
A 3D Digital Analysis of the Hard Palate Wound Healing after Free Gingival Graft Harvest: A Pilot Study in the Short Term

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Patient Screening and Informed Consent
2.3. Surgeries and Connective Tissues Grafts Harvesting
2.4. Patient Evaluation and Data Collected
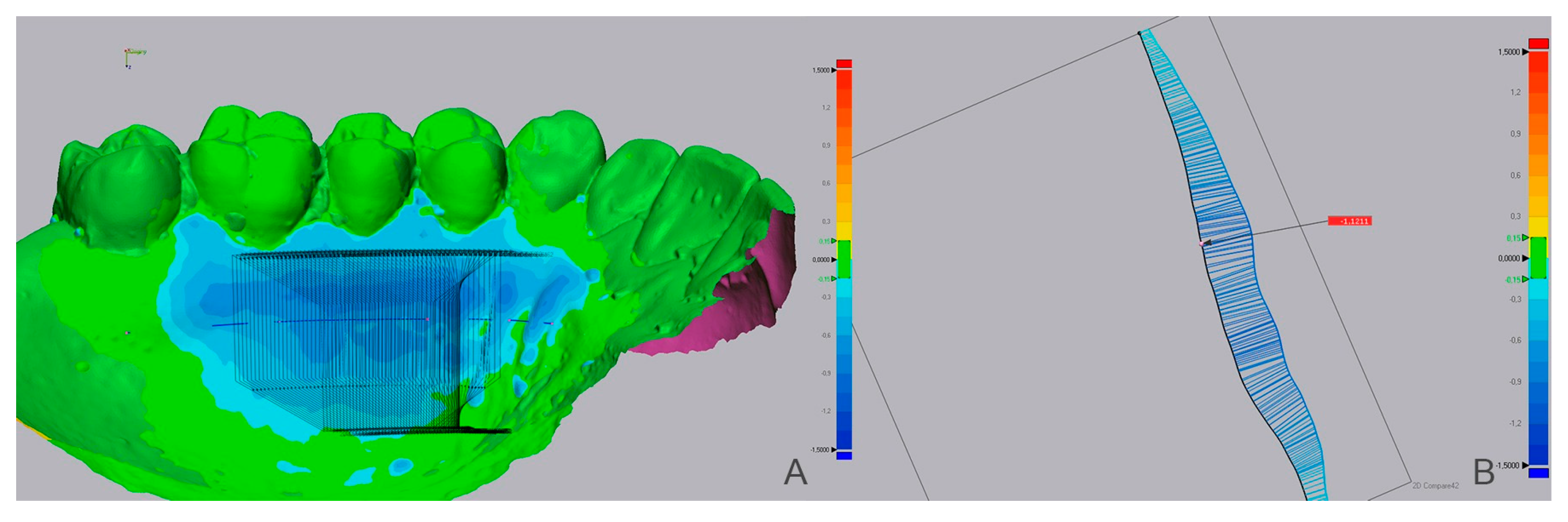
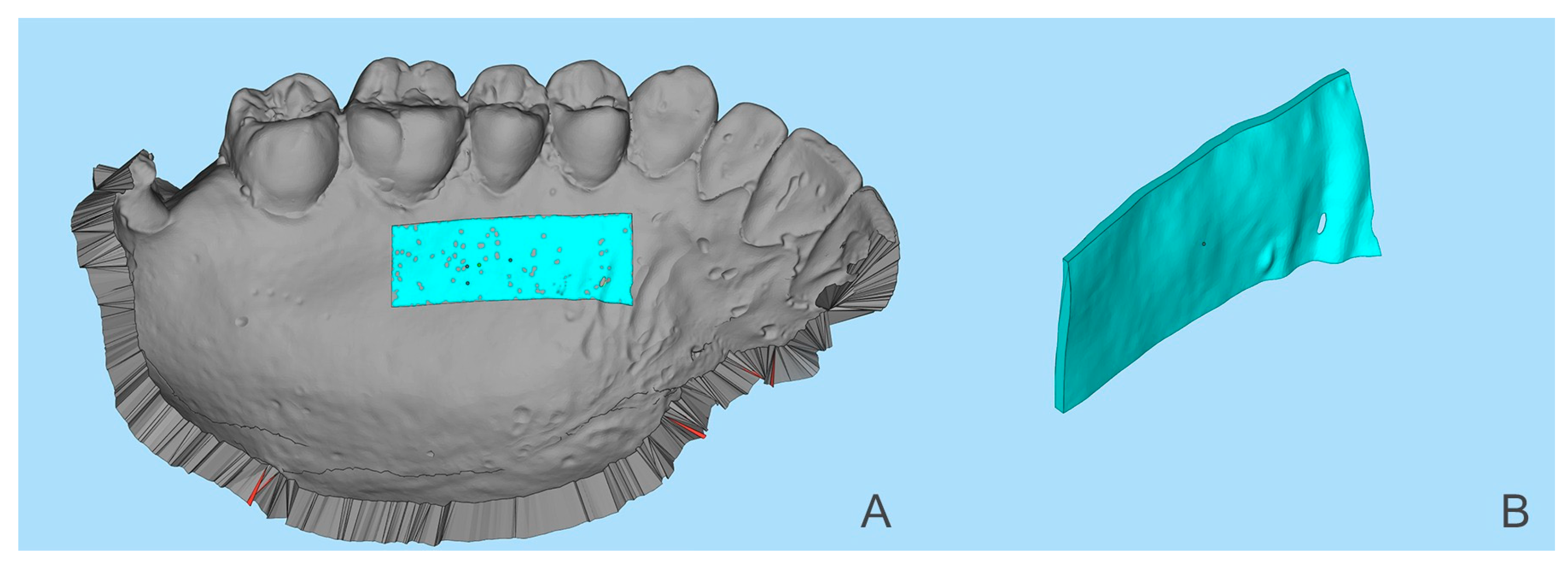
2.5. Measurements Obtained by Software Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Zucchelli, G.; Mounssif, I. Periodontal plastic surgery. Periodontol. 2000, 68, 333–368. [Google Scholar] [CrossRef] [PubMed]
- Klosek, S.K.; Rungruang, T. Anatomical study of the greater palatine artery and related structures of the palatal vault: Considerations for palate as the subepithelial connective tissue graft donor site. Surg. Radiol. Anat. 2009, 31, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Chambrone, L.; Tatakis, D.N. Periodontal Soft Tissue Root Coverage Procedures: A Systematic Review from the AAP Regeneration Workshop. J. Periodontol. 2015, 86, S8–S51. [Google Scholar] [CrossRef]
- Cortellini, P.; Tonetti, M.; Baldi, C.; Francetti, L.; Rasperini, G.; Rotundo, R.; Nieri, M.; Franceschi, D.; Labriola, A.; Pini Prato, G. Does placement of a connective tissue graft improve the outcomes of coronally advanced flap for coverage of single gingival recessions in upper anterior teeth? A multi-centre, randomized, double-blind, clinical trial. J. Clin. Periodontol. 2009, 36, 68–79. [Google Scholar] [CrossRef]
- Sullivan, H.C.; Atkins, J.H. Free autogenous gingival grafts. I. Principles of successful grafting. Periodontics 1968, 6, 121–129. [Google Scholar]
- Bertl, K.; Pifl, M.; Hirtler, L.; Rendl, B.; Nürnberger, S.; Stavropoulos, A.; Ulm, C. Relative Composition of Fibrous Connective and Fatty/Glandular Tissue in Connective Tissue Grafts Depends on the Harvesting Technique but not the Donor Site of the Hard Palate. J. Periodontol. 2015, 86, 1331–1339. [Google Scholar] [CrossRef]
- Studer, S.P.; Allen, E.P.; Rees, T.C.; Kouba, A. The Thickness of Masticatory Mucosa in the Human Hard Palate and Tuberosity as Potential Donor Sites for Ridge Augmentation Procedures. J. Periodontol. 1997, 68, 145–151. [Google Scholar] [CrossRef]
