


Smoking Cessation on Periodontal and Peri-Implant Health Status: A Systematic Review

 ,
,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Protocol
2.2. Search Strategy
2.3. Study Selection
2.4. Data Collection and Synthesis
2.5. Quality Assessment
3. Results
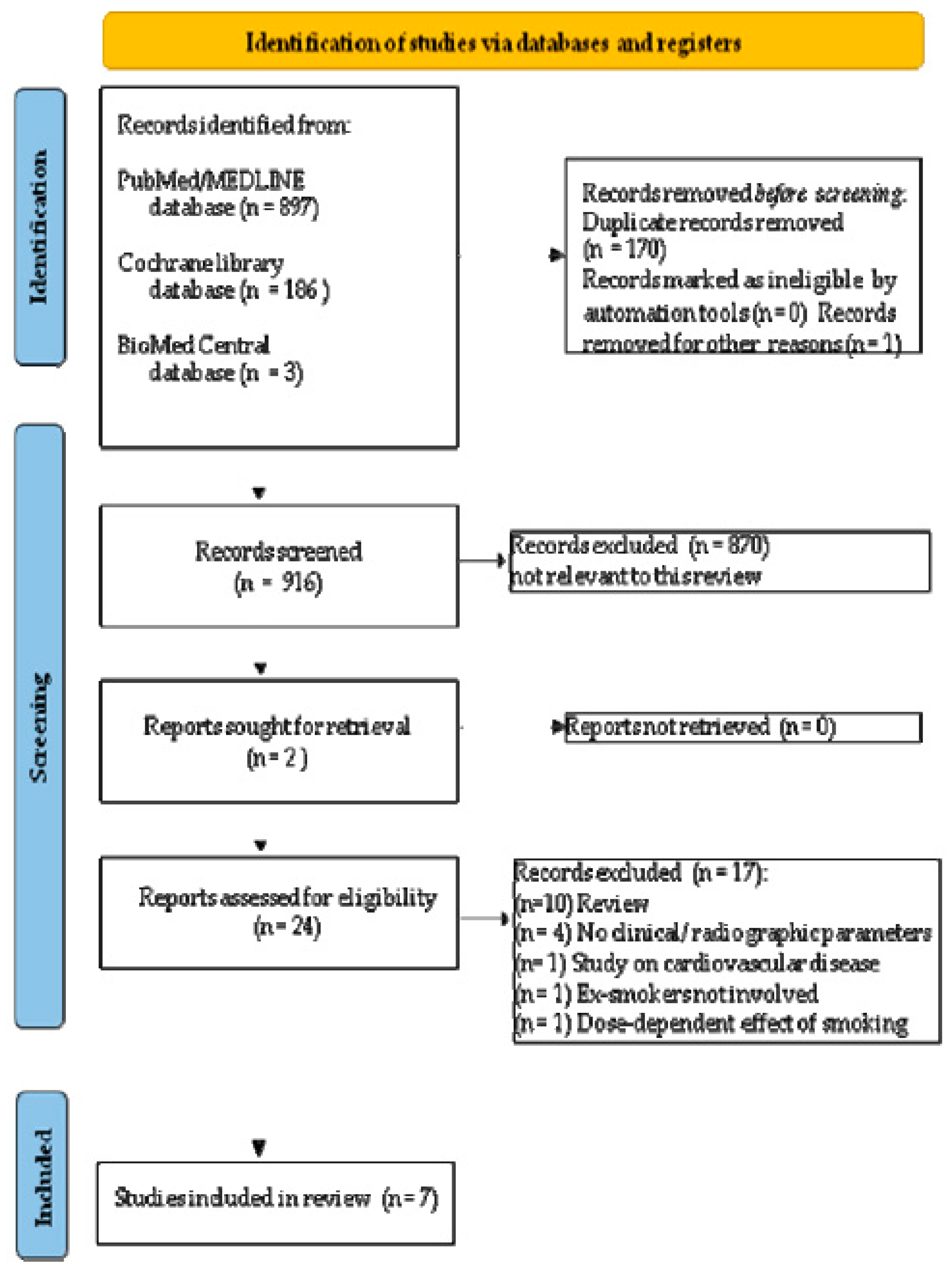
3.1. Study Selection
3.2. Study Characteristics and Descriptive Data Analysis
3.3. Quality Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nicolò, M.; Pirozzi, M.; Catalano, C.; Amato, M. Parodontiti associate a malattie sistemiche con deficit qualitativo della funzione fagocitaria. Nota I. Diabetemellito [Periodontitis associated with systemic diseases with qualitative deficiency of phagocyte function. I. Diabetes mellitus]. Minerva Stomatol. 1989, 38, 899–903. [Google Scholar]
- Nicolò, M.; Bucci, P.; Mignogna, M.D.; Amato, M. Parodontiti associate a malattie sistemiche con deficit qualitativo della funzione fagocitaria. Nota II. Sindrome di Down [Periodontitis associated with systemic diseases with qualitative deficiency of phagocyte function. II. Down’s syndrome]. Minerva Stomatol. 1989, 38, 905–909. [Google Scholar] [PubMed]
- Nicolò, M.; Amato, M.; Galizia, G.F. Parodontiti associate a malattie sistemiche con deficit qualitativo della funzione fagocitaria. Nota III. Sindrome di Papillon-Lefèvre [Periodontitis associated with systemic diseases with qualitative deficiency of phagocyte function. III. Papillon-Lefevre syndrome]. Minerva Stomatol. 1989, 38, 911–915. [Google Scholar] [PubMed]
- Di Spirito, F.; Iacono, V.J.; Iandolo, A.; Amato, A.; Sbordone, L. Evidence-based Recommendations on Periodontal Practice and the Management of Periodontal Patients during and after the COVID-19 Era: Challenging Infectious Diseases Spread by Air-borne Transmission. Open Dent. J. 2021, 15, 325–336. [Google Scholar] [CrossRef]
- Orsini, M.; Orsini, G.; Benlloch, D.; Aranda, J.J.; Sanz, M. Long-term clinical results on the use of bone-replacement grafts in the treatment of intrabony periodontal defects. Comparison of the use of autogenous bone graft plus calcium sulfate to autogenous bone graft covered with a bioabsorbable membrane. J. Periodontol. 2008, 79, 1630–1637. [Google Scholar] [CrossRef] [PubMed]
- Sbordone, C.; Toti, P.; Brevi, B.; Martuscelli, R.; Sbordone, L.; Di Spirito, F. Computed tomography-aided descriptive analysis of maxillary and mandibular atrophies. J. Stomatol. Oral Maxillofac. Surg. 2018, 120, 99–105. [Google Scholar] [CrossRef]
- Mattioli-Belmonte, M.; Teti, G.; Salvatore, V.; Focaroli, S.; Orciani, M.; Dicarlo, M.; Fini, M.; Orsini, G.; Di Primio, R.; Falconi, M. Stem cell origin differently affects bone tissue engineering strategies. Front. Physiol. 2015, 6, 266. [Google Scholar] [CrossRef]
- Di Spirito, F.; Toti, P.; Brevi, B.; Martuscelli, R.; Sbordone, L.; Sbordone, C. Computed tomography evaluation of jaw atrophies before and after surgical bone augmentation. Int. J. Clin. Dent. 2019, 12, 259–270. [Google Scholar]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Periodontol. 2018, 89, 159–172. [Google Scholar] [CrossRef]
- Contaldo, M.; Lucchese, A.; Romano, A.; Della Vella, F.; Di Stasio, D.; Serpico, R.; Petruzzi, M. Oral Microbiota Features in Subjects with Down Syndrome and Periodontal Diseases: A Systematic Review. Int. J. Mol. Sci. 2021, 22, 9251. [Google Scholar] [CrossRef]
- Folliero, V.; Dell’Annunziata, F.; Roscetto, E.; Amato, A.; Gasparro, R.; Zannella, C.; Casolaro, V.; De Filippis, A.; Catania, M.R.; Franci, G.; et al. Rhein: A novel antibacterial compound against Streptococcus mutans infection. Microbiol. Res. 2022, 261, 127062. [Google Scholar] [CrossRef] [PubMed]
- Contaldo, M.; Lucchese, A.; Lajolo, C.; Rupe, C.; Di Stasio, D.; Romano, A.; Petruzzi, M.; Serpico, R. The Oral Microbiota Changes in Orthodontic Patients and Effects on Oral Health: An Overview. J. Clin. Med. 2021, 10, 780. [Google Scholar] [CrossRef] [PubMed]
- Nastri, L.; Nucci, L.; Carozza, D.; Martina, S.; Serino, I.; Perillo, L.; d’Apuzzo, F.; Grassia, V. Gingival Recessions and Periodontal Status after Minimum 2-Year-Retention Post-Non-Extraction Orthodontic Treatment. Appl. Sci. 2022, 12, 1641. [Google Scholar] [CrossRef]
