
Are Physics Forceps Less Traumatic than Conventional Forceps for Tooth Extraction? A Systematic Review and Meta-Analysis of Randomized Controlled Trials


 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
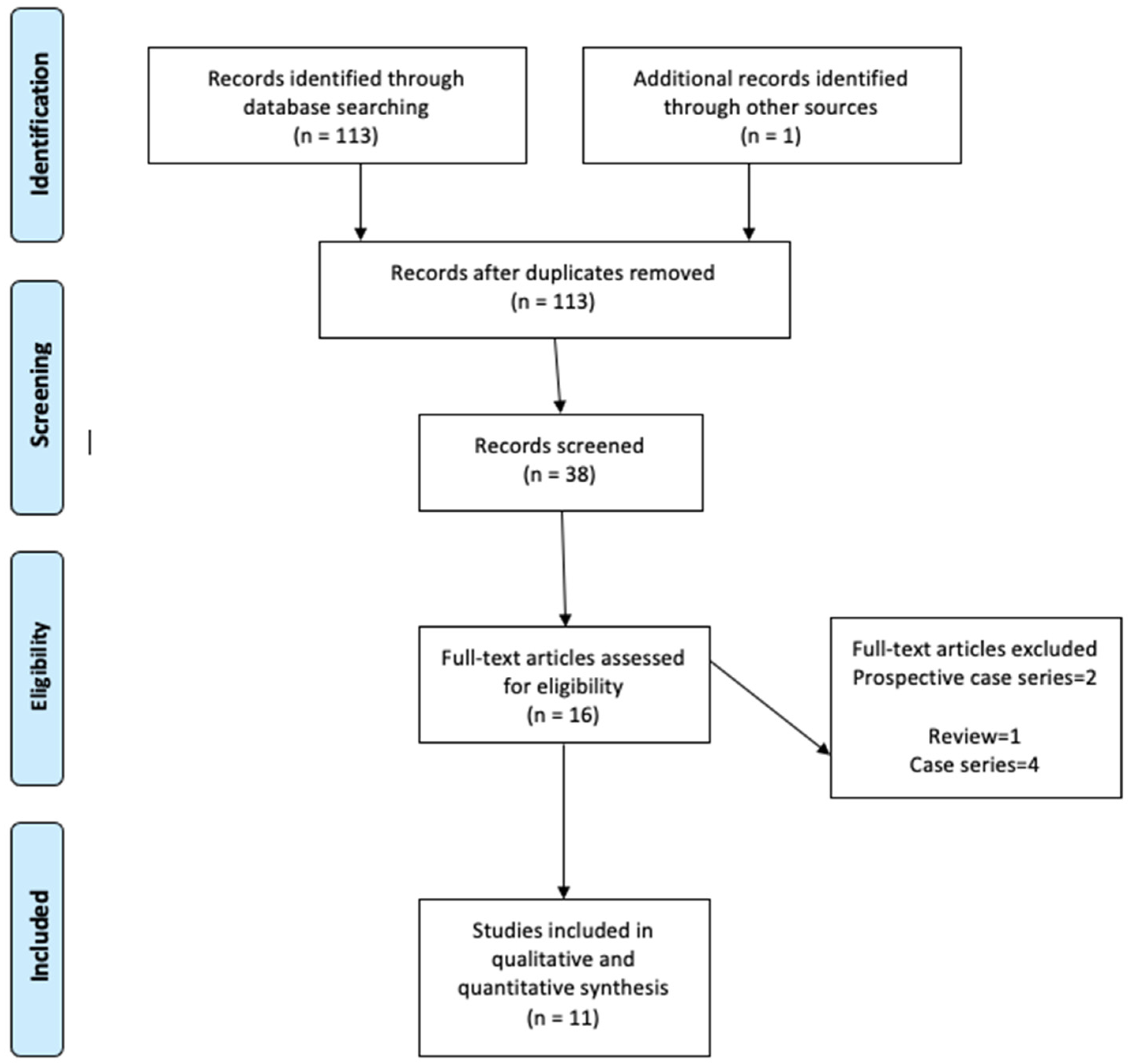
2.1. Literature Search
2.2. Study Selection
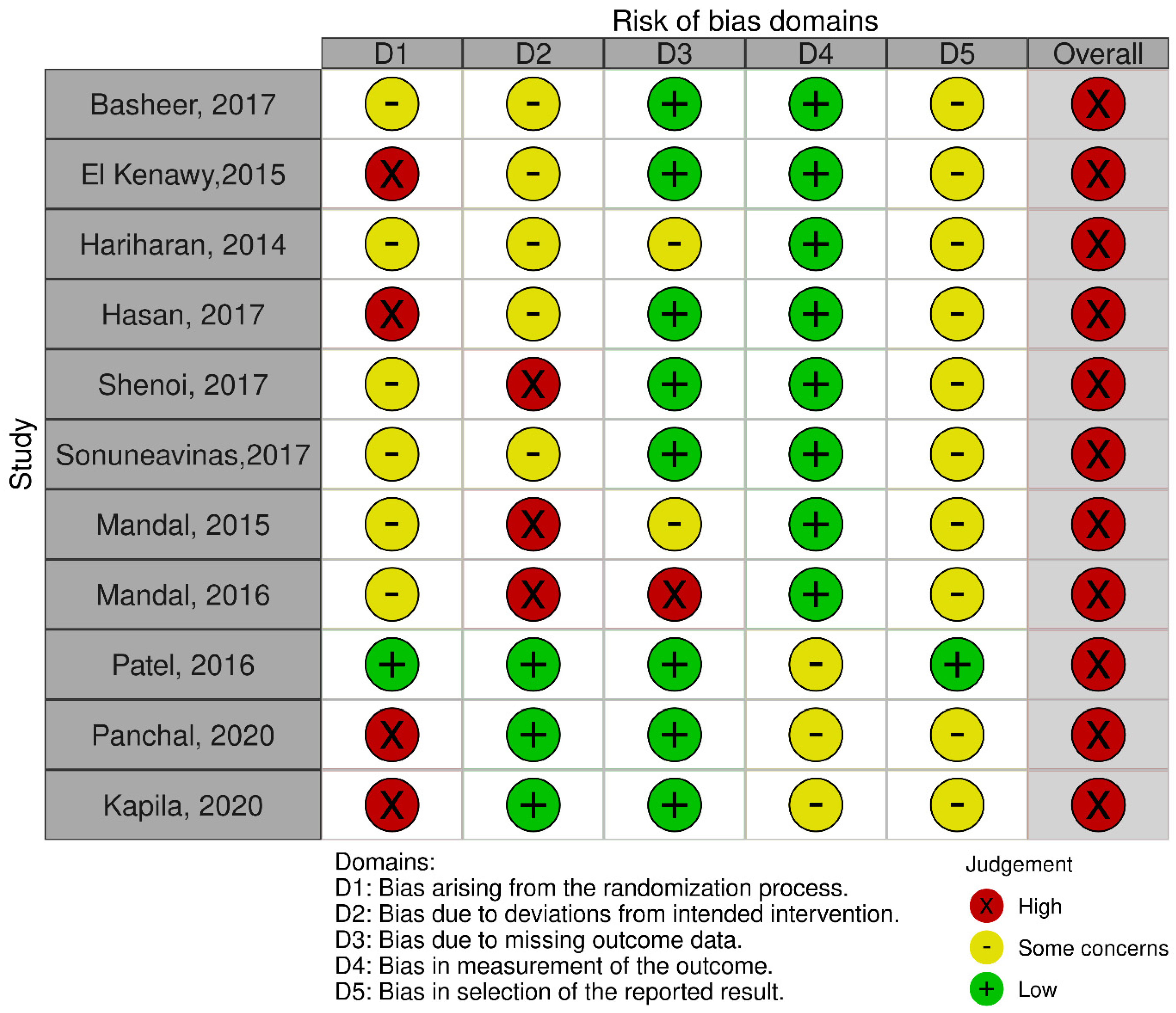
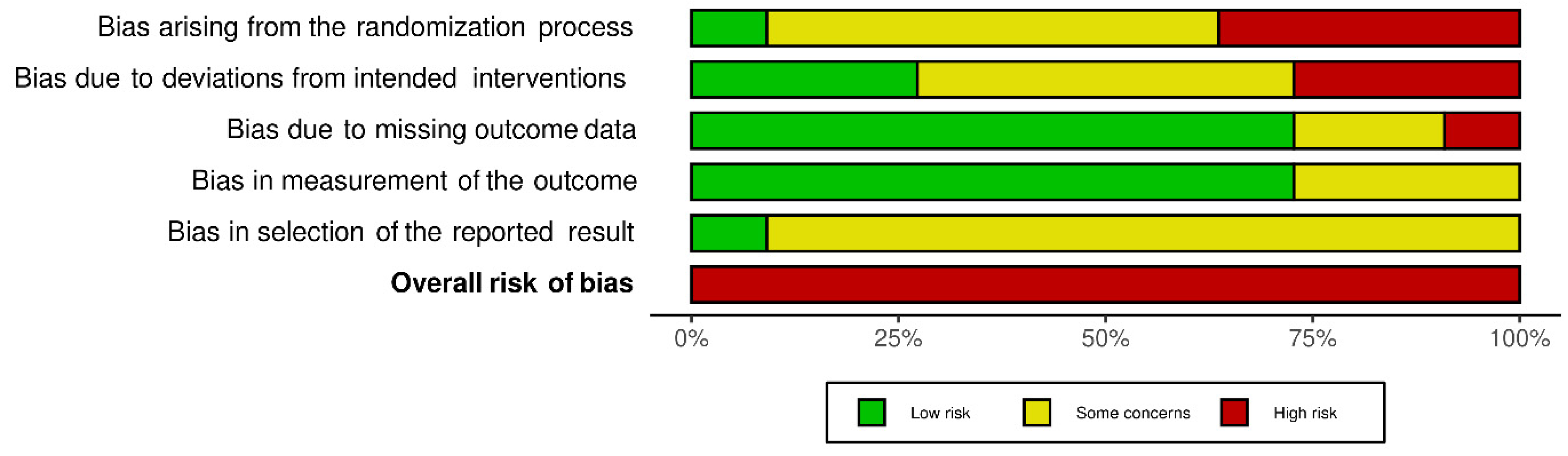
2.3. Quality Assessment
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- McKenzie, W.S. Principles of Exodontia. Oral Maxillofac. Surg. Clin. N. Am. 2020, 32, 511–517. [Google Scholar] [CrossRef] [PubMed]
- Dym, H.; Weiss, A. Exodontia: Tips and techniques for better outcomes. Dent. Clin. N. Am. 2012, 56, 245–266. [Google Scholar] [CrossRef] [PubMed]
- Weiss, A.; Stern, A.; Dym, H. Technological advances in extraction techniques and outpatient oral surgery. Dent. Clin. N. Am. 2011, 55, 501–513. [Google Scholar] [CrossRef] [PubMed]
- De Santis, D.; Sinigaglia, S.; Pancera, P.; Faccioni, P.; Portelli, M.; Luciano, U.; Cosola, S.; Penarrocha, D.; Bertossi, D.; Nocini, R.; et al. An overview of socket preservation. J. Biol. Regul. Homeost. Agents 2019, 33, 55–59. [Google Scholar]
- Quayle, A.A. Atraumatic removal of teeth and root fragments in dental implantology. Int. J. Oral Maxillofac. Implant. 1990, 5, 293–296. [Google Scholar]
- Levitt, D. Atraumatic extraction and root retrieval using the periotome: A precursor to immediate placement of dental implants. Dent. Today 2001, 20, 53–57. [Google Scholar]
- Kubilius, M.; Kubilius, R.; Gleiznys, A. The Preservation of Alveolar Bone Ridge during Tooth Extraction. Stomatologija 2012, 14, 3–11. Available online: http://www.ncbi.nlm.nih.gov/pubmed/22617329 (accessed on 15 October 2021).
- Misch, C.E.; Perez, H.M. Atraumatic Extractions: A Biomechanical Rationale. Dent. Today 2008, 27, 98, 100–101. Available online: http://www.ncbi.nlm.nih.gov/pubmed/18717405 (accessed on 15 October 2021).
