

The Long-Term Esthetic and Radiographic Outcome of Implants Placed in the Anterior Maxilla after Ridge Preservation, Combining Bovine Xenograft with Collagen Matrix

 and
and 
Abstract
:1. Introduction
2. Methods
2.1. Study Sample
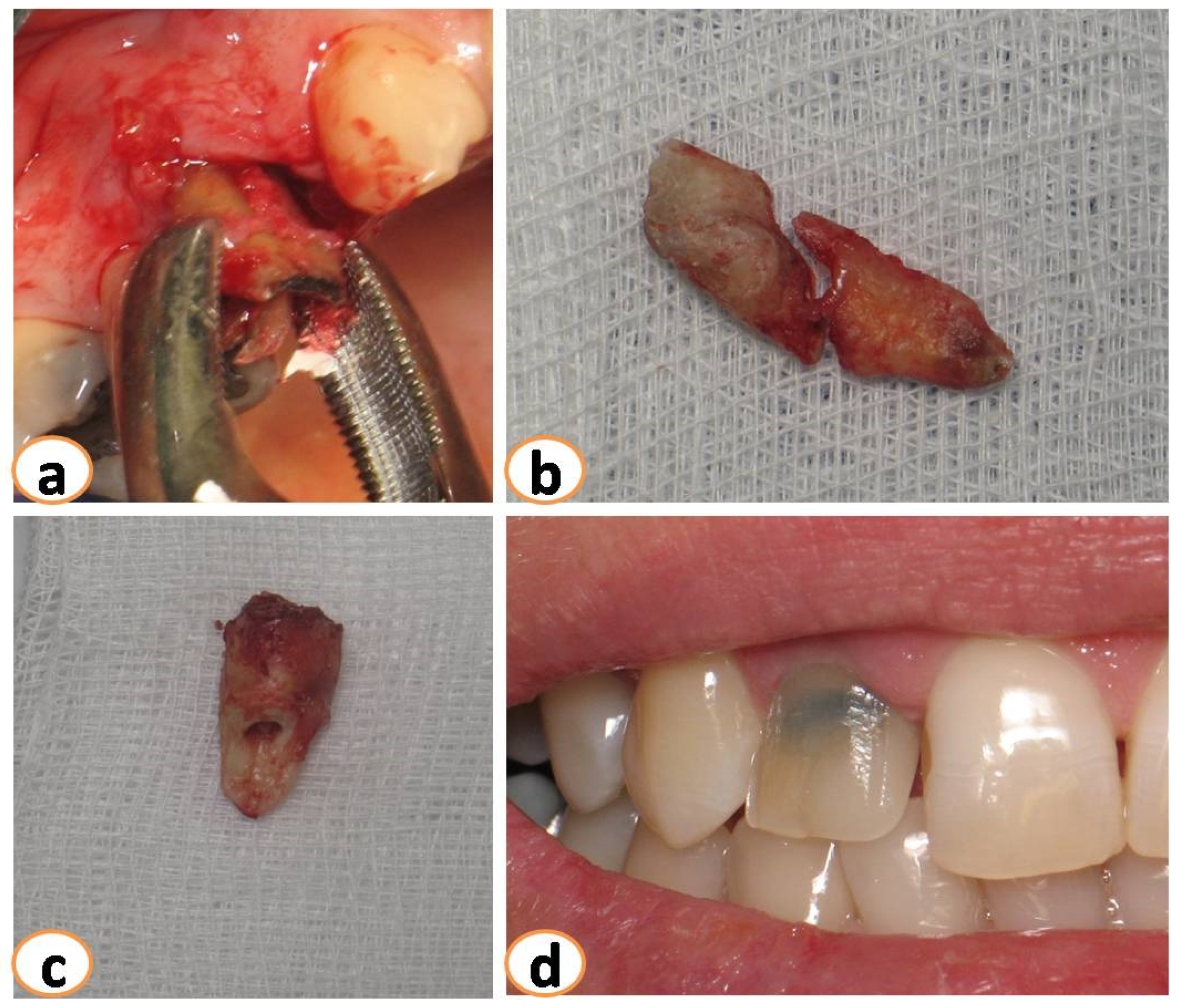
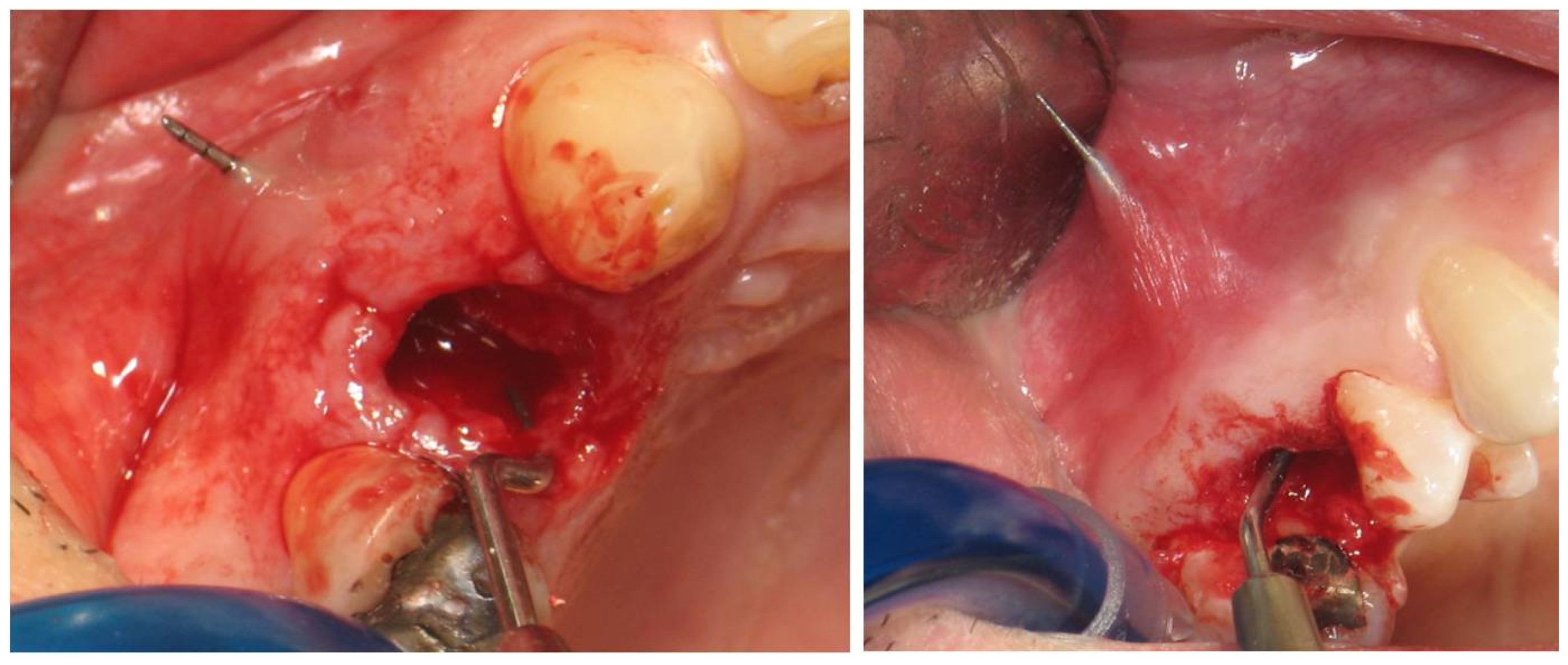
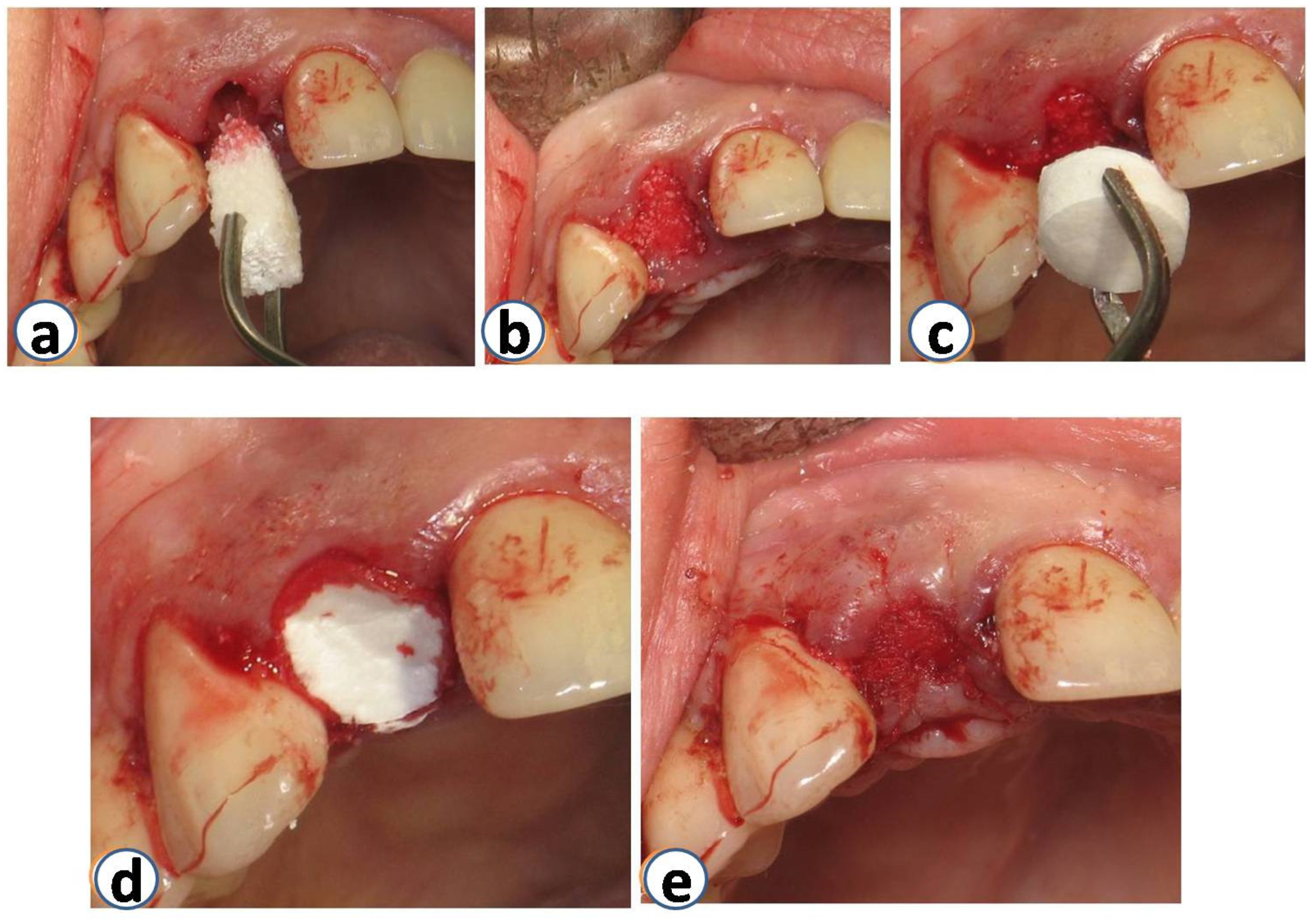
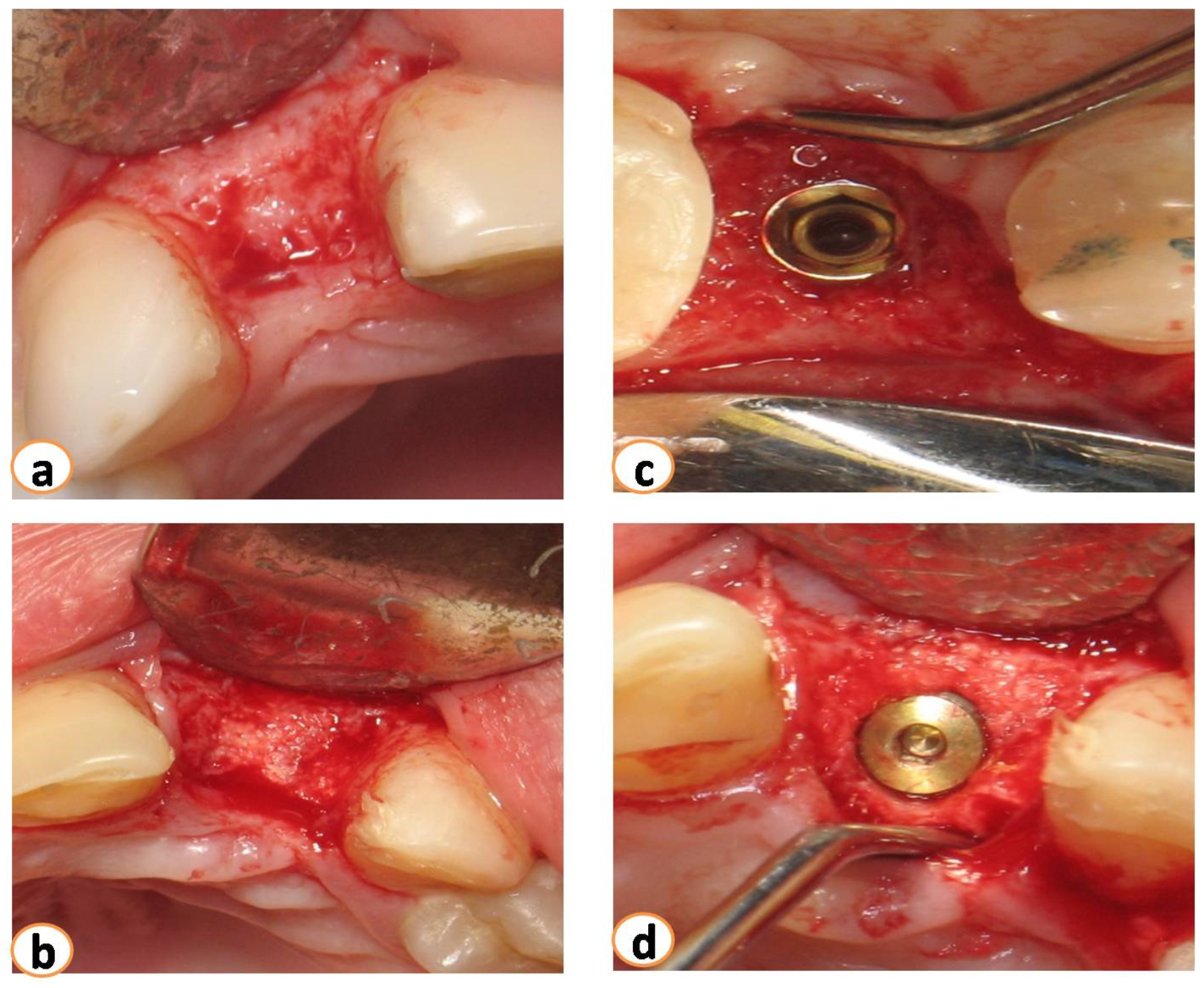
2.2. Surgical Procedures—Implant Rehabilitation
2.3. Infection and Pain Control
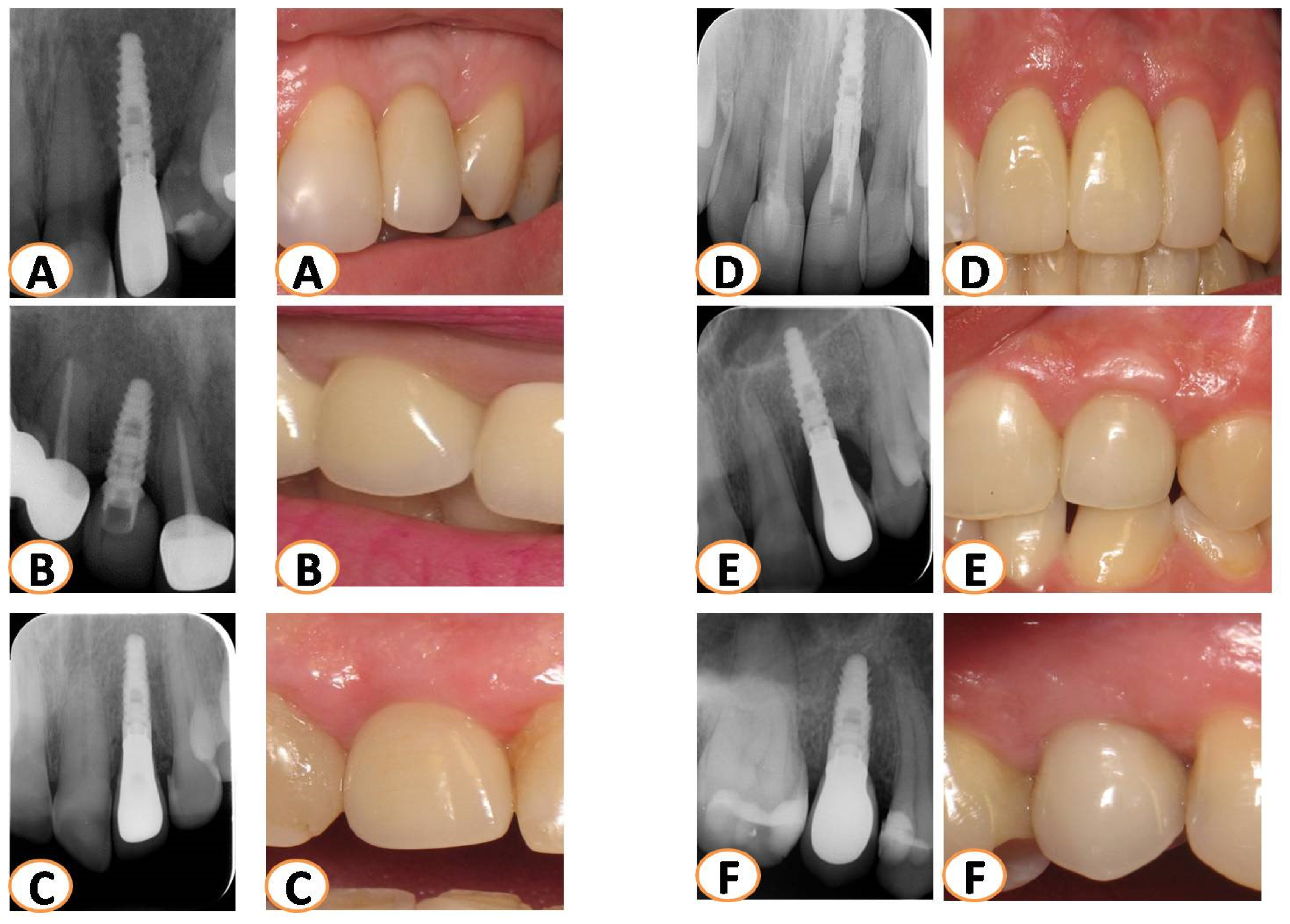
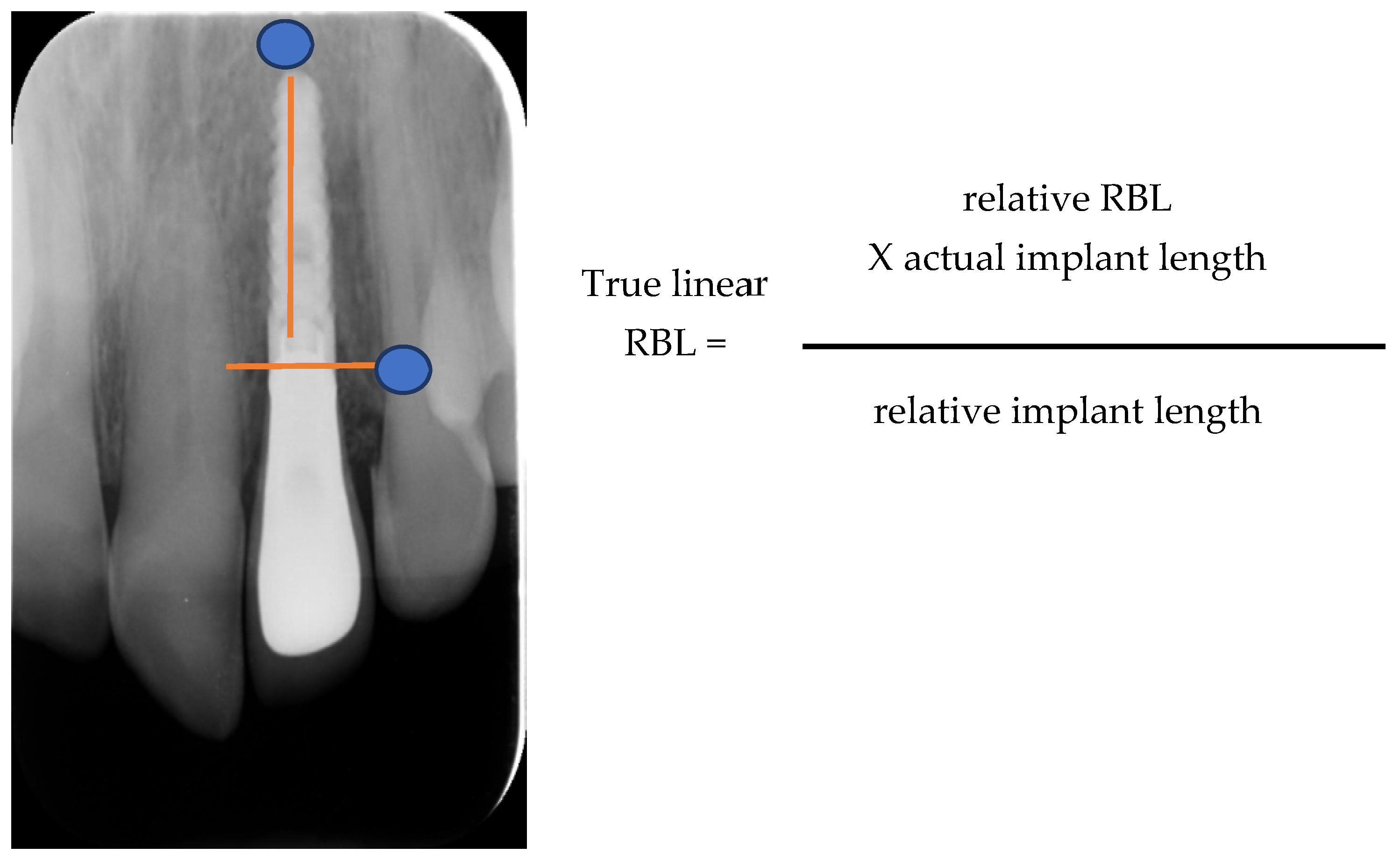
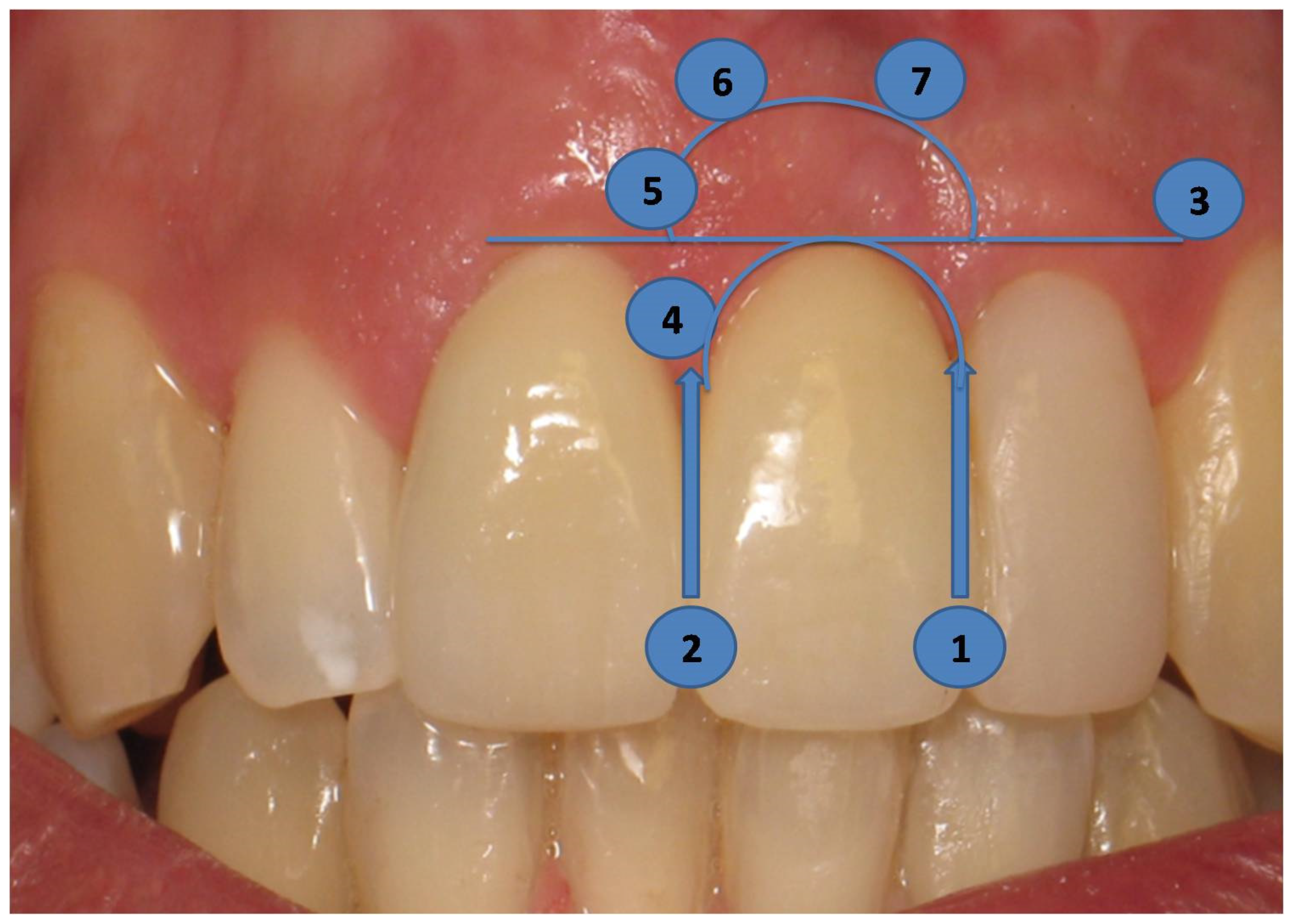
2.4. Long-Term Results of Soft Tissue Esthetic Outcome and Radiographic Evaluation
2.5. Statistical Analysis
3. Results
3.1. Radiographic Bone Loss
3.2. PES Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Araújo, M.G.; Silva, C.O.; Misawa, M.; Sukekava, F. Alveolar socket healing: What can we learn? Periodontology 2000 2015, 68, 122–134. [Google Scholar] [CrossRef] [PubMed]
- Botticelli, D.; Berglundh, T.; Lindhe, J. Hard-tissue alterations following immediate implant placement in extraction sites. J. Clin. Periodontol. 2004, 31, 820–828. [Google Scholar] [CrossRef]
- Farmer, M.; Darby, I. Ridge dimensional changes following single-tooth extraction in the aesthetic zone. Clin. Oral Implant. Res. 2014, 25, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Araujo, M.G.; Sukekava, F.; Wennstrom, J.L.; Lindhe, J. Ridge alterations following implant placement in fresh extraction sockets: An experimental study in the dog. J. Clin. Periodontol. 2005, 32, 645–652. [Google Scholar] [CrossRef]
- Thoma, D.S.; Benić, G.I.; Zwahlen, M.; Hämmerle, C.H.F.; Jung, R.E. A systematic review assessing soft tissue augmentation techniques. Clin. Oral Implant. Res. 2009, 20 (Suppl. S4), 146–165. [Google Scholar] [CrossRef] [PubMed]
