

Effects of Minocycline Hydrochloride as an Adjuvant Therapy for a Guided Bone Augmentation Procedure in The Rat Calvarium

 , , ,
, , ,
Abstract
:1. Introduction
2. Material and Methods
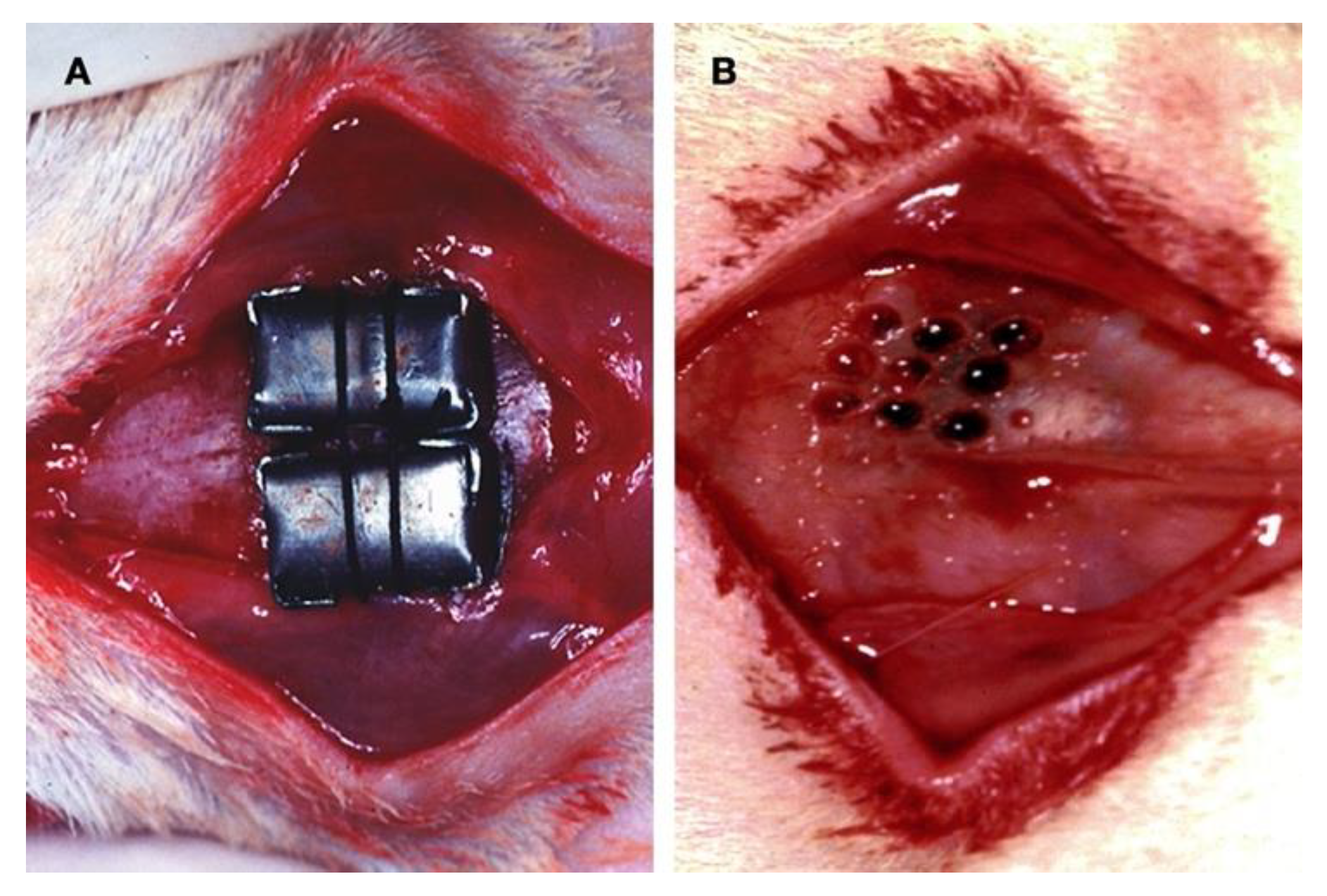
2.1. Animal Preparation and Surgical Procedures
- Control group (C): no calvaria manipulations; no drugs.
- Test group I (P): cortical perforations; no drugs.
- Test group II (MIN): no bone wounding; minocycline-fed.
- Test group III (MIN + P): cortical perforations; minocycline-fed.
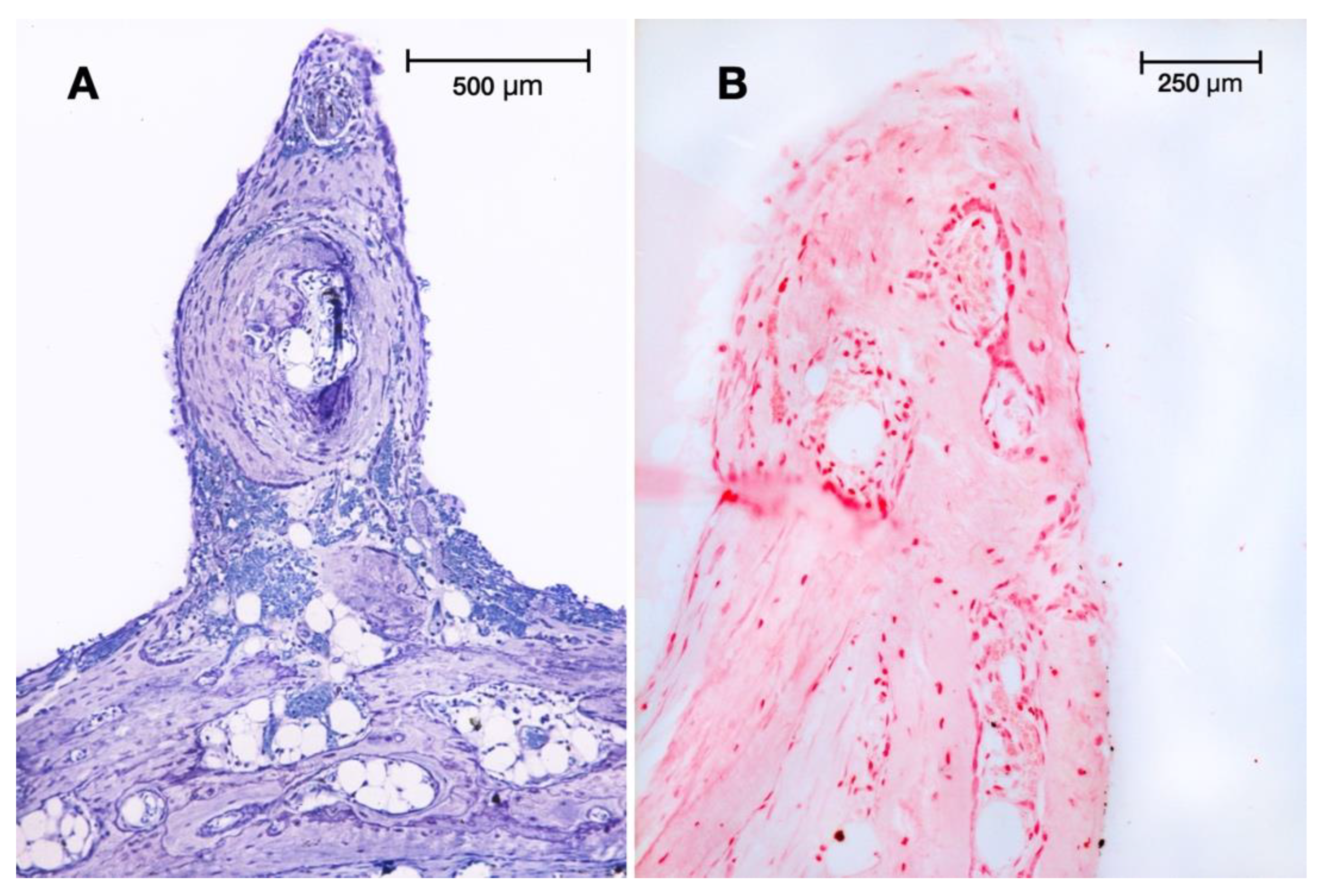
2.2. Histological Preparation
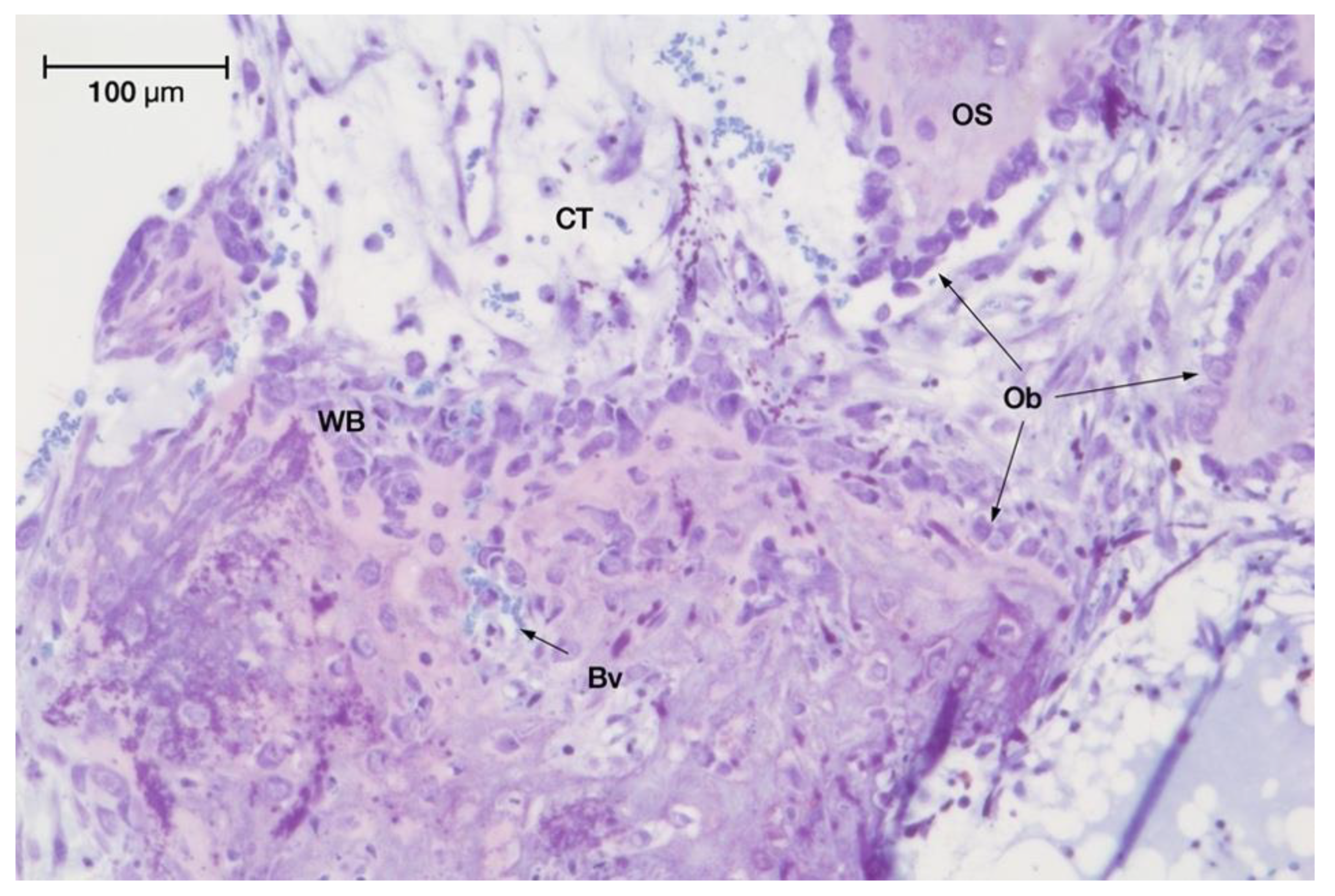
2.3. Microscopic Analysis
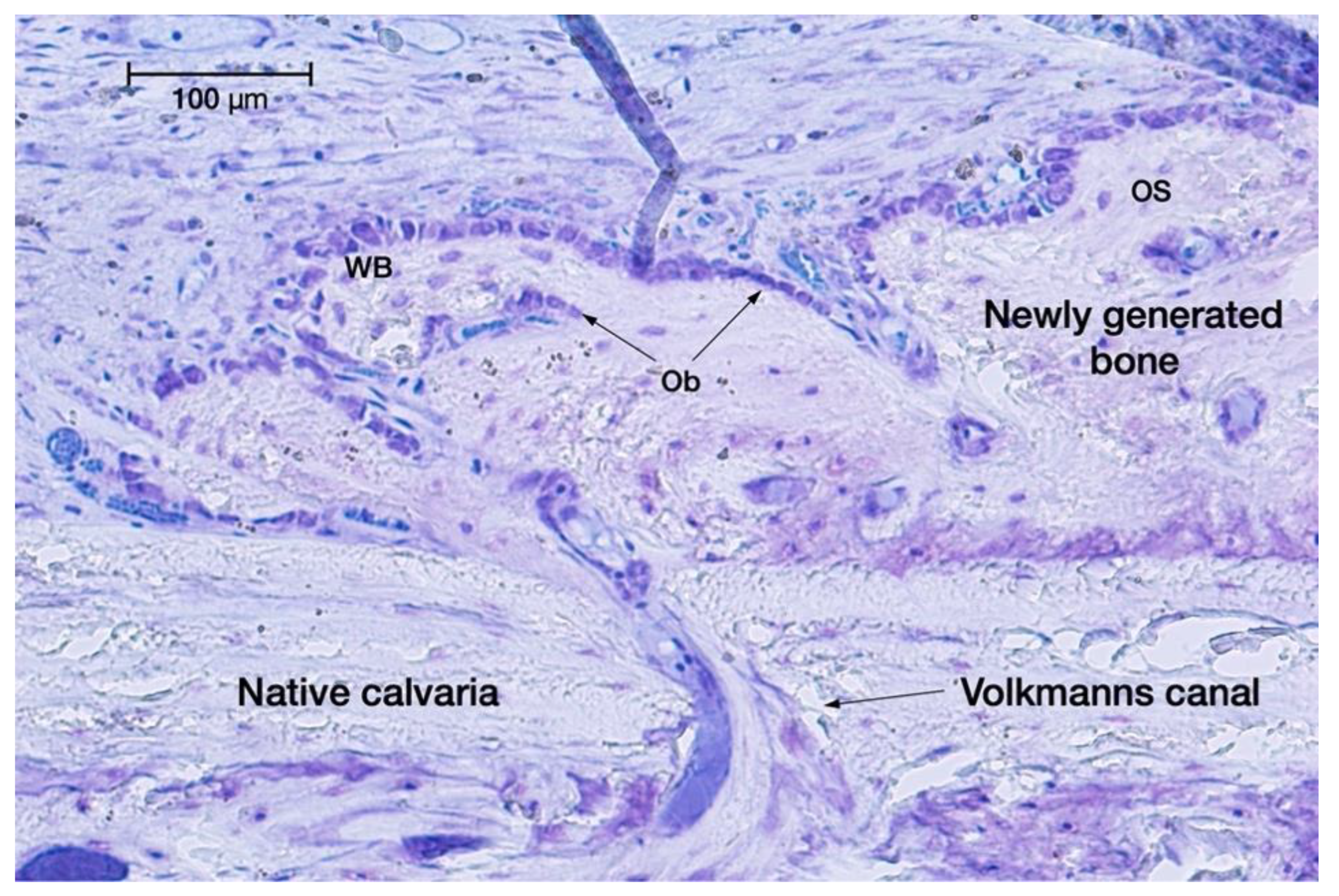
- Newly formed lamellar bone and osteoid tissue (%);
- Woven bone (%);
- Bone marrow (%);
- Connective tissue (%);
- Granulation tissue and blood clot (%);
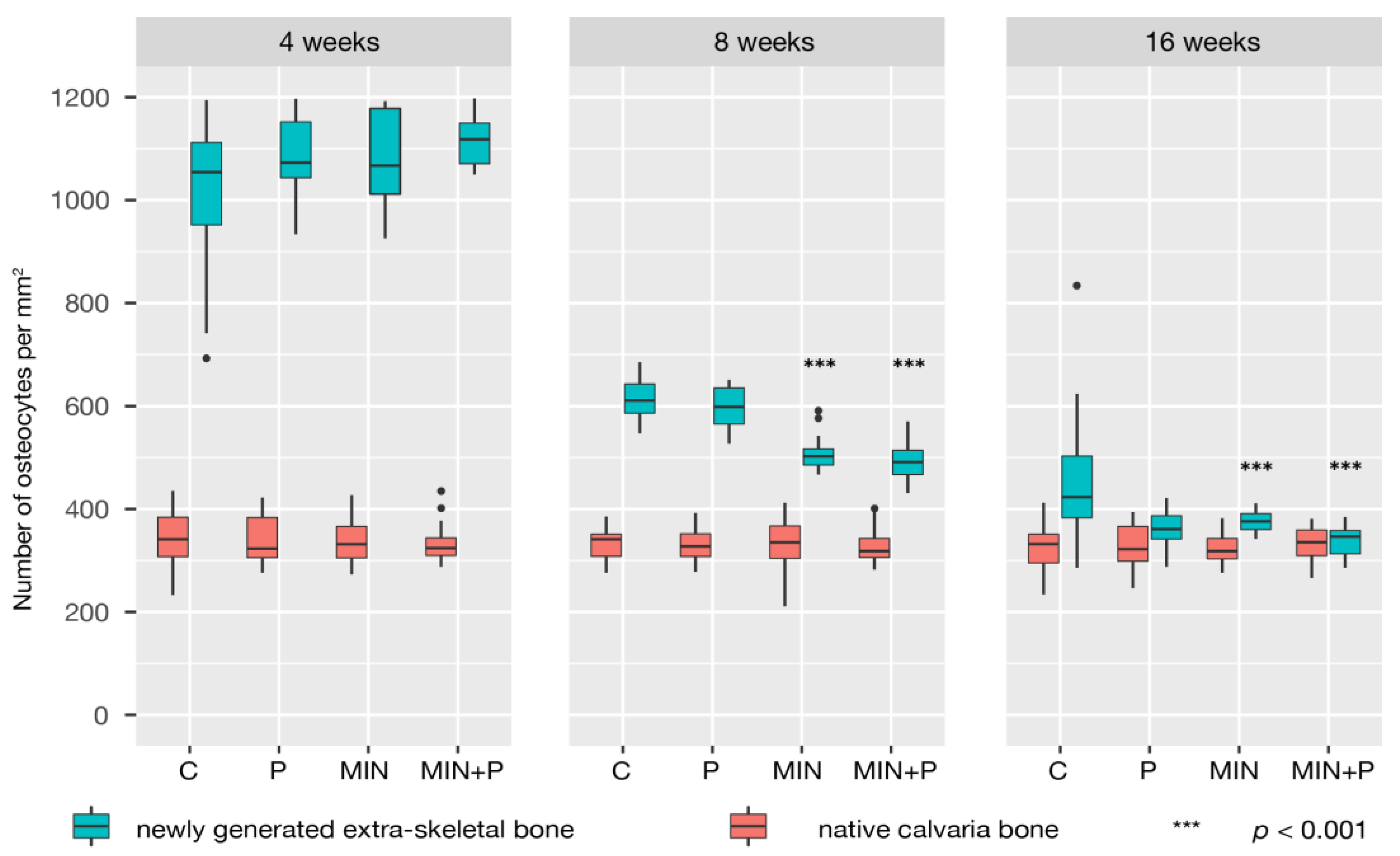
- Number of osteocytes (Oc) per mm2:
- Number of osteoblasts (Ob) per mm:
- Number of blood vessels in the newly formed tissue (capillaries per mm2);
2.4. Statistical Analysis
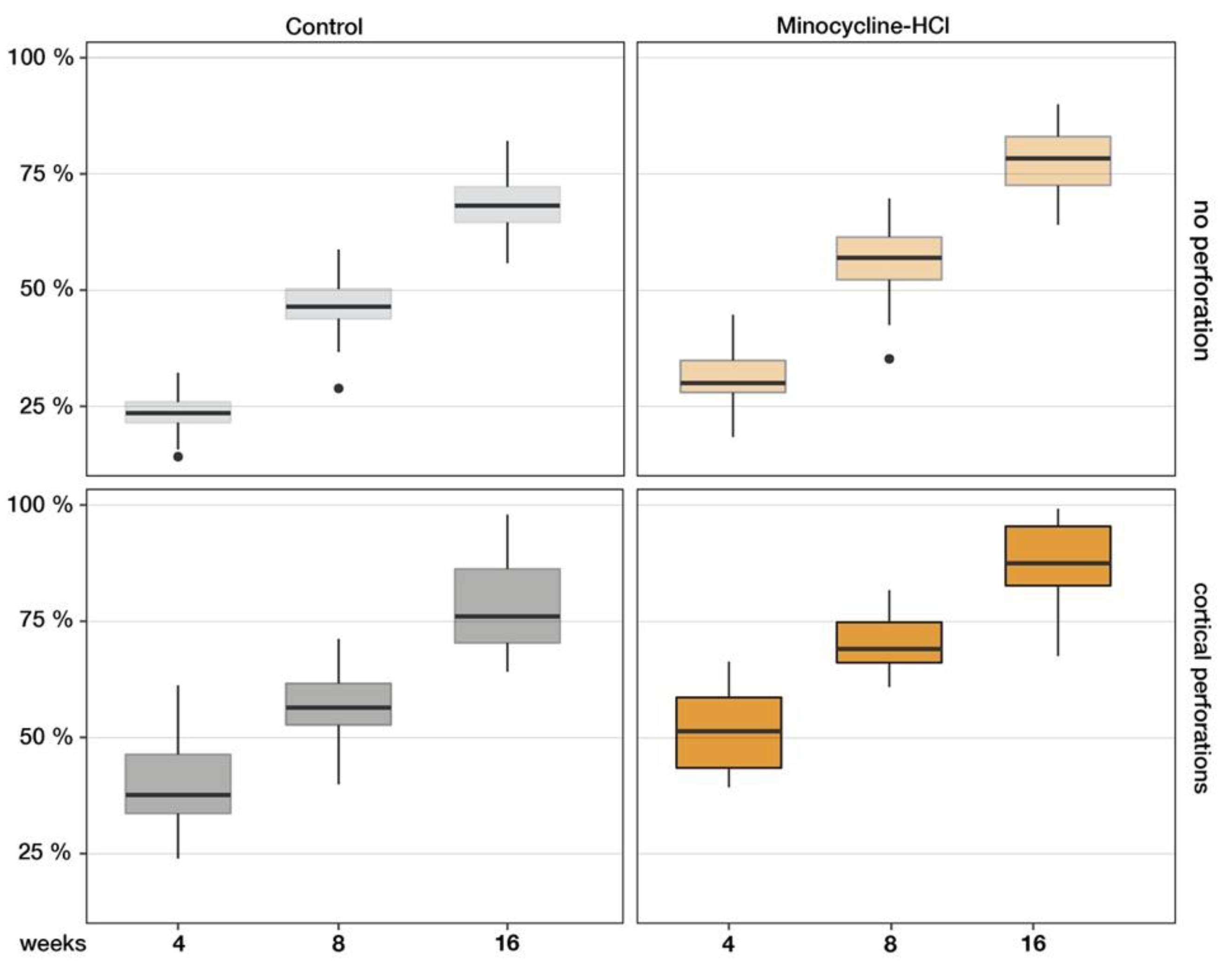
3. Results
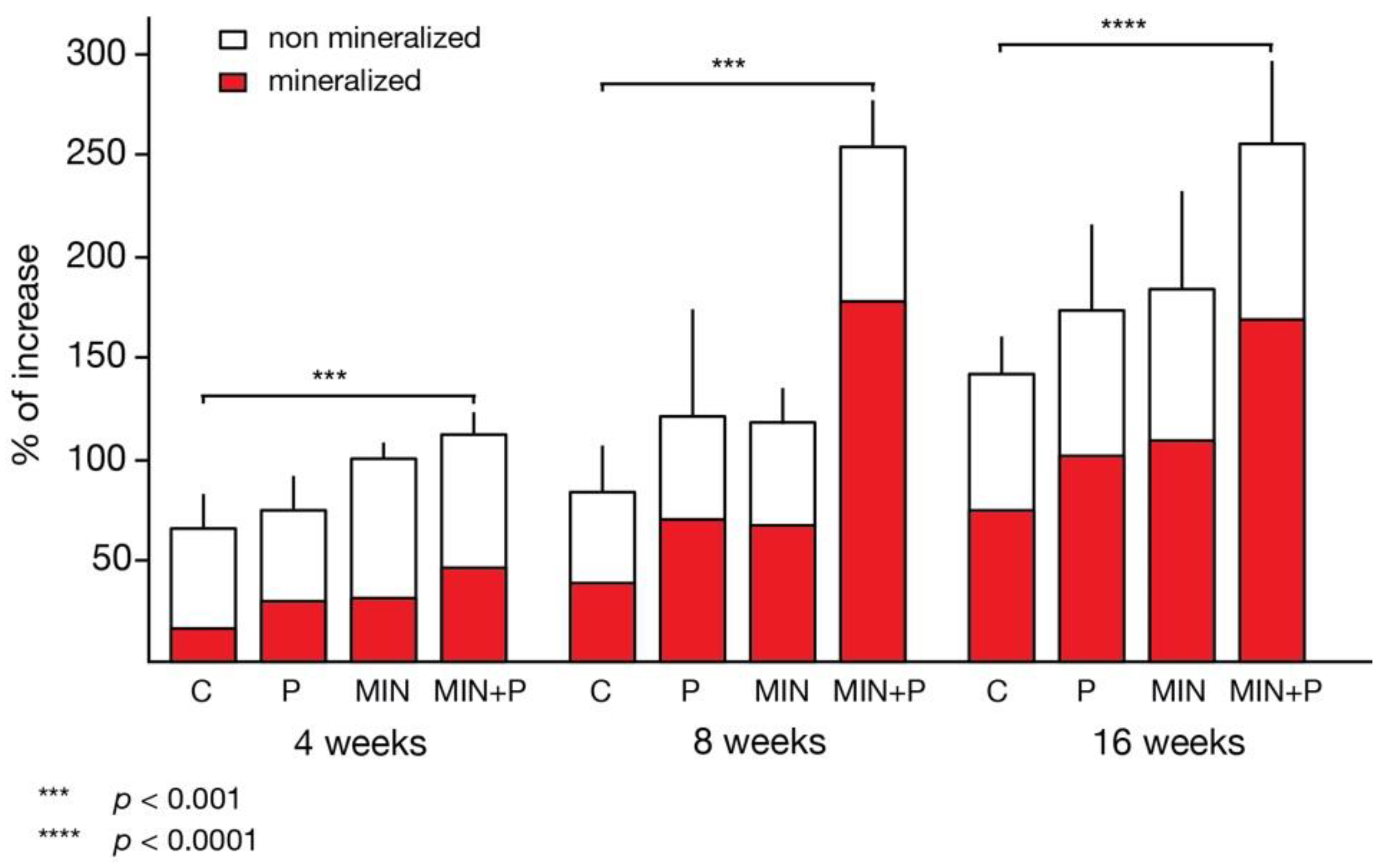
3.1. Four-Week Specimens
3.2. Eight-Week Specimens
3.3. Sixteen-Week Specimens
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hämmerle, C.H.F.; Jung, R.E.; Feloutzis, A. A Systematic Review of the Survival of Implants in Bone Sites Augmented with Barrier Membranes (Guided Bone Regeneration) in Partially Edentulous Patients: Implants in Regenerated Bone. J. Clin. Periodontol. 2002, 29, 226–231. [Google Scholar] [CrossRef]
- Fontana, F.; Maschera, E.; Rocchietta, I.; Simion, M. Clinical Classification of Complications in Guided Bone Regeneration Procedures by Means of a Nonresorbable Membrane. Int. J. Periodontics Restor. Dent. 2011, 31, 265–273. [Google Scholar]
- Rompen, E.H.; Biewer, R.; Vanheusden, A.; Zahedi, S.; Nusgens, B. The Influence of Cortical Perforations and of Space Filling with Peripheral Blood on the Kinetics of Guided Bone Generation. A Comparative Histometric Study in the Rat. Clin. Oral Implant. Res. 1999, 10, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Stavropoulos, A.; Nyengaard, J.R.; Kostopoulos, L.; Karring, T. Implant Placement in Bone Formed beyond the Skeletal Envelope by Means of Guided Tissue Regeneration: An Experimental Study in the Rat. J. Clin. Periodontol. 2005, 32, 1108–1115. [Google Scholar] [CrossRef] [PubMed]