- Thomson, P.J. Minimising trauma in dental extractions: The use of the periotome. Br. Dent. J. 1992, 172, 179. [Google Scholar] [CrossRef]
- Sharma, S.D.; Vidya, B.; Alexander, M.; Deshmukh, S. Periotome as an Aid to Atraumatic Extraction: A Comparative Double Blind Randomized Controlled Trial. J. Maxillofac. Oral Surg. 2015, 14, 611–615. [Google Scholar] [CrossRef] [Green Version]
- Krug, R.; Connert, T.; Soliman, S.; Syfrig, B.; Dietrich, T.; Krastl, G. Surgical extrusion with an atraumatic extraction system: A clinical study. J. Prosthet. Dent. 2018, 120, 879–885. [Google Scholar] [CrossRef] [PubMed]
- Al-Harbi, S.H. Minimizing trauma during tooth removal: A systematic sectioning approach. Eur. J. Esthet. Dent. Off. J. Eur. Acad. Esthet. Dent. 2010, 5, 274–287. [Google Scholar]
- Saund, D.; Dietrich, T. Minimally-invasive tooth extraction: Doorknobs and strings revisited! Dent. Update 2013, 40, 325–326, 328–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raghu, K.; Selvakumar, S.R.; Muthukumar, R.; Thangavelu, A.; Sathyanarayanan, R.; Mani, M.; Balasubramaniam, M. Beak and bumper—Physics forceps: Evaluation of new technique in extraction. Indian J. Dent. Res. Off. Publ. Indian Soc. Dent. Res. 2020, 31, 4–13. [Google Scholar] [CrossRef] [PubMed]
- El-Kenawy, M.H.; Ahmed, W.M.S. Comparison Between Physics and Conventional Forceps in Simple Dental Extraction. J. Maxillofac. Oral Surg. 2015, 14, 949–955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panchal, K.V.; Shah, N.S.; Panchal, B. Comparative evaluation of efficacy of physics forceps versus conventional forceps in therapeutic extractions of premolars: A prospective clinical study. Int. J. Res. Med. Sci. 2020, 8. [Google Scholar] [CrossRef]
