
Effectiveness of Autologous Platelet Concentrates in the Sinus Lift Surgery: Findings from Systematic Reviews and Meta-Analyses

 ,
, 
 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search and Review Selection
2.2. Data Extraction
2.3. Methodological Quality of Included Reviews
3. Results
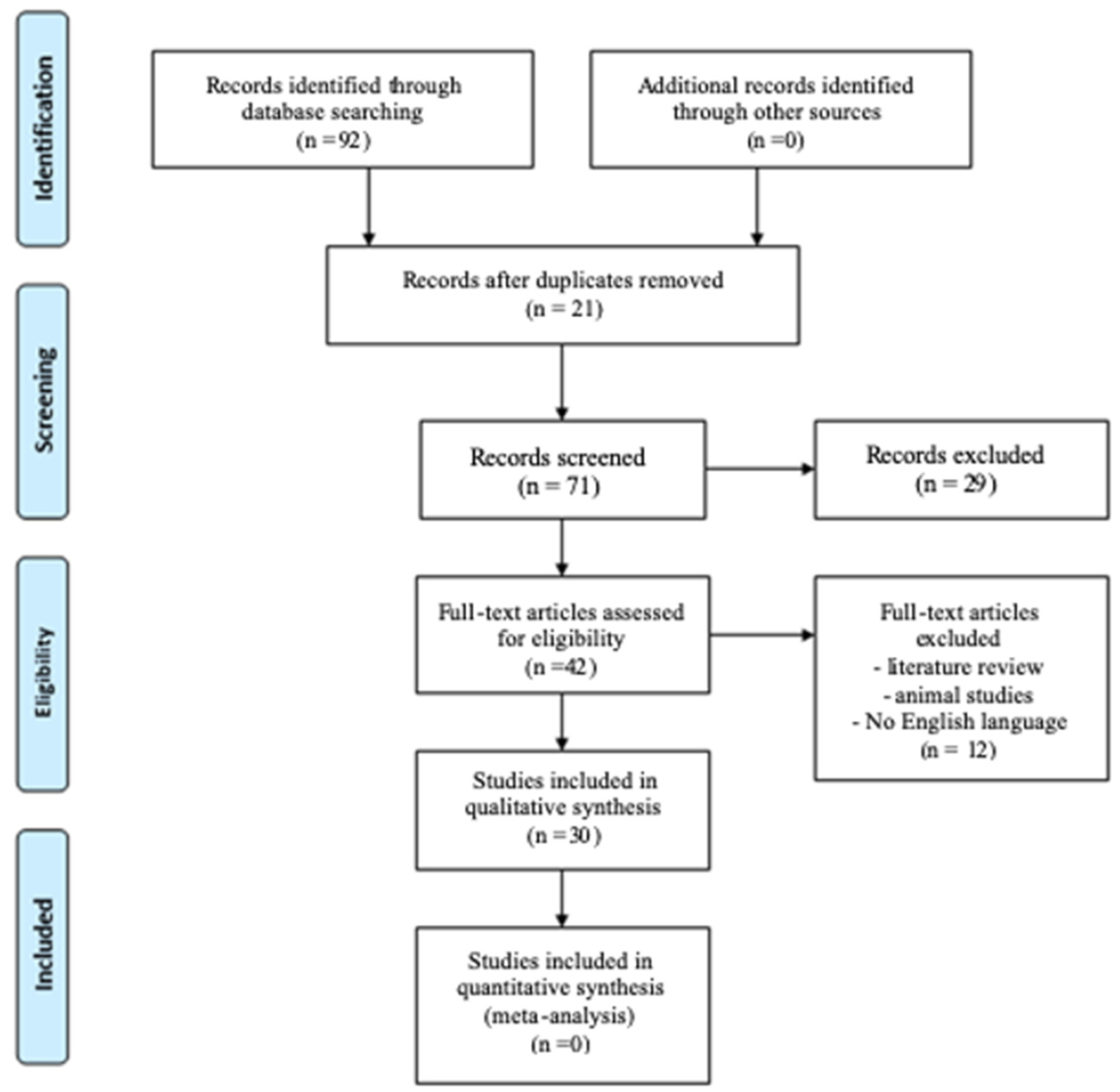
3.1. Search Results
3.2. Characteristics of Included Reviews
3.3. Methodological Quality of Included Reviews

{kind=link}
| Author, Year of Publication | Search Period | Databases | Study Design; Total No. of Subjects | Diagnosis | Intervention | Control | Quality Tool and Quality of the Individual Studies | Outcome | Conclusion |
|---|---|---|---|---|---|---|---|---|---|
| Abdalla RIB et al., 2018 [35] | Up to 6 September 2017 | PubMed, Cochrane Library | SR and MA of 4 RCTs; 106 subjects | Subjects with atrophic posterior maxilla | Type of sinus lift not reported. PRP in combination with AB, ABB, DBBM | Biomaterials alone | 3 RCTs showed an unclear risk of bias, 1 RCT low risk of bias | Implant failure, complications at treated sites (sinusitis, infection, hemorrhage) | The metanalysis revealed no statistically significant difference between the PRP versus non-PRP groups regarding implant failure and complication rate. |
| Ali S et al., 2015 [33] | From 2006 to 2013 | PubMed | SR of 8 clinical studies; 164 subjects | Subjects with atrophic posterior maxilla | Lateral sinus lift using PRF alone or in combination with DFDBA or bovine xenograft | No control group or DFDBA alone or bovine xenograft alone | NR | Implant survival, radiographic bone height, volume and density, hystomorphometric analyses | PRF showed optimistic results as a sole filling material for sinus lift with simultaneous implant placement. Then, it seemed to accelerate maturation of a DFDBA but it had no effect on deproteinized bovine maturation. PRF membranes represent an easy and successful method to cover the sinus membrane or osteotomy window. |
| Anitua E. et al., 2022 [36] | Up to 16 September 2021 | PubMed, Cochrane Library, OVID | SR and MA of 3 RCTs and 3 CCTs; 139 subjects | Subjects with atrophic posterior maxilla | Type of sinus lift not reported. P-PRP/L-PRP in combination with ABB | ABB alone | 3 RCTs showed a low risk of bias, 2 CCTs moderate, 1 CCT low | Percentage of NBF | A beneficial effect on bone formation after maxillary sinus floor elevation can be obtained when anorganic bovine bone is mixed with PRGF. |
| Arora NS et al., 2010 [37] | From 1950 to 2008 | PubMed, Cochrane Library | SR of 5 RCTs; 89 subjects | Subjects with atrophic posterior maxilla | Type of sinus lift not reported. PRP in combination with AB, FDBA, β-TCP | Biomaterials alone | NR | Histological and radiographic evaluation of NBF, early implant placement, quality of life, adverse effects | Although no additional benefit was found in one study, in the others test groups, PRP gave greater bone formation, acceleration of bone formation, higher implant survival rate. Moreover, the handling of the particulate bone grafts was improved. |
| Avila-Ortiz G et al., 2016 [38] | Up to 17 March 2014 | PubMed, Web of Knowledge, Scopus, EMBASE, Cochrane Library, ProQuest | RS of 89 studies of which 33 are on PRP/PRGF/PRF in sinus lift: 12 RCTs, 3 non-RCTs, 14 case series, 4 case reports; 754 subjects | Subjects with atrophic posterior maxillary ridge | Lateral and crestal sinus lift using PRP/PRGF/PRF alone or in combination with AB, bovine xenograft, allograft, β-TCP, algae-derived HA, aragonitic calcium carbonate | Biomaterials alone | RCTs showed a level of evidence 2, non-RCTs level of evidence 3, case series and case report level of evidence 4 (Oxford Scale) | Implant survival and success rate, complications, density of the grafted volume, bone height gain, MBL, BIC, histomorphometric measures | The use of blood-derived products did not suppose a significant benefit compared with the diverse control therapies for all the parameters analyzed with the exception of improved short-term bone formation and increased radiographic density. |
| Bae JH et al., 2011 [39] | From 2000 to January 2010 | PubMed, Cochrane Library, EMBASE | SR and MA of 6 RCTs and 2 CCTs; 191 subjects | Subjects with atrophic posterior maxillary ridge | Type of sinus lift not reported. PRP in combination with FDBA, AB, ABB | Biomaterials alone | No definite publication bias was found in MA of four studies | Implant survival, percentage of bone formation, BIC | Implant survival and BIC was not significantly different in the intervention group treated with PRP compared to control group; bone formation was significantly greater in PRP group. |
| J.V.D.S. Canellas et al., 2021 [40] | Up to 13 July 2020 | PubMed, EMBASE, Cochrane Library, Scopus, Web of Science, LILACS | SR and MA of 11 RCTs of which 2 are on L-PRF;23 subjects | Patients with bone height < 5 mm | Lateral sinus lift using L-PRF in combination with bovine xenograft | Bovine xenograft alone | All studies showed an unclear risk of bias | Percentage of NBF, percentage of residual bone substitute | L-PRF, did not improve bone healing in maxillary sinus floor elevation surgery filled with Bio-Oss. |
| Castro AB et al., 2017 [41] | Up to 31 July 2015 | PubMed, EMBASE, Cochrane Library | RS of 14 RCTs of which 3 are on L-PRF in sinus lift; 76 subjects | Subjects with atrophic posterior maxillary | Lateral and crestal sinus lift using L-PRF in combination with xenograft | Xenograft alone | All articles on sinus lift showed a moderate risk of bias | Time and percentage of NBF | When L-PRF was added to xenograft during lateral and crestal sinus floor elevation NBF occurred faster, although the percentage of NBF was not statistically different between test and control groups. |
