



Mandibular Reconstruction after Resection of Ameloblastoma by Custom-Made CAD/CAM Mandibular Titanium Prosthesis: Two Case Reports, Finite Element Analysis and Discussion of the Technique
 ,
,  ,
,  ,
,  and
and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Reports
2.1. Patient #1
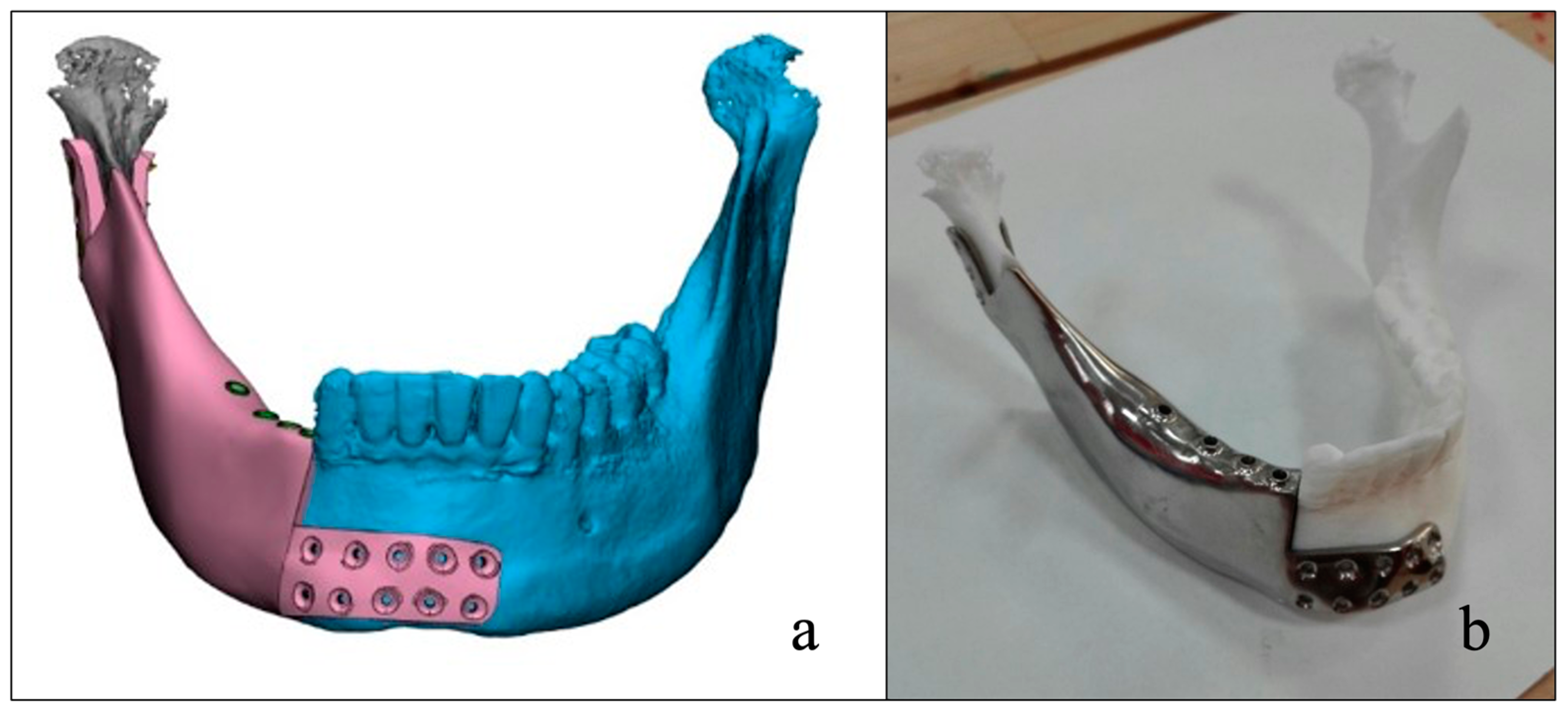
2.2. Design Case #1
2.3. Finite Element Analysis Case #1
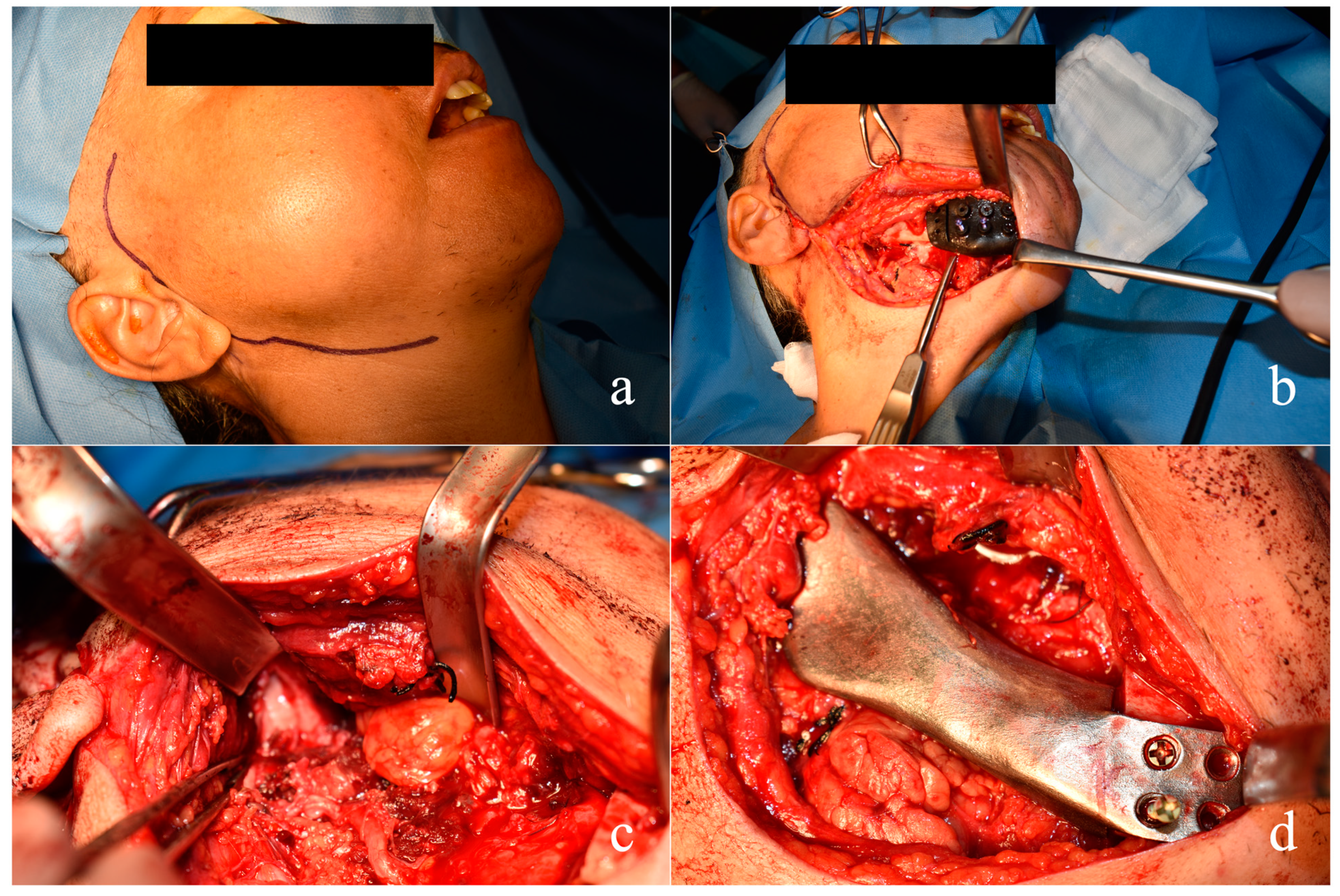
2.4. Surgical Sequence Case #1
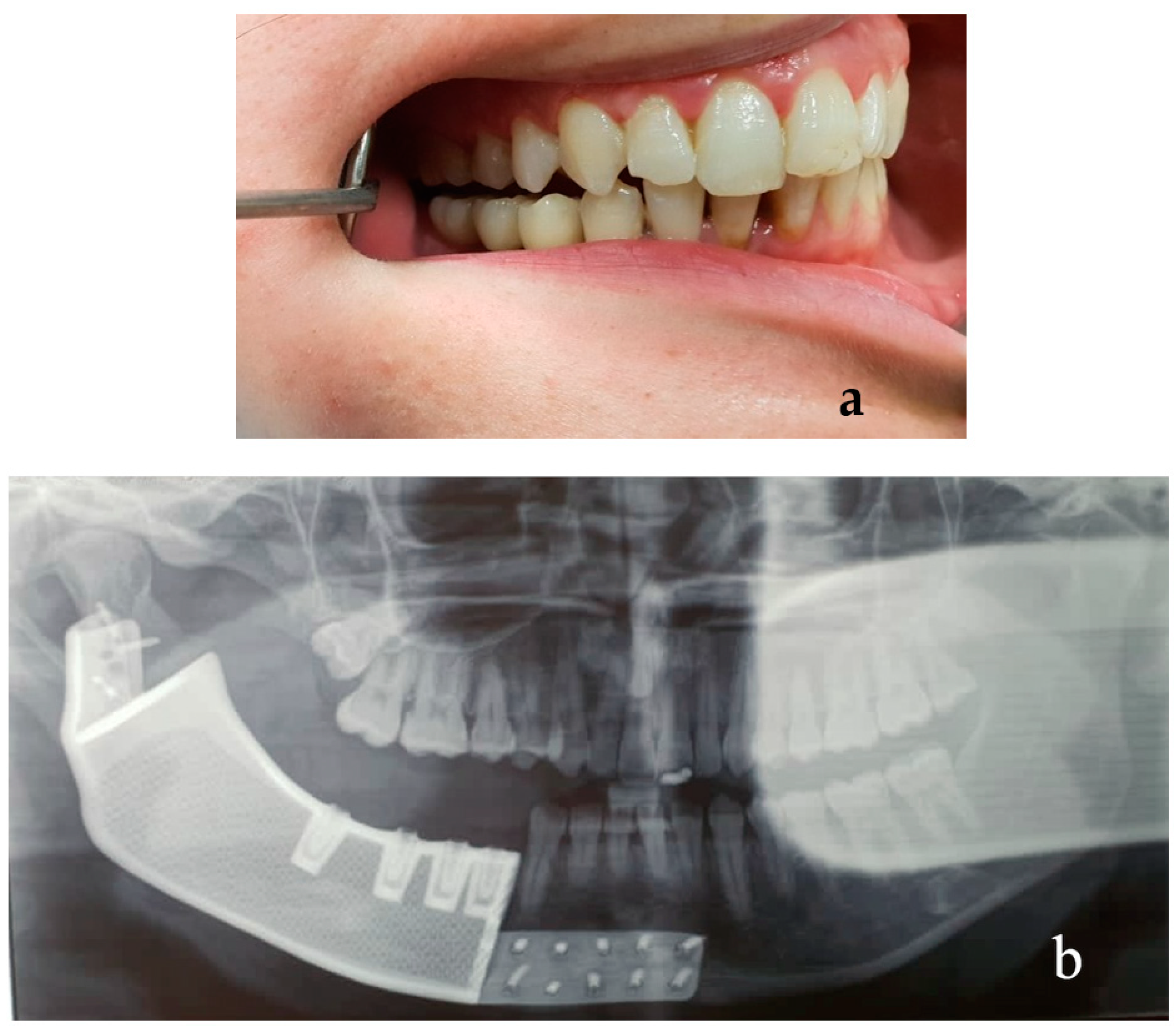
2.5. Results Case #1
2.6. Patient #2
2.7. Design Case #2
2.8. Surgical Sequence Case #2
2.9. Results Case #2
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wright, J.M.; Vered, M. WHO Classification of Head and Neck Tumours, 4th ed.; El-Naggar, A.K., Chan, J.K.C., Grandis, J.R., Takata, T., Slootweg, P., Eds.; IARC Press: Lyon, France, 2017; pp. 215–219. [Google Scholar]
- Soluk-Tekkesin, M.; Wright, J.M. The World Health Organization Classification of Odontogenic Lesions: A Summary of the Changes of the 2022 (5th) Edition. Turk. Patoloji Derg. 2022, 38, 168–184. [Google Scholar] [CrossRef] [PubMed]
- Shi, H.A.; Ng, C.W.B.; Kwa, C.T.; Sim, Q.X.C. Ameloblastoma: A succinct review of the classification, genetic understanding and novel molecular targeted therapies. Surgeon 2021, 19, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Effiom, O.A.; Ogundana, O.M.; Akinshipo, A.O.; Akintoye, S.O. Ameloblastoma: Current etiopathological concepts and management. Oral. Dis. 2018, 24, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Dandriyal, R.; Gupta, A.; Pant, S.; Baweja, H.H. Surgical management of ameloblastoma: Conservative or radical approach. Natl. J. Maxillofac. Surg. 2011, 2, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.M.; Chen, J.Y.; Chen, C.H.; Huang, C.J. Radiotherapy for a repeatedly recurrent ameloblastoma with malignant transformation. Head Neck 2014, 36, E1–E3. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Zhang, X.; Li, X. Molecular biology exploration and targeted therapy strategy of Ameloblastoma. Arch. Oral. Biol. 2022, 140, 105454. [Google Scholar] [CrossRef]
