
A Video-Game-Based Oral Health Intervention in Primary Schools—A Randomised Controlled Trial


Abstract
:
1. Introduction
2. Materials and Methods
2.1. Trial Design
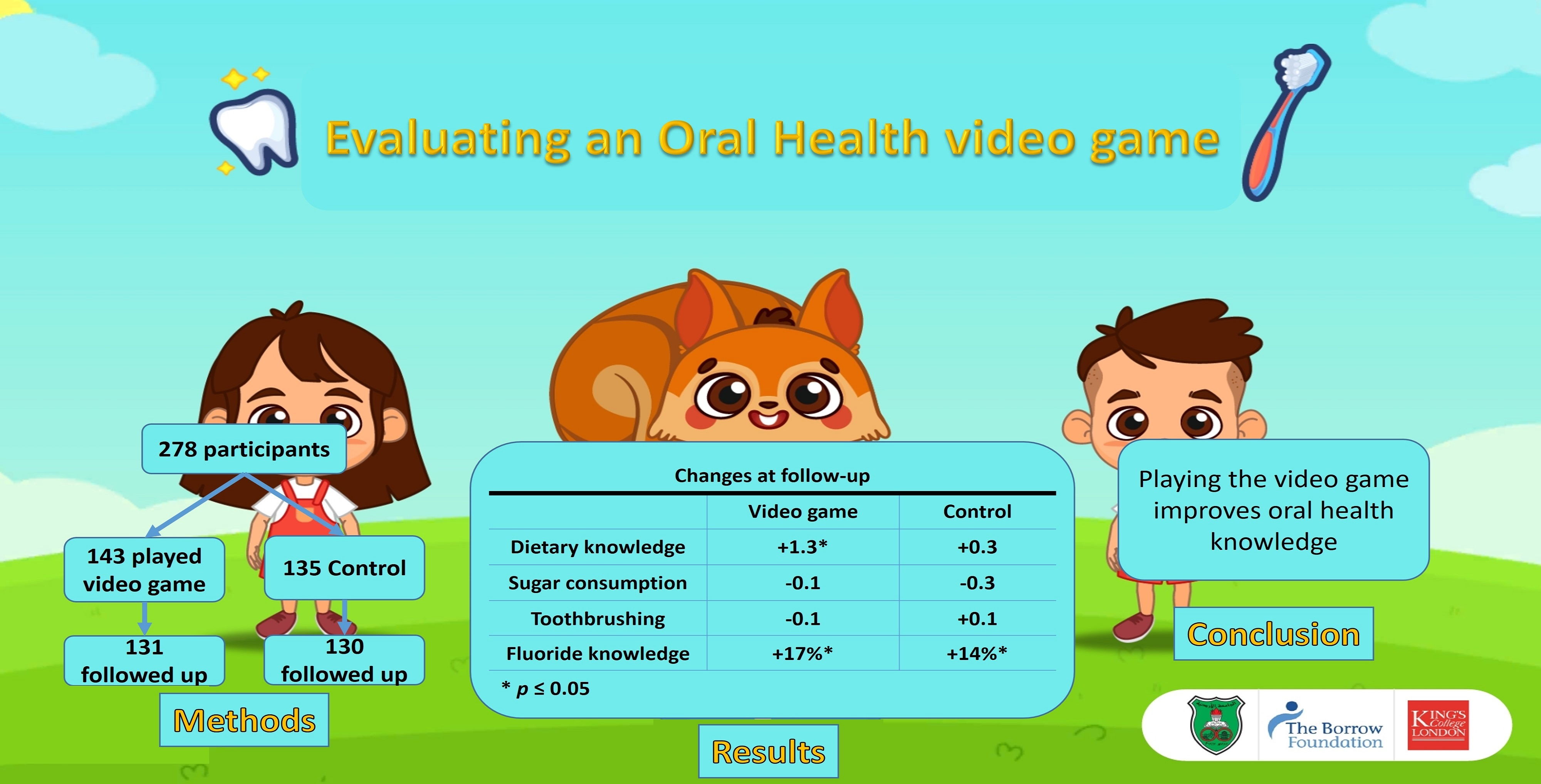