- Di Spirito, F.; Sbordone, L.; Pilone, V.; D’Ambrosio, F. Obesity and Periodontal Disease: A Narrative Review on Current Evidence and Putative Molecular Links. Open Dent. J. 2019, 13, 526–536. [Google Scholar] [CrossRef]
- Contaldo, M.; Fusco, A.; Stiuso, P.; Lama, S.; Gravina, A.G.; Itro, A.; Federico, A.; Itro, A.; Dipalma, G.; Inchingolo, F.; et al. Oral Microbiota and Salivary Levels of Oral Pathogens in Gastro-Intestinal Diseases: Current Knowledge and Exploratory Study. Microorganisms 2021, 9, 1064. [Google Scholar] [CrossRef] [PubMed]
- Di Spirito, F.; La Rocca, M.; De Bernardo, M.; Rosa, N.; Sbordone, C.; Sbordone, L. Possible Association of Periodontal Disease and Macular Degeneration: A Case-Control Study. Dent. J. 2020, 9, 1. [Google Scholar] [CrossRef] [PubMed]
- Chapple, I.L.C.; Genco, R. On behalf of working group 2 of the joint EFP/AAP workshop. Diabetes and periodontal diseases: Consensus report of the Joint EFP/AAPWorkshop on Periodontitis and Systemic Diseases. J. Periodontol. 2013, 84, 106–112. [Google Scholar] [CrossRef]
- Contaldo, M.; Itro, A.; Lajolo, C.; Gioco, G.; Inchingolo, F.; Serpico, R. Overview on Osteoporosis, Periodontitis and Oral Dysbiosis: The Emerging Role of Oral Microbiota. Appl. Sci. 2020, 10, 6000. [Google Scholar] [CrossRef]
- Di Spirito, F.; Toti, P.; Pilone, V.; Carinci, F.; Lauritano, D.; Sbordone, L. The Association between Periodontitis and Human Colorectal Cancer: Genetic and Pathogenic Linkage. Life 2020, 10, 211. [Google Scholar] [CrossRef]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Periimplant Diseases and Conditions. J. Clin. Periodontol. 2018, 45, S173–S182. [Google Scholar] [CrossRef]
- Genco, R.J.; Borgnakke, W.S. Risk factors for periodontal disease. Periodontology 2000 2013, 62, 59–94. [Google Scholar] [CrossRef]
- D’Ambrosio, F.; Caggiano, M.; Schiavo, L.; Savarese, G.; Carpinelli, L.; Amato, A.; Iandolo, A. Chronic Stress and Depression in Periodontitis and Periimplantitis: A Narrative Review on Neurobiological, Neurobehavioral and Immune–Microbiome Interplays and Clinical Management Implications. Dent. J. 2022, 10, 49. [Google Scholar] [CrossRef]
- Checchi, V.; Gasparro, R.; Pistilli, R.; Canullo, L.; Felice, P. Clinical Classification of Bone Augmentation Procedure Failures in the Atrophic Anterior Maxillae: Esthetic Consequences and Treatment Options. BioMed Res. Int. 2019, 2019, 4386709. [Google Scholar] [CrossRef]
- Marenzi, G.; Spagnuolo, G.; Sammartino, J.C.; Gasparro, R.; Rebaudi, A.; Salerno, M. Micro-Scale Surface Patterning of Titanium Dental Implants by Anodization in the Presence of Modifying Salts. Materials 2019, 12, 1753. [Google Scholar] [CrossRef] [PubMed]
- Bruno, V.; Berti, C.; Barausse, C.; Badino, M.; Gasparro, R.; Ippolito, D.R.; Felice, P. Clinical Relevance of Bone Density Values from CT Related to Dental Implant Stability: A Retrospective Study. BioMed Res. Int. 2018, 2018, 6758245. [Google Scholar] [CrossRef] [PubMed]
- Pisano, M.; Amato, A.; Sammartino, P.; Iandolo, A.; Martina, S.; Caggiano, M. Laser Therapy in the Treatment of Periimplantitis: State-of-the-Art, Literature Review and Meta-Analysis. Appl. Sci. 2021, 11, 5290. [Google Scholar] [CrossRef]
- Felice, P.; Bertacci, A.; Bonifazi, L.; Karaban, M.; Canullo, L.; Pistilli, R.; Sammartino, P.; Gasparro, R.; Barausse, C. A Proposed Protocol for Ordinary and Extraordinary Hygienic Maintenance in Different Implant Prosthetic Scenarios. Appl. Sci. 2021, 11, 2957. [Google Scholar] [CrossRef]
- Ramaglia, L.; Di Spirito, F.; Sirignano, M.; La Rocca, M.; Esposito, U.; Sbordone, L. A 5-year longitudinal cohort study on crown to implant ratio effect on marginal bone level in single implants. Clin. Implant Dent. Relat. Res. 2019, 21, 916–922. [Google Scholar] [CrossRef]
- Caggiano, M.; Amato, A.; Acerra, A.; D’Ambrosio, F.; Martina, S. Evaluation of Deviations between Computer-Planned Implant Position and In Vivo Placement through 3D-Printed Guide: A CBCT Scan Analysis on Implant Inserted in Esthetic Area. Appl. Sci. 2022, 12, 5461. [Google Scholar] [CrossRef]
- Di Spirito, F.; Schiavo, L.; Pilone, V.; Lanza, A.; Sbordone, L.; D’Ambrosio, F. Periodontal and Periimplant Diseases and Systemically Administered Statins: A Systematic Review. Dent. J. 2021, 9, 100. [Google Scholar] [CrossRef]
