
Digital Dental Models: Is Photogrammetry an Alternative to Dental Extraoral and Intraoral Scanners?

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
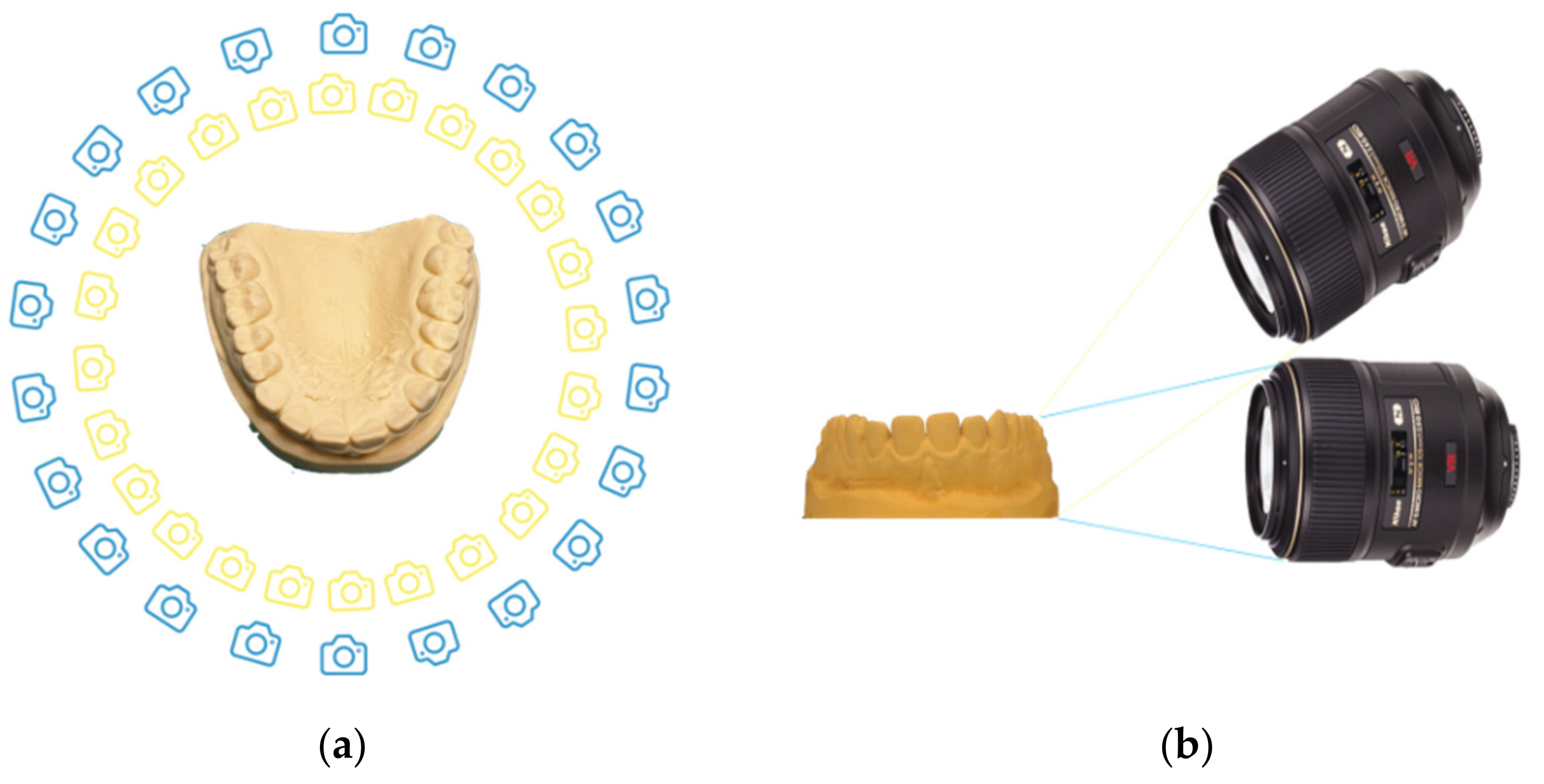
2.1. Photogrammetry Method
- 25 photos parallel to the occlusal plane, and
- 25 photos with an angle of 30° from the occlusal plane.
- A new project for each set was opened, and all the photos of each set were uploaded;
- Photos were masked, using the internal software plugin “Masquerade”, to remove the background;
- A sparse point cloud was generated by the pairing of the photos. The “category” was set to “Close Range” and the pre-set was set to “Deep” (Figure 2);
