

Anticholinergic Medication and Caries Status Predict Xerostomia under 65


Abstract
:1. Introduction
2. Methods
Statistical Analysis
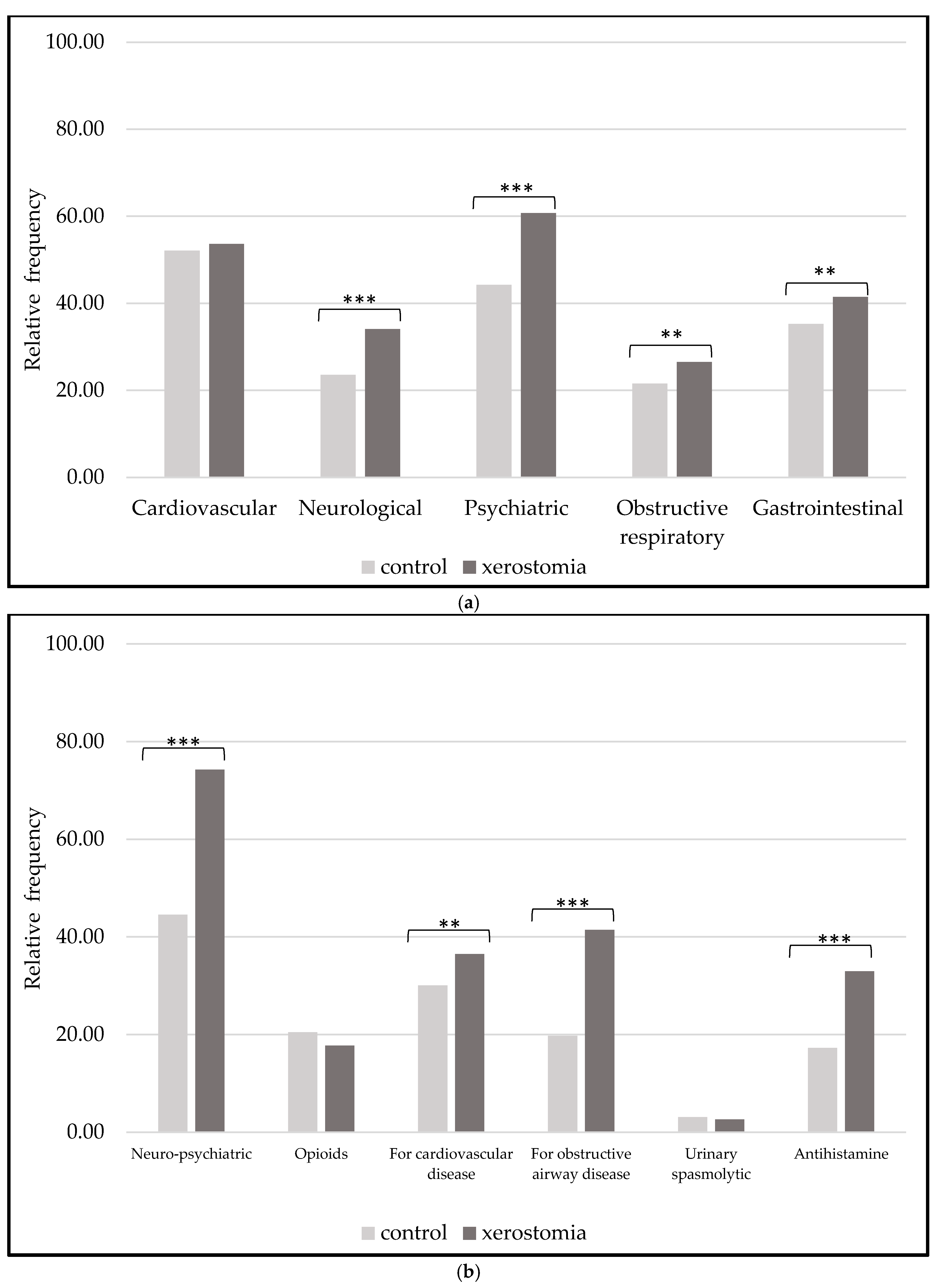
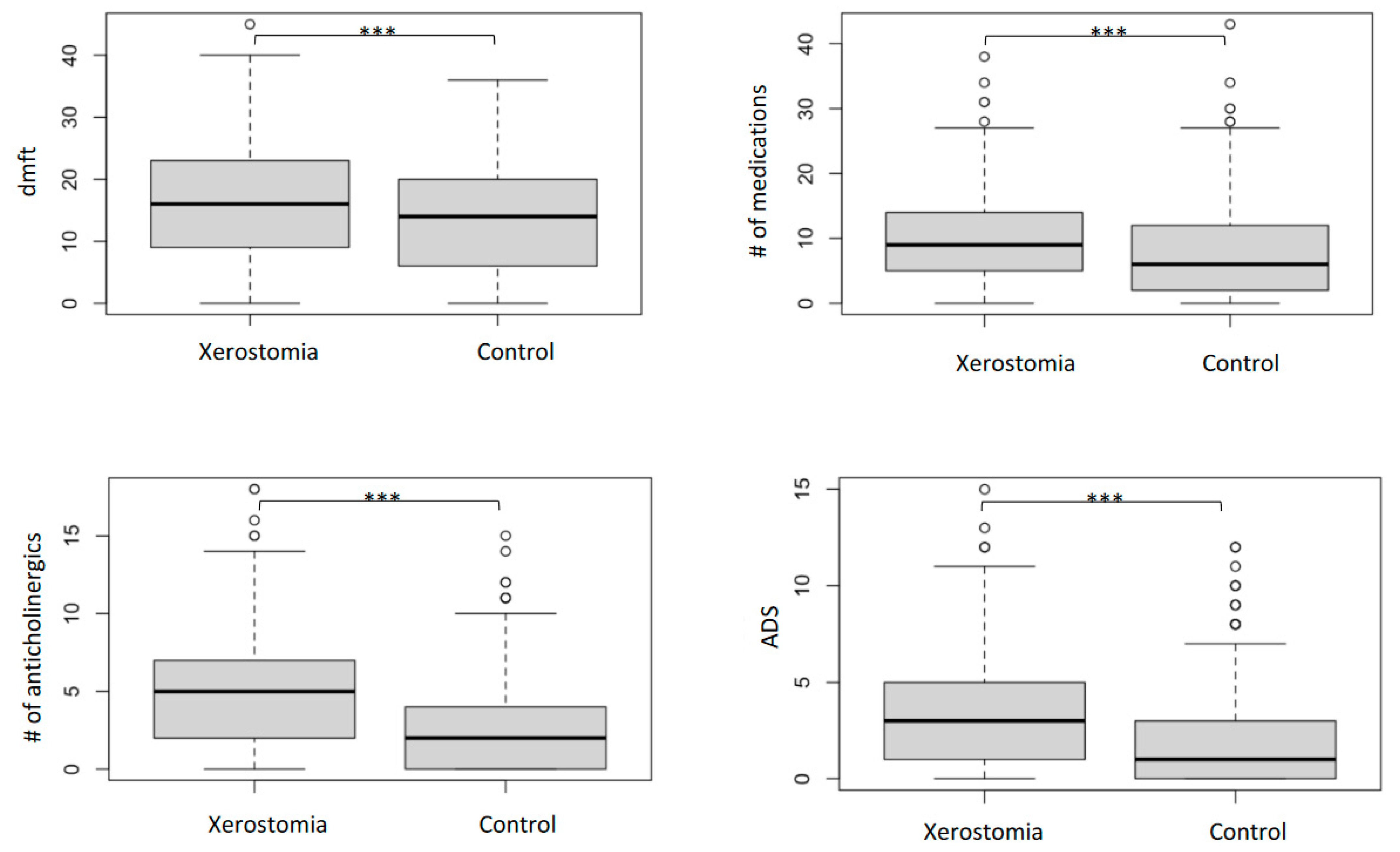
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ohara, Y.; Hirano, H.; Yoshida, H.; Obuchi, S.; Ihara, K.; Fujiwara, Y.; Mataki, S. Prevalence and factors associated with xerostomia and hyposalivation among community-dwelling older people in Japan. Gerodontology 2013, 33, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Villa, A.; Nordio, F.; Gohel, A. A risk prediction model for xerostomia: A retrospective cohort study. Gerodontology 2016, 33, 562–568. [Google Scholar] [CrossRef] [PubMed]
- Friedlander, A.H.; Norman, D.C. Late-life depression: Psychopathology, medical interventions, and dental implications. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2002, 94, 404–412. [Google Scholar] [CrossRef] [PubMed]
- Agostini, B.A.; Cericato, G.O.; da Silveira, E.R.; Nascimento, G.G.; dos Santos Costa, F.; Thomson, W.M.; Demarco, F.F. How Common is Dry Mouth? Systematic Review and Meta-Regression Analysis of Prevalence Estimates. Braz. Dent. J. 2018, 29, 606–618. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, L.; Kupek, E.; Peres, K.G. General health influences episodes of xerostomia: A prospective population-based study. Community Dent. Oral Epidemiol 2017, 45, 153–159. [Google Scholar] [CrossRef]
- Bardow, A.; Nyvad, B.; Nauntofte, B. Relationships between medication intake, complaints of dry mouth, salivary flow rate and composition, and the rate of tooth demineralization in situ. Arch. Oral Biol. 2001, 46, 413–423. [Google Scholar] [CrossRef]
- Hu, K.-F.; Chou, Y.-H.; Wen, Y.-H.; Hsieh, K.-P.; Tsai, J.-H.; Yang, P.; Yang, Y.-H.; Lin, C.-H.R. Antipsychotic medications and dental caries in newly diagnosed schizophrenia: A nationwide cohort study. Psychiatry Res. 2016, 245, 45–50. [Google Scholar] [CrossRef]
- Thomson, W.M.; Lawrence, H.P.; Broadbent, J.M.; Poulton, R. The impact of xerostomia on oral-health-related quality of life among younger adults. Health Qual. Life Outcomes 2006, 4, 86. [Google Scholar] [CrossRef]
- Aliko, A.; Wolff, A.; Dawes, C.; Aframian, D.; Proctor, G.; Ekström, J.; Narayana, N.; Villa, A.; Sia, Y.W.; Joshi, R.K.; et al. World Workshop on Oral Medicine VI: Clinical implications of medication-induced salivary gland dysfunction. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2015, 120, 185–206. [Google Scholar] [CrossRef]