- MacBeth, N.; Trullenque-Eriksson, A.; Donos, N.; Mardas, N. Hard and soft tissue changes following alveolar ridge preservation: A systematic review. Clin. Oral Implant. Res. 2017, 28, 982–1004. [Google Scholar] [CrossRef]
- Araújo, M.G.; Sukekava, F.; Wennström, J.L.; Lindhe, J. Tissue modeling following implant placement in fresh extraction sockets. Clin. Oral Implant. Res. 2006, 17, 615–624. [Google Scholar] [CrossRef]
- Ferrus, J.; Cecchinato, D.; Pjetursson, E.B.; Lang, N.P.; Sanz, M.; Lindhe, J. Factors influencing ridge alterations following immediate implant placement into extraction sockets. Clin. Oral Implant. Res. 2010, 21, 22–29. [Google Scholar] [CrossRef]
- Matarasso, S.; Salvi, G.E.; Siciliano, V.I.; Cafiero, C.; Blasi, A.; Lang, N.P. Dimensional ridge alterations following immediate implant placement in molar extraction sites: A six-month prospective cohort study with surgical re-entry. Clin. Oral Implant. Res. 2009, 20, 1092–1098. [Google Scholar] [CrossRef]
- Sanz, M.; Cecchinato, D.; Ferrús, J.; Pjetursson, E.B.; Lang, N.P.; Lindhe, J. A prospective, randomized-controlled clinical trial to evaluate bone preservation using implants with different geometry placed into extraction sockets in the maxilla. Clin. Oral Implant. Res. 2010, 21, 13–21. [Google Scholar] [CrossRef]
- Iocca, O.; Farcomeni, A.; Lopez, S.P.; Talib, H.S. Alveolar ridge preservation after tooth extraction: A Bayesian Network meta-analysis of grafting materials efficacy on prevention of bone height and width reduction. J. Clin. Periodontol. 2017, 44, 104–114. [Google Scholar] [CrossRef]
- Majzoub, J.; Ravidà, A.; Starch-Jensen, T.; Tattan, M.; Del Amo, F.S.-L. The Influence of Different Grafting Materials on Alveolar Ridge Preservation: A Systematic Review. J. Oral Maxillofac. Res. 2019, 10, e6. [Google Scholar] [CrossRef]
- De Angelis, P.; De Rosa, G.; Manicone, P.F.; De Giorgi, A.; Cavalcanti, C.; Speranza, A.; Grassi, R.; D’addona, A. Hard and soft tissue evaluation of alveolar ridge preservation compared to spontaneous healing: A retrospective clinical and volumetric analysis. Int. J. Implant. Dent. 2022, 8, 62. [Google Scholar] [CrossRef]
