773–783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hauck, M.; Metzner, S.; Rohlffs, F.; Lorenz, J.; Engel, A.K. The influence of music and music therapy on pain-induced neuronal oscillations measured by magnetencephalography. Pain 2013, 154, 539–547. [Google Scholar] [CrossRef] [PubMed]
- Koelsch, S. A neuroscientific perspective on music therapy. Ann. N. Y. Acad. Sci. 2009, 1169, 374–384. [Google Scholar] [CrossRef] [PubMed]
- Hinton, D.E.; Kirmayer, L.J. The Flexibility Hypothesis of Healing. Cult. Med. Psychiatry 2017, 41, 3–34. [Google Scholar] [CrossRef]
- Levitin, D.J.; Tirovolas, A.K. Current advances in the cognitive neuroscience of music. Ann. N. Y. Acad. Sci. 2009, 1156, 211–231. [Google Scholar] [CrossRef]
- Andrade, P.E.; Bhattacharya, J. Not Cure But Heal: Music and Medicine. Adv. Neurobiol. 2018, 21, 283–307. [Google Scholar] [CrossRef]
- Trainor, L.J.; Schmidt, L.A. Processing emotions induced by music. In The Cognitive Neuroscience of Music; Peretz, I., Zatorre, R., Eds.; Oxford University Press: Oxford, UK, 2003; pp. 311–324. [Google Scholar] [CrossRef]
- Peretz, I.; Zatorre, R.J. Brain organization for music processing. Annu. Rev. Psychol. 2005, 56, 89–114. [Google Scholar] [CrossRef] [Green Version]
- Koelsch, S. Investigating emotion with music: Neuroscientific approaches. Ann. N. Y. Acad. Sci. 2005, 1060, 412–418. [Google Scholar] [CrossRef] [Green Version]
- The British Academy of Sound Therapy. Available online: https://www.britishacademyofsoundtherapy.com/sound-affects/ (accessed on 30 April 2022).
- Batt-Rawden, K. The role of music in a salutogenic approach to health. Int. J. Ment. Health Promot. 2010, 12, 11–18. [Google Scholar] [CrossRef]
- Biddiss, E.; Knibbe, T.J.; McPherson, A. The effectiveness of interventions aimed at reducing anxiety in health care waiting spaces: A systematic review of randomized and nonrandomized trials. Anesth. Analg. 2014, 119, 433–448. [Google Scholar] [CrossRef]
- Jiang, S. Positive Distractions and Play in the Public Spaces of Pediatric Healthcare Environments: A Literature Review. HERD 2020, 13, 171–197. [Google Scholar] [CrossRef] [PubMed]
- Harris, D.D. The influence of flooring on environmental stressors: A study of three flooring materials in a hospital. HERD 2015, 8, 9–29. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Kim, J.M. Deflection of resilient materials for reduction of floor impact sound. Sci. World J. 2014, 2014, 612608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fediuk, R.; Amran, M.; Vatin, N.; Vasilev, Y.; Lesovik, V.; Ozbakkaloglu, T. Acoustic Properties of Innovative Concretes: A Review. Materials 2021, 14, 398. [Google Scholar] [CrossRef] [PubMed]
- Acoustiblok UK Ltd.; Thermablok Aerogel Ltd. Available online: https://www.acoustiblok.co.uk/soundproofing-materials/ (accessed on 16 May 2022).