- Kapila, S.; Kaur, T.; Bhullar, R.S.; Sandhu, A.; Dhawan, A.; Kaur, A. Use of Physics Forceps in Atraumatic Orthodontic Extractions of Bilateral Premolars: A Randomized Control Clinical Study. J. Maxillofac. Oral Surg. 2020, 19, 347–354. [Google Scholar] [CrossRef]
- Shenoi, R.; Vadera, S.K.; Moriwal, N. Comparative evaluation of efficacy of physics forceps and conventional extraction forceps in extraction of upper molars—A randomised controlled trial. Int. J. Curr. Adv. Res. 2017, 6, 5467–5471. [Google Scholar]
- Patel, H.S.; Managutti, A.M.; Menat, S.; Agarwal, A.; Shah, D.; Patel, J. Comparative evaluation of efficacy of physics forceps versus conventional forceps in orthodontic extractions: A prospective randomized split mouth study. J. Clin. Diagn. Res. 2016, 10, ZC41. [Google Scholar] [CrossRef]
- Hariharan, S.; Narayanan, V.; Soh, C.L. Split-mouth comparison of Physics forceps and extraction forceps in orthodontic extraction of upper premolars. Br. J. Oral Maxillofac. Surg. 2014, 52, e137–e140. [Google Scholar] [CrossRef]
- Mandal, D.; Gupta, S.K.; Mittal, A.; Garg, R. Collate on the Ability of Physics Forceps V/S Conventional Forceps in Multirooted Mandibular Tooth Extractions. IOSR J. Dent. Med Sci. 2015, 14, 63–66. [Google Scholar]
- Mandal, S.; Mandal, S.B.; Kamal, V.; Kumar, A.; Gorka, K.; Kumar, A. Physics Forceps: A New Sensation in Exodontia? Int. J. Oral Care Res. 2016, 4. [Google Scholar] [CrossRef]
- Hasan, A.M. The Efficiency Of Physics Forceps In Comparison To The Conventional Dental Extraction Forceps: A randomized Clinical Trial. J. Baghdad Coll. Dent. 2019, 31. [Google Scholar] [CrossRef]
- Basheer, S.A. Comparative Evaluation between Physics Forceps and Conventional Extraction Forceps in Extraction of Maxillary Molars. Int. J. Appl. Dent. Sci. 2017, 34, 152. [Google Scholar]