- Ucer, C.; Khan, R.S. Extraction Socket Augmentation with Autologous Platelet-Rich Fibrin (PRF): The Rationale for Socket Augmentation. Dent. J. 2023, 11, 196. [Google Scholar] [CrossRef]
- Araújo, M.G.; Liljenberg, B.; Lindhe, J. Dynamics of Bio-Oss® Collagen incorporation in fresh extraction wounds: An experimental study in the dog. Clin. Oral Implant. Res. 2010, 21, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Sbordone, C.; Toti, P.; Martuscelli, R.; Guidetti, F.; Ramaglia, L.; Sbordone, L. Retrospective volume analysis of bone remodeling after tooth extraction with and without deproteinized bovine bone mineral insertion. Clin. Oral Implant. Res. 2016, 27, 1152–1159. [Google Scholar] [CrossRef]
- Sivolella, S.; Botticelli, D.; Prasad, S.; Ricci, S.; Bressan, E.; Prasad, H. Evaluation and comparison of histologic changes and implant survival in extraction sites immediately grafted with two different xenografts: A randomized clinical pilot study. Clin. Oral Implant. Res. 2020, 31, 825–835. [Google Scholar] [CrossRef]
- Carmagnola, D.; Adriaens, P.; Berglundh, T. Healing of human extraction sockets filled with Bio-Oss®. Clin. Oral Implant. Res. 2003, 14, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Cardaropoli, D.; Tamagnone, L.; Roffredo, A.; Gaveglio, L.; Cardaropoli, G. Socket preservation using bovine bone mineral and collagen membrane: A randomized controlled clinical trial with histologic analysis. Int. J. Periodontics Restor. Dent. 2012, 32, 421–430. [Google Scholar]
- Jung, R.E.; Hürzeler, M.B.; Thoma, D.S.; Khraisat, A.; Hämmerle, C.H.F. Local tolerance and efficiency of two prototype collagen matrices to increase the width of keratinized tissue. J. Clin. Periodontol. 2011, 38, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Thoma, D.S.; Villar, C.C.; Cochran, D.L.; Hämmerle, C.H.F.; Jung, R.E. Tissue integration of collagen-based matrices: An experimental study in mice. Clin. Oral Implant. Res. 2012, 23, 1333–1339. [Google Scholar] [CrossRef]