- Hresko, A.; Burtyn, O.; Pavlovskiy, L.; Snisarevskyi, P.; Lapshyna, J.; Chepurnyi, Y.; Kopchak, A.; Karagozoglu, K.H.; Forouzanfar, T. Controversies in ameloblastoma management: Evaluation of decision making, based on a retrospective analysis. Med. Oral Patol. Oral Cir. Bucal 2021, 26, e181–e186. [Google Scholar] [CrossRef]
- Boffano, P.; Cavarra, F.; Tricarico, G.; Masu, L.; Brucoli, M.; Ruslin, M.; Forouzanfar, T.; Ridwan-Pramana, A.; Rodriguez-Santamarta, T.; Rui Ranz, M.; et al. The epidemiology and management of ameloblastomas: A European multicenter study. J. Craniomaxillofac. Surg. 2021, 49, 1107–1112. [Google Scholar] [CrossRef]
- Rodrigues, D.B.; Wolford, L.M.; Malaquias, P.; Campos, P.S. Concomitant treatment of mandibular ameloblastoma and bilateral temporomandibular joint osteoarthritis with bone graft and total joint prostheses. J. Oral Maxillofac. Surg. 2015, 73, 63–74. [Google Scholar] [CrossRef]
- Hayden, R.E.; Mullin, D.P.; Patel, A.K. Reconstruction of the segmental mandibular defect: Current state of the art. Curr. Opin. Otolaryngol. Head Neck Surg. 2012, 20, 231–236. [Google Scholar] [CrossRef]
- Shnayder, Y.; Lin, D.; Desai, S.C.; Nussenbaum, B.; Sand, J.P.; Wax, M.K. Reconstruction of the Lateral Mandibular Defect: A Review and Treatment Algorithm. JAMA Facial Plast. Surg. 2015, 17, 367–373. [Google Scholar] [CrossRef] [PubMed]
- Horen, S.R.; Hansdorfer, M.A.; Seu, M.; Murphy, J.; Figueroa, A.; Tragos, C. Alloplastic Temporomandibular Joint Reconstruction Following Recurrent Ameloblastoma Resection. J. Craniofac. Surg. 2022, 33, 284–288. [Google Scholar] [CrossRef] [PubMed]