- SonuneAvinash, M.; Borle, R.M.; Jadhav, A.A. Comparative Evaluation between Physics Forceps and Conventional Extraction Forceps in Orthodontic Extraction of Maxillary Premolars: A Prospective, Interventional, Single Blind, Randomized Split Mouth Study. Int. J. Pharm. Sci. Invent. 2017, 6, 4–8. [Google Scholar]
- Abdelwahab, M.; Nørholt, S.E.; Taneja, P. The Efficacy of Physics Forceps for Exodontia: A Systematic Review. J. Oral Maxillofac. Surg. Off. J. Am. Assoc. Oral Maxillofac. Surg. 2021, 79, 989.e1–989.e13. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Cochrane Handbook for Systematic Reviews of Interventions; Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Version 6.2; John Wiley & Sons: Chichester, UK, 2019; Available online: www.training.cochrane.org/handbook (accessed on 15 October 2021).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| (P) Patients or population | Extraction of any permanent tooth in healthy patients. | Extraction of deciduous teeth, teeth associated with pathology |
| (I) Intervention | Physics forceps | |
| (C) Comparator or control group | Conventional forceps | |
| (O) Outcomes | Primary outcome: BCPF, GL, tooth or root fracture. Secondary outcomes: operative time, pain after extraction | |
| (S) Study design | Studies in humans RCTs. | Uncontrolled clinical trials, prospective and retrospective comparative studies, reviews, case series, and reports. |
| Author, Country, Year | Study Design | Sample Size, PF CF | Age, Sex | Teeth Extracted | Outcome | Results |
|---|---|---|---|---|---|---|
| Basheer, India, 2017 [24] | Parallel group RCT | Patients: 100 Teeth: 100 PF: 50 CF: 50 | NG | Maxillary molars | BCPF GL Tooth/root fracture, socket healing, bleeding from socket, post-operative pain (1–5 days). | BCPF: NSD (p = 0.715). GL: NSD (p = 0.487). Tooth fracture: NSD (p = 0.678). Healing: SSD (p = 0.002). Bleeding: SSD (p = 0.001). Pain: SSD on Days 1 (p < 0.001) and 2 (p < 0.001), and NSD on Days 3 (p = 0.374), 4 (p = 0.543), and 5 (p = 1.00). |