- Thoma, D.S.; Gasser, T.J.W.; Hämmerle, C.H.F.; Strauss, F.J.; Jung, R.E. Soft tissue augmentation with a volume-stable collagen matrix or an autogenous connective tissue graft at implant sites: Five-year results of a randomized controlled trial post implant loading. J. Periodontol. 2023, 94, 230–243. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.T.; Buser, D. Clinical and esthetic outcomes of implants placed in postextraction sites. Int. J. Oral Maxillofac. Implant. 2009, 24, 186–217. [Google Scholar]
- A Atieh, M.; Alsabeeha, N.H.; Payne, A.G.; Duncan, W.; Faggion, C.M.; Esposito, M. Interventions for replacing missing teeth: Alveolar ridge preservation techniques for dental implant site development. Emergencias 2015, 2015, CD010176. [Google Scholar] [CrossRef] [PubMed]
- Juodzbalys, G.; Wang, H. Soft and hard tissue assessment of immediate implant placement: A case series. Clin. Oral Implant. Res. 2007, 18, 237–243. [Google Scholar] [CrossRef]
- Darby, I.; Chen, S.T.; Buser, D. Ridge preservation techniques for implant therapy. Int. J. Oral Maxillofac. Implant. 2009, 24, 260–271. [Google Scholar]
- Gehrke, P.; Lobert, M.; Dhom, G. Reproducibility of the pink esthetic score—Rating soft tissue esthetics around single-implant restorations with regard to dental observer specialization. J. Esthet. Restor. Dent. 2008, 20, 375–384. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.-L.; Lee, J.-K.; Um, H.-S.; Chang, B.-S. Esthetic evaluation of maxillary single-tooth implants in the esthetic zone. J. Periodontal Implant. Sci. 2010, 40, 188–193. [Google Scholar] [CrossRef]