- Walker, L.; Karl, C.A. The Hospital (Not So) Quiet Zone: Creating an Environment for Patient Satisfaction Through Noise Reduction Strategies. HERD 2019, 12, 197–202. [Google Scholar] [CrossRef]
- Wang, Z.; Downs, B.; Farell, A.; Cook, K.; Hourihan, P.; McCreery, S. Role of a service corridor in ICU noise control, staff stress, and staff satisfaction: Environmental research of an academic medical center. HERD 2013, 6, 80–94. [Google Scholar] [CrossRef]
- Ali, M.; Almuzaiqer, R.; Al-Salem, K.; Alabdulkarem, A.; Nuhait, A. New novel thermal insulation and sound-absorbing materials from discarded facemasks of COVID-19 pandemic. Sci. Rep. 2021, 11, 23240. [Google Scholar] [CrossRef]
- Johansson, L.; Lindahl, B.; Knutsson, S.; Ögren, M.; Persson Waye, K.; Ringdal, M. Evaluation of a sound environment intervention in an ICU: A feasibility study. Aust. Crit. Care 2018, 31, 59–70. [Google Scholar] [CrossRef] [Green Version]
- Monagahn, D.M.; Wilson, N.H.; Darvell, B.W. The performance of air-turbine handpieces in general dental practice. Oper. Dent. 2005, 30, 16–25. [Google Scholar]
- Lu, S.Y.; Huang, Y.H.; Lin, K.Y. Spectral content (colour) of noise exposure affects work efficiency. Noise Health 2020, 22, 19–27. [Google Scholar] [CrossRef]
- Friedrich, M.G.; Tirilomis, T.; Kollmeier, J.M.; Wang, Y.; Hanekop, G.G. Modifications of Surgical Suction Tip Geometry for Flow Optimisation: Influence on Suction-Induced Noise Pollution. Surg. Res. Pract. 2018, 2018, 3074819. [Google Scholar] [CrossRef] [PubMed]
- Antoniadou, M.; Tzoutzas, I.; Tzermpos, F.; Panis, V.; Maltezou, H.; Tseroni, M.; Madianos, F. Infection control during COVID-19 outbreak in a university dental school. J. Oral Hyg. Health 2020, 8, 4. [Google Scholar]
- Maltezou, H.C.; Tseroni, M.; Vorou, R.; Koutsolioutsou, A.; Antoniadou, M.; Tzoutzas, I.; Panis, V.; Tzermpos, F.; Madianos, P. Preparing dental schools to refunction safely during the COVID-19 pandemic: An infection prevention and control perspective. J. Infect. Dev. Ctries. 2021, 15, 22–31. [Google Scholar] [CrossRef]
- Pitre, C.; Pettit, K.; Ladd, L.; Chisholm, C.; Welch, J.L. Physician Time Management. MedEdPORTAL 2018, 14, 10681. [Google Scholar] [CrossRef] [PubMed]
- European Commission, Directorate-General for Environment; Kostelac Bjegovic, J. Handbook on the Implementation of EU Environmental Legislation; Publications Office: Luxembourg, 2016; Section 9. [Google Scholar]


{kind=link}
| Study | Study Type | Methods | Results | Conclusions |
|---|---|---|---|---|
| Marwah et al., 2005 [68] | Randomized Controlled Clinical Trial | 40 children (4–8 years) with no previous dental experience divided in three groups. Group A: control group, Group B: instrumental music group, Group C: nursery rhymes music group | A significant difference (p < 0.05) was observed regarding anxiety in groups B and C; higher anxiety levels in group C. A statistically significant (p < 0.05) difference was seen between the pulse rates in groups B and C, the anxiety being more in C. The values of oxygen saturation showed minimal variations during all the visits for all the groups, and the results were not statistically significant. | Audio distraction technique decreased the anxiety level but not to a very significant level. Instrumental music was the music of choice. Despite lack of any relief from pain, patients had a positive response to music and wanted to listen to it at their subsequent visits. |
| Nilsson et al., 2008 [13] | Systematic review | A systematic review of 42 randomized controlled trials of the effects of music interventions in perioperative settings. | Music intervention had positive effects on reducing patients’ anxiety and pain in approximately half of the reviewed studies. | Further research into music therapy and the potential ability of music to reduce peri-operative patient distress is needed. |
| Ullmann et al., 2008 [51] | Single descriptive study | 171 participants answered a questionnaire | Music makes 78.9% of the participants calmer and more efficient. Classical music is the most requested (58%). | Music has a positive effect on the staff working in the operating rooms. |