- Jager, D.H.J.; Bots, C.P.; Forouzanfar, T.; Brand, H.S. Clinical oral dryness score: Evaluation of a new screening method for oral dryness. Odontology 2018, 106, 439–444. [Google Scholar] [CrossRef]
- Wolff, A.; Zuk-Paz, L.; Kaplan, I. Major salivary gland output differs between users and non-users of specific medication categories. Gerodontology 2008, 25, 210–216. [Google Scholar] [CrossRef]
- Mathews, S.A.; Kurien, B.T.; Scofield, R.H. Oral manifestations of sjögren’s syndrome. J. Dent. Res. 2008, 87, 308–318. [Google Scholar] [CrossRef] [PubMed]
- Arany, S.; Kopycka-Kedzierawski, D.T.; Caprio, T.V.; Watson, G.E. Anticholinergic medication: Related dry mouth and effects on the salivary glands. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2021, 132, 662–670. [Google Scholar] [CrossRef] [PubMed]
- Kantor, E.D.; Rehm, C.D.; Du, M.; White, E.; Giovannucci, E.L. Trends in Dietary Supplement Use among US Adults From 1999–2012. JAMA 2016, 316, 1464–1474. [Google Scholar] [CrossRef]
- Thomson, W.M. Dry mouth and older people. Aust. Dent. J. 2015, 60 (Suppl. 1), 54–63. [Google Scholar] [CrossRef] [PubMed]
- Halli-Tierney, A.D.; Scarbrough, C.; Carroll, D. Polypharmacy: Evaluating Risks and Deprescribing. Am. Fam. Physician 2019, 100, 32–38. [Google Scholar] [PubMed]
- Menditto, E.; Gimeno-Miguel, A.; Juste, A.M.; Poblador-Plou, B.; Aza-Pascual-Salcedo, M.; Orlando, V.; Rubio, F.G.; Torres, A.P. Patterns of multimorbidity and polypharmacy in young and adult population: Systematic associations among chronic diseases and drugs using factor analysis. PLoS ONE 2019, 14, e0210701. [Google Scholar] [CrossRef]
- Ferrari, A.; Baraldi, C.; Licata, M.; Rustichelli, C. Polypharmacy Among Headache Patients: A Cross-Sectional Study. CNS Drugs 2018, 32, 567–578. [Google Scholar] [CrossRef]
- Field, E.; Fear, S.; Higham, S.; Ireland, R.; Rostron, J.; Willetts, R.M.; Longman, L. Age and medication are significant risk factors for xerostomia in an English population, attending general dental practice. Gerodontology 2001, 18, 21–24. [Google Scholar] [CrossRef]
- Tollefson, G.D.; Montague-Clouse, J.; Lancaster, S.P. The relationship of serum anticholinergic activity to mental status performance in an elderly nursing home population. J. Neuropsychiatry 1991, 3, 314–319. [Google Scholar] [CrossRef]