- Maréchal, M.; Luyten, F.; Nijs, J.; Postnov, A.; Schepers, E.; van Steenberghe, D. Histomorphometry and Micro-Computed Tomography of Bone Augmentation under a Titanium Membrane. Clin. Oral Implant. Res. 2005, 16, 708–714. [Google Scholar] [CrossRef]
- Esposito, M.; Grusovin, M.G.; Felice, P.; Karatzopoulos, G.; Worthington, H.V.; Coulthard, P. The Efficacy of Horizontal and Vertical Bone Augmentation Procedures for Dental Implants—A Cochrane Systematic Review. Eur. J. Oral Implant. 2009, 2, 167–184. [Google Scholar]
- Hämmerle, C.H.; Schmid, J.; Lang, N.P.; Olah, A.J. Temporal Dynamics of Healing in Rabbit Cranial Defects Using Guided Bone Regeneration. J. Oral. Maxillofac. Surg. 1995, 53, 167–174. [Google Scholar] [CrossRef]
- Schmid, J.; Hämmerle, C.H.; Flückiger, L.; Winkler, J.R.; Olah, A.J.; Gogolewski, S.; Lang, N.P. Blood-Filled Spaces with and without Filler Materials in Guided Bone Regeneration. A Comparative Experimental Study in the Rabbit Using Bioresorbable Membranes. Clin. Oral Implant. Res. 1997, 8, 75–81. [Google Scholar] [CrossRef]
- Danesh-Sani, S.A.; Tarnow, D.; Yip, J.K.; Mojaver, R. The Influence of Cortical Bone Perforation on Guided Bone Regeneration in Humans. Int. J. Oral Maxillofac. Surg. 2017, 46, 261–266. [Google Scholar] [CrossRef]
- Nishimura, I.; Shimizu, Y.; Ooya, K. Effects of Cortical Bone Perforation on Experimental Guided Bone Regeneration. Clin. Oral Implant. Res. 2004, 15, 293–300. [Google Scholar] [CrossRef]
- Kostopoulos, L.; Karring, T. Augmentation of the Rat Mandible Using Guided Tissue Regeneration. Clin. Oral Implant. Res. 1994, 5, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Kostopoulos, L.; Karring, T.; Uraguchi, R. Formation of Jawbone Tuberosities by Guided Tissue Regeneration. An Experimental Study in the Rat. Clin. Oral Implant. Res. 1994, 5, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Gendron, R.; Grenier, D.; Maheu-Robert, L. The Oral Cavity as a Reservoir of Bacterial Pathogens for Focal Infections. Microbes Infect. 2000, 2, 897–906. [Google Scholar] [CrossRef] [PubMed]
- Goel, A.; Arora, S.A.; Chhina, S. Comparative Efficacy of 1% Alendronate Gel and Tetracycline Fibers as an Adjunct to Scaling and Root Planing: A Randomized Control Clinical Trial. Int. J. Pharm. Sci. Res. 2016, 7, 4134–4139. [Google Scholar] [CrossRef]
- Chopra, I.; Roberts, M. Tetracycline Antibiotics: Mode of Action, Applications, Molecular Biology, and Epidemiology of Bacterial Resistance. Microbiol. Mol. Biol. Rev. 2001, 65, 232–260. [Google Scholar] [CrossRef] [Green Version]