- Duarte, P.M.; Nogueira, C.; Silva, S.M.; Pannuti, C.M.; Schey, K.C.; Miranda, T.S. Impact of Smoking Cessation on Periodontal Tissues. Int. Dent. J. 2022, 72, 31–36. [Google Scholar] [CrossRef] [PubMed]
- D’Ambrosio, F.; Pisano, M.; Amato, A.; Iandolo, A.; Caggiano, M.; Martina, S. Periodontal and Periimplant Health Status in Traditional vs. Heat-Not-Burn Tobacco and Electronic Cigarettes Smokers: A Systematic Review. Dent. J. 2022, 10, 103. [Google Scholar] [CrossRef] [PubMed]
- Di Spirito, F.; Pelella, S.; Argentino, S.; Sisalli, L.; Sbordone, L. Oral manifestations and the role of the oral healthcare workers in COVID-19. Oral Dis. 2022, 28, 1003–1004. [Google Scholar] [CrossRef]
- Japuntich, S.J.; Leventhal, A.M.; Piper, M.E.; Bolt, D.M.; Roberts, L.J.; Fiore, M.C.; Baker, T.B. Smoker characteristics and smoking-cessation milestones. Am. J. Prev. Med. 2011, 40, 286–294. [Google Scholar] [CrossRef] [PubMed]
- Di Spirito, F.; Iandolo, A.; Amato, A.; Caggiano, M.; Raimondo, A.; Lembo, S.; Martina, S. Prevalence, Features and Degree of Association of Oral Lesions in COVID-19: A Systematic Review of Systematic Reviews. Int. J. Environ. Res. Public Health 2022, 19, 7486. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Da Costa Santos, C.M.; Pimenta, C.A.M.; Nobre, M.R.C. The PICO strategy for the research question construction and evidence search. Revis. Lat.-Am. Enferm. 2007, 15, 508–511. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2008. [Google Scholar]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Henry, D.A. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef]
- Leite, F.; Nascimento, G.G.; Baake, S.; Pedersen, L.D.; Scheutz, F.; López, R. Impact of Smoking Cessation on Periodontitis: A Systematic Review and Meta-analysis of Prospective Longitudinal Observational and Interventional Studies. Nicotine Tob. Res. Off. J. Soc. Res. Nicotine Tob. 2019, 21, 1600–1608. [Google Scholar] [CrossRef]
- Souto, M.; Rovai, E.S.; Villar, C.C.; Braga, M.M.; Pannuti, C.M. Effect of smoking cessation on tooth loss: A systematic review with meta-analysis. BMC Oral Health 2019, 19, 245. [Google Scholar] [CrossRef] [PubMed]
- Ramseier, C.A.; Woelber, J.P.; Kitzmann, J.; Detzen, L.; Carra, M.C.; Bouchard, P. Impact of risk factor control interventions for smoking cessation and promotion of healthy lifestyles in patients with periodontitis: A systematic review. J. Clin. Periodontol. 2020, 47 (Suppl. S22), 90–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gugnani, N.; Gugnani, S. Can smoking cessation impact the incidence and progression of periodontitis? Evid.-Based Dent. 2020, 21, 122–123. [Google Scholar] [CrossRef] [PubMed]
- Al-Ansari, A. Smoking cessation is effective in reducing the risk of tooth loss. Evid.-Based Dent. 2020, 21, 120–121. [Google Scholar] [CrossRef]
- Chambrone, L.; Chambrone, D.; Lima, L.A.; Chambrone, L.A. Predictors of tooth loss during long-term periodontal maintenance: A systematic review of observational studies. J. Clin. Periodontol. 2010, 37, 675–684. [Google Scholar] [CrossRef]
- Chambrone, L.; Preshaw, P.M.; Rosa, E.F.; Heasman, P.A.; Romito, G.A.; Pannuti, C.M.; Tu, Y.K. Effects of smoking cessation on the outcomes of non-surgical periodontal therapy: A systematic review and individual patient data meta-analysis. J. Clin. Periodontol. 2013, 40, 607–615. [Google Scholar] [CrossRef]
- Fiorini, T.; Musskopf, M.L.; Oppermann, R.V.; Susin, C. Is there a positive effect of smoking cessation on periodontal health? A systematic review. J. Periodontol. 2014, 85, 83–91. [Google Scholar] [CrossRef]
- Holliday, R.; Hong, B.; McColl, E.; Livingstone-Banks, J.; Preshaw, P.M. Interventions for tobacco cessation delivered by dental professionals. Cochrane Database Syst. Rev. 2021, 2, CD005084. [Google Scholar] [CrossRef]
- Alexandridi, F.; Tsantila, S.; Pepelassi, E. Smoking cessation and response to periodontal treatment. Aust. Dent. J. 2018, 63, 140–149. [Google Scholar] [CrossRef]
- Preshaw, P.M.; Heasman, L.; Stacey, F.; Steen, N.; McCracken, G.I.; Heasman, P.A. The effect of quitting smoking on chronic periodontitis. J. Clin. Periodontol. 2005, 32, 869–879. [Google Scholar] [CrossRef]