| El-Kenawy and Ahmed, India, 2015 [15] | Parallel group RCT | Patients: 200 Teeth: 200 PF: 100 CF: 100 | Age: Mean: PF: 42.6 ± 15.9 (SD) CF: 41.6 ± 15.1 (SD) Gender: Male: 136 Female: 64 | Any tooth | BCPF Crown fracture, root fracture. | BCPF: NSD (p = 0.19). Crown fracture: SSD (p = 0.04). Root fracture: SSD (p = 0.027). |
| Hariharan et al., India, 2014 [20] | Split-mouth RCT | Patients: 27 Teeth: 54 PF: 27 CF: 27 | Age: Mean: 16 Range: 11–23 Gender: Male: 12 Female:15 | Maxillary premolars | BCPF Tooth/root fracture, dry socket delayed healing, acute infection, post-operative pain after 1, 3, and 7 days. | BCPF: NSD (p = NG) Tooth/Root fracture: NSD (p = NG) Delayed healing, dry socket, and acute infection: NSD (p = NG) Pain: SSD on Day 1 (p = 0.03), no pain on Days 3 and 7. Extraction Time: NSD (p = 0.204) |
| Hasan, Iraq, 2017 [23] | Parallel group RCT | Patients: 14 Teeth: 28 PF: 14 CF: 14 | Age: Mean: 40.7 Range 16–65 Gender: Male: 8 Female: 6 | Mandibular incisors, canines, and premolars | BCPF GL Tooth/root fracture, extraction time. | BCPF: NSD (p = 0.098) GL: SSD (p = 0.006). Crown fracture: NSD (p = 0.222). Root fracture: NSD (p = 1.00). Time: SSD (p = 0.01). |
| Shenoi et al., India, 2017 [18] | Parallel group RCT | Patients: 64 Teeth: 64 PF: 31 (1 excluded) CF: 32 | Age Mean: 44.11 Range: 21–70 Gender: Male: 30 Female: 30 | Maxillary molars | BCPF Root fracture, delayed healing, dry-socket infection pain after 1, 3, and 7 days, extraction time. | BCPF: NSD (p = 0.612). Root fracture: NSD (p = 0.129). Delayed healing, dry socket, and infection: NSD (p = not calculated, p = 1.000, and p = 0.150, respectively). Pain: SSD on post-operative Days 1 and 3. (p = 0.0007 and p = 0.0008, respectively) and no pain on Day 7. Time: SSD (p < 0.001). |