- Grevstad, H.J. Doxycycline Prevents Root Resorption and Alveolar Bone Loss in Rats after Periodontal Surgery. Scand. J. Dent. Res. 1993, 101, 287–291. [Google Scholar] [CrossRef]
- Ramamurthy, N.S.; Schroeder, K.L.; McNamara, T.F.; Gwinnett, A.J.; Evans, R.T.; Bosko, C.; Golub, L.M. Root-Surface Caries in Rats and Humans: Inhibition by a Non-Antimicrobial Property of Tetracyclines. Adv. Dent. Res. 1998, 12, 43–50. [Google Scholar] [CrossRef]
- Vanheusden, A.; Nusgens, B.; Goffinet, G.; Zahedi, S.; Lapière, C.M.; Rompen, E. In Vitro Modulation of Human Gingival Epithelial Cell Attachment and Migration by Minocycline-HCL. J. Periodontal Res. 1998, 33, 377–385. [Google Scholar] [CrossRef]
- Golub, L.M.; Elburki, M.S.; Walker, C.; Ryan, M.; Sorsa, T.; Tenenbaum, H.; Goldberg, M.; Wolff, M.; Gu, Y. Non-Antibacterial Tetracycline Formulations: Host-Modulators in the Treatment of Periodontitis and Relevant Systemic Diseases. Int. Dent. J. 2016, 66, 127–135. [Google Scholar] [CrossRef] [Green Version]
- Golub, L.M.; Lee, H.M.; Stoner, J.A.; Sorsa, T.; Reinhardt, R.A.; Wolff, M.S.; Ryan, M.E.; Nummikoski, P.V.; Payne, J.B. Subantimicrobial-Dose Doxycycline Modulates Gingival Crevicular Fluid Biomarkers of Periodontitis in Postmenopausal Osteopenic Women. J. Periodontol. 2008, 79, 1409–1418. [Google Scholar] [CrossRef] [Green Version]
- Kapoor, A.; Malhotra, R.; Grover, V.; Grover, D. Systemic Antibiotic Therapy in Periodontics. Dent. Res. J. 2012, 9, 505–515. [Google Scholar] [CrossRef] [PubMed]
- Killeen, A.C.; Harn, J.A.; Erickson, L.M.; Yu, F.; Reinhardt, R.A. Local Minocycline Effect on Inflammation and Clinical Attachment During Periodontal Maintenance: Randomized Clinical Trial. J. Periodontol. 2016, 87, 1149–1157. [Google Scholar] [CrossRef] [PubMed]
- Vernillo, A.T.; Rifkin, B.R. Effects of Tetracyclines on Bone Metabolism. Adv. Dent. Res. 1998, 12, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Vanheusden, A.J.; Goffinet, G.; Zahedi, S.; Nusgens, B.; Lapière, C.M.; Rompen, E.H. In Vitro Stimulation of Human Gingival Epithelial Cell Attachment to Dentin by Surface Conditioning. J. Periodontol. 1999, 70, 594–603. [Google Scholar] [CrossRef] [PubMed]
- Ramich, T.; Schacher, B.; Scharf, S.; Röllke, L.; Arndt, R.; Eickholz, P.; Nickles, K. Subgingival Plaque Sampling after Combined Mechanical and Antibiotic Nonsurgical Periodontal Therapy. Clin. Oral Investig. 2015, 19, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Kallala, R.; Graham, S.M.; Nikkhah, D.; Kyrkos, M.; Heliotis, M.; Mantalaris, A.; Tsiridis, E. In Vitro and in Vivo Effects of Antibiotics on Bone Cell Metabolism and Fracture Healing. Expert Opin. Drug Saf. 2012, 11, 15–32. [Google Scholar] [CrossRef]