- A dense point cloud was generated, setting the category to “Close Range” and the pre-set to “High Details” (Figure 3);
- A mesh was extracted from the dense point cloud by setting the category to “Close Range” and the pre-set to “High Details”;
- A textured mesh was generated by setting the category to “General” and the pre-set to “Default Single Texture”,
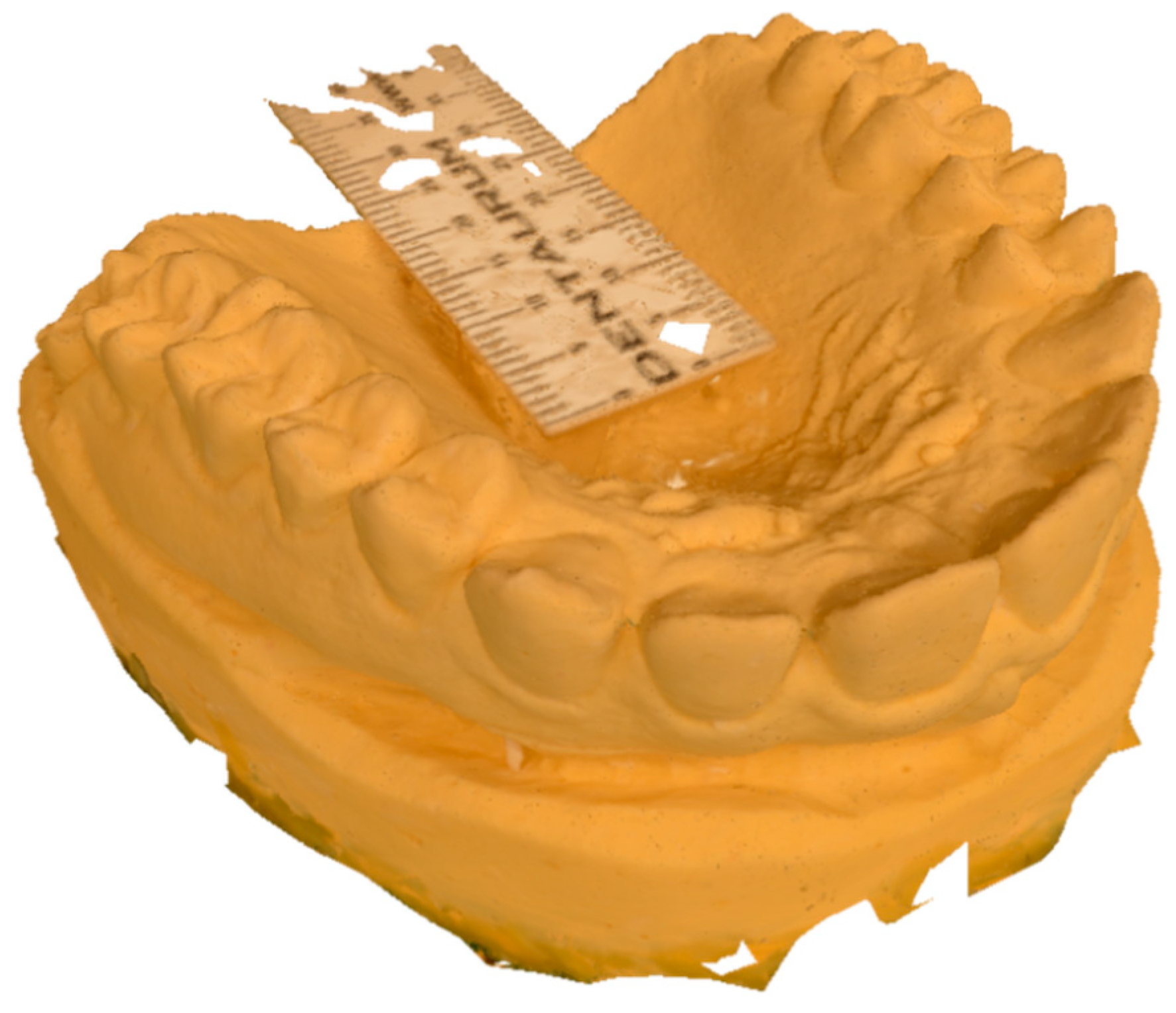
- The mesh was scaled using the double decimeter as a measure of reference;
- The mesh with texture was extracted from the software with the OBJ/MTL extension (Figure 4).