- Canullo, L.; Pesce, P.; Antonacci, D.; Ravidà, A.; Galli, M.; Khijmatgar, S.; Tommasato, G.; Sculean, A.; Del Fabbro, M. Soft tissue dimensional changes after alveolar ridge preservation using different sealing materials: A systematic review and network meta-analysis. Clin. Oral Investig. 2022, 26, 13–39. [Google Scholar] [CrossRef]
- Cosyn, J.; De Lat, L.; Seyssens, L.; Doornewaard, R.; Deschepper, E.; Vervaeke, S. The effectiveness of immediate implant placement for single tooth replacement compared to delayed implant placement: A systematic review and meta-analysis. J. Clin. Periodontol. 2019, 46, 224–241. [Google Scholar] [CrossRef]
- Iorio-Siciliano, V.; Ramaglia, L.; Blasi, A.; Bucci, P.; Nuzzolo, P.; Riccitiello, F.; Nicolò, M. Dimensional changes following alveolar ridge preservation in the posterior area using bovine-derived xenografts and collagen membrane compared to spontaneous healing: A 6-month randomized controlled clinical trial. Clin. Oral Investig. 2020, 24, 1013–1023. [Google Scholar] [CrossRef]
- Morelli, T.; Zhang, S.; Monaghan, E.; Moss, K.; Lopez, B.; Marchesan, J. Three-Dimensional Volumetric Changes After Socket Augmentation with Deproteinized Bovine Bone and Collagen Matrix. Int. J. Oral Maxillofac. Implant. 2020, 35, 566–575. [Google Scholar] [CrossRef]
- Tavelli, L.; McGuire, M.K.; Zucchelli, G.; Rasperini, G.; Feinberg, S.E.; Wang, H.; Giannobile, W.V. Extracellular matrix-based scaffolding technologies for periodontal and peri-implant soft tissue regeneration. J. Periodontol. 2020, 91, 17–25. [Google Scholar] [CrossRef]
- Rocchietta, I.; Schupbach, P.; Ghezzi, C.; Maschera, E.; Simion, M. Soft tissue integration of a porcine collagen membrane: An experimental study in pigs. Int. J. Periodontics Restor. Dent. 2012, 32, e34–e40. [Google Scholar]
- Schlee, M.; Ghanaati, S.; Willershausen, I.; Stimmlmayr, M.; Sculean, A.; Sader, R.A. Bovine pericardium based non-cross linked collagen matrix for successful root coverage, a clinical study in human. Head Face Med. 2012, 8, 6. [Google Scholar] [CrossRef]