- Payne, J.B.; Golub, L.M. Using Tetracyclines to Treat Osteoporotic/Osteopenic Bone Loss: From the Basic Science Laboratory to the Clinic. Pharmacol. Res. 2011, 63, 121–129. [Google Scholar] [CrossRef] [Green Version]
- Bettany, J.T.; Peet, N.M.; Wolowacz, R.G.; Skerry, T.M.; Grabowski, P.S. Tetracyclines Induce Apoptosis in Osteoclasts. Bone 2000, 27, 75–80. [Google Scholar] [CrossRef]
- Holmes, S.G.; Still, K.; Buttle, D.J.; Bishop, N.J.; Grabowski, P.S. Chemically Modified Tetracyclines Act through Multiple Mechanisms Directly on Osteoclast Precursors. Bone 2004, 35, 471–478. [Google Scholar] [CrossRef]
- Everts, V.; Delaissé, J.M.; Korper, W.; Beertsen, W. Cysteine Proteinases and Matrix Metalloproteinases Play Distinct Roles in the Subosteoclastic Resorption Zone. J. Bone Min. Res. 1998, 13, 1420–1430. [Google Scholar] [CrossRef]
- Ramamurthy, N.S.; Rifkin, B.R.; Greenwald, R.A.; Xu, J.; Liu, Y.; Turner, G.; Golub, L.M.; Vernillo, A.T. Inhibition of Matrix Metalloproteinase-Mediated Periodontal Bone Loss in Rats: Tetracyclines. J. Periodontol. 2002, 73, 726–734. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Zhang, P.; Zhang, C.; An, B.; Zhu, Z. Tetracyclines Inhibit Rat Osteoclast Formation and Activity in Vitro and Affect Bone Turnover in Young Rats In Vivo. Calcif. Tissue Int. 2010, 86, 163–171. [Google Scholar] [CrossRef]
- Bain, S.; Ramamurthy, N.S.; Impeduglia, T.; Scolman, S.; Golub, L.M.; Rubin, C. Tetracycline Prevents Cancellous Bone Loss and Maintains Near-Normal Rates of Bone Formation in Streptozotocin Diabetic Rats. Bone 1997, 21, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Gomes, P.S.; Fernandes, M.H. Effect of Therapeutic Levels of Doxycycline and Minocycline in the Proliferation and Differentiation of Human Bone Marrow Osteoblastic Cells. Arch. Oral Biol. 2007, 52, 251–259. [Google Scholar] [CrossRef]
- Park, J.-B. Effects of Doxycycline, Minocycline, and Tetracycline on Cell Proliferation, Differentiation, and Protein Expression in Osteoprecursor Cells. J. Craniofac. Surg. 2011, 22, 1839–1842. [Google Scholar] [CrossRef] [PubMed]
- Golub, L.M.; Ramamurthy, N.S.; Llavaneras, A.; Ryan, M.E.; Lee, H.M.; Liu, Y.; Bain, S.; Sorsa, T. A Chemically Modified Nonantimicrobial Tetracycline (CMT-8) Inhibits Gingival Matrix Metalloproteinases, Periodontal Breakdown, and Extra-Oral Bone Loss in Ovariectomized Rats. Ann. N. Y. Acad. Sci. 1999, 878, 290–310. [Google Scholar] [CrossRef]