- Kuriakose, A.; Raju, S. Assessment of thickness of palatal mucosal donor site and its association with age and gender. J. Indian Soc. Periodontol. 2012, 16, 370. [Google Scholar] [CrossRef]
- Wara-aswapati, N.; Pitiphat, W.; Chandrapho, N.; Rattanayatikul, C.; Karimbux, N. Thickness of Palatal Masticatory Mucosa Associated With Age. J. Periodontol. 2001, 72, 1407–1412. [Google Scholar] [CrossRef]
- Stipetic, J.; Hrala, Z.; Celebic, A. Thickness of masticatory mucosa in the human hard palate and tuberosity dependent on gender and body mass index. Coll. Antropol. 2005, 29, 243–247. [Google Scholar]
- Müller, H.P.; Schaller, N.; Eger, T.; Heinecke, A. Thickness of masticatory mucosa. J. Clin. Periodontol. 2000, 27, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Hungund, S.; Astekar, M.; Dodani, K. Evaluation of palatal mucosal thickness and its association with age and gender. Biotech. Histochem. 2014, 89, 481–487. [Google Scholar] [CrossRef] [PubMed]
- Griffin, T.J.; Cheung, W.S.; Zavras, A.I.; Damoulis, P.D. Postoperative complications following gingival augmentation procedures. J. Periodontol. 2006, 77, 2070–2079. [Google Scholar] [CrossRef] [PubMed]
- Zuhr, O.; Bäumer, D.; Hürzeler, M. The addition of soft tissue replacement grafts in plastic periodontal and implant surgery: Critical elements in design and execution. J. Clin. Periodontol. 2014, 41, S123–S142. [Google Scholar] [CrossRef]
- Kim, D.H.; Won, S.Y.; Bae, J.H.; Jung, U.W.; Park, D.S.; Kim, H.J.; Hu, K.S. Topography of the greater palatine artery and the palatal vault for various types of periodontal plastic surgery. Clin. Anat. 2014, 27, 578–584. [Google Scholar] [CrossRef]
- Schacher, B.; Bürklin, T.; Horodko, M.; Raetzke, P.; Ratka-Krüger, P.; Eickholz, P. Direct thickness measurements of the hard palate mucosa. Quintessence Int. 2010, 41, e149. [Google Scholar]
- Song, J.-E.; Um, Y.-J.; Kim, C.-S.; Choi, S.-H.; Cho, K.-S.; Kim, C.-K.; Chai, J.-K.; Jung, U.-W. Thickness of Posterior Palatal Masticatory Mucosa: The Use of Computerized Tomography. J. Periodontol. 2008, 79, 406–412. [Google Scholar] [CrossRef]
- Barriviera, M.; Duarte, W.R.; Januário, A.L.; Faber, J.; Bezerra, A.C.B. A new method to assess and measure palatal masticatory mucosa by cone-beam computerized tomography. J. Clin. Periodontol. 2009, 36, 564–568. [Google Scholar] [CrossRef]