| Damsaz M et al., 2020 [42] | From January 2009 to 3 February 2020 | PubMed, Google Scholar, Cochrane Library | SR of 7 clinical studies of which 6 are on L-PRF in sinus lift; 81 subjects | Subjects with atrophic posterior maxilla | Lateral sinus lift using L-PRF alone or in combination with DBBM or allogenous bone graft | No filling or biomaterials alone | 6 studies showed a moderate risk of bias, 1 study high risk of bias | Bone height, time and percentage of NBF, postoperative healing, soft-tissue healing | The addition of L-PRF accelerated bone healing and the amount of regenerated bone but the difference was not statistically different. Postoperative healing was uneventful, without reaching significance. |
| Del Fabbro M et al., 2011 [43] | Up to April 2010 | PubMed, EMBASE, Cochrane Library | SR of 12 studies: 10 RCTs, 2 CCT. 269 subjects | Patients with residual ridge height before surgery varied between 1 and 7 mm | Lateral sinus lift using PRP/PRF/PRGF in combination with FDBA, ABB, AB, β-TCP | Biomaterials alone | NR | Implant survival rate, histologic and histomorphometric analysis | No evident benefit can be evidenced regarding clinical outcomes for implant survival. The analysis of hystomorphometric data suggested a possible advantage of using platelet-derived growth factors in new bone formation. |
| Dragonas P et al., 2018 [44] | Up to 20 December 2017 | PubMed, Scopus, EMBASE, Cochrane Library, Web of Science, ProQuest, Google Scholar | RS of 17 studies of which 8 are on L-PRF in sinus lift: 6 RCTs and 2 CCTs;NR | Subjects with atrophic posterior maxilla | Lateral and crestal sinus lift using L-PRF in combination with xenograft, FDBA, β-TCP | Biomaterials alone | 5 studies showed an high risk of bias, 3 unclear risk of bias | Implant survival, percentage of NBF and bone to bone substitute contact | The use of L-PRF in maxillary sinus augmentation procedures was not associated with more favorable outcomes. |
| Dragonas P et al., 2019 [45] | Up to 23 April 2018 | PubMed, Scopus, EMBASE, Cochrane Library, Web of Science, ProQuest and Google Scholar | SR of 8 studies of which 5 are on PRGF in sinus lift: 4 RCTs, 1 CCTs; 158 subjects | Subjects with atrophic posterior maxillary | Lateral sinus lift using PRGF in combination with bovine xenograft or β-TCP | Biomaterials alone | 3 studies showed an unclear risk of bias, 2 studies low risk of bias | Percentage of NBF, postoperative complications | The addition of PRGF to sinus augmentation was not beneficial on new bone formation and regeneration. Limitations in daily functions were fewer for the PRGF versus control group during the initial postoperative period. |
| Esposito M et al., 2010 [46] | Up to 7 January 2010 | PubMed, Cochrane Library, EMBASE | SR of 10 RCTs of which 4 are on PRP; 114 subjects MA of 3 RCTs on PRP in sinus lift | Subjects with atrophic posterior maxillary | Lateral sinus lift using PRP in combination with AB or bovine xenograft | Biomaterials alone | 3 studies showed an high risk of bias, 1 low risk of bias | Prothesis failure, bone gain (mm or percentage), major complication at bone donor site, duration of the treatment period | No clinical benefit could be observed in any of the trials when using PRP; therefore, there appear to be no reasons to justify its use in this application. |
| Esposito M et al., 2014 [47] | Up to 17 January 2014 | PubMed, Cochrane Library, EMBASE | RS and MA of 18 RCTs on sinus lift of which 2 are on PRP; 62 subjects | Subjects with atrophic posterior maxillary | Lateral sinus lift using PRP with AB or bovine xenograft | Biomaterials alone | 1 RCT showed an unclear risk of bias, 1 RCT an high risk of bias | Prosthetic, implant and graft failures, complications, and histomorphometric evaluation | There were no statistically significant differences between groups who received PRP and those who did not for implant failures and complications. |
| Fujioka-Kobayashi M. et al., 2021 [48] | Up to June 2020 | PubMed, Cochrane Library, Scopus Embase, LILACS | RS of 18 studies of which 6 RCTs and 4 CCTs are on sinus lift; NR | Subjects with atrophic posterior maxillary | Lateral sinus lift using PRF alone or in combination with AB, DBBM, β-TCP | No control group or biomaterials alone | 8 studies showed a low risk of bias, 2 studies unclear risk | NFB, residual bone graft, implant survival rate, postoperative complications | No significant improvement was found in NFB when PRF was added to biomaterials. Only two articles showed an accelerated healing. |
| Ghanaati S et al., 2018 [49] | Up to May 2017 | PubMed | RS of 72 studies of which 8 are on PRF in sinus lift: 6 prospective CCTs studies, 1 is quasi-experimental study, 1 is case control study; 198 subjects | Severe maxillary bone atrophy (in 2 studies bone height < 5 mm) | Lateral and crestal sinus lift using PRF/L-PRF alone or in combination with AB, FDBA, DBBM | No control group or biomaterials alone | 6 studies are IIa, 1 is IIb, 1 is III level of scientific evidence according to US Agency for Healthcare Research and Quality | NFB, bone gain, implant survival rate and implant failure, bone height gain and resorption, periimplant bone density, postoperative complications | No statistically significant differences were found in the addition of PRF to biomaterial in sinus lift compared to biomaterials alone. |
| Guo T et al., 2020 [34] | Up to April 2019 | PubMed, Scopus, Cochrane Library | SR and MA of 8 retrospective cohort studies, 6 prospective cohort studies, 2 RCTs, 1 CCTs, 1 not clearly defined; NR | Subjects with atrophic posterior maxilla | Transcrestal sinus floor elevation using PRP, PRF, CGF, PRGF | Blood clot alone | 1 trial low risk of bias, 2 trials moderate risk of bias, 15 trials high quality with low risk of bias | Implant survival rate, MBL, endo-sinus bone gain | No significant differences were observed 1-year postsurgery on implant survival rate, MBL, and endosinus bone gain. Then, grafting platelet concentrations around dental implants at transcrestal sinus floor elevation sites did not significantly enhance the adjacent bone regeneration. |