- Kilkenny, C.; Browne, W.; Cuthill, I.C.; Emerson, M.; Altman, D.G. NC3Rs Reporting Guidelines Working Group Animal Research: Reporting in Vivo Experiments: The ARRIVE Guidelines. Br. J. Pharm. 2010, 160, 1577–1579. [Google Scholar] [CrossRef]
- Erben, R.G. Embedding of Bone Samples in Methylmethacrylate: An Improved Method Suitable for Bone Histomorphometry, Histochemistry, and Immunohistochemistry. J. Histochem. Cytochem. 1997, 45, 307–313. [Google Scholar] [CrossRef] [Green Version]
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2009; ISBN 978-0-387-98140-6. [Google Scholar]
- Messora, M.R.; Nagata, M.J.; Dornelles, R.C.M.; Bomfim, S.R.M.; Furlaneto, F.A.C.; De Melo, L.G.N.; Deliberador, T.M.; Bosco, A.F.; Garcia, V.G.; Fucini, S.E. Bone healing in critical-size defects treated with platelet-rich plasma activated by two different methods. A histologic and histometric study in rat calvaria. J. Periodontal Res. 2008, 43, 723–729. [Google Scholar] [CrossRef]
- Gomes, P.S.; Fernandes, M.H. Rodent Models in Bone-Related Research: The Relevance of Calvarial Defects in the Assessment of Bone Regeneration Strategies. Lab. Anim. 2011, 45, 14–24. [Google Scholar] [CrossRef]
- Bosch, C.; Melsen, B.; Vargervik, K. Importance of the Critical-Size Bone Defect in Testing Bone-Regenerating Materials. J. Craniofac. Surg. 1998, 9, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Lundgren, A.K.; Sennerby, L.; Lundgren, D. Guided Jaw-Bone Regeneration Using an Experimental Rabbit Model. Int. J. Oral Maxillofac. Surg. 1998, 27, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Rakhmatia, Y.D.; Ayukawa, Y.; Furuhashi, A.; Koyano, K. Current Barrier Membranes: Titanium Mesh and Other Membranes for Guided Bone Regeneration in Dental Applications. J. Prosthodont. Res. 2013, 57, 3–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Majzoub, Z.; Berengo, M.; Giardino, R.; Aldini, N.N.; Cordioli, G. Role of Intramarrow Penetration in Osseous Repair: A Pilot Study in the Rabbit Calvaria. J. Periodontol. 1999, 70, 1501–1510. [Google Scholar] [CrossRef] [PubMed]
- Tamura, T.; Fukase, Y.; Goke, E.; Yamada, Y.; Sato, S.; Nishiyama, M.; Ito, K. Three-Dimensional Evaluation for Augmented Bone Using Guided Bone Regeneration. J Periodontal Res. 2005, 40, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Slotte, C.; Lundgren, D.; Sennerby, L. Bone Morphology and Vascularization of Untreated and Guided Bone Augmentation-Treated Rabbit Calvaria: Evaluation of an Augmentation Model. Clin. Oral Implant. Res. 2005, 16, 228–235. [Google Scholar] [CrossRef]