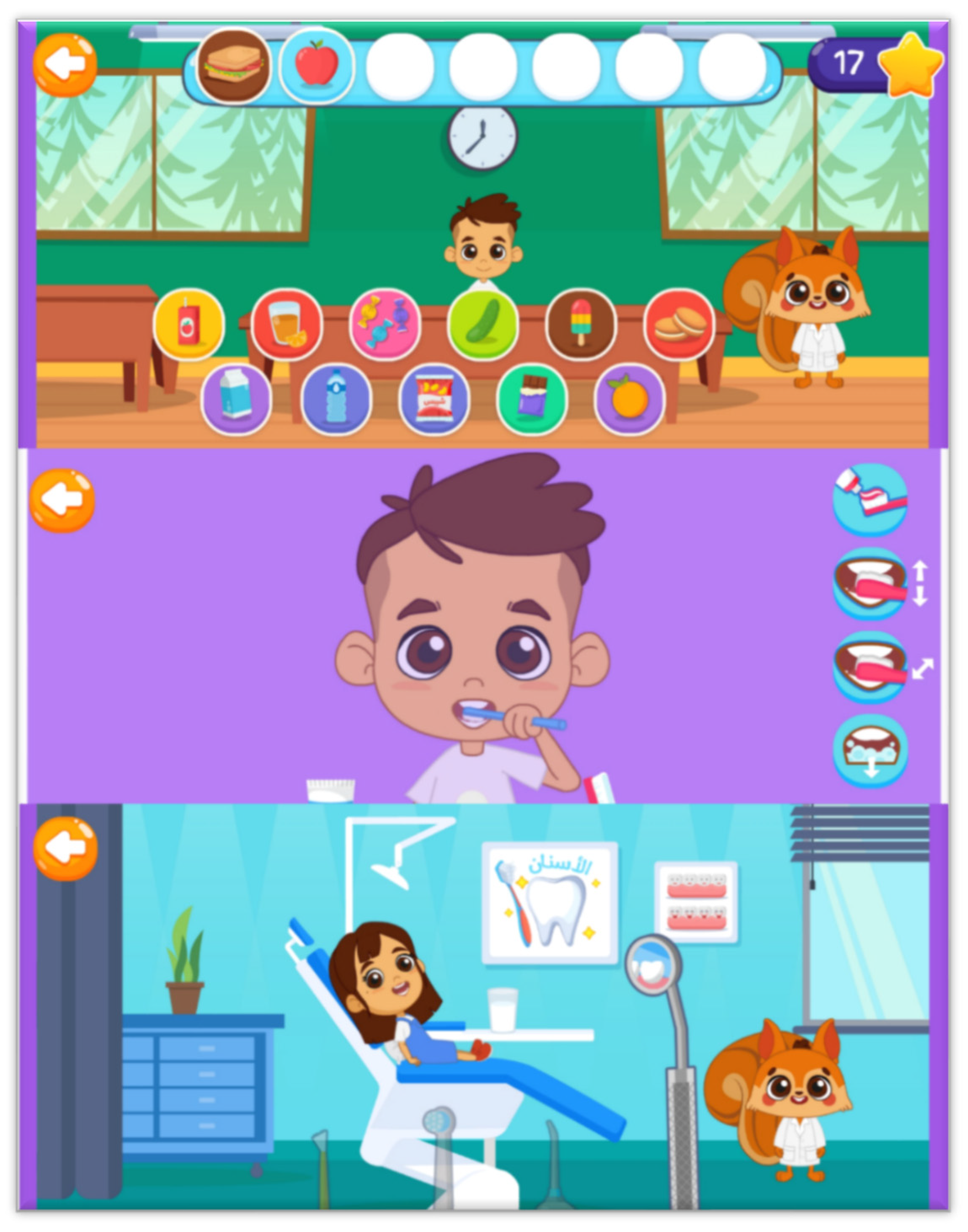
- Intervention group: children played an oral health education video game in school, and were given instructions to play the game at home.
- Control group: Received no intervention.