| Lemos CA et al., 2015 [32] | From January 2000 to 20 January 2015 | PubMed, EMBASE, Cochrane Library | SR of 12 RCTs and 5 prospective studies; 369 subjects Meta-analysis of 13 RCTs | Subjects with atrophic posterior maxillary | Type of sinus lift not reported. PRP in combination with AB, FDBA, bovine xenograft, β-TCP, algae-derived HA | Biomaterials alone | 12 studies showed an high quality, 5 studies low quality | Percentage of NBF, implant survival rate, ISQ, BIC, MBL and alveolar bone height | No influence of PRP with bone graft on NBF, implant survival and stability, MBL and alveolar bone height in maxillary sinus augmentation.PRP can used to facilitate the handling of bone grafts when they are particulate. |
| Liu R et al., 2019 [50] | NR | PubMed, EMBASE, Cochrane Library | MA of 5 RCTs; 133 subjects | Subjects with atrophic posterior maxillary | Type of sinus lift not reported. PRF/PRP in combination with allogenous, xenograft and β-TCP | Biomaterials alone | All studies showed an high risk of bias | Implant survival rate, complications, histological and histomorphometric evaluation (percentage of NBF, residual bone graft, contact between newly formed bone substitute and bone, soft-tissue area) | There were no statistical differences in survival rate, complications, new bone formation, contact between newly formed bone and bone substitute, percentage of residual bone graft and soft-tissue area between the non-PRF and PRF groups. |
| Meng Y et al., 2020 [51] | Up to 31 December 2019 | PubMed, Web of Science, EMBASE, Cochrane Library | SR and MA of 11 RCTs; 141 subjects | Subjects with atrophic posterior maxillary | Type of sinus lift not reported. PRF/PRP in combination with AB, DBBM, FDBA, β-TCP | Biomaterials alone | 5 studies showed a moderate risk of bias, 6 studies high risk of bias | Percentage of NFB, percentage of residual bone substitute material, percentage of soft-tissue area, radiographic bone density | PRF and PRP did not show additional effect on new bone formation and implant stability when combined with osteoconductive materials. The percentage of residual bone substitute material was not significant between APC group and non-APC group. |
| Ortega-Mejia H et al., 2020 [52] | Up to 9 December 2019 | PubMed, Cochrane Library | RS of 23 studies: 9 RCTs, 1 CCT, 2 case series, 5 retro-spective studies, 5 prospective studies; 547 subjects | Subjects with atrophic posterior maxillary | Type of sinus lift not reported. PRF, PRGF, i-PRF alone or PRF in combination with AB, DFDBA, DBBMA, synthetic nanocrystalline HA, β-TCP | Blood clot or biomaterials alone | Reported for only 9 RCTs: 7 studies showed an high risk of bias, 1 study unclear, 1 study low | Percentage of NBF, bone height, implant stability and implant survival, postoperative complications | No additional beneficial effects in terms of augmented bone height, implant survival rate and implant stability. The percentage of NBF was slightly higher in the PRF group, but this was not statistically significant. |
| Otero AIP et al., 2022 [53] | From January 2006 to August 2020 | PubMed, Science Direct, Scopus | SR of 6 RCTs, 5 CCTs, 2 retro-spective CTs, 1 clinical-histologic study, 1 case report; 354 subjects | Subjects with atrophic posterior maxillary | Lateral and crestal sinus lift using PRF alone or in combination with bovine xenograft, β-TCP, cortico-cancellous bone, FDBA | PRF alone or with allograft, bovine xenograft, synthetic bone graft or biomaterials alone | 8 CTs showed an high quality, 1 CT medium quality, 3 RCTs medium risk of bias, 3 RCTs high risk of bias | Clinical outcomes, bone gain and density | The application of PRF, either alone or with another biomaterials, has been suggested as an effective biomaterial reducing the time for new bone formation. No significant difference was found between groups in terms of ISQ. |
| Pocaterra A et al., 2016 [54] | Up to 3 November 2014 | PubMed, Cochrane Library, CINAHL, Science Direct, ISI Web of Knowledge, Scopus | SR of 7 RCTs; MA of 6 RCTs; 155 subjects | Subjects with atrophic posterior maxillary | Type of sinus lift not reported. PRP in combination with AB, FDBA, ABB | Biomaterials alone | All studies showed an high risk of bias | BIC, percentage of NBF, implant survival | The results of the MA seem to indicate that PRP does not provide additional benefits in newly bone formation or improve the implant survival rate. |
| Rickert D et al., 2011 [55] | Up to September 2010 | PubMed, EMBASE | SR of 12 RCTs of which 4 are on PRP in sinus lift; 73 subjects. MA of 5 RCTs of which 2 are on PRP; 23 subjects | Subjects with atrophic posterior maxillary | Type of sinus lift not reported. PRP in combination with AB | AB alone | NR | Percentage of NBF, implant survival | Adding PRP to grafting material did not promote new bone formation and implant survival. |
| Schliephake H, 2013 [56] | From 1995 to 2012 | PubMed, Cochrane Library | SR of 42 studies: 3 case reports, 9 case series, 5 cohort studies (n° subjects NR); 6 RCTs, 14 cohort studies (373 sub.); 5 SRs e MA | Subjects with atrophic posterior maxilla | Type of sinus lift not reported. PRP/PRF alone or in combination with AB, allograft and bovine xenograft | No control group or biomaterials alone | NR | Percentage of NBF, bone density, bone implant contact, perimplant bone height, implant stability, implant survival | No benefit for the final outcome could be shown for the use of PCs in sinus lift procedures. |
