
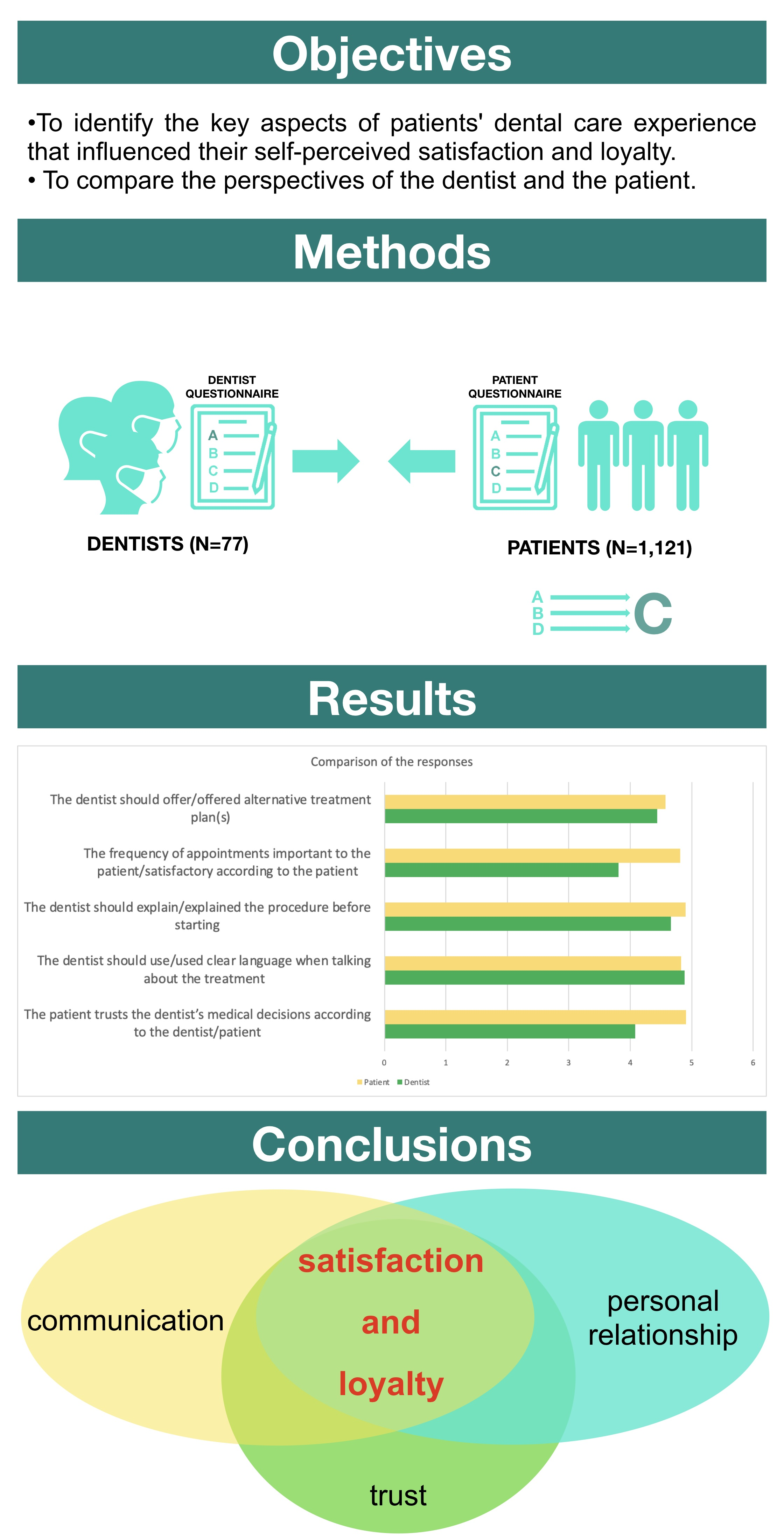
Factors Influencing Patient Satisfaction and Loyalty as Perceived by Dentists and Their Patients

 , ,
, ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Participants, Study Procedures, and Data Processing
2.2. The Questionnaires
2.2.1. The Patient Questionnaires
2.2.2. The Dentist Questionnaires
2.2.3. Pre-Testing and Psychometric Characteristics
2.3. Statistical Analysis
2.3.1. Descriptive Statistics and Hypothesis Tests
2.3.2. Dentist-Patient Comparisons
3. Results
3.1. The Study Population
3.2. “I Would Recommend My Dentist to Others”—Satisfaction
3.3. “I Am Very Committed to Continuing a Relationship with My Dentist”—Loyalty
3.4. Agreement/Disagreement between the Dentists’ and Their Patients’ Responses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, H.L.; Huang, J.Y.; Howng, S.L. The effect on patient loyalty of service quality, patient visit experience and perceived switching costs: Lessons from one Taiwan university hospital. Health Serv. Manag. Res. 2011, 24, 29–36. [Google Scholar] [CrossRef]
- Zolnierek, K.B.; Dimatteo, M.R. Physician communication and patient adherence to treatment: A meta-analysis. Med. Care 2009, 47, 826–834. [Google Scholar] [CrossRef]
- Schmid, M.; Wolf, R.C.; Freudenmann, R.W.; Schönfeldt-Lecuona, C. Tomophobia, the phobic fear caused by an invasive medical procedure—An emerging anxiety disorder: A case report. J. Med. Case Rep. 2009, 3, 131. [Google Scholar] [CrossRef]
- Hollander, M.A.G.; Greene, M.G. A conceptual framework for understanding iatrophobia. Patient Educ. Couns. 2019, 102, 2091–2096. [Google Scholar] [CrossRef] [PubMed]
- Jha, A.; Holla, R.; Satish, K.P.; Kundolil, F.S.; Goel, P.; Jaiswal, S.; Kumar, D.N.; Dasgupta, A. Trypanophobia among medical students—An overlooked concern. Clin. Epidemiol. Glob. Health 2023, 20, 101257. [Google Scholar] [CrossRef]
- Pioli, M.R.; Ritter, A.M.; de Faria, A.P.; Modolo, R. White coat syndrome and its variations: Differences and clinical impact. Integr. Blood Press. Control 2018, 11, 73–79. [Google Scholar] [CrossRef]
- Aburas, S.; Pfaffeneder-Mantai, F.; Hofmann, A.; Meller, O.; Schneider, B.; Turhani, D. Dentophobia and dental treatment: An umbrella review of the published literature. Spec. Care Dentist. 2023, 43, 163–173. [Google Scholar] [CrossRef]
- Oosterink, F.M.; de Jongh, A.; Hoogstraten, J. Prevalence of dental fear and phobia relative to other fear and phobia subtypes. Eur. J. Oral Sci. 2009, 117, 135–143. [Google Scholar] [CrossRef]
- de Jongh, A.; Muris, P.; Schoenmakers, N.; ter Horst, G. Negative cognitions of dental phobics: Reliability and validity of the dental cognitions questionnaire. Behav. Res. Ther. 1995, 33, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Liinavuori, A.; Tolvanen, M.; Pohjola, V.; Lahti, S. Longitudinal interrelationships between dental fear and dental attendance among adult Finns in 2000–2011. Community Dent. Oral Epidemiol. 2019, 47, 309–315. [Google Scholar] [CrossRef]
- Pohjola, V.; Lahti, S.; Vehkalahti, M.M.; Tolvanen, M.; Hausen, H. Association between dental fear and dental attendance among adults in Finland. Acta Odontol. Scand. 2007, 65, 224–230. [Google Scholar] [CrossRef]