- Jo, Y.Y.; Kim, S.G.; Kim, M.K.; Shin, S.H.; Ahn, J.; Seok, H. Mandibular Reconstruction Using a Customized Three-Dimensional Titanium Implant Applied on the Lingual Surface of the Mandible. J. Craniofac. Surg. 2018, 29, 415–419. [Google Scholar] [CrossRef] [PubMed]
- Qassemyar, Q.; Assouly, N.; Temam, S.; Kolb, F. Use of a three-dimensional custom-made porous titanium prosthesis for mandibular body reconstruction. Int. J. Oral Maxillofac. Surg. 2017, 46, 1248–1251. [Google Scholar] [CrossRef]
- Ardila, C.M.; Hernandez-Arenas, Y.; Alvarez-Martinez, E. Mandibular Body Reconstruction Utilizing a Three-Dimensional Custom-Made Porous Titanium Plate: A Four-Year Follow-Up Clinical Report. Case Rep. Dent. 2022, 2022, 5702066. [Google Scholar] [CrossRef]
- Ow, A.; Tan, W.; Pienkowski, L. Mandibular Reconstruction Using a Custom-Made Titanium Prosthesis: A Case Report on the Use of Virtual Surgical Planning and Computer-Aided Design/Computer-Aided Manufacturing. Craniomaxillofac. Trauma Reconstr. 2016, 9, 246–250. [Google Scholar] [CrossRef]
- Matos, J.D.M.; Queiroz, D.A.; Nakano, L.J.N.; Andrade, V.C.; Ribeiro, N.C.R.; Borges, A.L.S.; Bottino, M.A.; Lopes, G. Bioengineering Tools Applied to Dentistry: Validation Methods for In Vitro and In Silico Analysis. Dent. J. 2022, 10, 145. [Google Scholar] [CrossRef]
- Li, P.; Shen, L.; Li, J.; Liang, R.; Tian, W.; Tang, W. Optimal design of an individual endoprosthesis for the reconstruction of extensive mandibular defects with finite element analysis. J. Craniomaxillofac. Surg. 2014, 42, 73–78. [Google Scholar] [CrossRef]
- Merema, B.B.J.; Kraeima, J.; de Visscher, S.; van Minnen, B.; Spijkervet, F.K.L.; Schepman, K.P.; Witjes, M.J.H. Novel finite element-based plate design for bridging mandibular defects: Reducing mechanical failure. Oral Dis. 2020, 26, 1265–1274. [Google Scholar] [CrossRef]
- Anitua, E.; Larrazabal Saez de Ibarra, N.; Saracho Rotaeche, L. Implant-Supported Prostheses in the Edentulous Mandible: Biomechanical Analysis of Different Implant Configurations via Finite Element Analysis. Dent. J. 2022, 11, 4. [Google Scholar] [CrossRef]