- Linkevicius, T.; Puisys, A.; Steigmann, M.; Vindasiute, E.; Linkeviciene, L. Influence of Vertical Soft Tissue Thickness on Crestal Bone Changes Around Implants with Platform Switching: A Comparative Clinical Study. Clin. Implant. Dent. Relat. Res. 2015, 17, 1228–1236. [Google Scholar] [CrossRef] [PubMed]
- Del Amo, F.S.; Lin, G.; Monje, A.; Galindo-Moreno, P.; Wang, H. Influence of Soft Tissue Thickness on Peri-Implant Marginal Bone Loss: A Systematic Review and Meta-Analysis. J. Periodontol. 2016, 87, 690–699. [Google Scholar] [CrossRef] [PubMed]
- Thoma, D.S.; Naenni, N.; Figuero, E.; Hämmerle, C.H.F.; Schwarz, F.; Jung, R.E.; Sanz-Sánchez, I. Effects of soft tissue augmentation procedures on peri-implant health or disease: A systematic review and meta-analysis. Clin. Oral Implant. Res. 2018, 29 (Suppl. S15), 32–49. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients | Tooth | R.F.E | B.D. | Implant Type | W/L m.m. | Years Follow Up | T.L.B.L | % B.L |
|---|---|---|---|---|---|---|---|---|
| Patient 1 | 21 | Fracture | NO | 3i Biomet | 4/13 | 10 | 0.92 mm | 7.7% |
| Patient 2 | 24 | Fracture | NO | 3i Biomet | 4/13 | 10 | 0.0 mm | 0% |
| Patient 3 | 12 | Carries | NO | 3i Biomet | 4/12 | 10 | 0.37 mm | 2.8% |
| Patient 4 | 12 | Fracture | NO | Biohorizon | 3.8/12 | 9 | 0.0 mm | 0% |
| Patient 5 | 13 | Fracture | NO | Biohorizon | 3.8/12 | 7 | 0.0 mm | 0% |
| Patient 6 | 22 | Carries | NO | Biohorizon | 3.0/12 | 8 | 0.46 mm | 3.8% |
| Patient 7 | 21 | Fracture | NO | Biohorizon | 3.8/12 | 8 | 0.46 mm | 3.8% |
| Patient 8 | 14 | Fracture | Buccal | Biohorizon | 4.2/12 | 7 | 0 mm | 0% |
| Patient 9 | 22 | Fracture | NO | Biohorizon | 3.8/12 | 8 | 0.55 mm | 4.6% |
| Patient 10 | 12 | Carries | NO | Biohorizon | 3.8/12 | 8 | 0 mm | 0% |
| Patient 11 | 22 | Resorption | Palatal | Biohorizon | 3.8/12 | 7 | 0 mm | 0% |
| Patient 12 | 22 | Resorption | NO | Biohorizon | 3.8/12 | 7 | 0.46 mm | 3.8% |