- Shimazaki, Y.; Saito, T.; Kiyohara, Y.; Kato, I.; Kubo, M.; Iida, M.; Yamashita, Y. The influence of current and former smoking on gingival bleeding: The Hisayama study. J. Periodontol. 2006, 77, 1430–1435. [Google Scholar] [CrossRef] [PubMed]
- Peruzzo, D.C.; Gimenes, J.H.; Taiete, T.; Casarin, R.C.; Feres, M.; Sallum, E.A.; Casati, M.Z.; Kantovitz, K.R.; Nociti, F.H. Impact of smoking on experimental gingivitis. A clinical, microbiological and immunological prospective study. J. Periodontal Res. 2016, 51, 800–811. [Google Scholar] [CrossRef] [PubMed]
- Nemmar, A.; Al-Salam, S.; Beegam, S.; Zaaba, N.E.; Ali, B.H. Effect of smoking cessation on chronic waterpipe smoke inhalation-induced airway hyperresponsiveness, inflammation, and oxidative stress. Am. J. Physiol. Lung Cell. Mol. Physiol. 2021, 320, L791–L802. [Google Scholar] [CrossRef] [PubMed]
- More, A.B.; Rodrigues, A.; Sadhu, B.J. Effects of smoking on oral health: Awareness among dental patients and their attitude towards its cessation. Indian J. Dent. Res. Off. Publ. Indian Soc. Dent. Res. 2021, 32, 23–26. [Google Scholar] [CrossRef]
- Ravidà, A.; Troiano, G.; Qazi, M.; Saleh, M.; Saleh, I.; Borgnakke, W.S.; Wang, H.L. Dose-dependent effect of smoking and smoking cessation on periodontitis-related tooth loss during 10–47 years periodontal maintenance-A retrospective study in compliant cohort. J. Clin. Periodontol. 2020, 47, 1132–1143. [Google Scholar] [CrossRef]
- ALHarthi, S.; Natto, Z.S.; Midle, J.B.; Gyurko, R.; O’Neill, R.; Steffensen, B. Association between time since quitting smoking and periodontitis in former smokers in the National Health and Nutrition Examination Surveys (NHANES) 2009 to 2012. J. Periodontol. 2019, 90, 16–25. [Google Scholar] [CrossRef]
- Karaaslan, F.; Dikilitaş, A.; Yiğit, U. The effects of vaping electronic cigarettes on periodontitis. Aust. Dent. J. 2020, 65, 143–149. [Google Scholar] [CrossRef]
- Jeong, W.; Choi, D.W.; Kim, Y.K.; Lee, H.J.; Lee, S.A.; Park, E.C.; Jang, S.I. Associations of electronic and conventional cigarette use with periodontal disease in South Korean adults. J. Periodontol. 2020, 91, 55–64. [Google Scholar] [CrossRef]
- Costa, F.O.; Cota, L.O.; Lages, E.J.; Cyrino, R.M.; Oliveira, A.M.; Oliveira, P.A.; Cortelli, J.R. Associations of duration of smoking cessation and cumulative smoking exposure with periodontitis. J. Oral Sci. 2013, 55, 245–253. [Google Scholar] [CrossRef]
- Costa, F.O.; Cota, L. Cumulative smoking exposure and cessation associated with the recurrence of periodontitis in periodontal maintenance therapy: A 6-year follow-up. J. Periodontol. 2019, 90, 856–865. [Google Scholar] [CrossRef]
- Dietrich, T.; Walter, C.; Oluwagbemigun, K.; Bergmann, M.; Pischon, T.; Pischon, N.; Boeing, H. Smoking, Smoking Cessation, and Risk of Tooth Loss: The EPIC-Potsdam Study. J. Dent. Res. 2015, 94, 1369–1375. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.H.; Hwang, S.J. Effect of smoking cessation for 1 year on periodontal biomarkers in gingival crevicular fluid. J. Periodontal Res. 2016, 51, 366–375. [Google Scholar] [CrossRef] [PubMed]
- Beklen, A.; Yildirim, B.G.; Mimaroglu, M.; Yavuz, M.B. The impact of smoking on oral health and patient assessment of tobacco cessation support from Turkish dentists. Tob. Induc. Dis. 2021, 19, 49. [Google Scholar] [CrossRef]
- Valente, N.A.; Andreana, S. Peri-implant disease: What we know and what we need to know. J. Periodontal Implant Sci. 2016, 46, 136–151. [Google Scholar] [CrossRef] [PubMed]
- Helal, O.; Gostemeyer, G.; Krois, J.; Fawzy, E.S.; Sayed, K.; Graetz, C.; Schwendicke, F. Predictors for tooth loss in periodontitis patients: Systematic review and meta-analysis. J. Clin. Periodontol. 2019, 46, 699–712. [Google Scholar] [CrossRef]
- Koldsland, O.C.; Scheie, A.A.; Aass, A.M. The association between selected risk indicators and severity of peri-implantitis using mixed model analyses. J. Clin. Periodontol. 2011, 38, 285–292. [Google Scholar] [CrossRef]
- Di Spirito, F. Oral-Systemic Health and Disorders: Latest Prospects on Oral Antisepsis. Appl. Sci. 2022, 12, 8185. [Google Scholar] [CrossRef]
- Roos-Jansåker, A.M.; Renvert, H.; Lindahl, C.; Renvert, S. Nine- to fourteen-year follow-up of implant treatment. Part III: Factors associated with peri-implant lesions. J. Clin. Periodontol. 2006, 33, 296–301. [Google Scholar] [CrossRef]