| Sivakumar I. et al., 2023 [57] | Up to April 2021 | PubMed, Cochrane Library, Scopus | 6 RCTs; 188 subjects | Subjects with atrophic posterior maxillary | Type of sinus lift not reported. PRP alone | Biomaterials alone | 3 studies showed a low risk of bias, 3 studies unclear risk of bias | Cumulative survival and success of dental implants | The effect of platelet-rich plasma is uncertain on the survival of dental implants. |
| Stähli A et al., 2018 [58] | Up to 31 December 2017 | PubMed, EMBASE, Cochrane Library | RS of 22 studies of which 12 are on PRP in sinus lift: 7 RCTs, 5 CCTs; 374 subjects | Subjects with atrophic posterior maxillary | Type of sinus lift not reported. PRP in combination with AB, BBG, DBBM, β-TCP | Biomaterials alone | 9 studies showed a moderate risk of bias, 3 studies high risk of bias | Alveolar bone regeneration, soft-tissue healing, graft resorption, osseointegration, postoperative life quality | PRP/PRGF combined with grafting materials may transiently enhance bone formation and reduce postoperative pain and swelling. |
| Stumbas A et al., 2019 [59] | From 1 January 2008 to 1 January 2019 | PubMed | RS of 18 retrospective and prospective studies, clinical trials, case–control and case series studies. Of these articles, 4 are on PRP/L-PRF in sinus lift | Subjects with atrophic posterior maxillary | Lateral sinus lift using PRP/PRF in combination with AB and bovine xenograft | Biomaterials alone | All articles showed an unclear risk of bias | Percentage of NBF, residual graft particles, and soft-tissue healing | PRP combined together with bone graft materials enhances bone formation and vascularization; it might also reduce inflammation and the risk of complications. |
| Suárez-López del Amo F. et Monje A., 2022 [60] | From January 2000 to October 2021 | PubMed, Cochrane Library, EMBASE | SR of 12 RCTs of which 7 are on APCs; 100 subjects | Subjects with atrophic posterior maxillary | Lateral and crestal sinus lift using APCs alone or in combination with AB, DBBM, TCP, CaP | No control group or biomaterials alone | 92% of the studies present some concerns, while 8% of studies show low risk of bias | Data on linear and volumetric dimensional changes by CT, percentage of NBF | In mostly studies APCs do not improve linear and volumetric dimensional changes and the amount of new bone formation. |
| Trimmel B. et al., 2021 [7] | Up to 1 October 2019 | PubMed, Cochrane Library, EMBASE, EBSCO, WOS | SR and MA of 34 RCTs of which 9 are on APCs in sinus lift; NR | Subjects with atrophic posterior maxillary | Lateral sinus lift using PRF/PRP/PRGF in combination with AB, bovine xenograft, β-TCP, nanocrystalline HA | Biomaterials alone | 7 studies showed an unclear risk of bias, 2 high risk of bias | Percentage of NBF | The combination of biomaterials with APCs represents a feasible alternative for AB substitution to achieve high NBF levels with the conventionally used 5- to 8-month healing periods. |
3.4. Clinical, Radiographical and Histomorphometric Results
3.4.1. APCs as Solely Grafting Material
3.4.2. APCs in Combination with Other Biomaterials
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Tatum, J.H. Maxillary and sinus implant reconstructions. Dent. Clin. N. Am. 1986, 30, 207–229. [Google Scholar] [CrossRef] [PubMed]
- Chanavaz, M. Maxillary sinus: Anatomy, physiology, surgery, and bone grafting related to implantology-eleven years of surgical experience (1979–1990). J. Oral Implantol. 1990, 16, 199–209. [Google Scholar] [PubMed]
- Boyne, P.J.; James, R.A. Grafting of the maxillary sinus floor with autogenous marrow and bone. J. Oral Surg. 1980, 38, 613–616. [Google Scholar] [PubMed]
- Wallace, S.S.; Froum, S.J. Effect of maxillary sinus augmentation on the survival of endosseous dental implants. A systematic review. Ann. Periodontol. 2003, 8, 328–343. [Google Scholar] [CrossRef] [PubMed]
- Pjetursson, B.E.; Tan, W.C.; Zwahlen, M.; Lang, N.P. A systematic review of the success of sinus floor elevation and survival of implants inserted in combination with sinus floor elevation. J. Clin. Periodontol. 2008, 35 (Suppl. S8), 216–240. [Google Scholar] [PubMed]
- Carmagnola, D.; Adriaens, P.; Berglundh, T. Healing of human extraction sockets filled with Bio-Oss. Clin. Oral Implants Res. 2003, 14, 137–143. [Google Scholar] [CrossRef]
- Trimmel, B.; Gede, N.; Hegyi, P.; Szakács, Z.; Mezey, G.A.; Varga, E.; Kivovics, M.; Hanák, L.; Rumbus, Z.; Szabó, G. Relative performance of various biomaterials used for maxillary sinus augmentation: A Bayesian network meta-analysis. Clin. Oral Implants Res. 2021, 32, 135–153. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.W.; Chang, H.S.; Leung, K.W.; Lai, Y.L.; Kao, S.Y. Implant placement immediately after the lateral approach of the trap door window procedure to create a maxillary sinus lift without bone grafting: A 2-year retrospective evaluation of 47 implants in 33 patients. J. Oral Maxillofac. Surg. 2007, 65, 2324–2328. [Google Scholar] [CrossRef]
- Wikesjö, U.M.; Huang, Y.H.; Polimeni, G.; Qahash, M. Bone morphogenetic proteins: A realistic alternative to bone grafting for alveolar reconstruction. Oral Maxillofac. Surg. Clin. N. Am. 2007, 19, 535–551, vi–vii. [Google Scholar]
- Kirker-Head, C.A.; Boudrieau, R.J.; Kraus, K.H. Use of bone morphogenetic proteins for augmentation of bone regeneration. J. Am. Vet. Med. Assoc. 2007, 231, 1039–1055. [Google Scholar]
- Hallman, M.; Thor, A. Bone substitutes and growth factors as an alternative/complement to autogenous bone for grafting in implant dentistry. Periodontology 2000 2008, 47, 172–192. [Google Scholar] [CrossRef] [PubMed]
- Al-Hamed, F.S.; Mahri, M.; Al-Waeli, H.; Torres, J.; Badran, Z.; Tamimi, F. Regenerative Effect of Platelet Concentrates in Oral and Craniofacial Regeneration. Front. Cardiovasc. Med. 2019, 6, 126. [Google Scholar]