- Seol, K.-Y.; Kim, S.-G.; Kim, H.-K.; Moon, S.-Y.; Kim, B.-O.; Ahn, J.-M.; Jang, H.-S.; Kim, H.-J.; Min, J.-B.; Lee, B.-J.; et al. Effects of decortication in the treatment of bone defect around particulate dentin-coated implants: An experimental pilot study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2009, 108, 529–536. [Google Scholar] [CrossRef] [PubMed]
- de Carvalho, P.S.; Vasconcellos, L.W.; Pi, J. Influence of bed preparation on the incorporation of autogenous bone grafts: A study in dogs. Int. J. Oral Maxillofac. Implant. 2000, 15, 565–570. [Google Scholar]
- Min, S.; Sato, S.; Murai, M.; Okuno, K.; Fujisaki, Y.; Yamada, Y.; Ito, K. Effects of marrow penetration on bone augmentation within a titanium cap in rabbit calvarium. J. Periodontol. 2007, 78, 1978–1984. [Google Scholar] [CrossRef]
- Viboolvorakul, S.; Niimi, H.; Wongeak-in, N.; Eksakulkla, S.; Patumraj, S. Increased Capillary Vascularity in the Femur of Aged Rats by Exercise Training. Microvasc. Res. 2009, 78, 459–463. [Google Scholar] [CrossRef]
- Lindbom, L.; Tuma, R.F.; Arfors, K.E. Influence of Oxygen on Perfused Capillary Density and Capillary Red Cell Velocity in Rabbit Skeletal Muscle. Microvasc. Res. 1980, 19, 197–208. [Google Scholar] [CrossRef] [PubMed]
- Metz, L.N.; Martin, R.B.; Turner, A.S. Histomorphometric Analysis of the Effects of Osteocyte Density on Osteonal Morphology and Remodeling. Bone 2003, 33, 753–759. [Google Scholar] [CrossRef] [PubMed]
- Qiu, S.; Rao, D.S.; Palnitkar, S.; Parfitt, A.M. Relationships between Osteocyte Density and Bone Formation Rate in Human Cancellous Bone. Bone 2002, 31, 709–711. [Google Scholar] [CrossRef] [PubMed]
- Buckwalter, J.A.; Glimcher, M.J.; Cooper, R.R.; Recker, R. Bone biology. Part I: Structure, blood supply, cells, matrix, and mineralization. J. Bone Jt. Surg.—Ser. A 1995, 77, 1256–1275. [Google Scholar] [CrossRef]
- Turner, R.T. Cancellous Bone Turnover in Growing Rats: Time-Dependent Changes in Association between Calcein Label and Osteoblasts. J. Bone Min. Res. 1994, 9, 1419–1424. [Google Scholar] [CrossRef]
- Kinugawa, S.; Koide, M.; Kobayashi, Y.; Mizoguchi, T.; Ninomiya, T.; Muto, A.; Kawahara, I.; Nakamura, M.; Yasuda, H.; Takahashi, N.; et al. Tetracyclines Convert the Osteoclastic-Differentiation Pathway of Progenitor Cells to Produce Dendritic Cell-like Cells. J. Immunol. 2012, 188, 1772–1781. [Google Scholar] [CrossRef] [Green Version]