| Sonun Avinash et al., India, 2017 [25] | Split-mouth RCT | Patients: 50 Teeth: 100 PF: 50 CF: 50 | Range: 14–25 NG | Maxillary premolars | BCPF GL Tooth/ root fracture, bleeding, soft-tissue healing after 7, 14, and 21 days, pain after 1–7 days, ease of technique, extraction time. | BCPF: NSD (p = 0.55) GL: NSD (p = 0.30) Tooth or root fracture: NSD (p = 0.15). Bleeding: SSD (p < 0.001). Post-operative healing after 7 days: NSD (p = 0.21). Pain: NSD on Days 1 to 4 (p = 0.07–0.97) and no pain on Days 5–7. Techical ease and learning curve: NSD (p = 0.26) Time: SSD (p = not calculated) |
| Mandal et al., India, 2015 [21] | Parallel group RCT | Patients: 50 Teeth: 50 PF: 25 CF: 25 | >14 NG | Mandibular molars | BCPF, GL, Pain after 3 and 7 days, and extraction time. | BCPF: SSD (p = 0.001). GL: SSD (p = 0.032). Pain: SSD on day 3 (p = 0.035) Extraction Time: SSD (p = not calculated) |
| Mandal et al., India, 2016 [22] | Parallel group RCT | Patients: 50 Teeth: 50 PF: 25 CF: 25 | >14 NG | Mandibular incisors, canines and premolars | BCPF, GL, tooth fracture extraction time. | BCPF: NG GL: SSD (p = 0.032). Tooth fracture: NG. Time: SSD (p = not calculated) |
| Patel et al., India, 2016 [19] | Split- mouth RCT | Patients: 11 Teeth: 42 PF:21 CF:21 | Age: Mean: 19.4 Range: 14–23 years Gender: Male: 7 Female:4 | Maxillary and mandibular premolar teeth | BCPF, GL, ease of technique, pain, extraction time, other complications. | BCPF: PF 4.76%, CF: none Root fracture: PF: 4.76%, CF: none GL: SSD (p = 0.035). Marginal bone loss: SSD (p = 0.037). Time: SSD (p = 0.019) Techncal ease and learning curve: NSD (p = NG) Pain: NSD (p = NG) |
| Kapila et al., India, 2020 [17] | Split mouth RCT | Patients: 50 Teeth: 200 PF: 100 CF: 100 | Age Mean: 17.6 Range: 14–25 Gender Male: 14 Female:36 | Maxillary and mandibular premolars | Time, BCPF, GL, volume of analgesics, healing post-operative pain on the day, and 1, 3, and 7 days after extraction, complications. | Time: SSD (p = 0.001) Pain: NSD Day of extraction (p = 0.927), 1 day after extraction (p = 0.513), 3 days after (p = 0.349), 7 days after (p = 0.445) Volume of analgesics: not significant (p = 0.522) BCPF: no significant difference (p = NG) GL: NSD (p = NG) Tooth, root, or alveolus fracture: No event in any group |
| Panchal et al., India, 2020 [16] | Split mouth RCT | Patients: 35 Teeth: 140 PF: 70 CF: 70 | Range: 18–40 Gender: NG | Maxillary and Mandibular Premolars | Time, BL, GL, success score and pain. | Time: SSD (p = 0.001) GL: SSD (p = 0.001). Bone loss: SSD (p = 0.001). Success score: Mean score: PF: 5 (95.92%) CF: 3.9 (91.84%) |
| Physics Forceps Compared to Conventional Forceps for Closed Tooth Extraction | |||||
|---|---|---|---|---|---|
| Patient or population: closed tooth extraction Setting: Intervention: physics forceps Comparison: conventional forceps | |||||
| Outcomes | N° of participants (studies) Follow up | Certainty of the evidence (GRADE) | Relative effect (95% CI) | Anticipated absolute effects | |
| Risk with Conventional forceps | Risk difference with Physics forceps | ||||
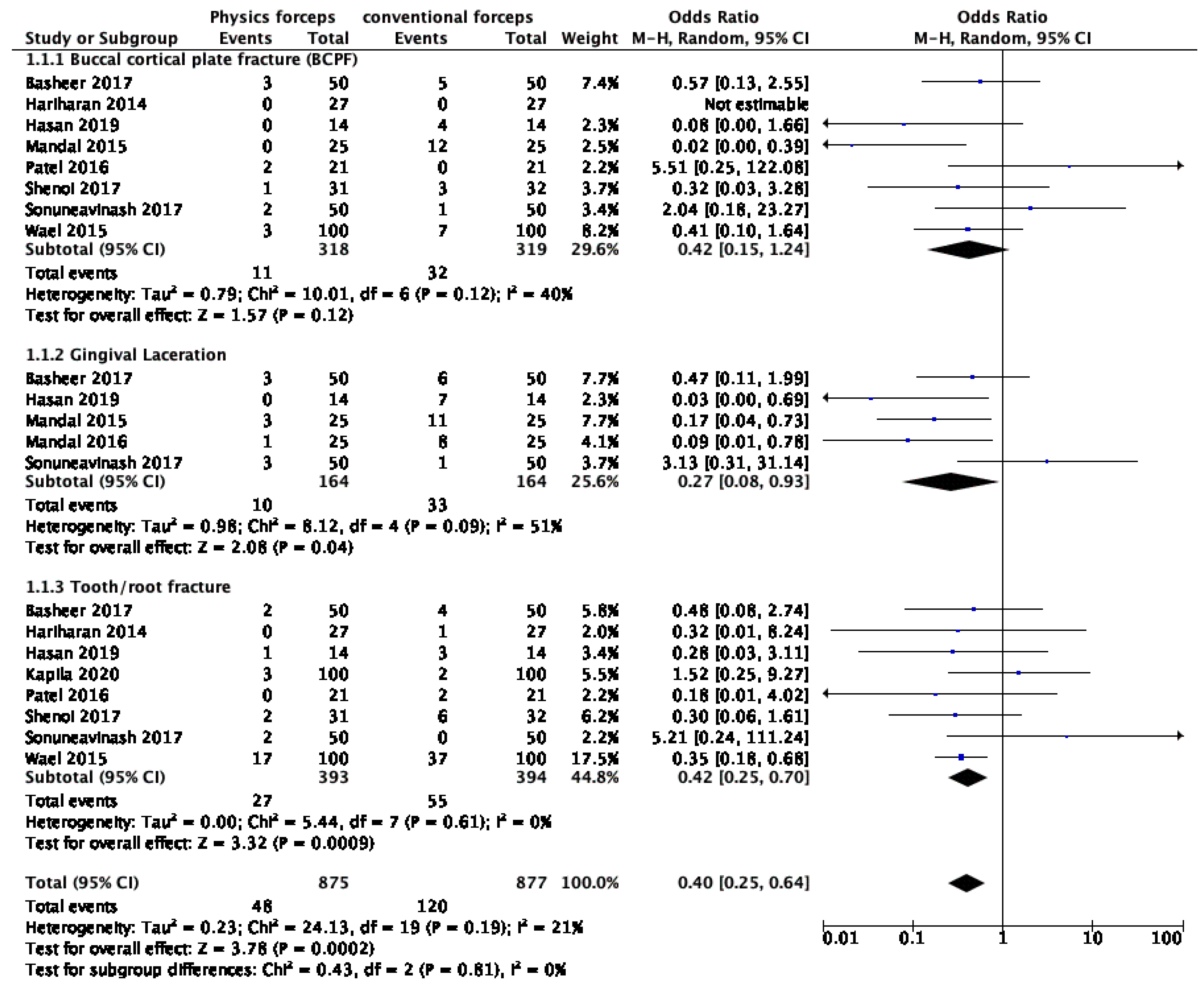
| Adverse events | 1752 (10 RCTs) | ⨁⨁◯◯ LOW | OR 0.40 (0.25 to 0.64) | 137 per 1000 | 77 fewer per 1000 (99 fewer to 45 fewer) |
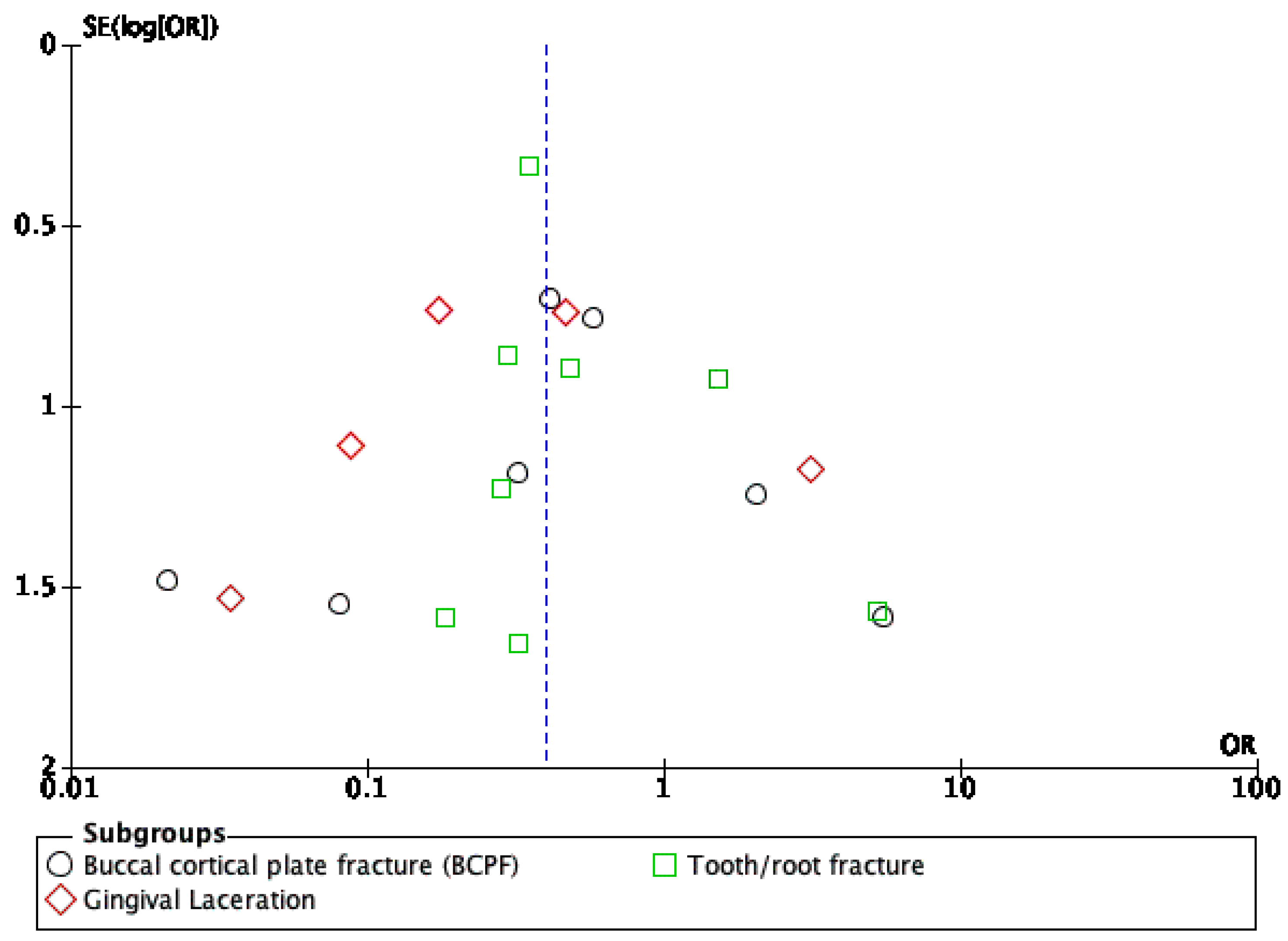
| Adverse events—buccal cortical plate fracture (BCPF) | 637 (8 RCTs) | ⨁⨁◯◯ LOW | OR 0.42 (0.15 to 1.24) | 100 per 1000 | 56 fewer per 1000 (84 fewer to 21 more) |
| Adverse events—gingival Laceration | 328 (5 RCTs) | ⨁◯◯◯ VERY LOW | OR 0.27 (0.08 to 0.93) | 201 per 1000 | 138 fewer per 1000 (181 fewer to 11 fewer) |
| Adverse events—tooth/root fracture | 787 (8 RCTs) | ⨁◯◯◯ VERY LOW | OR 0.42 (0.25 to 0.70) | 140 per 1000 | 76 fewer per 1000 (101 fewer to 38 fewer) |
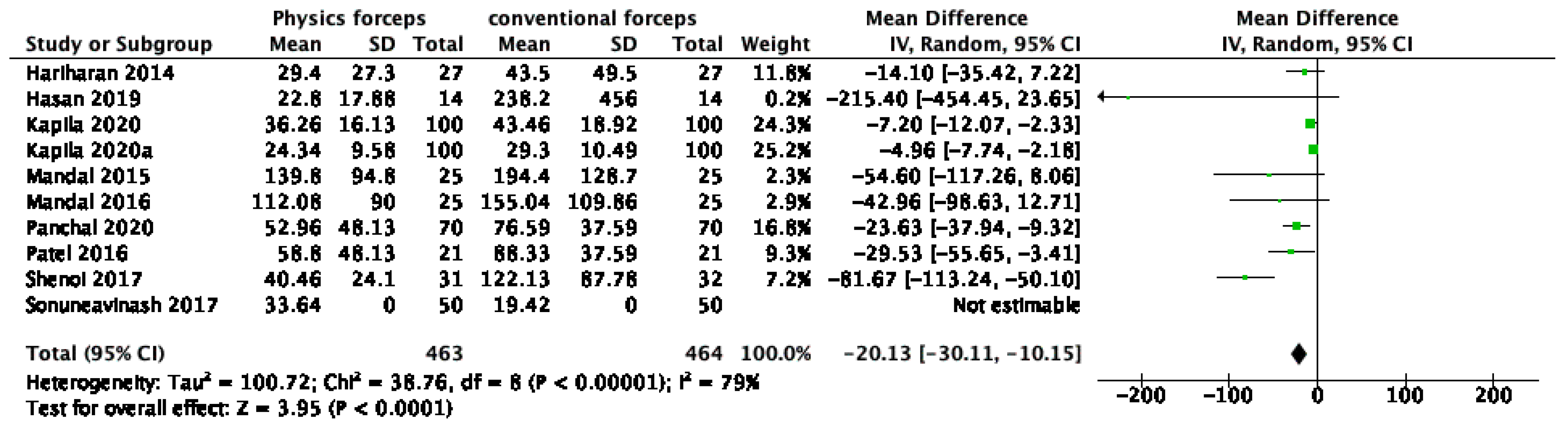