- McLeod, D.E.; Reyes, E.; Branch-Mays, G. Treatment of Multiple Areas of Gingival Recession Using a Simple Harvesting Technique for Autogenous Connective Tissue Graft. J. Periodontol. 2009, 80, 1680–1687. [Google Scholar] [CrossRef]
- Zucchelli, G.; Mele, M.; Stefanini, M.; Mazzotti, C.; Marzadori, M.; Montebugnoli, L.; Stefanini, M.; Mazzotti, C. Patient morbidity and root coverage outcome after subepithelial connective tissue and de-epithelialized grafts: A comparative randomized- controlled clinical trial. J. Clin. Periodontol. 2010, 37, 728–738. [Google Scholar] [CrossRef]
- Del Pizzo, M.; Modica, F.; Bethaz, N.; Priotto, P.; Romagnoli, R. The connective tissue graft: A comparative clinical evaluation of wound healing at the palatal donor site—A preliminary study. J. Clin. Periodontol. 2002, 29, 848–854. [Google Scholar] [CrossRef] [PubMed]
- Keskiner, I.; Aydogdu, A.; Balli, U.; Kaleli, A.E. Quantitative changes in palatal donor site thickness after free gingival graft harvesting: A pilot study. J. Clin. Periodontol. 2016, 43, 976–984. [Google Scholar] [CrossRef] [PubMed]
- Von den Hoff, J.W.; Maltha, J.C.; Kuijpers-Jagtman, A.M. Palatal Wound Healing: The Effects of Scarring on Growth. In Cleft Lip and Palate; Springer: Berlin/Heidelberg, Germany, 2013; pp. 309–324. ISBN 9783642307706. [Google Scholar]
- Cairo, F.; Nieri, M.; Cincinelli, S.; Mervelt, J.; Pagliaro, U. The interproximal clinical attachment level to classify gingival recessions and predict root coverage outcomes: An explorative and reliability study. J. Clin. Periodontol. 2011, 38, 661–666. [Google Scholar] [CrossRef]
- Rebele, S.F.; Zuhr, O.; Schneider, D.; Jung, R.E.; Hürzeler, M.B. Tunnel technique with connective tissue graft versus coronally advanced flap with enamel matrix derivative for root coverage: A RCT using 3D digital measuring methods. Part II. Volumetric studies on healing dynamics and gingival dimensions. J. Clin. Periodontol. 2014, 41, 593–603. [Google Scholar] [CrossRef] [Green Version]
- Chan, H.-L.; Sinjab, K.; Li, J.; Chen, Z.; Wang, H.-L.; Kripfgans, O.D. Ultrasonography for noninvasive and real-time evaluation of peri-implant tissue dimensions. J. Clin. Periodontol. 2018, 45, 986–995. [Google Scholar] [CrossRef]