- Anitua, E.; Larrazabal Saez de Ibarra, N.; Morales Martin, I.; Saracho Rotaeche, L. Influence of Implant Tilting and Length on the Biomechanics of Single-Tooth Restoration: A Finite Element Analysis in Atrophic Mandible. Dent. J. 2022, 10, 77. [Google Scholar] [CrossRef] [PubMed]
- Hudieb, M.; AlKhader, M.; Mortaja, S.; Abusamak, M.; Wakabayashi, N.; Kasugai, S. Impact of Bone Augmentation of Facial Bone Defect around Osseointegrated Implant: A Three Dimensional Finite Element Analysis. Dent. J. 2021, 9, 114. [Google Scholar] [CrossRef] [PubMed]
- Kelkar, K.C.; Bhat, V.; Hegde, C. Finite element analysis of the effect of framework materials at the bone-implant interface in the all-on-four implant system. Dent. Res. J. 2021, 18, 1. [Google Scholar]
- Dayan, S.C.; Geckili, O. The influence of framework material on stress distribution in maxillary complete-arch fixed prostheses supported by four dental implants: A three-dimensional finite element analysis. Comput. Methods Biomech. Biomed. Eng. 2021, 24, 1606–1617. [Google Scholar] [CrossRef]
- Grande, F.; Pozzan, M.C.; Marconato, R.; Mollica, F.; Catapano, S. Evaluation of Load Distribution in a Mandibular Model with Four Implants Depending on the Number of Prosthetic Screws Used for OT-Bridge System: A Finite Element Analysis (FEA). Materials 2022, 15, 7963. [Google Scholar] [CrossRef]
- Li, H.; Wang, P.; Wen, C. Recent Progress on Nanocrystalline Metallic Materials for Biomedical Applications. Nanomaterials 2022, 12, 2111. [Google Scholar] [CrossRef]
- Niinomi, M. Mechanical biocompatibilities of titanium alloys for biomedical applications. J. Mech. Behav. Biomed. Mater. 2008, 1, 30–42. [Google Scholar] [CrossRef]
- Dahake, S.; Kuthe, A.; Kulkarni, S.; Mawale, M. Finite element analysis of customized implant in mandibular reconstruction after tumor resection with and without using customized surgical osteotomy guide. Int. J. Med. Robot. 2018, 14. [Google Scholar] [CrossRef]