| Patient 13 | 15 | Fracture | Buccal | Biohorizon | 3.8/12 | 8 | 0.6 mm | 5% |
| Patient 14 | 11 | Carries | NO | Biohorizon | 3.8/12 | 8 | 0 mm | 0% |
| Patient 15 | 15 | Fracture | Buccal | Biohorizon | 4.2/12 | 7 | 0 mm | 0% |
| 1st Assesment | 2nd Assesment | |||||
|---|---|---|---|---|---|---|
| Examiner 1 | Examiner 2 | Examiner 3 | ||||
| Variable | ICC * (95% CI) | p Value | ICC (95% CI) | p Value | ICC (95% CI) | p Value |
| Mesial Papilla | 0.576 (0.088–0.841) | 0.12 | 0.847 (0.690–0.948) | <0.01 | 1.000 | <0.01 |
| Distal Papilla | 0.896 (0.708–0.965) | <0.01 | 0.732 (0.350–0.905) | <0.01 | 0.930 (0.796–0.977) | <0.01 |
| Level of the soft tissue margin | 0.727 (0.345–0.904) | <0.01 | 0.860 (0.621–0.953) | <0.01 | 1.000 | <0.01 |
| Soft tissue contour | 0.772 (0.428–0.921) | <0.01 | 1.000 | <0.01 | 1.000 | <0.01 |
| Color | 0.866 (0.634–0.955) | <0.01 | 0.847 (0.546–0.948) | <0.01 | 0.896 (0.708–0.965) | <0.01 |
| Texture | 0.778 (0.441–0.923) | <0.01 | 0.930 (0.796–0.977) | <0.01 | 0.839 (0.727–0.972) | <0.01 |
| Overall | 0.732 (0.431–0.905) | <0.01 | 0.920 (0.804–0.985) | <0.01 | 0.958 (0.975–0.986) | <0.01 |
| Mean Value (±SD) | |||
|---|---|---|---|
| PES Variable | 1st Assesment | 2nd Assesment | p Value |
| Mesial Papilla | 1.69 (±0.46) | 1.71 (±0.45) | 0.564 |
| Distal Papilla | 1.40 (±0.44) | 1.42 (±0.63) | 0.655 |
| Level of the soft tissue margin | 1.64 (±0.48) | 1.61 (±0.49) | 0.564 |
| Soft tissue contour | 1.83 (±0.37) | 1.85 (±0.35) | 0.317 |
| Alveolar Process | 1.95 (±0.21) | 1.99 (±0.18) | 0.157 |
| Color | 1.57 (±0.5) | 1.59 (±0.54) | 0.554 |
| Texture | 1.26 (±0.07) | 1.06 (±0.7) | 0.981 |
| 1st Evaluation | ||
| Variable | ICC * (95% CI) | p Value |
| Mesial Papilla | 0.925 (0.817–0.974) | <0.01 |
| Distal Papilla | 0.924 (0.815–0.974) | <0.01 |
| Level of the soft tissue margin | 0.879 (0.702–0.958) | <0.01 |
| Soft tissue contour | 0.940 (0.853–0.979) | <0.01 |