- Bergström, J. Tobacco smoking and chronic destructive periodontal disease. Odontology 2004, 92, 1–8. [Google Scholar] [CrossRef]
- Dietrich, T.; Bernimoulin, J.P.; Glynn, R.J. The effect of cigarette smoking on gingival bleeding. J. Periodontol. 2004, 75, 16–22. [Google Scholar] [CrossRef]
- Bašić, K.; Peroš, K.; Bošnjak, Z.; Šutej, I. Subgingival Microbiota Profile in Association with Cigarette Smoking in Young Adults: A Cross-Sectional Study. Dent. J. 2021, 9, 150. [Google Scholar] [CrossRef] [PubMed]
- Nociti, F.H.; Casati, M.Z.; Duarte, P.M. Current perspective of the impact of smoking on the progression and treatment of periodontitis. Periodontology 2000 2015, 67, 187–210. [Google Scholar] [CrossRef] [PubMed]
- Jha, P.; Peto, R. Global effects of smoking, of quitting, and of taxing tobacco. N. Engl. J. Med. 2014, 370, 60–68. [Google Scholar] [CrossRef]
- Chaffee, B.W.; Couch, E.T.; Vora, M.V.; Holliday, R.S. Oral and periodontal implications of tobacco and nicotine products. Periodontology 2000 2021, 87, 241–253. [Google Scholar] [CrossRef] [PubMed]
- Dhillon, A.Z.; Doran, T.; Aggarwal, V.R. Perceptions of Waterpipe Smoking among Young Adults: A Phenomenological Study. Dent. J. 2020, 8, 134. [Google Scholar] [CrossRef] [PubMed]
- Julkunen-Iivari, A.; Heikkinen, A.M.; Räisänen, I.T.; Ruokonen, H.; Meurman, J.H.; Toppila-Salmi, S.; Söder, P.-Ö.; Söder, B. Tobacco Products, Periodontal Health and Education Level: Cohort Study from Sweden. Dent. J. 2020, 8, 90. [Google Scholar] [CrossRef]
- Di Spirito, F.; Amato, A.; Di Palo, M.P.; Contaldo, M.; D’Ambrosio, F.; Lo Giudice, R.; Amato, M. Oral Lesions Following Anti-SARS-CoV-2 Vaccination: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 10228. [Google Scholar] [CrossRef]
- D’Ambrosio, F.; Di Spirito, F.; De Caro, F.; Lanza, A.; Passarella, D.; Sbordone, L. Adherence to Antibiotic Prescription of Dental Patients: The Other Side of the Antimicrobial Resistance. Healthcare 2022, 10, 1636. [Google Scholar] [CrossRef]
- Amato, A. Oral-Systemic Health and Disorders: Latest Advances on Oral–Gut–Lung Microbiome Axis. Appl. Sci. 2022, 12, 8213. [Google Scholar] [CrossRef]


{kind=link}
| Study | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Characteristics | ||
| Type | Clinical | Narrative reviews |
| Books and chapters | ||
| Conference papers | ||
| Oral communications | ||
| In vitro | ||
| Pre-clinical in vivo | ||
| Design | Cross-sectional | Case series |
| Case-control | Case reports | |
| Retrospective | ||
| Prospective | ||
| Randomized Clinical Trials (RCT) | ||
| Sample size | ≥50 | <50 |
| Population | Periodontal subjects | Periodontally healthy subjects |
| Age | ≥18 years old | <18 years old |
| Gender | No restrictions | No restrictions |
| Characteristics | Ex-smokers | Smokers |
| Non-smokers | ||
| Pregnancy; lactation | ||
| Comorbidities | Any | Neoplastic disease |
| Medication-related osteonecrosis of the jaws | ||
| Systemic disease affecting bone metabolism or periodontal/peri-implant disease | ||
| Non-surgical/surgical periodontal treatment (within <3 months) | ||
| Radiations (head and neck) | ||
| Antibiotics, corticosteroids (within 3 months) | ||
| Drugs affecting bone metabolism | ||
| Treatments | Non-surgical/surgical periodontal treatment (within ≥3 months) | |
| Intervention | Smoking cessation (ex-smokers) | No discontinuing tobacco smoking |
| Comparison | No smoking cessation (current smokers) | |
| No smoking habit (non-smokers) | ||
| Outcome(s) | Periodontal and peri-implant status | Endodontic-periodontal lesions |
| Endodontic lesions | ||
| Failure of osseointegration | ||
| Clinical Attachment Level (CAL) | ||
| Clinical periodontal parameters | Periodontal Probing Depth (PPD) | |
| Plaque Index (PI) | ||
| Gingival Index (GI) | ||
| Bleeding on Probing (BOP) | ||
| Tooth loss; implant loss | ||
| Radiographic periodontal parameters | ||
| Radiographic bone loss around natural teeth (RBL) | ||
| Marginal bone loss around dental implants (MBL) | ||
| Other periodontal parameters | Gingival crevicular (GC) inflammatory mediators |
| Included Studies | Methods | Periodontal Parameters Around Natural Teeth Statistically Significant (p < 0.05) | Conclusion(s) |