- Li, P.; Tang, Y.; Li, J.; Shen, L.; Tian, W.; Tang, W. Establishment of sequential software processing for a biomechanical model of mandibular reconstruction with custom-made plate. Comput. Methods Programs Biomed. 2013, 111, 642–649. [Google Scholar] [CrossRef]
- Cortese, A.; Caggiano, M.; Carlino, F.; Pantaleo, G. Zygomatic fractures: Technical modifications for better aesthetic and functional results in older patients. Int. J. Surg. 2016, 33 (Suppl. 1), S9–S15. [Google Scholar] [CrossRef]
- Tribst, J.P.M.; Campanelli de Morais, D.; Melo de Matos, J.D.; Lopes, G.; Dal Piva, A.M.O.; Souto Borges, A.L.; Bottino, M.A.; Lanzotti, A.; Martorelli, M.; Ausiello, P. Influence of Framework Material and Posterior Implant Angulation in Full-Arch All-on-4 Implant-Supported Prosthesis Stress Concentration. Dent. J. 2022, 10, 12. [Google Scholar] [CrossRef] [PubMed]
- Rodby, K.A.; Turin, S.; Jacobs, R.J.; Cruz, J.F.; Hassid, V.J.; Kolokythas, A.; Antony, A.K. Advances in oncologic head and neck reconstruction: Systematic review and future considerations of virtual surgical planning and computer aided design/computer aided modeling. J. Plast. Reconstr. Aesthet. Surg. 2014, 67, 1171–1185. [Google Scholar] [CrossRef] [PubMed]
- Ferretti, C.; Ripamonti, U. Pediatric Mandibular Defect Rehabilitation by Human Transforming Growth Factor-beta3 with an Implant-Supported Prosthesis. Int. J. Oral Maxillofac. Implant. 2022, 37, 1256–1260. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, A.; Chiba, H.; Toyoda, J.; Abukawa, H.; Fujikawa, K.; Tsuzuki, M.; Watanabe, M. Mandibular reconstruction using a tray with particulate cancellous bone and marrow and platelet-rich plasma by an intraoral approach. J. Oral Maxillofac. Surg. 2011, 69, 1807–1814. [Google Scholar] [CrossRef] [PubMed]