- Tune, L.E.; Damlouji, N.F.; Holland, A.; Gardner, T.J.; Folstein, M.F.; Coyle, J.T. Association of postoperative delirium with raised serum levels of anticholinergic drugs. Lancet 1981, 2, 651–653. [Google Scholar] [CrossRef] [PubMed]
- Tiisanoja, A.; Syrjälä, A.-M.; Kullaa, A.; Ylöstalo, P. Anticholinergic Burden and Dry Mouth in Middle-Aged People. JDR Clin. Transl. Res. 2020, 5, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Carnahan, R.M.; Lund, B.C.; Perry, P.J.; Pollock, B.G.; Culp, K.R. The Anticholinergic Drug Scale as a Measure of Drug-Related Anticholinergic Burden: Associations with Serum Anticholinergic Activity. J. Clin. Pharmacol. 2006, 46, 1481–1486. [Google Scholar] [CrossRef]
- Kersten, H.; Wyller, T.B.; Molden, E. Association between inherited cyp2d6/2c19 phenotypes and anticholinergic measures in elderly patients using anticholinergic drugs. Ther. Drug Monit. 2014, 36, 125–130. [Google Scholar] [CrossRef]
- Tiisanoja, A.; Syrjala, A.M.; Anttonen, V.; Ylostalo, P. Anticholinergic burden, oral hygiene practices, and oral hygiene status-cross-sectional findings from the northern finland birth cohort 1966. Clin. Oral. Investig. 2021, 25, 1829–1837. [Google Scholar] [CrossRef]
- Chapuis, J.; Siu-Paredes, F.; Pavageau, C.; Amador, G.; Rude, N.; Denis, F. Anticholinergic drugs and oral health-related quality of life in patients with schizophrenia: A pilot study. Transl. Neurosci. 2020, 11, 10–16. [Google Scholar] [CrossRef]
- Janssens, B.; Vanobbergen, J.; Petrovic, M.; Jacquet, W.; Schols, J.M.; De Visschere, L. The impact of a preventive and curative oral healthcare program on the prevalence and incidence of oral health problems in nursing home residents. PLoS ONE 2018, 13, e0198910. [Google Scholar] [CrossRef]
- Lexomboon, D.; Tan, E.C.; Höijer, J.; Garcia-Ptacek, S.; Eriksdotter, M.; Religa, D.; Fastbom, J.; Johnell, K.; Sandborgh-Englund, G. The Effect of Xerostomic Medication on Oral Health in Persons with Dementia. J. Am. Med. Dir. Assoc. 2018, 19, 1080–1085.e2. [Google Scholar] [CrossRef]
- Durán, C.E.; Azermai, M.; Stichele, R.H.V. Systematic review of anticholinergic risk scales in older adults. Eur. J. Clin. Pharmacol. 2013, 69, 1485–1496. [Google Scholar] [CrossRef] [PubMed]