2.2. Participants
2.3. Interventions
2.4. Outcomes
2.4.1. Primary Outcome Measures
- Changes in children’s dietary knowledge recorded using a Pictorial Dietary Questionnaire (PDQ) [12]. The PDQ contains 70 food and drink items that the children are asked to classify into ‘healthy’ and ‘unhealthy’.
2.4.2. Secondary Outcome Measures
- Changes in dietary and toothbrushing practices reported by children using toothbrushing and diet diaries.
- Changes in dietary practices reported by parents using the Child Dietary Questionnaire (CDQ) [17]. The CDQ measures dietary intake in four domains: Fruits and vegetables, sweetened drinks, non-core foods, and fat from dairy.
- Changes in children’s toothbrushing habits, and changes to parental recognition of fluoride toothpaste concentration and in-office preventive treatments, recorded using a parental questionnaire.
- Changes in children’s plaque scores using the Simplified Oral Hygiene Index (S-OHI) [18].
- Number of children downloading and playing the game at home recorded using Google and Unity developer tools.
2.4.3. Data Collection
2.5. The Dental Examination
2.6. Sample Size
2.7. Randomisation and Blinding
2.8. Statistical Methods
3. Results
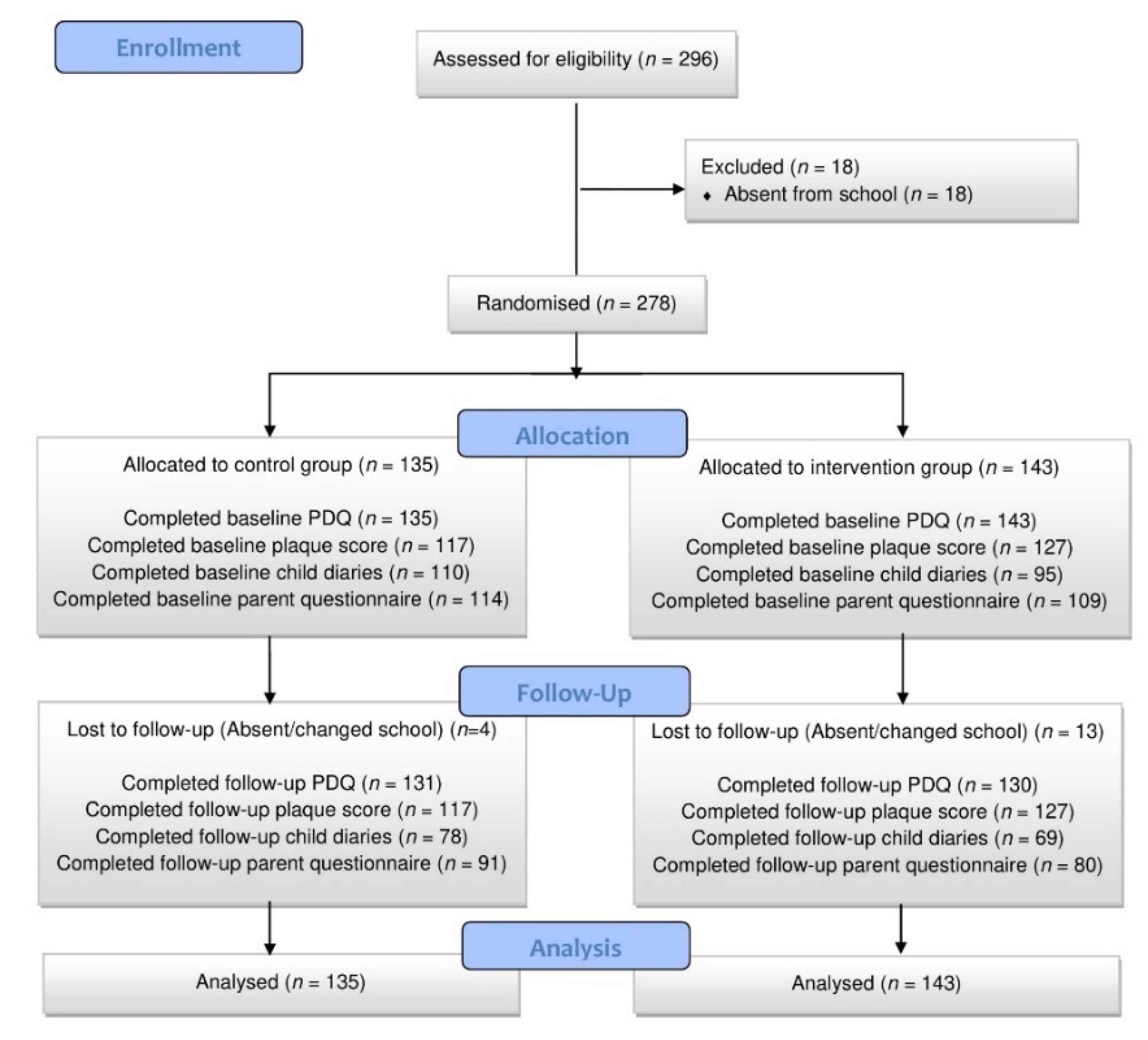
3.1. Recruitment
3.2. Sample Description
3.3. Children’s Dietary Knowledge
3.4. Child-Reported Dietary Practices
3.5. Parent-Reported Dietary Intake
3.6. Children’s Plaque Score
3.7. Child-Reported Toothbrushing Practices
3.8. Parent-Reported Toothbrushing Practices
3.9. Parent’s Knowledge of Preventive Therapies
3.10. Video Game Usage Patterns
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Petersen, P.E. The World Oral Health Report 2003: Continuous improvement of oral health in the 21st century-the approach of the WHO Global Oral Health Programme. Community Dent. Oral Epidemiol. 2013, 31, 3–24. [Google Scholar] [CrossRef] [PubMed]
- Marthaler, T.M. Changes in dental caries 1953–2003. Caries Res. 2004, 38, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Rajab, L.D.; Petersen, P.E.; Baqain, Z.; Bakaeen, G. Oral Health Status Among 6- and 12-year-old Jordanian Schoolchildren. Oral Health Prev. Dent. 2014, 12, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Rajab, L.D.; Hamdan, M.A.M. Early childhood caries and risk factors in Jordan. Community Dent. Health 2002, 19, 224–229. [Google Scholar] [PubMed]