- Horner, K.; Islam, M.; Flygare, L.; Tsiklakis, K.; Whaites, E. Basic principles for use of dental cone beam computed tomography: Consensus guidelines of the European Academy of Dental and Maxillofacial Radiology. Dentomaxillofacial Radiol. 2009, 38, 187–195. [Google Scholar] [CrossRef] [Green Version]
- Ramos, S.; Marques, T.; Santos, N.; Borges, T.; Correia, A.; Sousa, M.; Fernandes, G. Palatal soft-tissue changes after connective tissue graft harvesting—Tridimensional evaluation. Clin. Oral. Implants Res. 2019, 30, 444. [Google Scholar] [CrossRef]
- Windisch, S.I.; Jung, R.E.; Sailer, I.; Studer, S.P.; Ender, A.; Hämmerle, C.H.F. A new optical method to evaluate three-dimensional volume changes of alveolar contours: A methodological in vitro study. Clin. Oral Implants Res. 2007, 18, 545–551. [Google Scholar] [CrossRef]
- Ronay, V.; Sahrmann, P.; Bindl, A.; Attin, T.; Schmidlin, P.R. Current Status and Perspectives of Mucogingival Soft Tissue Measurement Methods. J. Esthet. Restor. Dent. 2011, 23, 146–156. [Google Scholar] [CrossRef]
- Yan, S.; Shi, S.-G.; Niu, Z.-Y.; Pei, Z.; Shi, S.-M.; Mu, C. Soft tissue image reconstruction using cone-beam computed tomography combined with laser scanning: A novel method to evaluate the masticatory mucosa. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. 2014, 118, 725–731. [Google Scholar] [CrossRef]
- Silva, C.O.; Ribeiro, E.D.P.; Sallum, A.W.; Tatakis, D.N. Free Gingival Grafts: Graft Shrinkage and Donor-Site Healing in Smokers and Non-Smokers. J. Periodontol. 2010, 81, 692–701. [Google Scholar] [CrossRef] [PubMed]
- Tavelli, L.; Barootchi, S.; Siqueira, R.; Kauffmann, F.; Majzoub, J.; Stefanini, M.; Zucchelli, G.; Wang, H.-L. Three-dimensional volumetric analysis of the palatal donor site following soft tissue harvesting. Int. J. Periodontics Restor. Dent. 2022, 42, 393–399. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case Number | TA (mm) | MTL (mm) | MTL (mm) | VA (mm3) |
|---|---|---|---|---|
| 1 | 0.18 ± 0.12 | −0.23 | 0.08 ± 0.06 | 4.18 |
| 2 | −0.15 ± 0.11 | −0.66 | −0.27 ± 0.04 | 30.90 |
| 3 | −0.04 ± 0.10 | −0.45 | −0.23 ± 0.03 | 2.72 |
| 4 | −0.03 ± 0.12 | −0.47 | −0.15 ± 0.07 | 3.47 |
| 5 | −0.19 ± 0.17 | −1.08 | −0.47 ± 0.04 | 37.20 |
| 6 | 0.04 ± 0.08 | −0.20 | −0.03 ± 0.06 | 2.19 |
| 7 | −1.10 ± 0.34 | −2.15 | −1.49 ± 0.14 | 161.61 |
| 8 | −0.58 ± 0.13 | −0.91 | −0.68 ± 0.09 | 90.90 |
| 9 | −0.30 ± 0.13 | −0.70 | −0.39 ± 0.06 | 52.48 |