- Bardow, A.; Moe, D.; Nyvad, B.; Nauntofte, B. The buffer capacity and buffer systems of human whole saliva measured without loss of CO2. Arch. Oral Biol. 1999, 45, 1–12. [Google Scholar] [CrossRef]
- Scully, C. Drug effects on salivary glands: Dry mouth. Oral. Dis. 2003, 9, 165–176. [Google Scholar] [CrossRef] [PubMed]
- Kachru, N.; Carnahan, R.M.; Johnson, M.L.; Aparasu, R.R. Potentially Inappropriate Anticholinergic Medication Use in Community-Dwelling Older Adults: A National Cross-Sectional Study. Drugs Aging 2015, 32, 379–389. [Google Scholar] [CrossRef]
- Tan, E.C.K.; Lexomboon, D.; Englund, G.S.; Haasum, Y.; Johnell, K. Medications That Cause Dry Mouth as an Adverse Effect in Older People: A Systematic Review and Metaanalysis. J. Am. Geriatr. Soc. 2018, 66, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Nederfors, T.; Isaksson, R.; Mornstad, H.; Dahlof, C. Prevalence of perceived symptoms of dry mouth in an adult Swedish population--relation to age, sex and pharmacotherapy. Community Dent. Oral Epidemiol. 1997, 25, 211–216. [Google Scholar] [CrossRef]
- Minagi, H.O.; Yamanaka, Y.; Nohara, K.; Ikai, K.; Sakai, T. Analysis of medication-induced xerostomia in elderly Japanese patients. Clin. Oral Investig. 2021, 26, 2021–2029. [Google Scholar] [CrossRef] [PubMed]
- Marcott, S.; Dewan, K.; Kwan, M.; Baik, F.; Lee, Y.-J.; Sirjani, D. Where Dysphagia Begins: Polypharmacy and Xerostomia. Fed. Pract. Health Care Prof. VA DoD PHS 2020, 37, 234–241. [Google Scholar]
- Tiisanoja, A.; Syrjälä, A.-M.; Komulainen, K.; Lampela, P.; Hartikainen, S.; Taipale, H.; Knuuttila, M.; Ylöstalo, P. Anticholinergic burden and dry mouth among Finnish, community-dwelling older adults. Gerodontology 2018, 35, 3–10. [Google Scholar] [CrossRef]
- Kersten, H.; Molden, E.; Willumsen, T.; Engedal, K.; Wyller, T.B. Higher anticholinergic drug scale (ADS) scores are associated with peripheral but not cognitive markers of cholinergic blockade. Cross sectional data from 21 Norwegian nursing homes. Br. J. Clin. Pharmacol. 2013, 75, 842–849. [Google Scholar] [CrossRef]
- Ziad, A.; Olekhnovitch, R.; Ruiz, F.; Berr, C.; Bégaud, B.; Goldberg, M.; Zins, M.; Mura, T. Anticholinergic drug use and cognitive performances in middle age: Findings from the constances cohort. J. Neurol. Neurosurg. Psychiatry 2018, 89, 1107–1115. [Google Scholar] [CrossRef]