- Platonova, E.A.; Kennedy, K.N.; Shewchuk, R.M. Understanding patient satisfaction, trust, and loyalty to primary care physicians. Med. Care Res. Rev. 2008, 65, 696–712. [Google Scholar] [CrossRef]
- Unal, O.; Akbolat, M.; Amarat, M. The influence of patient-physician communication on physician loyalty and hospital loyalty of the patient. Pak. J. Med. Sci. 2018, 34, 999–1003. [Google Scholar] [CrossRef]
- Liu, S.; Li, G.; Liu, N.; Hongwei, W. The Impact of Patient Satisfaction on Patient Loyalty with the Mediating Effect of Patient Trust. Inquiry 2021, 58, 469580211007221. [Google Scholar] [CrossRef]
- AlOmari, F.; Hamid, A.A.B. Strategies to improve patient loyalty and medication adherence in Syrian healthcare setting: The mediating role of patient satisfaction. PLoS ONE 2022, 17, e0272057. [Google Scholar] [CrossRef]
- Little, P.; Everitt, H.; Williamson, I.; Warner, G.; Moore, M.; Gould, C.; Ferrier, K.; Payne, S. Observational study of effect of patient centredness and positive approach on outcomes of general practice consultations. BMJ 2001, 323, 908–911. [Google Scholar] [CrossRef]
- Lucarotti, P.S.; Burke, F.J. Factors influencing patients’ continuing attendance at a given dentist. Br. Dent. J. 2015, 218, E13. [Google Scholar] [CrossRef]
- Caruana, A.; Fenech, N. The Effect of Perceived Value and Overall Satisfaction on Loyalty: A Study among Dental Patients. J. Med. Market. 2005, 5, 245–255. [Google Scholar] [CrossRef]
- Holt, V.P.; McHugh, K. Factors influencing patient loyalty to dentist and dental practice. Br. Dent. J. 1997, 183, 365–370. [Google Scholar] [CrossRef]
- Riley, J.L., 3rd; Gordan, V.V.; Hudak-Boss, S.E.; Fellows, J.L.; Rindal, D.B.; Gilbert, G.H. Concordance between patient satisfaction and the dentist’s view: Findings from The National Dental Practice-Based Research Network. J. Am. Dent. Assoc. 2014, 145, 355–362. [Google Scholar] [CrossRef]
- Gurdal, P.; Cankaya, H.; Onem, E.; Dincer, S.; Yilmaz, T. Factors of patient satisfaction/dissatisfaction in a dental faculty outpatient clinic in Turkey. Community Dent. Oral Epidemiol. 2000, 28, 461–469. [Google Scholar] [CrossRef] [PubMed]
- Mellor, A.C.; Milgrom, P. Dentists’ attitudes toward frustrating patient visits: Relationship to satisfaction and malpractice complaints. Community Dent. Oral Epidemiol. 1995, 23, 15–19. [Google Scholar] [CrossRef]
- Kiesler, D.J.; Auerbach, S.M. Optimal matches of patient preferences for information, decision-making and interpersonal behavior: Evidence, models and interventions. Patient Educ. Couns. 2006, 61, 319–341. [Google Scholar] [CrossRef] [PubMed]
- Murray, E.; Pollack, L.; White, M.; Lo, B. Clinical decision-making: Patients’ preferences and experiences. Patient Educ. Couns. 2007, 65, 189–196. [Google Scholar] [CrossRef] [PubMed]
- de Haes, H. Dilemmas in patient centeredness and shared decision making: A case for vulnerability. Patient Educ. Couns. 2006, 62, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Szabó, R.; Farkas, G.; Keszeg, M.; Eördegh, G.; Buzás, N.; Antal, M. The role of the “compromise effect” in dental treatment choice. A pilot study in 676 Hungarian volunteers. Orv. Hetil. 2019, 160, 1503–1509. [Google Scholar] [CrossRef]