- Sayegh, A.; Dini, E.; Holt, R.; Bedi, R. Oral health, sociodemographic factors, dietary and oral hygiene practices in Jordanian children. J. Dent. 2005, 33, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Rajab, L.D.; Petersen, P.E.; Bakaeen, G.; Hamdan, M.A. Oral health behaviour of schoolchildren and parents in Jordan. Int. J. Paediatr. Dent. 2002, 12, 168–176. [Google Scholar] [CrossRef] [PubMed]
- ElKarmi, R.; Aljafari, A.; Eldali, H.; Hosey, M.T. Do expectant mothers know how early childhood caries can be prevented? A cross-sectional study. Eur. Arch. Paediatr. Dent. 2019, 20, 595–601. [Google Scholar] [CrossRef]
- World Health Organization. An International Conference on Health Promotion: The Move Towards a New Public Health; Ottawa Charter for Health Promotion: Ottawa, ON, Canada, 1986. [Google Scholar]
- Michie, S.; West, R. Behaviour change theory and evidence: A presentation to Government. Health Psychol. Rev. 2013, 7, 1–22. [Google Scholar] [CrossRef]
- Vogel, J.J.; Vogel, D.S.; Cannon-Bowers, J.; Bowers, C.A.; Muse, K.; Wright, M. Computer Gaming and Interactive Simulations for Learning: A Meta-Analysis. J. Educ. Comput. Res. 2006, 34, 229–243. [Google Scholar] [CrossRef]
- Primack, B.A.; Carroll, M.V.; McNamara, M.; Klem, M.L.; King, B.; Rich, M.; Chan, C.W.; Nayak, S. Role of Video Games in Improving Health-Related Outcomes: A Systematic Review. Am. J. Prev. Med. 2012, 42, 630–638. [Google Scholar] [CrossRef] [Green Version]
- Aljafari, A.; Rice, C.; Gallagher, J.E.; Hosey, M.T. An oral health education video game for high caries risk children: Study protocol for a randomized controlled trial. Trials 2015, 16, 237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aljafari, A.; Gallagher, J.E.; Hosey, M.T. Can oral health education be delivered to high-caries-risk children and their parents using a computer game?-A randomised controlled trial. Int. J. Paediatr. Dent. 2017, 27, 476–485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Education. ICT Use and Diffusion in Schools in Jordan; Ministry of Education: Amman, Jordan, 2012. [Google Scholar]
- Pew Research Center. Social Media Use Continues to Rise in Developing Countries, but Plateaus across Developed Ones; Pew Research Center: Washington DC, USA, 2018; Available online: https://www.pewresearch.org/global/2018/06/19/global-technology-use-appendix-d-detailed-tables/ (accessed on 4 November 2021).