- Fortuna, G.; Whitmire, S.; Sullivan, K.; Alajbeg, I.; Andabak-Rogulj, A.; Pedersen, A.M.L.; Vissink, A.; di Fede, O.; Aria, M.; Jager, D.J.; et al. Impact of medications on salivary flow rate in patients with xerostomia: A retrospective study by the Xeromeds Consortium. Clin. Oral Investig. 2022, 27, 235–248. [Google Scholar] [CrossRef]
- Lagerberg, T.; Molero, Y.; D’Onofrio, B.M.; de la Cruz, L.F.; Lichtenstein, P.; Mataix-Cols, D.; Rück, C.; Hellner, C.; Chang, Z. Antidepressant prescription patterns and CNS polypharmacy with antidepressants among children, adolescents, and young adults: A population-based study in Sweden. Eur. Child Adolesc. Psychiatry 2019, 28, 1137–1145. [Google Scholar] [CrossRef] [PubMed]
- Rad, M.; Kakoie, S.; Brojeni, F.N.; Pourdamghan, N. Effect of Long-term Smoking on Whole-mouth Salivary Flow Rate and Oral Health. J. Dent. Res. Dent. Clin. Dent. Prospect. 2010, 4, 110–114. [Google Scholar] [CrossRef]
- Setia, S.; Pannu, P.; Gambhir, R.; Galhotra, V.; Ahluwalia, P.; Sofat, A. Correlation of oral hygiene practices, smoking and oral health conditions with self perceived halitosis amongst undergraduate dental students. J. Nat. Sci. Biol. Med. 2014, 5, 67–72. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Xerostomia (n = 649) | Control (n = 649) | ||
|---|---|---|---|
| Age (years) | |||
| Mean | 47.53 | 47.32 | |
| SD | 11.78 | 12.08 | |
| Gender (%) | |||
| Female | 72.63 | 72.26 | |
| Male | 27.37 | 27.74 | |
| Race (%) | p < 0.001 | ||
| White | 60.40 | 43.91 | |
| Black | 17.10 | 24.65 | |
| NA | 22.50 | 31.44 | |
| Smoking (%) | 45.92 | 33.89 | p < 0.001 |
| Diabetes (%) | 22.68 | 16.48 | p < 0.05 |
| Sleep apnea (%) | 10.79 | 4.47 | p < 0.001 |
| Wearing dentures (%) | 55.47 | 16.79 | p < 0.001 |
| Complete edentulous (%) | 10.48 | 8.01 | |
| D; number of decayed teeth | |||
| Mean | 1.86 | 1.5 | p < 0.001 |
| SD | 3.35 | 2.76 | |
| M; number of missing teeth | |||
| Mean | 7.65 | 6.16 | p < 0.001 |
| SD | 8.89 | 7.50 | |
| F; number of filled teeth | |||
| Mean | 6.62 | 6.32 | p < 0.001 |
| SD | 5.45 | 5.47 |
| Xerostomia (n = 649) | Control (n = 649) | ||||
|---|---|---|---|---|---|
| ADS | Number of patients | Cumulative frequency | Number of patients | Cumulative frequency | |
| ADS < 3 | low | 287 | 45.6 | 421 | 70.2 |
| 3 ADS | medium | 215 | 79.7 | 121 | 90.4 |
| ADS > | high | 128 | 100 | 58 | 100 |