- Reissmann, D.R.; Bellows, J.C.; Kasper, J. Patient Preferred and Perceived Control in Dental Care Decision Making. JDR Clin. Trans. Res. 2019, 4, 151–159. [Google Scholar] [CrossRef]
- Lin, W.; Yin, W. Impacts of service quality, brand image, and perceived value on outpatient’s loyalty to China’s private dental clinics with service satisfaction as a mediator. PLoS ONE 2022, 17, e0269233. [Google Scholar] [CrossRef]
- Palaiologou, A.; Kotsakis, G.A. Dentist-Patient Communication of Treatment Outcomes in Periodontal Practice: A Need for Dental Patient-Reported Outcomes. J. Evid. Based Dent. Pract. 2020, 20, 101443. [Google Scholar] [CrossRef]
- Newton, J.T. Dentist/patient communication: A review. Dent. Update 1995, 22, 118–122. [Google Scholar]
- Mataki, S. Patient-dentist relationship. J. Med. Dent. Sci. 2000, 47, 209–214. [Google Scholar]
- Sondell, K.; Soderfeldt, B.; Palmqvist, S. Dentist-patient communication and patient satisfaction in prosthetic dentistry. Int. J. Prosthodont. 2002, 15, 28–37. [Google Scholar]
- Rozier, R.G.; Horowitz, A.M.; Podschun, G. Dentist-patient communication techniques used in the United States: The results of a national survey. J. Am. Dent. Assoc. 2011, 142, 518–530. [Google Scholar] [CrossRef] [PubMed]
- Otte, S.V. Improved Patient Experience and Outcomes: Is Patient-Provider Concordance the Key? J. Patient Exp. 2022, 9, 23743735221103033. [Google Scholar] [CrossRef]
- Cooper, L.A.; Roter, D.L.; Johnson, R.L.; Ford, D.E.; Steinwachs, D.M.; Powe, N.R. Patient-centered communication, ratings of care, and concordance of patient and physician race. Ann. Intern. Med. 2003, 139, 907–915. [Google Scholar] [CrossRef]
- Street, R.L., Jr.; O’Malley, K.J.; Cooper, L.A.; Haidet, P. Understanding concordance in patient-physician relationships: Personal and ethnic dimensions of shared identity. Ann. Fam. Med. 2008, 6, 198–205. [Google Scholar] [CrossRef]
- Hall, J.A.; Irish, J.T.; Roter, D.L.; Ehrlich, C.M.; Miller, L.H. Gender in medical encounters: An analysis of physician and patient communication in a primary care setting. Health Psychol. 1994, 13, 384–392. [Google Scholar] [CrossRef]
- Thornton, R.L.; Powe, N.R.; Roter, D.; Cooper, L.A. Patient-physician social concordance, medical visit communication and patients’ perceptions of health care quality. Patient Educ. Couns. 2011, 85, e201–e208. [Google Scholar] [CrossRef]
- Elderkin-Thompson, V.; Waitzkin, H. Differences in clinical communication by gender. J. Gen. Intern. Med. 1999, 14, 112–121. [Google Scholar] [CrossRef]
- Christen, R.N.; Alder, J.; Bitzer, J. Gender differences in physicians’ communicative skills and their influence on patient satisfaction in gynaecological outpatient consultations. Soc. Sci. Med. 2008, 66, 1474–1483. [Google Scholar] [CrossRef]
- Al-Mobeeriek, A. Dentist-patient communication as perceived by patients in Riyadh, Saudi Arabia. Int. J. Occup. Med. Environ. Health 2012, 25, 89–96. [Google Scholar] [CrossRef]
- Lamprecht, R.; Struppek, J.; Heydecke, G.; Reissmann, D.R. Patients’ criteria for choosing a dentist: Comparison between a university-based setting and private dental practices. J. Oral Rehabil. 2020, 47, 1023–1030. [Google Scholar] [CrossRef]
- Sharma, N.; Patterson, P. Switching costs, alternative attractiveness and experience as moderators of relationship commitment in professional, consumer services. Int. J. Serv. Ind. Manag. 2000, 11, 470–490. [Google Scholar] [CrossRef]