- Public Health England. Delivering Better Oral Health: An Evidence-Based Toolkit for Prevention, 3rd ed.; Public Health England: London, UK, 2017. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/605266/Delivering_better_oral_health.pdf (accessed on 4 November 2021).
- Magarey, A.; Golley, R.; Spurrier, N.; Goodwin, E.; Ong, F. Reliability and validity of the Children’s Dietary Questionnaire; a new tool to measure children’s dietary patterns. Int J. Pediatr. Obes. 2009, 4, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Greene, J.G.; Vermillion, J.R. The Simplified Oral Hygiene Index. J. Am. Dent. Assoc. 1964, 68, 7–13. [Google Scholar] [CrossRef]
- World Health Organization. Oral Health Surveys Basic Methods, 5th ed.; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- MacPherson, L.M.D.; Anopa, Y.; Conway, D.I.; McMahon, A.D. National Supervised Toothbrushing Program and Dental Decay in Scotland. J. Dent. Res. 2012, 92, 109–113. [Google Scholar] [CrossRef]
- Weintraub, J.A.; Ramos-Gomez, F.; Jue, B.; Shain, S.; Hoover, C.I.; Featherstone, J.D.B.; Gansky, S.A. Fluoride varnish efficacy in preventing early childhood caries. J. Dent. Res. 2006, 85, 172–176. [Google Scholar] [CrossRef]
- Allen, M.; Allen, J.; Hogarth, S.; Marmot, M. Working for Health Equity: The Role of Health Professionals; UCL Institute of Health Equity: London, UK, 2013. [Google Scholar]
- Baranowski, T.; Baranowski, J.; Cullen, K.W.; Marsh, T.; Islam, N.; Zakeri, I.; Honess-Morreale, L.; Demoor, C. Squire’s Quest! Dietary outcome evaluation of a multimedia game. Am. J. Prev. Med. 2003, 24, 52–61. [Google Scholar] [CrossRef]
- Turnin, M.C.; Tauber, M.T.; Couvaras, O.; Jouret, B.; Bolzonella, C.; Bourgeois, O.; Buisson, J.C.; Fabre, D.; Cance-Rouzaud, A.; Tauber, J.P.; et al. Evaluation of microcomputer nutritional teaching games in 1876 children at school. Clin. Trial 2001, 27, 459–464. [Google Scholar]
- Jacobson, D.; Jacobson, J.; Leong, T.; Lourenco, S.; Mancl, L.; Chi, D.L. Evaluating Child Toothbrushing Behavior Changes Associated with a Mobile Game App: A Single Arm Pre/Post Pilot Study. Int. J. Clin. Pediatr. Dent. 2019, 41, 299–303. [Google Scholar]
- Scribante, A.; Gallo, S.; Bertino, K.; Meles, S.; Gandini, P.; Sfondrini, M.F. The Effect of Chairside Verbal Instructions Matched with Instagram Social Media on Oral Hygiene of Young Orthodontic Patients: A Randomized Clinical Trial. Appl. Sci. 2021, 11, 706. [Google Scholar] [CrossRef]
- Parsons, H.M. What happened at Hawthorne? New evidence suggests the Hawthorne effect resulted from operant reinforcement contingencies. Science 1974, 183, 922–932. [Google Scholar] [CrossRef] [PubMed]