| Operative time | 927 (10 RCTs) | ⨁⨁⨁◯ MODERATE | - | MD 20.13 lower (30.11 lower to 10.15 lower) | |
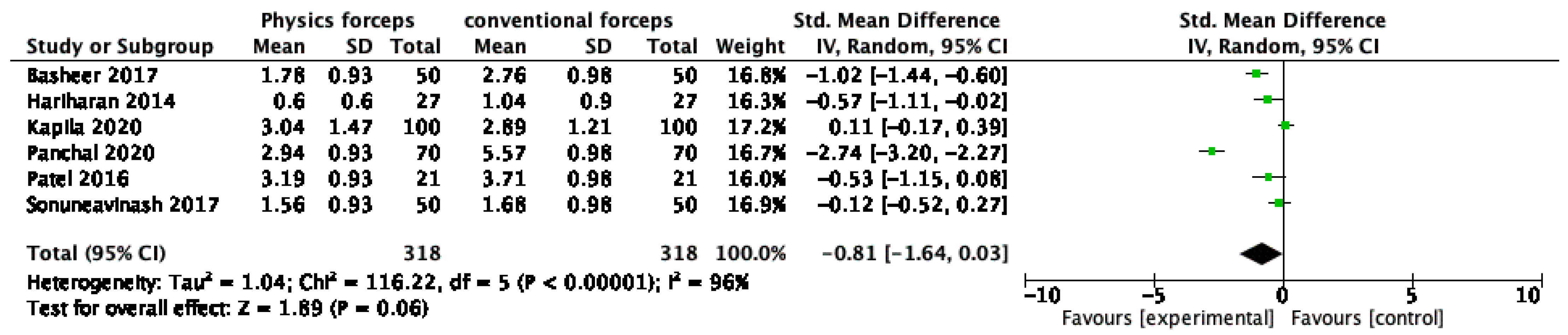
| Pain on first post-operative day | 636 (6 RCTs) | ⨁◯◯◯ VERY LOW | - | - | SMD 0.81 lower (1.64 lower to 0.03 higher) |
| * Risk in intervention group (and its 95% confidence interval) based on assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; OR: odds ratio; MD: mean difference; SMD: standardised mean difference. | |||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited, and the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate, and the true effect is likely to be substantially different from the estimate of effect. | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Singh, A.K.; Khanal, N.; Acharya, N.; Rokaya, D.; Hasan, M.R.; Saito, T. Are Physics Forceps Less Traumatic than Conventional Forceps for Tooth Extraction? A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Dent. J. 2022, 10, 21. https://doi.org/10.3390/dj10020021
Singh AK, Khanal N, Acharya N, Rokaya D, Hasan MR, Saito T. Are Physics Forceps Less Traumatic than Conventional Forceps for Tooth Extraction? A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Dentistry Journal. 2022; 10(2):21. https://doi.org/10.3390/dj10020021
Chicago/Turabian StyleSingh, Ashutosh Kumar, Nikita Khanal, Nisha Acharya, Dinesh Rokaya, Md Riasat Hasan, and Takashi Saito. 2022. "Are Physics Forceps Less Traumatic than Conventional Forceps for Tooth Extraction? A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Dentistry Journal 10, no. 2: 21. https://doi.org/10.3390/dj10020021
APA StyleSingh, A. K., Khanal, N., Acharya, N., Rokaya, D., Hasan, M. R., & Saito, T. (2022). Are Physics Forceps Less Traumatic than Conventional Forceps for Tooth Extraction? A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Dentistry Journal, 10(2), 21. https://doi.org/10.3390/dj10020021