2.2. Dental Extraoral Laboratory Scanner Method
2.3. Intraoral Scanner Method
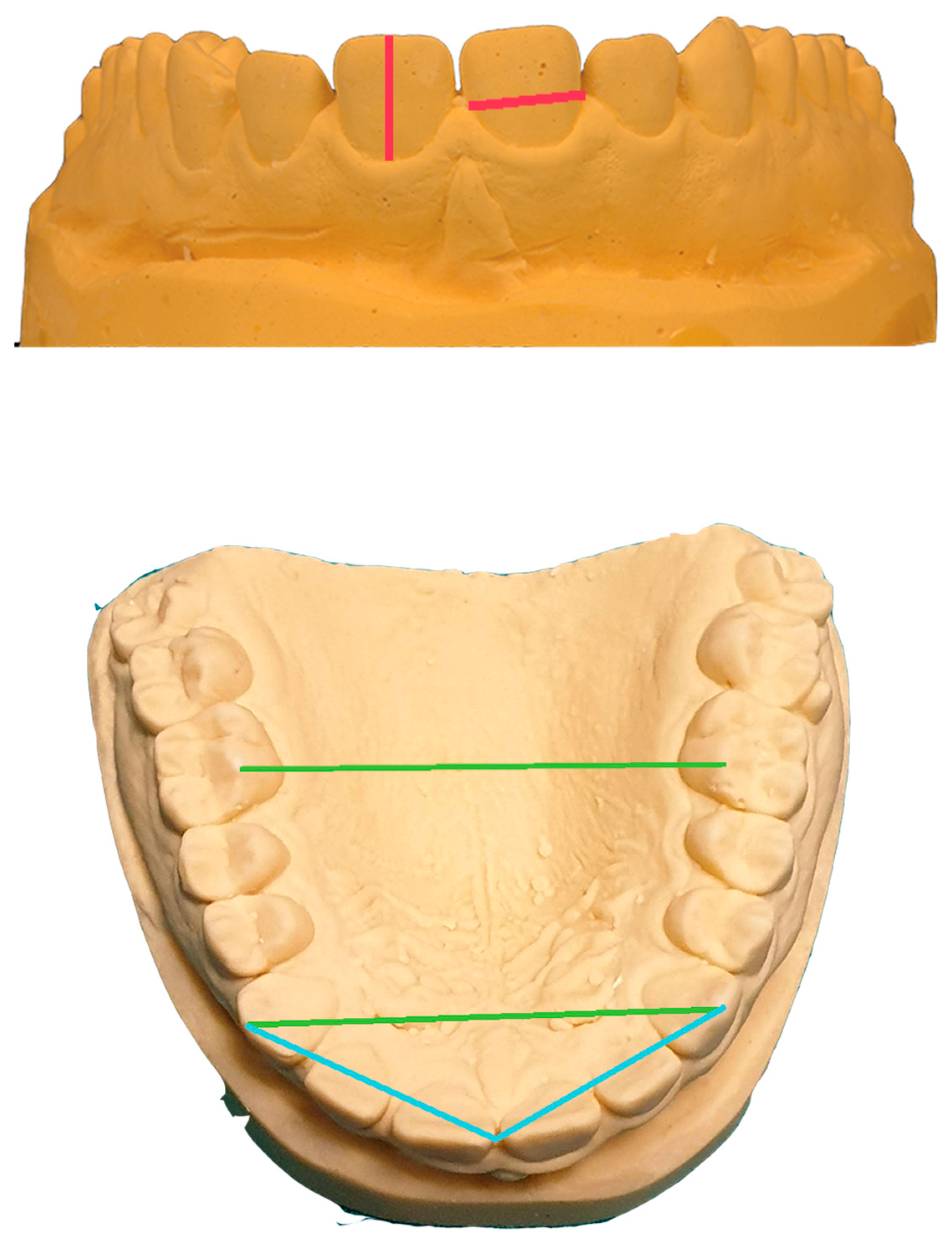
2.4. Measurements
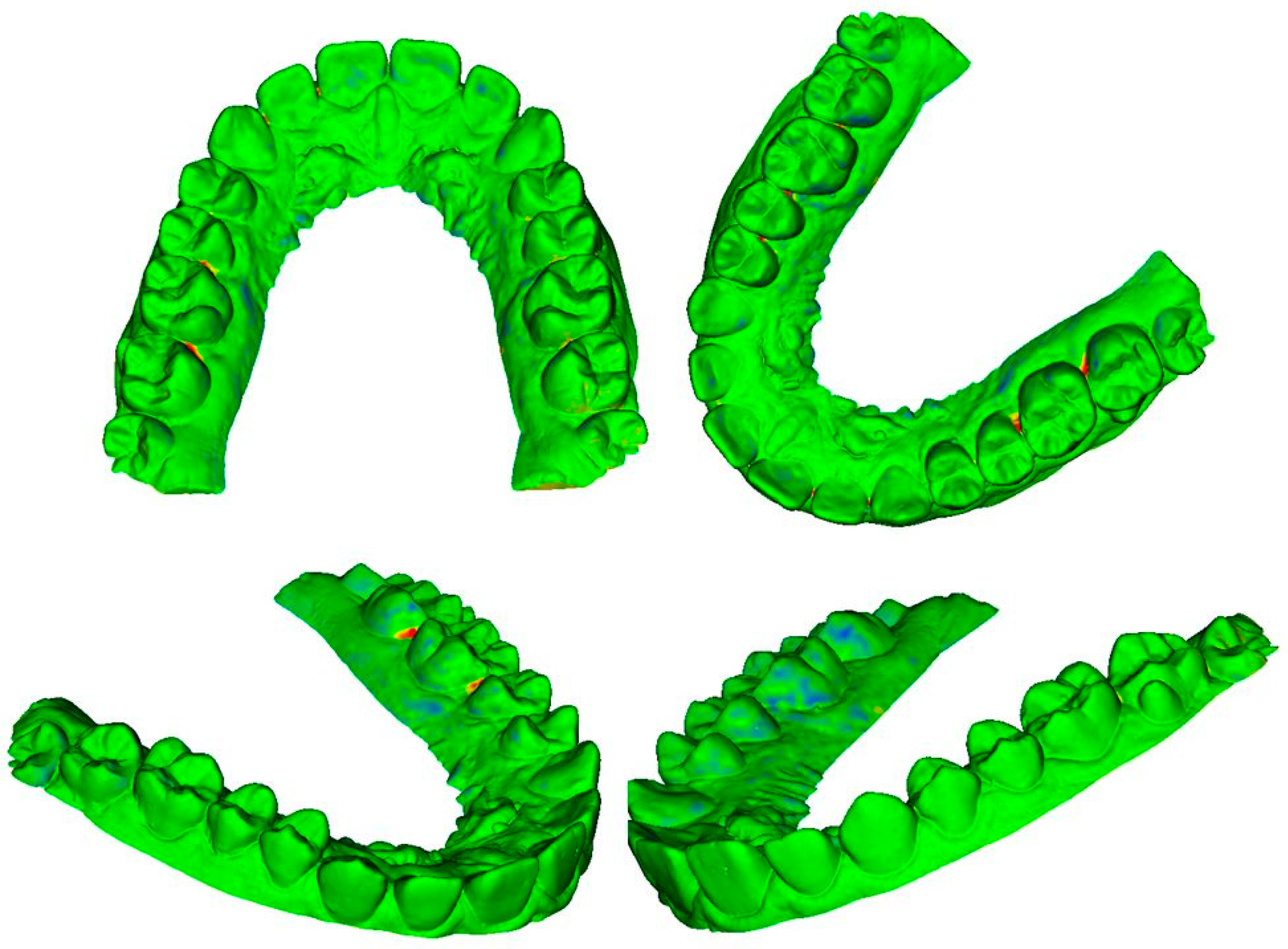
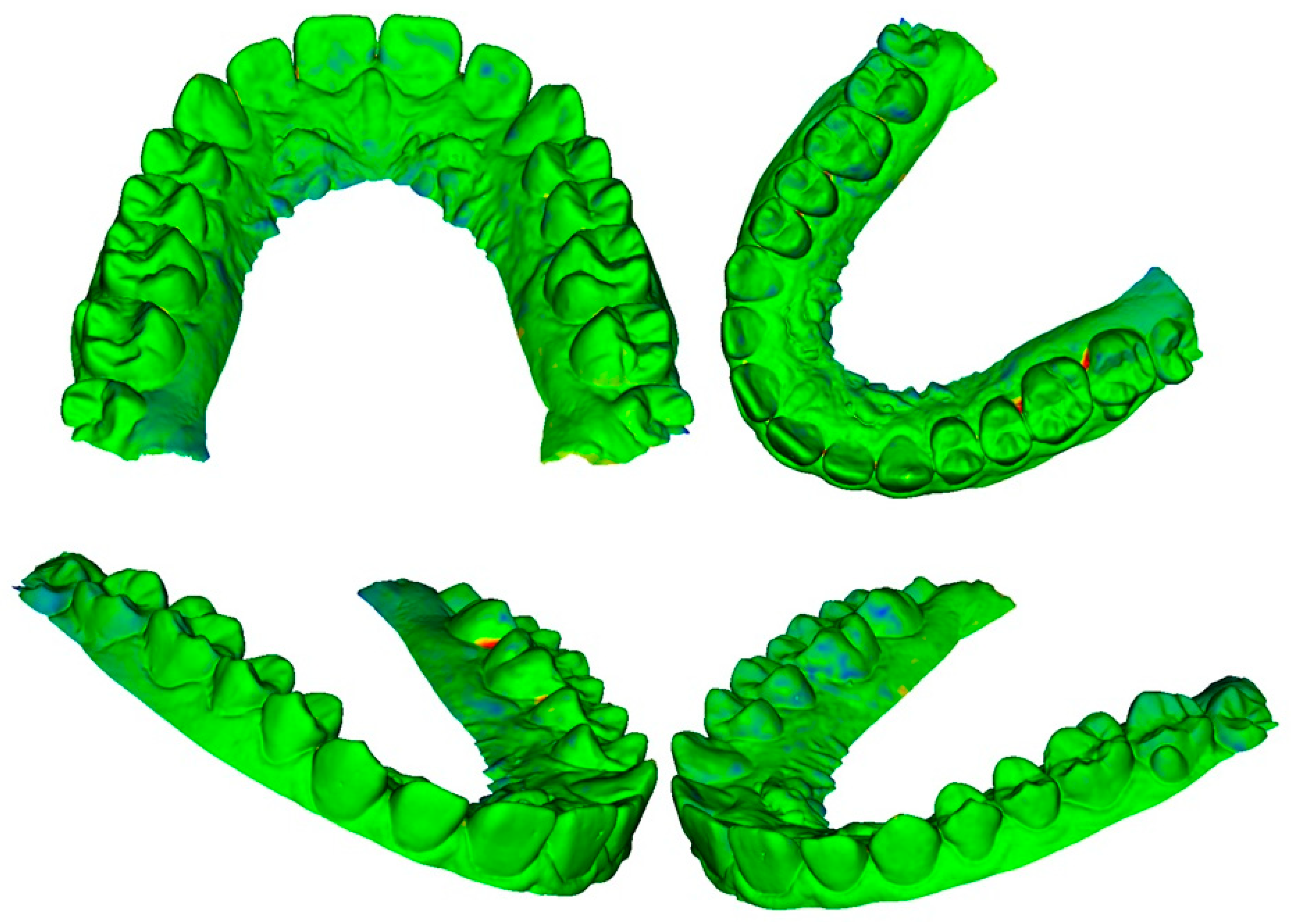
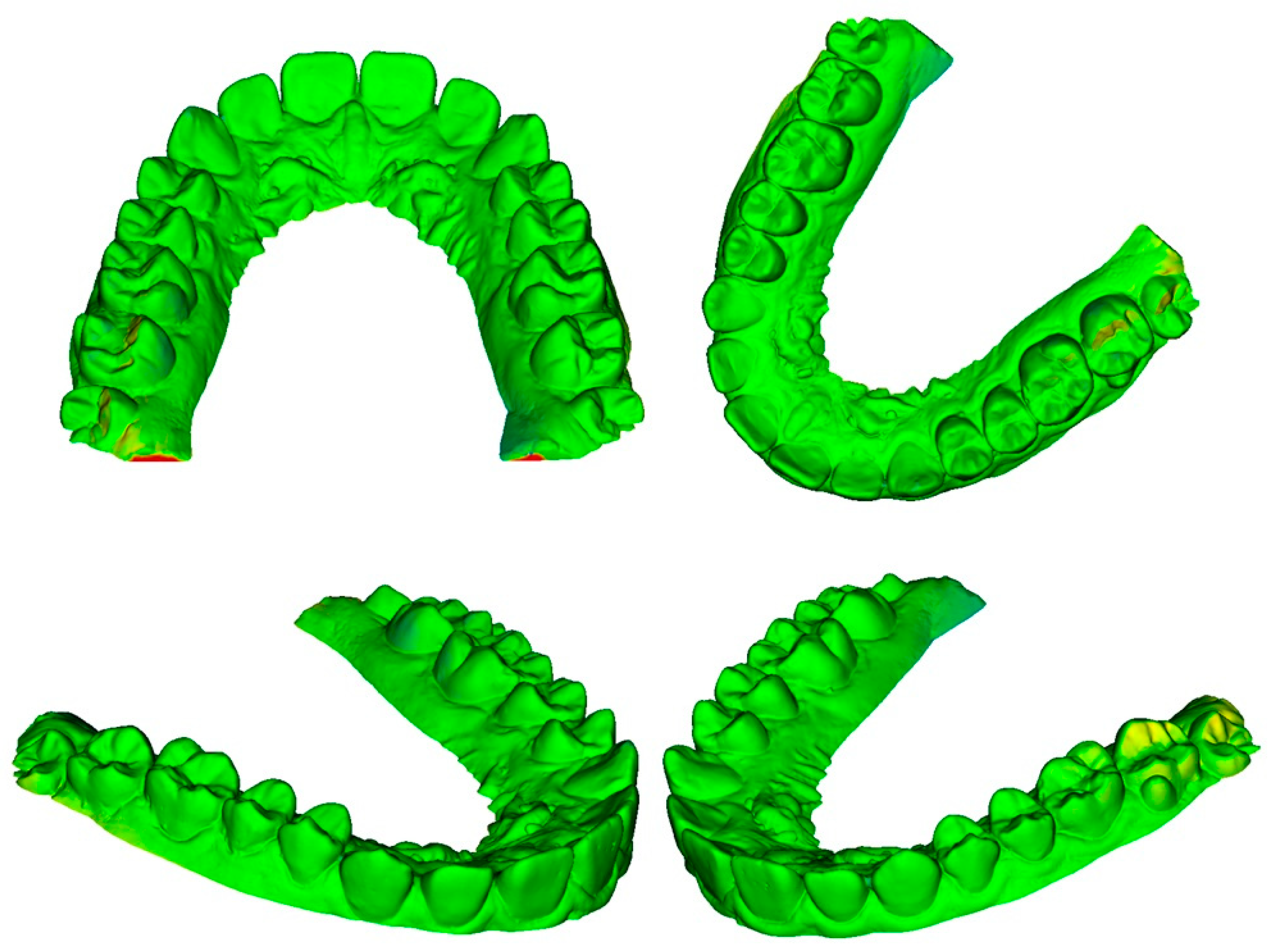
2.5. Superimposition
- A new project was created and two STL files were uploaded;
- Meshes were cut using the Easy Clip module to keep only the teeth from the second molar to the second molar;
- Meshes were approached using the “surface registration” module and setting the type of registration to “fiducial registration”;
- Meshes were superimposed using the “Surface Registration” module and setting the type of registration to “Surface Registration”;
- Mean distances and standard deviation from all the points of the meshes were measured using the “Model to Model distance” module and a VTK file with all the distances was created;
- The “Mesh Statistic” module was used to read the mean distance and the standard deviation from the saved VTK file;
- The VTK file was uploaded to the “Shape Population Viewer” module to create a color map and to view discrepancies ranging from −0.5 mm to 0.5 mm.