| Thoma et al., 2014 [57] | Randomized controlled clinical trial | 92 consecutive volunteer patients, N1 = 46, listening to music for 10 min and a control group n = 46, waiting in silence | State anxiety levels in the music group decreased significantly after intervention as compared to the control group (1/90) = 8.06; p = 0.006). | Listening to music prior to dental hygiene treatment decreases anxiety levels to a greater extent than waiting in silence. |
| Kühlmann et al., 2018 [69] | Meta-analysis | Systematic literature search- 92 RCTs | Music intervention significantly decreased anxiety and pain compared with controls, equivalent to a decrease of 21 mm for anxiety and 10 mm for pain on a 100 mm visual analogue scale. | Music intervention significantly reduces anxiety and pain in adult surgical patients. |
| Packyanathan et al., 2019 [6] | Randomized Controlled Clinical Trial | 50 patients in Saveetha Dental College were randomly selected and allocated to test group and control group. The test group (N = 25) was subjected to music during extractions and control (N = 25) was not exposed. Dental anxiety levels and hemodynamic changes were assessed before and after extraction. | The control population had elevated hemodynamic changes, as the diastolic pressure rise was significant. In the test population, there was a statistically significant fall in the hemodynamic changes. | Music seems to be a psychological and spiritual way to calm oneself down. Hence, music therapy can be used as an anxiolytic agent for stressful dental procedures. |
| Oomens et al., 2019 [52] | Systematic review | Systematic literature search—9 studies (212 participants) | Beneficial effects of music were reported on time to task completion, instrument handling, quality of surgical task performance and general surgical performance. | Insufficient evidence to definitively conclude that music has a beneficial effect on surgical performance in the simulated setting |
| Gupta et al., 2020 [8] | Pilot study | 50 adult patients attending the MOS Clinic at Birmingham Dental Hospital. Instrumental music was played for the patient via earphones during MOS treatment. Both physiological and psychological measures of anxiety were recorded using heart rate measurements, patient completed questionnaires and a subjective ten-point anxiety score. | Τhe majority of patients reported music reduced their anxiety levels, pain and discomfort (92%). Almost half of the respondents (48%) reported that music made communication with the dental team easier, and 90% of patients reported that they would request to have music playing during their next dental visit. | Music can be helpful in making patients feel more at ease during dental treatment. |
| Fu VX et al., 2021 [35] | Systematic review | Systematic literature search—22 prospective studies (3507 participants) | Over half of the surveyed staff found noise levels to be a disturbing stressor and impacted performance negatively. | Although music increased decibel levels in the operation room, attitude of surgical team members toward music during surgery is generally regarded favorable. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antoniadou, M.; Tziovara, P.; Antoniadou, C. The Effect of Sound in the Dental Office: Practices and Recommendations for Quality Assurance—A Narrative Review. Dent. J. 2022, 10, 228. https://doi.org/10.3390/dj10120228
Antoniadou M, Tziovara P, Antoniadou C. The Effect of Sound in the Dental Office: Practices and Recommendations for Quality Assurance—A Narrative Review. Dentistry Journal. 2022; 10(12):228. https://doi.org/10.3390/dj10120228
Chicago/Turabian StyleAntoniadou, Maria, Panagiota Tziovara, and Christina Antoniadou. 2022. "The Effect of Sound in the Dental Office: Practices and Recommendations for Quality Assurance—A Narrative Review" Dentistry Journal 10, no. 12: 228. https://doi.org/10.3390/dj10120228
APA StyleAntoniadou, M., Tziovara, P., & Antoniadou, C. (2022). The Effect of Sound in the Dental Office: Practices and Recommendations for Quality Assurance—A Narrative Review. Dentistry Journal, 10(12), 228. https://doi.org/10.3390/dj10120228