| Age Group | 18–35 Years | 36–50 Years | 51–65 Years | |||
|---|---|---|---|---|---|---|
| Control (n = 121) | Xerostomia (n = 122) | Control (n = 192) | Xerostomia (n = 203) | Control (n = 337) | Xerostomia (n = 324) | |
| Polypharmacy | 44 | 81 | 117 | 170 | 216 | 280 |
| p = 0.007 | p = 0.042 | p = 0.015 | ||||
| Anticholinergic polypharmacy | 13 | 44 | 47 | 118 | 98 | 185 |
| p < 0.001 | p < 0.001 | p < 0.001 | ||||
| Term | Coefficient | SE Coef | 95% CI | Z-Value | p-Value | VIF |
|---|---|---|---|---|---|---|
| Constant | −0.842 | 0.140 | (−1.116, −0.569) | −6.03 | 0.000 | |
| Total number of medications | −0.112 | 0.0186 | (−0.148, −0.075) | −5.99 | 0.000 | 3.45 |
| Number of anticholinergics | 0.389 | 0.046 | (0.299, 0.480) | 8.48 | 0.000 | 4.47 |
| DMFT (D + M + F) | 0.0188 | 0.007 | (0.005, 0.033) | 2.67 | 0.008 | 1.03 |
| ADS | 0.0272 | 0.037 | (−0.045, 0.099) | 0.74 | 0.461 | 2.14 |
| Odds Ratio | 95% CI | |||||
| Total number of medications | 0.894 | (0.862, 0.928) | ||||
| Number of anticholinergics | 1.477 | (1.349, 1.616) | ||||
| DMFT (D + M + F) | 1.019 | (1.005, 1.033) | ||||
| ADS | 1.028 | (0.956, 1.105) | ||||
| Wald Test | ||||||
| Source | DF | Chi-Squared | p-Value | |||
| Regression | 4 | 136.09 | 0.000 | |||
| Total number of medications | 1 | 35.89 | 0.000 | |||
| Number of anticholinergics | 1 | 71.85 | 0.000 | |||
| DMFT (D + M + F) | 1 | 7.12 | 0.008 | |||
| ADS | 1 | 0.54 | 0.461 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheah, H.L.; Gray, M.; Aboelmagd, S.; Barmak, A.B.; Arany, S. Anticholinergic Medication and Caries Status Predict Xerostomia under 65. Dent. J. 2023, 11, 87. https://doi.org/10.3390/dj11040087
Cheah HL, Gray M, Aboelmagd S, Barmak AB, Arany S. Anticholinergic Medication and Caries Status Predict Xerostomia under 65. Dentistry Journal. 2023; 11(4):87. https://doi.org/10.3390/dj11040087
Chicago/Turabian StyleCheah, Hui Ling, Michael Gray, Shahenda Aboelmagd, Abdul Basir Barmak, and Szilvia Arany. 2023. "Anticholinergic Medication and Caries Status Predict Xerostomia under 65" Dentistry Journal 11, no. 4: 87. https://doi.org/10.3390/dj11040087
APA StyleCheah, H. L., Gray, M., Aboelmagd, S., Barmak, A. B., & Arany, S. (2023). Anticholinergic Medication and Caries Status Predict Xerostomia under 65. Dentistry Journal, 11(4), 87. https://doi.org/10.3390/dj11040087