|---|---|---|---|
| Author Year [Reference] Journal Study design | Population | Clinical | |
| Participants (n.) | Clinical Attachment Level (CAL) | ||
| Age (y.o.) | |||
| Male/female (M/F) | Periodontal Probing Depth (PPD) | ||
| Periodontal status | |||
| Comorbidities | Bleeding on Probing (BOP) | ||
| Smoking habit duration (years) | |||
| Smoking habit characteristics: traditional tobacco; | Gingival Index (GI) | ||
| Heat-Not-Burn tobacco; electronic nicotine delivery systems (E-cigs); | Plaque Index (PI) | ||
| Cigarettes or equivalent n./day | |||
| Intervention | Tooth loss | ||
| Smoking cessation (duration) | Implant loss | ||
| (ex-smokers) | |||
| Comparison | Radiographic | ||
| Ongoing smoking habit (smokers) | Radiographic bone loss (RGB) | ||
| No smoking habit (non-smokers) | |||
| Procedure(s) | Gingival crevicular (GC) inflammatory mediators | ||
| Non-surgical periodontal treatment | Any | ||
| Surgical periodontal treatment | |||
| Karaslaan et al., 2020 [58] Aust. Dent. J. Case-control study | Study participants (n.57) | Clinical | GI was significantly higher among E-cigs smokers and ex-smokers compared to tobacco smokers GI was significantly lower among E-cigs smokers compared to ex-smokers |
| Age (35.19 +/− 2.23) | CAL | ||
| Male/female (39/18) | GI | ||
| Periodontal subjects | PI | ||
| Comorbidities: MD | |||
| Radiographic | |||
| Smoking habit duration: MD | MD | ||
| Smoking habit characteristics: tobacco smokers (13.95 +/−3.01 years) | |||
| E-cigs smokers (2.32 +/− 0.75 years) | GC Inflammatory mediators | ||
| Interleukin-8 | |||
| Intervention | Tumor Necrosis Factor-alfa | ||
| Smoking cessation (duration MD) | Glutathione peroxidase | ||
| 8-hydroxydeoxyguanosine | |||
| Comparison | |||
| |||
| |||
| |||
| Procedure(s) | |||
| Non-surgical periodontal treatment | |||
| Jeong et al., 2020 [59] J. Periodont. Case-control study | Study participants (n.13551) | Clinical | Periodontitis rate was significantly higher in tobacco smokers and E-cigs smokers compared to ex-smokers and smokers |
| Age (divided into range of 10 years) | CPI divided into 0–4 points | ||
| Male/female (5715/7836) | 0 for healthy periodontal tissue | ||
| Periodontal status: MD | 1 (bleeding periodontal tissue) | ||
| Comorbidities: MD | 2 (gingival biofilm) | ||
| 3 (3.5 ≤ pocket depth < 5.5 mm) | |||
| Smoking habit duration: MD | 4 (pocket depth ≥ 5.5 mm). | ||
| Smoking habit characteristics: Tobacco smokers | A score of 3–4 denotes periodontal disease | ||
| E-cigs smokers | |||
| Radiographic | |||
| Intervention | MD | ||
| Evaluation of periodontal diseases among the group | |||
| GC Inflammatory mediators | |||
| Comparison | MD | ||
| |||
| |||
| |||
| |||
| Procedure(s) | |||
| Non-surgical periodontal treatment | |||
| Costa et al., 2013 [60] J. Oral Sci. Cross-sectional study | Study participants (n.705) | Clinical | Cumulative smoking exposure and duration of smoking cessation were significantly associated with periodontitis |
| Age (35–65 y.o.) | CAL | ||
| Male/female (341/364) | PI | ||
| Periodontal status: MD | BOP | ||
| Comorbidities: MD | PPD | ||
| Smoking habit duration: | Radiographic | ||
| in ex-smokers (28.6 +/− 12.7 years) and in smokers (35.5 + 7 − 14.8 years) | MD | ||
| Smoking habit characteristics: non-smokers | |||
| tobacco smokers | GC inflammatory mediators | ||
| ex-smokers | MD | ||
| Intervention | |||
| Smoking cessation (duration MD) | |||
| Comparison | |||
| |||
| |||
| |||
| Costa et al. 2019 [61] J. Periodont. Cohort study | Study participants (n.142) | Clinical | Smoking negatively affects periodontitis and, in particular, smoking cessation positively affects periodontitis |
| Age (MD) | CAL | ||
| Male/female (MD) | BOP | ||
| Periodontal status: MD | PPD | ||
| Comorbidities: diabetes | PI | ||
| Smoking habit duration: MD | Radiographic | ||
| Smoking habit characteristics: non-smokers | MD | ||
| tobacco smokers | |||
| ex-smokers | GC inflammatory mediators | ||
| MD | |||
| Intervention | |||
| Smoking cessation (6 years) | |||
| Comparison | |||
| |||
| |||
| |||