- Hollý, D.; Klein, M.; Mazreku, M.; Zamborský, R.; Polák, Š.; Danišovič, Ľ.; Csöbönyeiová, M. Stem Cells and Their Derivatives-Implications for Alveolar Bone Regeneration: A Comprehensive Review. Int. J. Mol. Sci. 2021, 22, 11746. [Google Scholar] [CrossRef] [PubMed]
- Gasparro, R.; Qorri, E.; Valletta, A.; Masucci, M.; Sammartino, P.; Amato, A.; Marenzi, G. Non-Transfusional Hemocomponents: From Biology to the Clinic-A Literature Review. Bioengineering 2018, 5, 27. [Google Scholar] [CrossRef]
- Marx, R.E. Platelet-rich plasma: Evidence to support its use. J. Oral Maxillofac. Surg. 2004, 62, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Choukroun, J.; Diss, A.; Simonpieri, A.; Girard, M.O.; Schoeffler, C.; Dohan, S.L.; Dohan, A.J.; Mouhyi, J.; Dohan, D.M. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part IV: Clinical effects on tissue healing. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, e56–e60. [Google Scholar] [CrossRef]
- Rodella, L.F.; Favero, G.; Boninsegna, R.; Buffoli, B.; Labanca, M.; Scarì, G.; Sacco, L.; Batani, T.; Rezzani, R. Growth factors, CD34 positive cells, and fibrin network analysis in concentrated growth factors fraction. Microsc. Res. Tech. 2011, 74, 772–777. [Google Scholar] [CrossRef] [PubMed]
- Andia, I.; Abate, M. Platelet-rich plasma: Underlying biology and clinical correlates. Regen. Med. 2013, 8, 645–658. [Google Scholar] [CrossRef]
- Gasparro, R.; Sammartino, G.; Mariniello, M.; di Lauro, A.E.; Spagnuolo, G.; Marenzi, G. Treatment of periodontal pockets at the distal aspect of mandibular second molar after surgical removal of impacted third molar and application of L-PRF: A split-mouth randomized clinical trial. Quintessence Int. 2020, 51, 204–211. [Google Scholar]
- Gasparro, R.; Adamo, D.; Masucci, M.; Sammartino, G.; Mignogna, M.D. Use of injectable platelet-rich fibrin in the treatment of plasma cell mucositis of the oral cavity refractory to corticosteroid therapy: A case report. Dermatol. Ther. 2019, 32, e13062. [Google Scholar] [CrossRef]
- D’Esposito, V.; Lecce, M.; Marenzi, G.; Cabaro, S.; Ambrosio, M.R.; Sammartino, G.; Misso, S.; Migliaccio, T.; Liguoro, P.; Oriente, F.; et al. Platelet-rich plasma counteracts detrimental effect of high-glucose concentrations on mesenchymal stem cells from Bichat fat pad. J. Tissue Eng. Regen. Med. 2020, 14, 701–713. [Google Scholar] [CrossRef] [PubMed]
- Emer, J. Platelet-Rich Plasma (PRP): Current Applications in Dermatology. Ski. Ther. Lett. 2019, 24, 1–6. [Google Scholar]
- Braccini, F.; Tardivet, L.; Dohan Ehrenfest, D.M. The relevance of Choukroun’s Platelet-Rich Fibrin (PRF) during middle ear surgery: Preliminary results. Rev. Laryngol. Otol. Rhinol. 2009, 130, 175–180. [Google Scholar]
- Braccini, F.; Dohan, D.M. The relevance of Choukroun’s platelet rich fibrin (PRF) during facial aesthetic lipostructure (Coleman’s technique): Preliminary results. Rev. Laryngol. Otol. Rhinol. 2007, 128, 255–260. [Google Scholar]
- Charrier, J.B.; Monteil, J.P.; Albert, S.; Collon, S.; Bobin, S.; Dohan Ehrenfest, D.M. Relevance of Choukroun’s Platelet-Rich Fibrin (PRF) and SMAS flap in primary reconstruction after superficial or subtotal parotidectomy in patients with focal pleiomorphic adenoma: A new technique. Rev. Laryngol. Otol. Rhinol. 2008, 129, 313–318. [Google Scholar]
- Man, D.; Plosker, H.; Winland-Brown, J.E. The use of autologous platelet-rich plasma (platelet gel) and autologous platelet-poor plasma (fibrin glue) in cosmetic surgery. Plast. Reconstr. Surg. 2001, 107, 229–237; discussion 238–239. [Google Scholar] [CrossRef] [PubMed]
- Everts, P.A.; Devilee, R.J.; Brown Mahoney, C.; Eeftinck-Schattenkerk, M.; Box, H.A.; Knape, J.T.; Van Zundert, A. Platelet gel and fibrin sealant reduce allogeneic blood transfusions in total knee arthroplasty. Acta Anaesthesiol. Scand. 2006, 50, 593–599. [Google Scholar] [CrossRef] [PubMed]
- Mishra, A.; Harmon, K.; Woodall, J.; Vieira, A. Sports medicine applications of platelet rich plasma. Curr. Pharm. Biotechnol. 2012, 13, 1185–1195. [Google Scholar] [CrossRef] [PubMed]
- Fanning, J.; Murrain, L.; Flora, R.; Hutchings, T.; Johnson, J.M.; Fenton, B.W. Phase I/II prospective trial of autologous platelet tissue graft in gynecologic surgery. J. Minim. Invasive Gynecol. 2007, 14, 633–637. [Google Scholar] [CrossRef]
- Khalafi, R.S.; Bradford, D.W.; Wilson, M.G. Topical application of autologous blood products during surgical closure following a coronary artery bypass graft. Eur. J. Cardiothorac. Surg. 2008, 34, 360–364. [Google Scholar] [CrossRef]
- Alio, J.L.; Abad, M.; Artola, A.; Rodriguez-Prats, J.L.; Pastor, S.; Ruiz-Colecha, J. Use of autologous platelet-rich plasma in the treatment of dormant corneal ulcers. Ophthalmology 2007, 114, 1286–1293.e1. [Google Scholar] [CrossRef] [PubMed]
- Lemos, C.A.; Mello, C.C.; dos Santos, D.M.; Verri, F.R.; Goiato, M.C.; Pellizzer, E.P. Effects of platelet-rich plasma in association with bone grafts in maxillary sinus augmentation: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2016, 45, 517–525. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.; Bakry, S.A.; Abd-Elhakam, H. Platelet-Rich Fibrin in Maxillary Sinus Augmentation: A Systematic Review. J. Oral Implantol. 2015, 41, 746–753. [Google Scholar] [CrossRef] [PubMed]
- Guo, T.; Gulati, K.; Shen, Z.; Han, P.; Fan, Z. Therapeutic outcomes of non-grafted and platelet concentrations-grafted transcrestal maxillary sinus elevation (TSFE): A systematic review and meta-analysis. Sci. Rep. 2020, 10, 5935. [Google Scholar] [CrossRef]
- Abdalla, R.I.B.; Alqutaibi, A.Y.; Kaddah, A. Does the adjunctive use of platelet-rich plasma to bone graft during sinus augmentation reduce implant failure and complication? Systematic review and meta-analysis. Quintessence Int. 2018, 49, 139–146. [Google Scholar]