- Lahti, S.; Tuutti, H.; Hausen, H.; Kääriäinen, R. Dentist and patient opinions about the ideal dentist and patient-developing a compact questionnaire. Community Dent. Oral Epidemiol. 1992, 20, 229–234. [Google Scholar] [CrossRef]
- Lahti, S.; Tuutti, H.; Hausen, H.; Käärlänen, R. Patients’ expectations of an ideal dentist and their views concerning the dentist they visited: Do the views conform to the expectations and what determines how well they conform? Community Dent. Oral Epidemiol. 1996, 24, 240–244. [Google Scholar] [CrossRef]
- Lahti, S.; Verkasalo, M.; Hausen, H.; Tuutti, H. Ideal role behaviours as seen by dentists and patients themselves and by their role partners: Do they differ? Community Dent. Oral Epidemiol. 1996, 24, 245–248. [Google Scholar]
- Burnham, T.; Frels, J.; Mahajan, V. Consumer switching costs: A typology, antecedents, and consequences. J. Acad. Mark. Sci. 2003, 31, 109–126. [Google Scholar] [CrossRef]
- Reichheld, F.F. The one number you need to grow. Harv. Bus. Rev. 2003, 81, 46–124. [Google Scholar]
- Oliver, R. Satisfaction: A Behavioral Perspective on the Customer; McGraw Hill: New York, NY, USA, 1996. [Google Scholar]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef]
- Jerant, A.; Bertakis, K.D.; Fenton, J.J.; Tancredi, D.J.; Franks, P. Patient-provider sex and race/ethnicity concordance: A national study of healthcare and outcomes. Med. Care 2011, 49, 1012–1020. [Google Scholar] [CrossRef]
- Armfield, J.M.; Heaton, L.J. Management of fear and anxiety in the dental clinic: A review. Aust. Dent. J. 2013, 58, 390–407. [Google Scholar] [CrossRef]
- Krist, A.H.; Tong, S.T.; Aycock, R.A.; Longo, D.R. Engaging Patients in Decision-Making and Behavior Change to Promote Prevention. Stud. Health Technol. Inform. 2017, 240, 284–302. [Google Scholar] [CrossRef]
- Murgic, L.; Hebert, P.C.; Sovic, S.; Pavlekovic, G. Paternalism and autonomy: Views of patients and providers in a transitional (post-communist) country. BMC Med. Ethics 2015, 16, 65. [Google Scholar] [CrossRef]
- Thompson, G.A.; Segura, J.; Cruz, D.; Arnita, C.; Whiffen, L.H. Cultural Differences in Patients’ Preferences for Paternalism: Comparing Mexican and American Patients’ Preferences for and Experiences with Physician Paternalism and Patient Autonomy. Int. J. Environ. Res. Public Health 2022, 19, 663. [Google Scholar] [CrossRef] [PubMed]
- Krupat, E.; Rosenkranz, S.L.; Yeager, C.M.; Barnard, K.; Putnam, S.M.; Inui, T.S. The practice orientations of physicians and patients: The effect of doctor-patient congruence on satisfaction. Patient Educ. Couns. 2000, 39, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Hall, J.A.; Roter, D.L. Medical communication and gender: A summary of research. J. Gend. Specif. Med. 1998, 1, 39–42. [Google Scholar]
- Schmid Mast, M.; Hall, J.A.; Roter, D.L. Disentangling physician sex and physician communication style: Their effects on patient satisfaction in a virtual medical visit. Patient Educ. Couns. 2007, 68, 16–22. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Item Pair | Topic | Dentist Mean (±SD) | Patient Mean (±SD) | |
|---|---|---|---|---|