- Udagawa, N.; Koide, M.; Nakamura, M.; Takahashi, N. Minocycline to Be Used a Potential Anti-Bone Resorption Agents Due to the Suppression of Osteoclastic Bone Resorption. J. Oral Biosci. 2013, 55, 16–22. [Google Scholar] [CrossRef]
- Silva, A.C.; Oliveira, M.R.; Amaral, L.F.A.; Ferreira, S.; Garcia, I.R.; Mariano, R.C. Effect of Doxycycline in Gel Form on Bone Regeneration: Histomorphometric and Tomographic Study in Rat Calvaria. J. Periodontol. 2016, 87, 74–82. [Google Scholar] [CrossRef]
- Florencio-Silva, R.; Sasso, G.R.d.S.; Sasso-Cerri, E.; Simões, M.J.; Cerri, P.S. Biology of Bone Tissue: Structure, Function, and Factors That Influence Bone Cells. Biomed Res. Int. 2015, 2015, 421746. [Google Scholar] [CrossRef] [Green Version]
- Prideaux, M.; Findlay, D.M.; Atkins, G.J. Osteocytes: The Master Cells in Bone Remodelling. Curr. Opin Pharm. 2016, 28, 24–30. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No Minocycline-HCI | Minocycline-HCI | Perforation (p) | Minocycline (p) | Interaction (p) | ||||
|---|---|---|---|---|---|---|---|---|
| No Perforation | Bone Perforation | No Perforation | Bone Perforation | |||||
| Capillary density (cap/mm2) | 4 | 130.0 ± 60.0 | 138.6 ± 52.7 | 124.3 ± 55.5 | 140.1 ± 58.2 | 0.726 | 0.740 | 0.003 |
| 8 | 104.0 ± 52.4 | 88.6 ± 38.3 | 108.3 ± 49.8 | 139.1 ± 55.4 | ||||
| 16 | 88.1 ± 33.7 | 90.0 ± 43.9 | 96.3 ± 51.9 | 136.2 ± 42.6 | ||||
| Capillary density (cap/mm2) | 4 | 48.5 ± 5.8 | 46.8 ± 8 7 | 46.7 ± 7.7 | 48.7 ± 8.1 | 0.000 | 0.113 | 0.065 |
| 8 | 48.9 ± 6.3 | 42.6 ± 4.9 | 47.4 ± 4.5 | 48.0 ± 4.7 | ||||
| 16 | 40.7 ± 5.5 | 38 9 ± 4.9 | 47.5 ± 4.7 | 43 0 ± 4 6 | ||||
| Capillary density (cap/mm2) | 4 | 1106.9 ± 193.1 | 1166.8 ± 121.6 | 1203.7 ± 126.5 | 1154.1 ± 75.5 | 0.288 | 0.052 | 0.383 |
| 8 | 615.4 ± 35.6 | 596.4 ± 38.8 | 507.4 ± 29.6 | 491.9 ± 36.1 | ||||
| 16 | 447.6 ± 103.9 | 363.5 ± 31.0 | 376.2 ± 19.5 | 338.7 ± 29.2 | ||||
| No Minocycline-HCI | Minocycline-HCI | ||||
|---|---|---|---|---|---|
| No Perforation (C) | Perforation (P) | No Perforation (MIN) | Perforation (MIN + P) | ||
| 4 weeks | Newly generated tissue rate | 65.6 ± 15.5 | 73.5 ± 15.0 | 99.3 ± 7.6 ** | 111.6 ± 9.6 * |
| Osseous tissues (Σ) | 23.6 ± 4.0 | 40.2 ± 9.9 | 31.3 ± 6.4 ** | 51.5 ± 9.1 * | |
| Woven bone | 10.2 ± 2.6 | 17.3 ± 3.9 | 12.8 ± 4.2 | 16.3 ± 5.2 | |
| Lamellar bone | 13.0 ± 2.8 | 22.2 ± 7.5 | 17.4 ± 6.0 | 31.8 ± 9.6 | |
| Bone Marrow | 0.4 ± 0.7 | 0.7 ± 11.2 | 1.2 ± 1.7 | 3.4 ± 3.3 | |