- Anitua, E.; Allende, M.; Eguia, A.; Alkhraisat, M.H. Bone-Regenerative Ability of Platelet-Rich Plasma Following Sinus Augmentation with Anorganic Bovine Bone: A Systematic Review with Meta-Analysis. Bioengineering 2022, 9, 597. [Google Scholar] [CrossRef]
- Arora, N.S.; Ramanayake, T.; Ren, Y.F.; Romanos, G.E. Platelet-rich plasma in sinus augmentation procedures: A systematic literature review: Part II. Implant Dent. 2010, 19, 145–157. [Google Scholar] [CrossRef]
- Avila-Ortiz, G.; Bartold, P.M.; Giannobile, W.; Katagiri, W.; Nares, S.; Rios, H.; Spagnoli, D.; Wikesjö, U.M. Biologics and Cell Therapy Tissue Engineering Approaches for the Management of the Edentulous Maxilla: A Systematic Review. Int. J. Oral Maxillofac. Implants 2016, 31, s121–s164. [Google Scholar] [CrossRef]
- Bae, J.H.; Kim, Y.K.; Myung, S.K. Effects of platelet-rich plasma on sinus bone graft: Meta-analysis. J. Periodontol. 2011, 82, 660–667. [Google Scholar] [CrossRef]
- Canellas, J.V.D.S.; Drugos, L.; Ritto, F.G.; Fischer, R.G.; Medeiros, P.J.D. Xenograft materials in maxillary sinus floor elevation surgery: A systematic review with network meta-analyses. Br. J. Oral Maxillofac. Surg. 2021, 59, 742–751. [Google Scholar] [CrossRef]
- Castro, A.B.; Meschi, N.; Temmerman, A.; Pinto, N.; Lambrechts, P.; Teughels, W.; Quirynen, M. Regenerative potential of leucocyte- and platelet-rich fibrin. Part B: Sinus floor elevation, alveolar ridge preservation and implant therapy. A systematic review. J. Clin. Periodontol. 2017, 44, 225–234. [Google Scholar] [CrossRef]
- Damsaz, M.; Castagnoli, C.Z.; Eshghpour, M.; Alamdari, D.H.; Alamdari, A.H.; Noujeim, Z.E.F.; Haidar, Z.S. Evidence-Based Clinical Efficacy of Leukocyte and Platelet-Rich Fibrin in Maxillary Sinus Floor Lift, Graft and Surgical Augmentation Procedures. Front. Surg. 2020, 7, 537138. [Google Scholar] [CrossRef] [PubMed]
- Del Fabbro, M.; Bortolin, M.; Taschieri, S.; Weinstein, R.L. Effect of autologous growth factors in maxillary sinus augmentation: A systematic review. Clin. Implant Dent. Relat. Res. 2013, 15, 205–216. [Google Scholar] [CrossRef]
- Dragonas, P.; Schiavo, J.H.; Avila-Ortiz, G.; Palaiologou, A.; Katsaros, T. Plasma rich in growth factors (PRGF) in intraoral bone grafting procedures: A systematic review. J. Craniomaxillofac. Surg. 2019, 47, 443–453. [Google Scholar] [CrossRef]
- Dragonas, P.; Katsaros, T.; Avila-Ortiz, G.; Chambrone, L.; Schiavo, J.H.; Palaiologou, A. Effects of leukocyte-platelet-rich fibrin (L-PRF) in different intraoral bone grafting procedures: A systematic review. Int. J. Oral Maxillofac. Surg. 2019, 48, 250–262. [Google Scholar] [CrossRef]
- Esposito, M.; Grusovin, M.G.; Rees, J.; Karasoulos, D.; Felice, P.; Alissa, R.; Worthington, H.; Coulthard, P. Effectiveness of sinus lift procedures for dental implant rehabilitation: A Cochrane systematic review. Eur. J. Oral Implantol. 2010, 3, 7–26. [Google Scholar]
- Esposito, M.; Felice, P.; Worthington, H.V. Interventions for replacing missing teeth: Augmentation procedures of the maxillary sinus. Cochrane Database Syst. Rev. 2014, 5, CD008397. [Google Scholar] [CrossRef]
- Fujioka-Kobayashi, M.; Miron, R.J.; Moraschini, V.; Zhang, Y.; Gruber, R.; Wang, H.L. Efficacy of platelet-rich fibrin on bone formation, part 2: Guided bone regeneration, sinus elevation and implant therapy. Int. J. Oral Implantol. 2021, 14, 285–302. [Google Scholar]
- Ghanaati, S.; Herrera-Vizcaino, C.; Al-Maawi, S.; Lorenz, J.; Miron, R.J.; Nelson, K.; Schwarz, F.; Choukroun, J.; Sader, R. Fifteen Years of Platelet Rich Fibrin in Dentistry and Oromaxillofacial Surgery: How High is the Level of Scientific Evidence? J. Oral Implantol. 2018, 44, 471–492. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Yan, M.; Chen, S.; Huang, W.; Wu, D.; Chen, J. Effectiveness of Platelet-Rich Fibrin as an Adjunctive Material to Bone Graft in Maxillary Sinus Augmentation: A Meta-Analysis of Randomized Controlled Trails. BioMed Res. Int. 2019, 2019, 7267062. [Google Scholar] [CrossRef] [PubMed]
- Meng, Y.; Huang, X.; Wu, M.; Yang, X.; Liu, Y. The Effect of Autologous Platelet Concentrates on Maxillary Sinus Augmentation: A Meta-Analysis of Randomized Controlled Trials and Systematic Review. BioMed Res. Int. 2020, 2020, 7589072. [Google Scholar] [CrossRef] [PubMed]
- Ortega-Mejia, H.; Estrugo-Devesa, A.; Saka-Herrán, C.; Ayuso-Montero, R.; López-López, J.; Velasco-Ortega, E. Platelet-Rich Plasma in Maxillary Sinus Augmentation: Systematic Review. Materials 2020, 13, 622. [Google Scholar] [CrossRef] [PubMed]
- Otero, A.I.P.; Fernandes, J.C.H.; Borges, T.; Nassani, L.; Castilho, R.M.; Fernandes, G.V.O. Sinus Lift Associated with Leucocyte-Platelet-Rich Fibrin (Second Generation) for Bone Gain: A Systematic Review. J. Clin. Med. 2022, 11, 1888. [Google Scholar] [CrossRef] [PubMed]
- Pocaterra, A.; Caruso, S.; Bernardi, S.; Scagnoli, L.; Continenza, M.A.; Gatto, R. Effectiveness of platelet-rich plasma as an adjunctive material to bone graft: A systematic review and meta-analysis of randomized controlled clinical trials. Int. J. Oral Maxillofac. Surg. 2016, 45, 1027–1034. [Google Scholar] [CrossRef] [PubMed]
- Rickert, D.; Slater, J.J.; Meijer, H.J.; Vissink, A.; Raghoebar, G.M. Maxillary sinus lift with solely autogenous bone compared to a combination of autogenous bone and growth factors or (solely) bone substitutes. A systematic review. Int. J. Oral Maxillofac. Surg. 2012, 41, 160–167. [Google Scholar] [CrossRef]
- Schliephake, H. Clinical efficacy of growth factors to enhance tissue repair in oral and maxillofacial reconstruction: A systematic review. Clin. Implant Dent. Relat. Res. 2015, 17, 247–273. [Google Scholar] [CrossRef] [PubMed]