| D5 | P8 | The patient trusts the dentist’s medical decisions according to the dentist/patient | 4.08 (±0.68) | 4.91 (±0.33) |
| D9 | P18 | The dentist should show/showed interest in the patient’s symptoms | 4.94 (±0.25) | 4.90 (±0.38) |
| D15 | P26 | Frequency of appointments important to patient/satisfactory according to patient | 3.81 (±0.90) | 4.81 (±0.50) |
| D16 | P27 | The quality of treatment is important to the patient/satisfactory according to patient | 4.70 (±0.59) | 4.94 (±0.27) |
| Item Pair | Topic | Dentist Mean (±SD) | Patient Mean (±SD) | |
|---|---|---|---|---|
| D5 | P8 | The patient trusts the dentist’s medical decisions according to the dentist/patient | 4.08 (±0.68) | 4.91 (±0.33) |
| D12 | P23 | The dentist should use/used clear language when talking about the treatment | 4.88 (±0.32) | 4.83 (±0.46) |
| D13 | P24 | The dentist should explain/explained the procedure before starting | 4.66 (±0.50) | 4.90 (±0.34) |
| D15 | P26 | The frequency of appointments important to the patient/satisfactory according to the patient | 3.81 (±0.90) | 4.81 (±0.50) |
| D17 | P29 | The dentist should offer/offered alternative treatment plan(s) | 4.44 (±0.87) | 4.57 (±0.80) |
| PATIENTS | |||
|---|---|---|---|
| Item No. | Item | Mean Score | |
| 27 | I am satisfied with the quality of the treatment. | 4.94 | 75th percentile |
| 11 | I would recommend my dentist to others. | 4.92 | |
| 8 | I trust this dentist’s judgments about my medical care. | 4.91 | |
| 20 | The dentist explained clearly what the problem was. | 4.91 | |
| 28 | I am satisfied with the explanation given by the dentist. | 4.91 | |
| 18 | The dentist was interested when I spoke about my symptoms. | 4.90 | |
| 24 | The dentist told me what s/he was going to do before starting the procedure. | 4.90 | |
| 7 | I have developed a personal relationship with my current dentist | 4.27 | 25th percentile |
| 9 | I’m confident that my dentist knows me. | 4.22 | |
| 14 | I possess good knowledge of health care services. | 4.00 | |
| 19 | The dentist was interested in the effects of the problem on my family or private life. | 3.91 | |
| 13 | For me, the costs in time/money/effort to switch dentists are high. | 3.59 | |
| 15 | I am quite experienced in the health care area. | 3.47 | |
| DENTISTS | |||
| 9 | It matters to the patients that their dentist shows interest when they speak about their symptoms. | 4.94 | 75th percentile |
| 12 | It matters to the patients that their dentist uses words that are understandable in talking about their dental care. | 4.88 | |
| 10 | It matters to the patients that their dentist explains clearly what the problem is. | 4.87 | |
| 18 | It matters to the patients that their dentist discusses the treatment plan with them. | 4.77 | |
| 12 | It matters to the patients that the dentist encourages them to ask questions about their treatment. | 4.05 | 25th percentile |
| 13 | The duration of an appointment matters to the patients. | 4.05 | |
| 14 | The frequency of appointments matters to the patients. | 3.81 | |
| 15 | Most of the patients possess good knowledge of health care services. | 3.48 | |
| Item Pair | Topic | Full Agreement N (%) | Full Disagreement N (%) | Degree of Disagreement (Mean) | SD | 95% CI Lower Limit | 95% CI Upper Limit | |