2.6. Precision of Photogrammetry
2.7. Trueness of Photogrammetry
3. Results
3.1. Precision of Photogrammetry
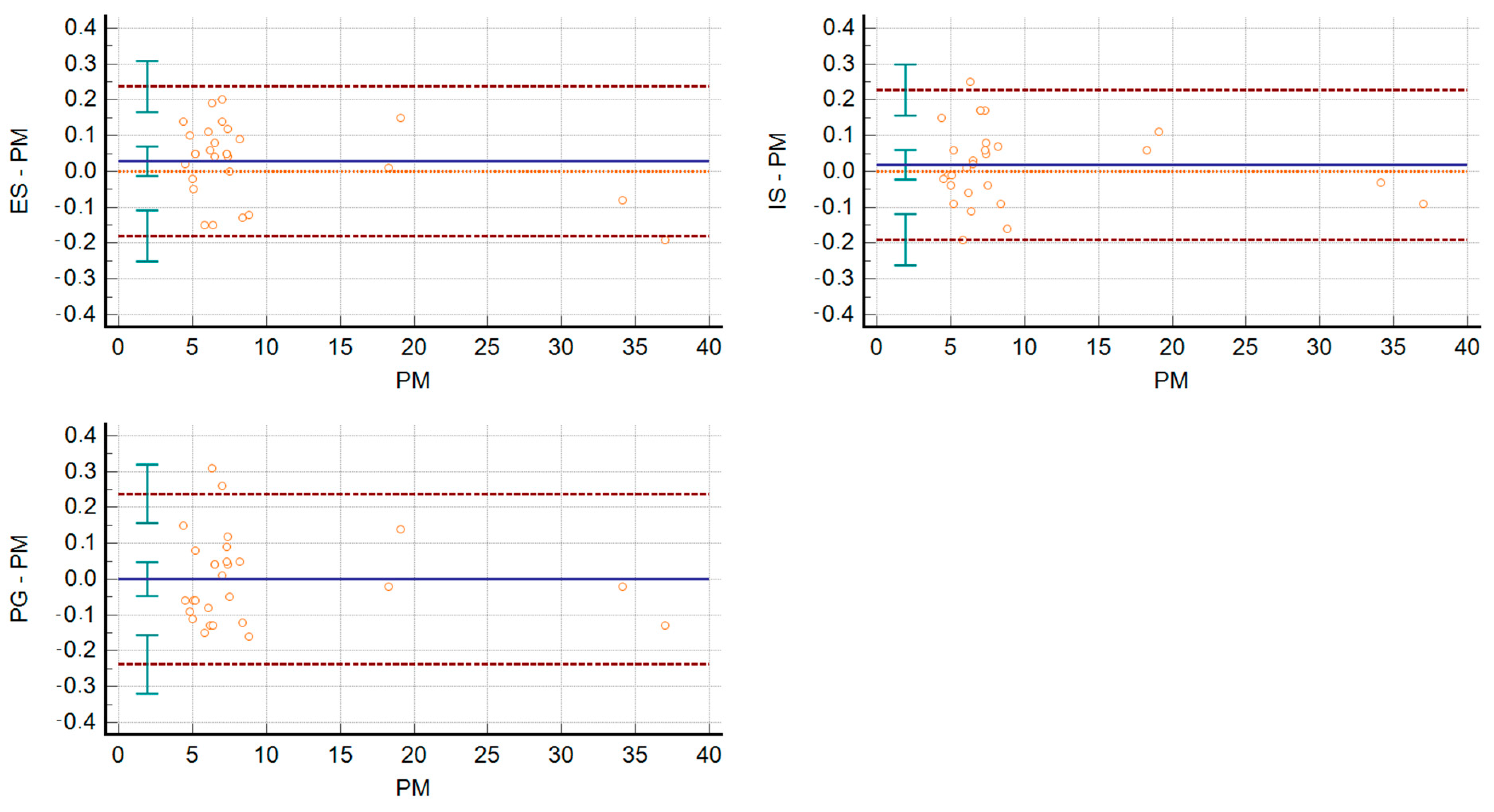
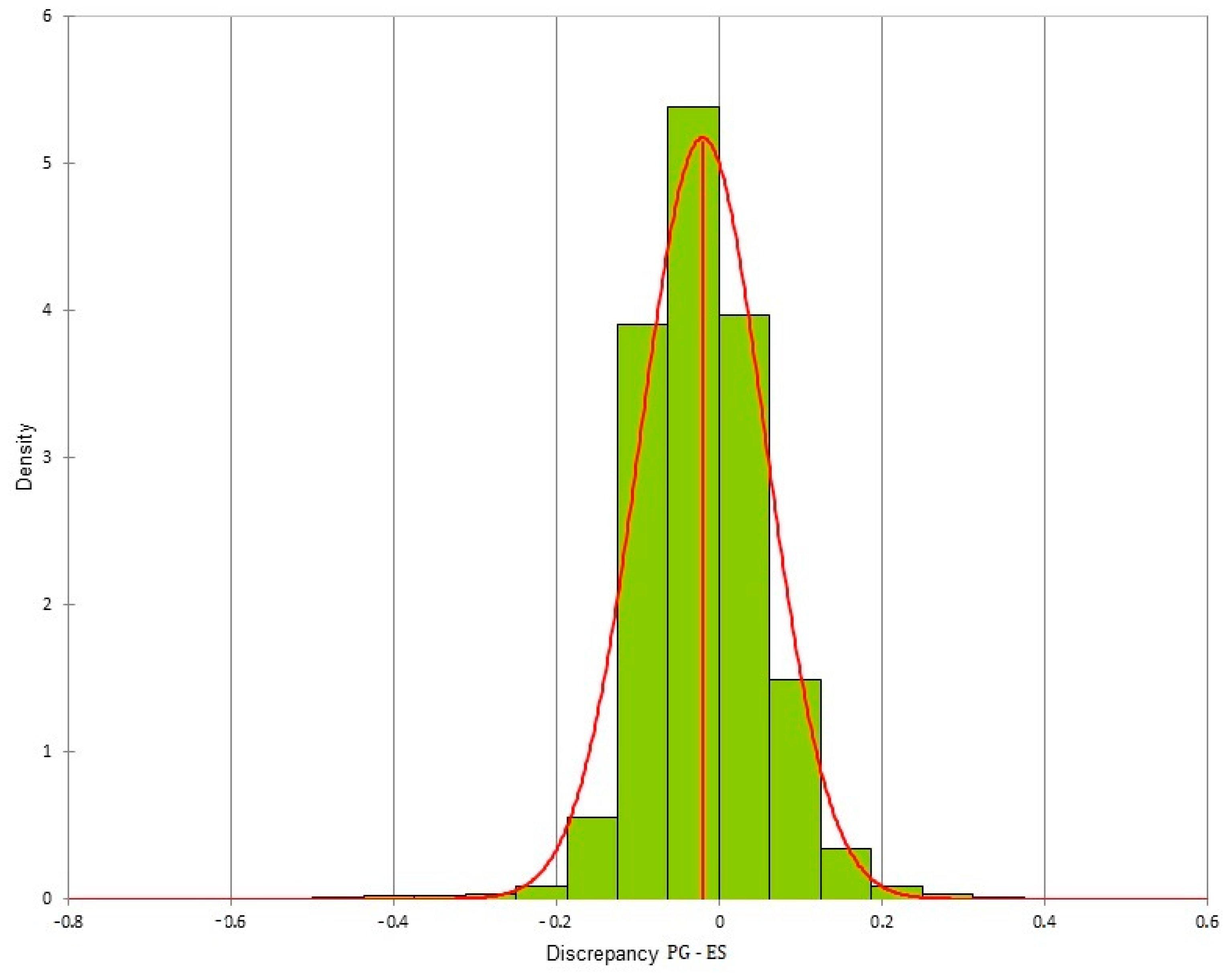
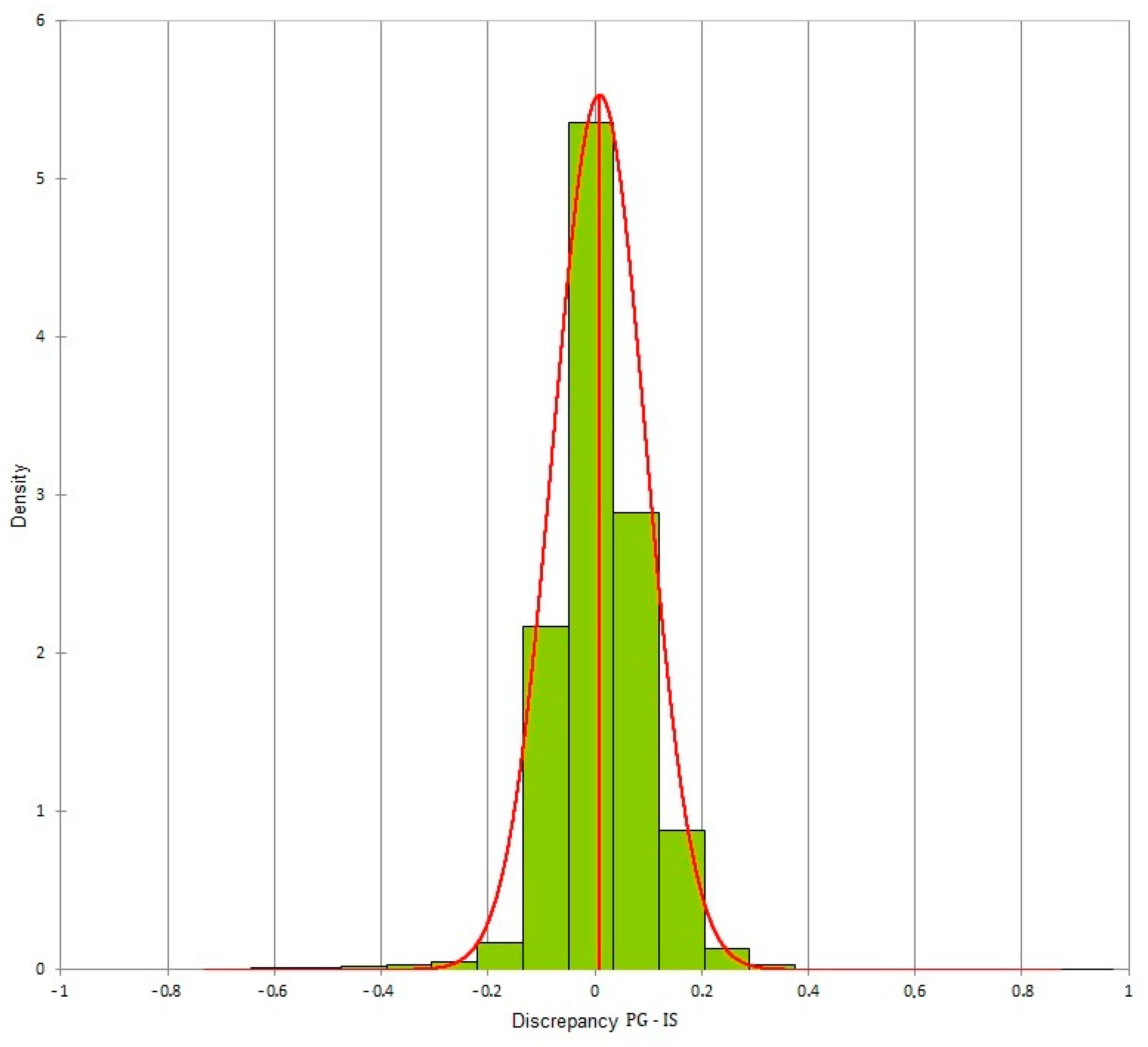
3.2. Trueness of Photogrammetry
- Photogrammetry/Dental extraoral laboratory scanner: −0.02 ± 0.077;
- Photogrammetry/Intraoral Scanner: 0.009 ± 0.087;
- Intraoral Scanner/Dental extraoral laboratory scanner: 0.031 ± 0.058.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Akyalcin, S. Are Digital Models Replacing Plaster Casts? Dentistry 2011, 1, 1–2. [Google Scholar] [CrossRef] [Green Version]
- Santoro, M.; Galkin, S.; Teredesai, M.; Nicolay, O.F.; Cangialosi, T.J. Comparison of measurements made on digital and plaster models. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 101–105. [Google Scholar] [CrossRef]
- Fleming, P.S.; Marinho, V.; Johal, A. Orthodontic measurements on digital study models compared with plaster models: A systematic review. Orthod. Craniofac. Res. 2011, 14, 1–16. [Google Scholar] [CrossRef] [PubMed]
- The American Society for Photogrammetry and Remote Sensing. Photogramm. Eng. Remote Sens. 1989, 55, 979–984.