| 10 | −0.61 ± 0.24 | −1.23 | −0.85 ± 0.10 | 131.52 |
| 11 | −0.16 ± 0.11 | −0.46 | −0.27 ± 0.04 | 16.92 |
| 12 | −0.21 ± 0.18 | −1.31 | −0.62 ± 0.04 | 35.54 |
| 13 | −0.23 ± 0.30 | −0.81 | −0.44 ± 0.06 | 56.74 |
| 14 | −0.25 ± 0.13 | −0.79 | −0.41 ± 0.05 | 41.51 |
| 15 | −0.26 ± 0.16 | −0.75 | −0.40 ± 0.07 | 37.07 |
| Age | ||||||||
|---|---|---|---|---|---|---|---|---|
| Variables | <28 Year | ≥28 Year | Mann–Whitney U | |||||
| Mean | SD | n | Mean | SD | n | U | p-Value | |
| MTA (mm) | −0.19 | 0.19 | 9 | −0.37 | 0.43 | 6 | 18.000 | 0.289 |
| MTL (mm) | −0.70 | 0.37 | 9 | −0.98 | 0.64 | 6 | 18.000 | 0.289 |
| VA (mm3) | 36.94 | 41.10 | 9 | 62.08 | 56.14 | 6 | 16.000 | 0.195 |
| Gender | ||||||||
|---|---|---|---|---|---|---|---|---|
| Variables | Female | Male | Mann–Whitney U | |||||
| Mean | SD | n | Mean | SD | n | U | p-Value | |
| MTA (mm) | −0.26 | 0.18 | 11 | −0.25 | 0.58 | 4 | 13.000 | 0.240 |
| MTL (mm) | −0.81 | 0.32 | 11 | −0.83 | 0.89 | 4 | 15.000 | 0.361 |
| VA (mm3) | 48.45 | 35.64 | 11 | 42.99 | 79.08 | 4 | 14.000 | 0.296 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marques, T.; Ramos, S.; Santos, N.B.M.d.; Borges, T.; Montero, J.; Correia, A.; Fernandes, G.V.d.O. A 3D Digital Analysis of the Hard Palate Wound Healing after Free Gingival Graft Harvest: A Pilot Study in the Short Term. Dent. J. 2022, 10, 109. https://doi.org/10.3390/dj10060109
Marques T, Ramos S, Santos NBMd, Borges T, Montero J, Correia A, Fernandes GVdO. A 3D Digital Analysis of the Hard Palate Wound Healing after Free Gingival Graft Harvest: A Pilot Study in the Short Term. Dentistry Journal. 2022; 10(6):109. https://doi.org/10.3390/dj10060109
Chicago/Turabian StyleMarques, Tiago, Sara Ramos, Nuno Bernardo Malta dos Santos, Tiago Borges, Javier Montero, André Correia, and Gustavo Vicentis de Oliveira Fernandes. 2022. "A 3D Digital Analysis of the Hard Palate Wound Healing after Free Gingival Graft Harvest: A Pilot Study in the Short Term" Dentistry Journal 10, no. 6: 109. https://doi.org/10.3390/dj10060109
APA StyleMarques, T., Ramos, S., Santos, N. B. M. d., Borges, T., Montero, J., Correia, A., & Fernandes, G. V. d. O. (2022). A 3D Digital Analysis of the Hard Palate Wound Healing after Free Gingival Graft Harvest: A Pilot Study in the Short Term. Dentistry Journal, 10(6), 109. https://doi.org/10.3390/dj10060109