|---|---|---|---|---|---|---|---|---|
| D5 | P8 | The patient trusts the dentist’s medical decisions according to the dentist/patient | 291 (25.9%) | 0 (0%) | 0.90 | 0.80 | 0.85 | 0.95 |
| D8 | P14 | The patient is informed about healthcare according to the dentist/patient | 300 (26.7%) | 4 (0.4%) | 0.48 | 1.23 | 0.41 | 0.55 |
| D15 | P34 | The frequency of visits is important to the patient/satisfactory according to the patient | 305 (27.2%) | 0 (0%) | 1.03 | 1.02 | 0.97 | 1.09 |
| D14 | P33 | The duration of visits is important to the patient/satisfactory according to the patient | 398 (35.5%) | 0 (0%) | 0.86 | 0.86 | 0.80 | 0.92 |
| D11 | P30 | The dentist should encourage/encouraged questions about treatment | 407 (36.3%) | 0 (0%) | 0.59 | 0.57 | 0.53 | 0.66 |
| D6 | P11 | The patient would recommend the dentist to others according to the dentist/patient | 570 (50.8%) | 0 (0%) | 0.41 | 0.64 | 0.37 | 0.44 |
| D7 | P12 | The patient is strongly committed according to the dentist/patient | 582 (51.9%) | 14 (1.2%) | 0.24 | 0.96 | 0.18 | 0.29 |
| D17 | P37 | The dentist should offer/offered alternative treatment plan(s) | 590 (52.6%) | 17 (1.5%) | 0.04 | 1.11 | −0.02 | 0.11 |
| D19 | P39 | The dentist and the patient should agree/agreed on the treatment plan | 722 (64.3%) | 2(0.2%) | 0.23 | 0.66 | 0.19 | 0.27 |
| D13 | P32 | The dentist should explain/explained the procedure before starting | 728 (64.9%) | 0 (0%) | 0.26 | 0.55 | 0.23 | 0.30 |
| D16 | P35 | The quality of treatment is important to the patient/satisfactory according to the patient | 770 (68.6%) | 0 (0%) | 0.31 | 0.77 | 0.27 | 0.36 |
| D18 | P38 | The dentist should discuss/discussed treatment plan with the patient | 824 (73.4%) | 0 (0%) | 0.14 | 0.59 | 0.11 | 0.17 |
| D12 | P31 | The dentist should use/used clear language when talking about the treatment | 863 (76.9%) | 0 (0%) | −0.06 | 0.57 | −0.09 | −0.02 |
| D10 | P28 | The dentist should explain/explained the problem with the teeth in an intelligible way | 935 (83.3%) | 1 (0.1%) | 0.03 | 0.47 | 0.00 | 0.05 |
| D9 | P26 | The dentist should show/showed interest in the patient’s symptoms | 958 (85.4%) | 1 (0.1%) | −0.03 | 0.47 | −0.05 | 0.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szabó, R.M.; Buzás, N.; Braunitzer, G.; Shedlin, M.G.; Antal, M.Á. Factors Influencing Patient Satisfaction and Loyalty as Perceived by Dentists and Their Patients. Dent. J. 2023, 11, 203. https://doi.org/10.3390/dj11090203
Szabó RM, Buzás N, Braunitzer G, Shedlin MG, Antal MÁ. Factors Influencing Patient Satisfaction and Loyalty as Perceived by Dentists and Their Patients. Dentistry Journal. 2023; 11(9):203. https://doi.org/10.3390/dj11090203
Chicago/Turabian StyleSzabó, Réka Magdolna, Norbert Buzás, Gábor Braunitzer, Michele Goldzieher Shedlin, and Mark Ádám Antal. 2023. "Factors Influencing Patient Satisfaction and Loyalty as Perceived by Dentists and Their Patients" Dentistry Journal 11, no. 9: 203. https://doi.org/10.3390/dj11090203
APA StyleSzabó, R. M., Buzás, N., Braunitzer, G., Shedlin, M. G., & Antal, M. Á. (2023). Factors Influencing Patient Satisfaction and Loyalty as Perceived by Dentists and Their Patients. Dentistry Journal, 11(9), 203. https://doi.org/10.3390/dj11090203