- Sivakumar, I.; Arunachalam, S.; Mahmoud Buzayan, M.; Sharan, J. Does the use of platelet-rich plasma in sinus augmentation improve the survival of dental implants? A systematic review and meta-analysis. J. Oral Biol. Craniofac. Res. 2023, 13, 57–66. [Google Scholar] [CrossRef]
- Stähli, A.; Strauss, F.J.; Gruber, R. The use of platelet-rich plasma to enhance the outcomes of implant therapy: A systematic review. Clin. Oral Implants Res. 2018, 29 (Suppl. S18), 20–36. [Google Scholar] [CrossRef] [PubMed]
- Stumbras, A.; Krukis, M.M.; Januzis, G.; Juodzbalys, G. Regenerative bone potential after sinus floor elevation using various bone graft materials: A systematic review. Quintessence Int. 2019, 50, 548–558. [Google Scholar]
- Suárez-López Del Amo, F.; Monje, A. Efficacy of biologics for alveolar ridge preservation/reconstruction and implant site development: An American Academy of Periodontology best evidence systematic review. J. Periodontol. 2022, 93, 1827–1847. [Google Scholar] [CrossRef]
- Simonpieri, A.; Choukroun, J.; Del Corso, M.; Sammartino, G.; Dohan Ehrenfest, D.M. Simultaneous sinus-lift and implantation using microthreaded implants and leukocyte- and platelet-rich fibrin as sole grafting material: A six-year experience. Implant Dent. 2011, 20, 2–12. [Google Scholar] [CrossRef] [PubMed]
- Simonpieri, A.; Del Corso, M.; Sammartino, G.; Dohan Ehrenfest, D.M. The relevance of Choukroun’s platelet-rich fibrin and metronidazole during complex maxillary rehabilitations using bone allograft. Part I: A new grafting protocol. Implant Dent. 2009, 18, 102–111. [Google Scholar] [CrossRef]
- Tatullo, M.; Marrelli, M.; Cassetta, M.; Pacifici, A.; Stefanelli, L.V.; Scacco, S.; Dipalma, G.; Pacifici, L.; Inchingolo, F. Platelet Rich Fibrin (P.R.F.) in reconstructive surgery of atrophied maxillary bones: Clinical and histological evaluations. Int. J. Med. Sci. 2012, 9, 872–880. [Google Scholar] [CrossRef]
- Batas, L.; Tsalikis, L.; Stavropoulos, A. PRGF as Adjunct to DBB in Maxillary Sinus Floor Augmentation: Histological Results of a Pilot Split-Mouth Study. Int. J. Implant Dent. 2019, 5, 14. [Google Scholar] [CrossRef] [PubMed]
- Intini, G. The use of platelet-rich plasma in bone reconstruction therapy. Biomaterials 2009, 30, 4956–4966. [Google Scholar] [CrossRef]
- Forabosco, A.; Gheno, E.; Spinato, S.; Garuti, G.; Forabosco, E.; Consolo, U. Concentrated growth factors in maxillary sinus floor augmentation: A preliminary clinical comparative evaluation. Int. J. Growth Factors Stem Cells Dent. 2018, 1, 2–7. [Google Scholar]
- Stacchi, C.; Spinato, S.; Lombardi, T.; Bernardello, F.; Bertoldi, C.; Zaffe, D.; Nevins, M. Minimally Invasive Management of Implant-Supported Rehabilitation in the Posterior Maxilla, Part I. Sinus Floor Elevation: Biologic Principles and Materials. Int. J. Periodontics Restor. Dent. 2020, 40, e85–e93. [Google Scholar] [CrossRef]
- Bennardo, F.; Barone, S.; Buffone, C.; Colangeli, W.; Antonelli, A.; Giudice, A. Removal of dental implants displaced into the maxillary sinus: A retrospective single-center study. Head Face Med. 2022, 18, 34. [Google Scholar] [CrossRef] [PubMed]
- Avila, G.; Wang, H.L.; Galindo-Moreno, P.; Misch, C.E.; Bagramian, R.A.; Rudek, I.; Benavides, E.; Moreno-Riestra, I.; Braun, T.; Neiva, R. The influence of the bucco-palatal distance on sinus augmentation outcomes. J. Periodontol. 2010, 81, 1041–1050. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. Br. Med. J. 2017, 358, j4008. [Google Scholar] [CrossRef]
- Booth, A.; Clarke, M.; Ghersi, D.; Moher, D.; Petticrew, M.; Stewart, L. An international registry of systematic-review protocol. Lancet 2011, 377, 108–109. [Google Scholar] [CrossRef]
- Al-Moraissi, E.A.; Alkhutari, A.S.; Abotaleb, B.; Altairi, N.H.; Del Fabbro, M. Do osteoconductive bone substitutes result in similar bone regeneration for maxillary sinus augmentation when compared to osteogenic and osteoinductive bone grafts? A systematic review and frequentist network meta-analysis. Int. J. Oral Maxillofac. Surg. 2020, 49, 107–120. [Google Scholar] [CrossRef] [PubMed]
- Bernardi, S.; Macchiarelli, G.; Bianchi, S. Autologous Materials in Regenerative Dentistry: Harvested Bone, Platelet Concentrates and Dentin Derivates. Molecules 2020, 25, 5330. [Google Scholar] [CrossRef] [PubMed]
- Dai, Y.Z.; Ye, P. Recent advance in research of platelet-rich fibrin (correction of plasma). Zhonghua Kou Qiang Yi Xue Za Zhi 2011, 46, 382–383. [Google Scholar] [PubMed]
- Esposito, M.; Grusovin, M.G.; Coulthard, P.; Worthington, H.V. The efficacy of various bone augmentation procedures for dental implants: A Cochrane systematic review of randomized controlled clinical trials. Int. J. Oral Maxillofac. Implants 2006, 21, 696–710. [Google Scholar]
- Farshidfar, N.; Amiri, M.A.; Jafarpour, D.; Hamedani, S.; Niknezhad, S.V.; Tayebi, L. The feasibility of injectable PRF (I-PRF) for bone tissue engineering and its application in oral and maxillofacial reconstruction: From bench to chairside. Biomater. Adv. 2022, 134, 112557. [Google Scholar] [CrossRef] [PubMed]
- Franchini, M.; Cruciani, M.; Mengoli, C.; Masiello, F.; Marano, G.; D’Aloja, E.; Dell’Aringa, C.; Pati, I.; Veropalumbo, E.; Pupella, S.; et al. The use of platelet-rich plasma in oral surgery: A systematic review and meta-analysis. Blood Transfus. 2019, 17, 357–367. [Google Scholar] [PubMed]
- Kumar, K.R.; Genmorgan, K.; Abdul Rahman, S.M.; Rajan, M.A.; Kumar, T.A.; Prasad, V.S. Role of plasma-rich fibrin in oral surgery. J. Pharm. Bioallied Sci. 2016, 8 (Suppl. 1), S36–S38. [Google Scholar] [CrossRef] [PubMed]
- Maniyar, N. Platelet-Rich Fibrin: A ‘Wonder Material’ in Advanced Surgical Dentistry. Med. J. Dr. D Y Patil Univ. 2018, 11, 287–290. [Google Scholar] [CrossRef]