- Sarlabous, M.; Psutka, D.J. Treatment of Mandibular Ameloblastoma Involving the Mandibular Condyle: Resection and Concomitant Reconstruction with a Custom Hybrid Total Joint Prosthesis and Iliac Bone Graft. J. Craniofac. Surg. 2018, 29, e307–e314. [Google Scholar] [CrossRef] [PubMed]
- Toure, G.; Gouet, E. Use of a 3-Dimensional Custom-Made Porous Titanium Prosthesis for Mandibular Body Reconstruction with Prosthetic Dental Rehabilitation and Lipofilling. J. Oral Maxillofac. Surg. 2019, 77, 1305–1313. [Google Scholar] [CrossRef]












Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cortese, A.; Spirito, F.; Claudio, P.P.; Lo Muzio, L.; Ruggiero, A.; Gargiulo, M. Mandibular Reconstruction after Resection of Ameloblastoma by Custom-Made CAD/CAM Mandibular Titanium Prosthesis: Two Case Reports, Finite Element Analysis and Discussion of the Technique. Dent. J. 2023, 11, 106. https://doi.org/10.3390/dj11040106
Cortese A, Spirito F, Claudio PP, Lo Muzio L, Ruggiero A, Gargiulo M. Mandibular Reconstruction after Resection of Ameloblastoma by Custom-Made CAD/CAM Mandibular Titanium Prosthesis: Two Case Reports, Finite Element Analysis and Discussion of the Technique. Dentistry Journal. 2023; 11(4):106. https://doi.org/10.3390/dj11040106
Chicago/Turabian StyleCortese, Antonio, Francesca Spirito, Pier Paolo Claudio, Lorenzo Lo Muzio, Alessandro Ruggiero, and Maurizio Gargiulo. 2023. "Mandibular Reconstruction after Resection of Ameloblastoma by Custom-Made CAD/CAM Mandibular Titanium Prosthesis: Two Case Reports, Finite Element Analysis and Discussion of the Technique" Dentistry Journal 11, no. 4: 106. https://doi.org/10.3390/dj11040106
APA StyleCortese, A., Spirito, F., Claudio, P. P., Lo Muzio, L., Ruggiero, A., & Gargiulo, M. (2023). Mandibular Reconstruction after Resection of Ameloblastoma by Custom-Made CAD/CAM Mandibular Titanium Prosthesis: Two Case Reports, Finite Element Analysis and Discussion of the Technique. Dentistry Journal, 11(4), 106. https://doi.org/10.3390/dj11040106