- Aljafari, A.; ElKarmi, R.; Kussad, J.; Hosey, M.T. General dental practitioners’ approach to caries prevention in high-caries-risk children. Eur. Arch. Paediatr. Dent. 2020, 22, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, P.A.; Donaldson, A.N.; Liossi, C.; Newton, J.T.; Donaldson, N.K.; Arias, R.; Haria, P.; Huntington, C.; Alharatani, R.; Hosey, M.T. How families prepare their children for tooth extraction under general anaesthesia: Family and clinical predictors of non-compliance with a ‘serious game’. Int. J. Paediatr. Dent. 2019, 29, 117–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacPherson, L.M.D.; Ball, G.E.; Brewster, L.; Duane, B.; Hodges, C.-L.; Wright, W.; Gnich, W.; Rodgers, J.; McCall, D.R.; Turner, S.; et al. Childsmile: The national child oral health improvement programme in Scotland. Part 1: Establishment and development. Br. Dent. J. 2010, 209, 73–78. [Google Scholar] [CrossRef]
- Roberts, K.; Flaherty, S.J. Review of Dietary Assessment Methods in Public Health; National Obesity Observatory: Oxford, UK, 2010. [Google Scholar]
- Gil, G.S.; Morikava, F.S.; Santin, G.C.; Pintarelli, T.P.; Fraiz, F.C.; Ferreira, F.M. Reliability of self-reported toothbrushing frequency as an indicator for the assessment of oral hygiene in epidemiological research on caries in adolescents: A cross-sectional study. BMC Med. Res. Methodol. 2015, 15, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Department of Statistics [Jordan] and ICF. Jordan Population and Family Health Survey 2017–18: Key Findings; Department of Statistics [Jordan]: Amman, Jordan; ICF: Rockville, MA, USA, 2019. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
| Intervention Group | Control Group | |
|---|---|---|
| Mean ± SD | Mean ± SD | |
| Age | 6.5 ± 0.5 | 6.5 ± 0.5 |
| dmft | 5.3 ± 2.9 | 4.8 ± 3.0 |
| Mother’s age | 34.8 ± 6.6 | 35.4 ± 6.1 |
| Father’s age | 41.8 ± 8.1 | 41.8 ± 7.3 |
| n (%) | n (%) | |
| First grade | 69 (48%) | 65 (48%) |
| Second grade | 74 (52%) | 70 (52%) |
| Male | 77 (54%) | 65 (48%) |
| Female | 66 (46%) | 70 (52%) |
| Both parents unemployed | 12 (11%) | 10 (9%) |
| At least one parent employed | 95 (89%) | 98 (91%) |
| Mother attended primary school only | 32 (30%) | 12 (11%) |
| Mother attended secondary school or higher | 76 (70%) | 96 (89%) |
| Father attended primary school only | 40 (38%) | 14 (13%) |
| Father attended secondary school or higher | 66 (62%) | 94 (87%) |
| Domain | Baseline Mean ± SD | Follow-Up Mean ± SD | p-Value | ||
|---|---|---|---|---|---|
| Dietary knowledge | PDQ score | Control | 57.2 ± 4.9 | 57.5 ± 5.1 | 0.60 |
| Intervention | 56.5 ± 5.9 | 57.8 ± 6.3 | 0.019 * | ||
| Intergroup difference at follow up p = 0.12 | |||||
| Dietary practices | Number of sugary snacks | Control | 1.6 ± 1.1 | 1.3 ± 1.0 | 0.20 |
| Intervention | 1.2 ± 0.9 | 1.1 ± 0.9 | 0.92 | ||
| Intergroup difference at follow up p = 0.12 | |||||
| Fruits and vegetables (recommended ≥ 14) | Control | 13.4 ± 5.5 | 14.7 ± 5.3 | 0.06 | |
| Intervention | 13.6 ± 5.9 | 14.1 ± 6.9 | 0.61 | ||
| Intergroup difference at follow up p = 0.36 | |||||
| Fat from dairy (recommended = 0) | Control | 6.7 ± 5.2 | 7.5 ± 4.9 | 0.25 | |