| Dietrich et al. 2015 [62] J. Dent. Res. Prospective cohort study | Study participants (n.23376) | Clinical | Smoking habit had a stronger association with tooth loss in M > F and in younger > older subjects Smoking cessation was associated with a reduction in tooth loss risk in approximately 20 years |
| Age (non-smokers, 50.3 ± 8.8; ex-smokers, 50.5 ± 9.0; smokers, 47.2 ± 8.7) | Tooth loss | ||
| Male/female (9032/14,344) | |||
| Periodontal status: MD | Radiographic | ||
| Comorbidities: diabetes and hypertension | MD | ||
| Smoking habit duration: MD | GC Inflammatory mediators | ||
| Smoking habit characteristics: non-smokers | MD | ||
| tobacco smokers | |||
| ex-smokers | |||
| Intervention | |||
| Smoking cessation (duration MD) | |||
| Comparison | |||
| |||
| |||
| |||
| Liu et al., 2015 [63] J. Perio. Res. Prospective study | Study participants (n.122) | Clinical | No significant differences in GC Matrix Metalloproteasis-8 and Matrix Metalloproteasis-9 were detected between smokers, ex-smokers (for 1 year), and non-smokers This 1-year prospective smoking cessation study shows GC Interleukin-1b could have a positive relationship with nicotine and cotinine levels in saliva |
| Age (MD) | GI | ||
| Male/female (122/0) | PI | ||
| Periodontal status: MD | |||
| Comorbidities: MD | Radiographic | ||
| MD | |||
| Smoking habit duration: MD | |||
| Smoking habit characteristics: n.13 non-smokers | GC inflammatory mediators | ||
| n.11 ex-smokers | Matrix Metalloproteasis-8 | ||
| n.9 smokers | Matrix Metalloproteasis-9 | ||
| n.6 oscillators | Interleukin-1b | ||
| Cotinine | |||
| Intervention | Nicotine | ||
| Smoking cessation (1 year) | |||
| Comparison | |||
| |||
| |||
| |||
| |||
| Beklen et al., 2021 [64] TobInduc. Dis. Cross-sectional study | Study participants (n.226) | Clinical | Higher PI was found in smokers (2.78 ± 0.92) compared to non-smokers (1.0 ± 0.6) and ex-smokers (1.1 ± 0.8) PD values were significantly (p < 0.05) higher in smokers (5.6 ± 1.9) compared to non-smokers (1.6 ± 0.8) and ex-smokers (2.4 ± 1.3) |
| Age (>18 years) | PI | ||
| Male/female (90/136) | GI | ||
| Periodontal status: MD | PD | ||
| Comorbidities: MD | |||
| Radiographic | |||
| Smoking habit duration: MD | MD | ||
| Smoking habit characteristics: non-smokers | |||
| tobacco smokers | GC Inflammatory mediators | ||
| ex-smokers | MD | ||
| Intervention | |||
| Smoking cessation (duration MD) | |||
| Comparison | |||
| |||
| |||
|
| Periodontal Parameter | Main Result(s) | Author, Year |
|---|---|---|
| CAL | Mean CAL values and the percentage of sites with a CAL value ≥ 5 mm and tooth loss were lower in ex-smokers and non-smokers compared to smokers; | Costa et al., 2013 [60] |
| Mean CAL values and the percentage of sites with a CAL value ≥ 5 mm and tooth loss were lower in ex-smokers and non-smokers compared to smokers; | Costa et al., 2019 [61] | |
| Mean CAL values were not significantly different among ex-smokers, smokers, and non-smokers. | Karaaslan et al., 2020 [58] | |
| PI | Mean PI values were lower in ex-smokers and non-smokers compared to smokers; | Costa et al., 2013 [60] |
| Mean PI values were not significantly different among ex-smokers, smokers, and non-smokers; | Liu et al., 2015 [63] | |
| Mean PI values were not significantly different among ex-smokers, smokers, and non-smokers; | Karaaslan et al., 2020 [58] | |
| Mean PI values were lower in ex-smokers (1.1 ± 0.8) and non-smokers (1.0 ± 0.6) compared to smokers (2.78 ± 0.92); | Beklen et al., 2021 [64] | |
| Mean PI values were lower in ex-smokers and non-smokers compared to smokers (PI values for smokers > ex-smokers > non-smokers). | Costa et al., 2019 [61] | |
| BOP | The mean number of sites with BOP was significantly lower in smokers compared to ex-smokers and non-smokers; | Costa et al., 2013 [60] |
| The mean number of sites with BOP was significantly lower in smokers compared to ex-smokers and non-smokers. | Costa et al., 2019 [61] | |
| PD | Mean PD values were not significantly different among ex-smokers, smokers, and non-smokers; | Karaaslan et al., 2020 [58] |
| Mean PD values and he percentage of sites with a PD ≥ 5 mm were lower in ex-smokers and non-smokers compared to smokers; | Costa et al., 2013 [60] | |
| Mean PD values and the percentage of sites with a PD ≥ 5 mm were lower in ex-smokers (2.4 ± 1.3) and non-smokers (1.6 ± 0.8) compared to smokers (5.6 ± 1.9); | Beklen et al., 2021 [64] | |