| Alveolar Process | ||
| Color | 0.834 (0.594–0.94) | <0.01 |
| Texture | 0.944 (0.843–0.984) | <0.01 |
| Overall | 0.935 (0.842–0.977) | <0.01 |
| 2nd Evaluation | ||
| Variable | ICC (95% CI) | p Value |
| Mesial Papilla | 0.918 (0.758–0.971) | <0.01 |
| Distal Papilla | 0.802 (0.515–0.931) | <0.01 |
| Level of the soft tissue margin | 0.877 (0.697–0.977) | <0.01 |
| Soft tissue contour | 1.000 | <0.01 |
| Color | 0.829 (0.581–0.941) | <0.01 |
| Texture | 0.969 (0.924–0.989) | <0.01 |
| Overall | 0.920 (0.844–0.935) | <0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Batas, L.; Xanthopoulou, V.; Gnigou, M.; Vagdouti, T.; Fragkioudakis, I.; Vouros, I. The Long-Term Esthetic and Radiographic Outcome of Implants Placed in the Anterior Maxilla after Ridge Preservation, Combining Bovine Xenograft with Collagen Matrix. Dent. J. 2024, 12, 80. https://doi.org/10.3390/dj12030080
Batas L, Xanthopoulou V, Gnigou M, Vagdouti T, Fragkioudakis I, Vouros I. The Long-Term Esthetic and Radiographic Outcome of Implants Placed in the Anterior Maxilla after Ridge Preservation, Combining Bovine Xenograft with Collagen Matrix. Dentistry Journal. 2024; 12(3):80. https://doi.org/10.3390/dj12030080
Chicago/Turabian StyleBatas, Leonidas, Vithleem Xanthopoulou, Maria Gnigou, Triantafyllia Vagdouti, Ioannis Fragkioudakis, and Ioannis Vouros. 2024. "The Long-Term Esthetic and Radiographic Outcome of Implants Placed in the Anterior Maxilla after Ridge Preservation, Combining Bovine Xenograft with Collagen Matrix" Dentistry Journal 12, no. 3: 80. https://doi.org/10.3390/dj12030080
APA StyleBatas, L., Xanthopoulou, V., Gnigou, M., Vagdouti, T., Fragkioudakis, I., & Vouros, I. (2024). The Long-Term Esthetic and Radiographic Outcome of Implants Placed in the Anterior Maxilla after Ridge Preservation, Combining Bovine Xenograft with Collagen Matrix. Dentistry Journal, 12(3), 80. https://doi.org/10.3390/dj12030080