| Other | |||||
| Connective tissue | 66.3 ± 5.7 | 55.2 ± 9.9 | 63.1 ± 8.7 | 44.2 ± 9.4 | |
| Granulation tissue/Blood clot | 10.1 ± 6.3 | 4.6 ± 4.2 | 5.6 ± 4.5 | 4.3 ± 3.9 | |
| 8 weeks | Newly generated tissue rate | 82.9 ± 21.9 | 120.7 ± 52.1 | 116.9 ± 17.4 * | 253.6 ± 21.7 ** |
| Osseous tissues (Σ) | 46.5 ± 5.9 | 56.9 ± 7.3 | 56.4 ± 8.3 ** | 70.1 ± 5.9 ** | |
| Woven bone | 8.2 ± 1.9 | 12.7 ± 2.5 | 9.9 ± 2.7 | 12.1 ± 2.5 | |
| Lamellar bone | 33.8 ± 5.4 | 39.0 ± 6.1 | 43.2 ± 7.1 | 50.9 ± 5.8 | |
| Bone Marrow | 4.5 ± 3.4 | 5.2 ± 1.4 | 3.3 ± 2.7 | 7.2 ± 3.1 | |
| Other | |||||
| Connective tissue | 48.7 ± 6.6 | 41.1 ± 7.6 | 40.9 ± 8.6 | 28.7 ± 6.4 | |
| Granulation tissue/Blood clot | 4.7 ± 3.1 | 2.0 ± 2.6 | 2.8 ± 2.8 | 1.3 ± 2.1 | |
| 16 weeks | Newly generated tissue rate | 137.8 ± 25.8 | 172.6 ± 41.7 | 182.7 ± 47.3 | 253.9 ± 38.9 * |
| Osseous tissues (Σ) | 68.4 ± 6.7 | 77.6 ± 9.5 | 77.9 ± 6.3 ** | 87.2 ± 8.9 ** | |
| Woven bone | 7.1 ± 1.9 | 9.7 ± 2.2 | 10.1 ± 2.3 | 11.5 ± 2.0 | |
| Lamellar bone | 52.6 ± 5.6 | 58.9 ± 7.2 | 59.2 ± 5.5 | 66.1 ± 8.8 | |
| Bone Marrow | 8.6 ± 2.2 | 9.0 ± 2.5 | 8.5 ± 2.8 | 9.6 ± 2.7 | |
| Other | |||||
| Connective tissue | 29.7 ± 7.5 | 22.0 ± 9.5 | 21.3 ± 12.8 | 12.4 ± 9.3 | |
| Granulation tissue/Blood clot | 1.9 ± 2.4 | 0.4 ± 1.0 | 0.8 ± 1.7 | 0.4 ± 1.2 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biewer, B.; Rompen, E.; Mittelbronn, M.; Hammer, G.P.; Quatresooz, P.; Borgmann, F.K. Effects of Minocycline Hydrochloride as an Adjuvant Therapy for a Guided Bone Augmentation Procedure in The Rat Calvarium. Dent. J. 2023, 11, 92. https://doi.org/10.3390/dj11040092
Biewer B, Rompen E, Mittelbronn M, Hammer GP, Quatresooz P, Borgmann FK. Effects of Minocycline Hydrochloride as an Adjuvant Therapy for a Guided Bone Augmentation Procedure in The Rat Calvarium. Dentistry Journal. 2023; 11(4):92. https://doi.org/10.3390/dj11040092
Chicago/Turabian StyleBiewer, Bob, Eric Rompen, Michel Mittelbronn, Gaël P. Hammer, Pascale Quatresooz, and Felix Kleine Borgmann. 2023. "Effects of Minocycline Hydrochloride as an Adjuvant Therapy for a Guided Bone Augmentation Procedure in The Rat Calvarium" Dentistry Journal 11, no. 4: 92. https://doi.org/10.3390/dj11040092
APA StyleBiewer, B., Rompen, E., Mittelbronn, M., Hammer, G. P., Quatresooz, P., & Borgmann, F. K. (2023). Effects of Minocycline Hydrochloride as an Adjuvant Therapy for a Guided Bone Augmentation Procedure in The Rat Calvarium. Dentistry Journal, 11(4), 92. https://doi.org/10.3390/dj11040092