- Evgenikou, V.; Georgopoulos, A. Investigating 3D reconstruction methods for small artifacts. Int. Arch. Photogramm. Remote Sens. Spat. Inf. Sci.-ISPRS Arch. 2015, 40, 101–108. [Google Scholar] [CrossRef] [Green Version]
- Stuani, V.T.; Ferreira, R.; Manfredi, G.G.P.; Cardoso, M.V.; Sant’Ana, A.C.P. Photogrammetry as an alternative for acquiring digital dental models: A proof of concept. Med. Hypotheses 2019, 128, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Silvester, C.M.; Hillson, S. A critical assessment of the potential for Structure-from-Motion photogrammetry to produce high fidelity 3D dental models. Am. J. Phys. Anthropol. 2020, 173, 381–392. [Google Scholar] [CrossRef]
- De Santis, D.; Sinigaglia, S.; Pancera, P.; Faccioni, P.; Luciano, U.; Setti, A.P.; Bursi, P.; Nocini, R.; Nocini, P.F.; Bertossi, D. An overview of guided bone regeneration. J. Biol. Regul. Homeost. Agents 2019, 33, 49–53. [Google Scholar]
- Da Pozzo, F.; Gibelli, D.; Beltramini, G.A.; Dolci, C.; Giannì, A.B.; Sforza, C. The Effect of Orthognathic Surgery on Soft-Tissue Facial Asymmetry: A Longitudinal Three-Dimensional Analysis. J. Craniofac. Surg. 2020, 31, 1578–1582. [Google Scholar] [CrossRef]
- Germec-Cakan, D.; Canter, H.I.; Nur, B.; Arun, T. Comparison of facial soft tissue measurements on three-dimensional images and models obtained with different methods. J. Craniofac. Surg. 2010, 21, 1393–1399. [Google Scholar] [CrossRef]
- Prakash, A. Photogrammetry As a Tool To Aid Orthodontic Diagnosis and Treatment. J. Contemp. Orthod. 2017, 1, 50–55. [Google Scholar]
- Piedra-Cascón, W.; Methani, M.M.; Quesada-Olmo, N.; Jiménez-Martínez, M.J.; Revilla-León, M. Scanning accuracy of nondental structured light extraoral scanners compared with that of a dental-specific scanner. J. Prosthet. Dent. 2020, 126, 110–114. [Google Scholar] [CrossRef] [PubMed]
- Mandelli, F.; Gherlone, E.; Gastaldi, G.; Ferrari, M. Evaluation of the accuracy of extraoral laboratory scanners with a single-tooth abutment model: A 3D analysis. J. Prosthodont. Res. 2017, 61, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Vlaar, S.T.; Van Der Zel, J.M. Accuracy of dental digitizers. Int. Dent. J. 2006, 56, 301–309. [Google Scholar] [CrossRef] [PubMed]
- Ender, A.; Mehl, A. Accuracy of complete-Arch dental impressions: A new method of measuring trueness and precision. J. Prosthet. Dent. 2013, 109, 121–128. [Google Scholar] [CrossRef] [Green Version]
- Flügge, T.V.; Schlager, S.; Nelson, K.; Nahles, S.; Metzger, M.C. Precision of intraoral digital dental impressions with iTero and extraoral digitization with the iTero and a model scanner. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Joda, T.; Lenherr, P.; Dedem, P.; Kovaltschuk, I.; Bragger, U.; Zitzmann, N.U. Time efficiency, difficulty, and operator’s preference comparing digital and conventional implant impressions: A randomized controlled trial. Clin. Oral Implant. Res. 2016, 28, 1318–1323. [Google Scholar] [CrossRef] [PubMed]
- Wismeijer, D.; Mans, R.; van Genuchten, M.; Reijers, H.A. Patients’ preferences when comparing analogue implant impressions using a polyether impression material versus digital impressions (Intraoral Scan) of dental implants. Clin. Oral Implants Res. 2014, 25, 1113–1118. [Google Scholar] [CrossRef]
- Yuzbasioglu, E.; Kurt, H.; Turunc, R.; Bilir, H. Comparison of digital and conventional impression techniques: Evaluation of patients’ perception, treatment comfort, effectiveness and clinical outcomes. BMC Oral Health 2014, 14, 10. [Google Scholar] [CrossRef] [Green Version]
- Park, H.R.; Park, J.M.; Chun, Y.S.; Lee, K.N.; Kim, M. Changes in views on digital intraoral scanners among dental hygienists after training in digital impression taking. BMC Oral Health 2015, 15, 151. [Google Scholar] [CrossRef] [Green Version]
- Joda, T.; Brägger, U. Time-Efficiency Analysis Comparing Digital and Conventional Workflows for Implant Crowns: A Prospective Clinical Crossover Trial. Int. J. Oral Maxillofac. Implants 2015, 30, 1047–1053. [Google Scholar] [CrossRef] [PubMed]
- Joda, T.; Brägger, U. Digital vs. conventional implant prosthetic workflows: A cost/time analysis. Clin. Oral Implants Res. 2015, 26, 1430–1435. [Google Scholar] [CrossRef] [PubMed]