| Mean PD values were not significantly different among ex-smokers, smokers, and non-smokers. | Liu et al., 2015 [63] | |
| GI | Mean GI values were not significantly different among ex-smokers, smokers, and non-smokers at baseline; | Liu et al., 2015 [63] |
| GI values were lower in ex-smokers (1.9 ± 1.0) and non-smokers (0.5 ± 0.4) compared to smokers (2.5 ± 0.5); | Beklen et al., 2021 [64] | |
| GI values were significantly higher in ex-smokers and electronic cigarette smokers compared to smokers and were significantly lower in electronic cigarette smokers compared to ex-smokers. | Karaaslan et al., 2020 [58] | |
| Tooth loss | Tooth loss was lower in ex-smokers and non-smokers compared to smokers; | Costa et al., 2019 [61] |
| Tooth loss was significantly higher in ex-smokers and smokers compared to non-smokers; | Costa et al., 2013 [60] | |
| A negative dose-dependent association between cigarette smoking, smoking cessation, and number of natural teeth was found at baseline. | Dietrich et al., 2015 [62] | |
| Tumor Necrosis Factor-alfa (TNF-a) | GC TNF-a levels were significantly higher in smokers (4.20 +/− 0.14) compared to electronic cigarette smokers; no data concerning ex-smokers. | Karaaslan et al., 2020 [58] |
| Interleukin-1b (IL-1b) | GC IL-1b was significantly lower (p = 0.007) in ex-smokers, non-smokers, and oscillators compared to smokers at 2-month follow-up. | Liu et al., 2015 [63] |
| Interleukin-8 (IL-8) | GC IL-8 levels were significantly higher in ex-smokers (70.47 +/− 2.76) and electronic cigarette smokers compared to smokers. | Karaaslan et al., 2020 [58] |
| CPI | Periodontal disease was more prevalent in electronic cigarette smokers and tobacco smokers compared to non-smokers; no data concerning ex-smokers. | Jeong et al., 2020 [59] |
| Matrix metalloproteasis-8 and -9 (MMP-8 -9) | GC MMP-8 and MMP-9 were not significantly different between smokers and ex-smokers (for 1 year). | Liu et al., 2015 [63] |
| Glutathione peroxidase | GC glutathione peroxidase levels were significantly higher in ex-smokers compared to tobacco smokers, electronic cigarette smokers, and ex-smokers. | Karaaslan et al., 2020 [58] |
| Studies | Bias Due to Confounding | Bias in Selection of Participants | Bias in Measurement Classification of Interventions | Bias Due to Deviations from Intended Interventions | Bias Due to Missing Data | Bias in Measurement of Outcomes | Bias Due to Selection of the Reported Result |
|---|---|---|---|---|---|---|---|
| Costa et al., 2013 [60] | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Costa et al., 2019 [61] | Probably yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Karaaslan et al., 2020 [58] | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Liu et al., 2015 [63] | Probably no | Yes | Yes | Yes | Yes | Yes | Yes |
| Dietrich et al., 2015 [62] | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Beklen et al., 2021 [64] | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Jeong et al., 2020 [59] | Probably no | Yes | Yes | Yes | Yes | Probably yes | Yes |
| Risk of bias judgements | Serious | Low | Low | Low | Low | Moderate | Low |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caggiano, M.; Gasparro, R.; D’Ambrosio, F.; Pisano, M.; Di Palo, M.P.; Contaldo, M. Smoking Cessation on Periodontal and Peri-Implant Health Status: A Systematic Review. Dent. J. 2022, 10, 162. https://doi.org/10.3390/dj10090162
Caggiano M, Gasparro R, D’Ambrosio F, Pisano M, Di Palo MP, Contaldo M. Smoking Cessation on Periodontal and Peri-Implant Health Status: A Systematic Review. Dentistry Journal. 2022; 10(9):162. https://doi.org/10.3390/dj10090162
Chicago/Turabian StyleCaggiano, Mario, Roberta Gasparro, Francesco D’Ambrosio, Massimo Pisano, Maria Pia Di Palo, and Maria Contaldo. 2022. "Smoking Cessation on Periodontal and Peri-Implant Health Status: A Systematic Review" Dentistry Journal 10, no. 9: 162. https://doi.org/10.3390/dj10090162
APA StyleCaggiano, M., Gasparro, R., D’Ambrosio, F., Pisano, M., Di Palo, M. P., & Contaldo, M. (2022). Smoking Cessation on Periodontal and Peri-Implant Health Status: A Systematic Review. Dentistry Journal, 10(9), 162. https://doi.org/10.3390/dj10090162