| Intervention | 7.6 ± 4.9 | 7.7 ± 5.3 | 0.95 | ||
| Intergroup difference at follow up p = 0.46 | |||||
| Sweetened drinks (recommended ≤ 1) | Control | 2.5 ± 1.7 | 2.4 ± 1.7 | 0.84 | |
| Intervention | 2.6 ± 1.8 | 2.5 ± 1.7 | 0.62 | ||
| Intergroup difference at follow up p = 0.81 | |||||
| Non-core foods (recommended ≤ 2) | Control | 2.7 ± 1.3 | 2.8 ± 1.7 | 0.65 | |
| Intervention | 3.1 ± 1.5 | 3.3 ± 1.6 | 0.57 | ||
| Intergroup difference at follow up p = 0.91 | |||||
| Domain | Baseline | Follow-Up | |||
|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | p-Value | |||
| Oral hygiene practices | Plaque score | Control | 1.09 ± 0.39 | 1.21 ± 0.35 | 0.01 * |
| Intervention | 1.16 ± 0.30 | 1.17 ± 0.29 | 0.29 | ||
| Intergroup difference at follow up p = 0.08 | |||||
| Brushing frequency | Control | 1.3 ± 0.74 | 1.4 ± 0.72 | 0.60 | |
| Intervention | 1.7 ± 0.44 | 1.6 ± 0.47 | 0.65 | ||
| Intergroup difference at follow up p = 0.81 | |||||
| n (%) | n (%) | ||||
| Child brushes twice or more daily | Control | 32 (29%) | 35 (41%) | 0.14 | |
| Intervention | 40 (37%) | 32 (41%) | 0.99 | ||
| Intergroup difference at follow up p = 0.65 | |||||
| Child brushes supervised | Control | 17 (16%) | 8 (10%) | 0.13 | |
| Intervention | 15 (14%) | 12 (15%) | 0.99 | ||
| Intergroup difference at follow up p = 0.51 | |||||
| Parent not sure of correct toothpaste concentration | Control | 71 (65%) | 56 (64%) | 0.82 | |
| Intervention | 64 (59%) | 42 (55%) | 0.06 | ||
| Intergroup difference at follow up p = 0.14 | |||||
| Parental familiarity with preventive treatments | Parent familiar with fluoride varnish | Control | 38 (35%) | 44 (49%) | 0.019 * |
| Intervention | 36 (33%) | 39 (50%) | 0.035 * | ||
| Intergroup difference at follow up p = 0.94 | |||||
| Parent familiar with fissure sealants | Control | 19 (17%) | 30 (65%) | 0.002 * | |
| Intervention | 23 (21%) | 17 (22%) | 0.99 | ||
| Intergroup difference at follow up p = 0.001 * | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aljafari, A.; ElKarmi, R.; Nasser, O.; Atef, A.; Hosey, M.T. A Video-Game-Based Oral Health Intervention in Primary Schools—A Randomised Controlled Trial. Dent. J. 2022, 10, 90. https://doi.org/10.3390/dj10050090
Aljafari A, ElKarmi R, Nasser O, Atef A, Hosey MT. A Video-Game-Based Oral Health Intervention in Primary Schools—A Randomised Controlled Trial. Dentistry Journal. 2022; 10(5):90. https://doi.org/10.3390/dj10050090
Chicago/Turabian StyleAljafari, Ahmad, Rawan ElKarmi, Osama Nasser, Ala’a Atef, and Marie Therese Hosey. 2022. "A Video-Game-Based Oral Health Intervention in Primary Schools—A Randomised Controlled Trial" Dentistry Journal 10, no. 5: 90. https://doi.org/10.3390/dj10050090
APA StyleAljafari, A., ElKarmi, R., Nasser, O., Atef, A., & Hosey, M. T. (2022). A Video-Game-Based Oral Health Intervention in Primary Schools—A Randomised Controlled Trial. Dentistry Journal, 10(5), 90. https://doi.org/10.3390/dj10050090