- Ender, A.; Attin, T.; Mehl, A. In vivo precision of conventional and digital methods of obtaining complete-arch dental impressions. J. Prosthet. Dent. 2016, 115, 313–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masri, R.; Driscoll, C.F.; Gagliani, M. Clinical Application of Digital Dental Technology; Wiley-Blackwell: Ames, Iowa, 2017. [Google Scholar]
- Mangano, F.; Gandolfi, A.; Luongo, G.; Logozzo, S. Intraoral scanners in dentistry: A review of the current literature. BMC Oral Health 2017, 17, 149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandeweghe, S.; Vervack, V.; Vanhove, C.; Dierens, M.; Jimbo, R.; De Bruyn, H. Accuracy of Optical Dental Digitizers: An In Vitro Study. Int. J. Prosthodont. Restor. Dent. 2015, 35, 115–121. [Google Scholar] [CrossRef]
- Lie, A.; Jemt, T. Photogrammetric measurements of implant positions. Description of a technique to determine the fit between implants and superstructures. Clin. Oral Implants Res. 1994, 5, 30–36. [Google Scholar] [CrossRef]
- Sánchez-Monescillo, A.; Sánchez-Turrión, A.; Vellon-Domarco, E.; Salinas-Goodier, C.; Prados-Frutos, J. Photogrammetry Impression Technique: A Case History Report. Int. J. Prosthodont. 2016, 29, 71–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Revilla-León, M.; Att, W.; Özcan, M.; Rubenstein, J. Comparison of conventional, photogrammetry, and intraoral scanning accuracy of complete-arch implant impression procedures evaluated with a coordinate measuring machine. J. Prosthet. Dent. 2021, 125, 470–478. [Google Scholar] [CrossRef]
- Fu, X.; Peng, C.; Li, Z.; Liu, S.; Tan, M.; Song, J. The application of multi-baseline digital close-range photogrammetry in three-dimensional imaging and measurement of dental casts. PLoS ONE 2017, 12, e0178858. [Google Scholar] [CrossRef] [Green Version]
- Katz, D.; Friess, M. Technical note: 3D from standard digital photography of human crania-A preliminary assessment. Am. J. Phys. Anthropol. 2014, 154, 152–158. [Google Scholar] [CrossRef]
- Fourie, Z.; Damstra, J.; Gerrits, P.O.; Ren, Y. Evaluation of anthropometric accuracy and reliability using different three-dimensional scanning systems. Forensic Sci. Int. 2011, 207, 127–134. [Google Scholar] [CrossRef] [PubMed]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Mean | SD | CV (%) |
|---|---|---|---|
| Height 1.6. | 4.44 | 0.01 | 0.28 |
| Height 1.5. | 4.66 | 0.08 | 1.65 |
| Height 1.4. | 6.02 | 0.02 | 0.42 |
| Height 1.3. | 7.44 | 0.02 | 0.30 |
| Height 1.2. | 5.95 | 0.10 | 1.71 |
| Height 1.1. | 7.41 | 0.07 | 0.99 |
| Height 2.1. | 7.54 | 0.03 | 0.35 |
| Height 2.2. | 6.47 | 0.11 | 1.76 |
| Height 2.3. | 8.23 | 0.10 | 1.22 |
| Height 2.4. | 6.44 | 0.14 | 2.13 |
| Height 2.5. | 5.01 | 0.07 | 1.30 |
| Height 2.6. | 4.57 | 0.02 | 0.37 |
| Width 1.6. | 8.60 | 0.07 | 0.80 |
| Width 1.5. | 5.63 | 0.09 | 1.60 |
| Width 1.4. | 5.11 | 0.02 | 0.49 |
| Width 1.3. | 7.04 | 0.04 | 0.57 |
| Width 1.2. | 6.47 | 0.13 | 2.04 |
| Width 1.1. | 7.36 | 0.04 | 0.48 |
| Width 2.1. | 7.37 | 0.08 | 1.02 |
| Width 2.2. | 6.37 | 0.13 | 2.00 |
| Width 2.3. | 7.29 | 0.06 | 0.89 |
| Width 2.4. | 5.29 | 0.04 | 0.75 |
| Width 2.5. | 4.97 | 0.06 | 1.23 |
| Width 2.6. | 8.28 | 0.02 | 0.23 |
| Transverse 1.3.–2.3. | 34.11 | 0.13 | 0.37 |
| Transverse 1.6.–2.6. | 36.78 | 0.17 | 0.47 |
| Midline—1.3. | 18.24 | 0.14 | 0.77 |
| Midline—2.3. | 19.17 | 0.16 | 0.82 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zotti, F.; Rosolin, L.; Bersani, M.; Poscolere, A.; Pappalardo, D.; Zerman, N. Digital Dental Models: Is Photogrammetry an Alternative to Dental Extraoral and Intraoral Scanners? Dent. J. 2022, 10, 24. https://doi.org/10.3390/dj10020024
Zotti F, Rosolin L, Bersani M, Poscolere A, Pappalardo D, Zerman N. Digital Dental Models: Is Photogrammetry an Alternative to Dental Extraoral and Intraoral Scanners? Dentistry Journal. 2022; 10(2):24. https://doi.org/10.3390/dj10020024
Chicago/Turabian StyleZotti, Francesca, Luca Rosolin, Massimo Bersani, Andrea Poscolere, Davide Pappalardo, and Nicoletta Zerman. 2022. "Digital Dental Models: Is Photogrammetry an Alternative to Dental Extraoral and Intraoral Scanners?" Dentistry Journal 10, no. 2: 24. https://doi.org/10.3390/dj10020024
APA StyleZotti, F., Rosolin, L., Bersani, M., Poscolere, A., Pappalardo, D., & Zerman, N. (2022). Digital Dental Models: Is Photogrammetry an Alternative to Dental Extraoral and Intraoral Scanners? Dentistry Journal, 10(2), 24. https://doi.org/10.3390/dj10020024