- Miron, R.J.; Zucchelli, G.; Pikos, M.A.; Salama, M.; Lee, S.; Guillemette, V.; Fujioka-Kobayashi, M.; Bishara, M.; Zhang, Y.; Wang, H.L.; et al. Use of platelet-rich fibrin in regenerative dentistry: A systematic review. Clin. Oral Investig. 2017, 21, 1913–1927. [Google Scholar] [CrossRef]
- Yuen, T. Sinus elevation. Caldwell Luc approach—Has it gone passed its use-by date? Ann. R. Australas. Coll. Dent. Surg. 2000, 15, 71–73. [Google Scholar] [PubMed]

| Databases | Search Strategy |
|---|---|
| PubMed | ((“sinus lift” [All Fields]) OR (“sinus lifting” [All Fields]) OR (“sinus augmentation [All Fields]”) OR (“sinus elevation [All Fileds]”) OR (“maxillary sinus lift” [All Fields]) OR (“maxillary sinus elevation” [All Fields]) OR (“maxillary sinus augmentation [All Fields]”) OR (“maxillary sinus floor elevation” [All Fields]) OR (“maxillary sinus floor lift” [All Fields]) OR (“maxillary sinus floor augmentation” [All Fields] OR (“maxillary sinus/surgery” [MeSH Terms]) OR (“sinus floor augmentation” [MesH Terms])) AND ((“prp” [All Fields]) OR (“platelet rich plasma” [All Fields]) OR (“prf” [All Fields]) OR (“platelet rich fibrin” [All Fields]) OR (“autologous platelet concentrates” [All Fields]) OR (“platelet concentrates” [All Fields]) OR (platelet concentrations-grafted [Title/Abstract])) AND ((meta-analysis [Filter] OR systematic review [Filter])) |
| Scopus | (TITLE-ABS-KEY (sinus lift) OR TITLE-ABS-KEY (sinus lifting) OR TITLE-ABS-KEY (sinus augmentation) OR TITLE-ABS-KEY (sinus elevation) OR TITLE-ABS-KEY (maxillary sinus lift) OR TITLE-ABS-KEY (maxillary sinus elevation) OR TITLE-ABS-KEY (maxillary sinus augmentation) OR TITLE-ABS-KEY (maxillary sinus floor elevation) OR TITLE-ABS-KEY (maxillary sinus floor lift) OR TITLE-ABS-KEY (maxillary sinus floor augmentation) OR TITLE-ABS-KEY (maxillary sinus/surgery) OR TITLE-ABS-KEY (sinus floor augmentation)) AND (TITLE-ABS-KEY (prp) OR TITLE-ABS-KEY (platelet rich plasma) OR TITLE-ABS-KEY (prf) OR TITLE-ABS-KEY (platelet rich fibrin) OR TITLE-ABS-KEY (autologous platelet concentrates) OR TITLE-ABS-KEY (platelet concentrates) OR TITLE-ABS-KEY (platelet concentrations-grafted)) AND (LIMIT-TO (DOCTYPE, “re”)) |
| Cochrane | (Platelet concentrates in maxillary sinus lift):ti,ab,kw |
| Abdalla RIB et al., 2018 [35] | Ali S et al., 2015 [33] | Anitua E. et al., 2022 [36] | Arora NS et al., 2010 [37] | Avila-Ortiz G et al., 2016 [38] | Bae JH et al., 2011 [39] | J.V.D.S. Canellas et al., 2021 [40] | Castro AB et al., 2017 [41] | Damsaz M et al., 2020 [42] | Del Fabbro M et al., 2011 [43] | Dragonas P et al., 2018 [44] | Dragonas P et al., Mar 2019 [45] | Esposito M et al., 2010 [46] | Esposito M et al., 2014 [47] | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Did the research questions and inclusion criteria for the review include the components of PICO? | N | N | Y | N | Y | N | Y | Y | Y | N | Y | Y | N | N | ||
| Did the report of the review contain an explicit statement that the review methods were established prior to the conduct of the review and did the report justify any significant deviations from the protocol? | N | N | N | N | N | N | N | N | N | N | N | N | N | N | ||
| Did the review authors explain their selection of the study designs for inclusion in the review? | Y | PY | Y | Y | Y | Y | Y | Y | PY | Y | Y | Y | Y | Y | ||
| Did the review authors use a comprehensive literature search strategy? | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | ||
| Did the review authors perform study selection in duplicate? | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | ||
| Did the review authors perform data extraction in duplicate? | Y | Y | N | Y | N | Y | NR | Y | Y | Y | Y | Y | Y | Y | ||
| Did the review authors provide a list of excluded studies and justify the exclusions? | Y | N | Y | Y | Y | Y | N | Y | N | N | Y | Y | Y | Y | ||
| Did the review authors describe the included studies in adequate detail? | Y | PY | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | PY | Y | ||
| Did the review authors use a satisfactory technique for assessing the risk of bias (RoB) in individual studies that were included in the review? | Y | N | Y | N | Y | N | Y | Y | PY | N | Y | Y | Y | Y | ||
| Did the review authors report on the sources of funding for the studies included in the review? | N | N | Y | Y | Y | Y | N | Y | Y | N | Y | Y | N | Y | ||
| If meta-analysis was performed did the review authors use appropriate methods for statistical combination of results? | Y | Nm | Y | Nm | Nm | Y | Y | Nm | Nm | Nm | Nm | Nm | Y | Y | ||
| If meta-analysis was performed did the review authors assess the potential impact of RoB in individual studies on the results of the meta-analysis or other evidence synthesis? | Y | Nm | Y | Nm | Nm | N | Y | Nm | Nm | Nm | Nm | Nm | Y | Y | ||
| Did the review authors account for RoB in individual studies when interpreting/discussing the results of the review? | Y | N | Y | N | Y | N | Y | Y | N | N | Y | N | Y | Y | ||
| Did the review authors provide a satisfactory explanation for, and discussion of, any heterogeneity observed in the results of the review? | Y | PY | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | ||
| If they performed quantitative synthesis did the review authors carry out an adequate investigation of publication bias (small study bias) and discuss its likely impact on the results of the review? | N | Nm | N | Nm | Nm | N | Y | Nm | Nm | Nm | Nm | Nm | N | N | ||
| Did the review authors report any potential sources of conflict of interest, including any funding they received for conducting the review? | N | N | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | ||
| OVERALL QUALITY ASSESSMENT | M | L | H | M | L | M | H | M | L | L | M | M | M | H | ||
| Fujioka-Kobayashi M., 2021 [48] | Ghanaati S et al., 2018 [49] | Guo T et al., 2020 [34] | Lemos CA et al., 2015 [32] | Liu R et al., 2019 [50] | Meng Y et al., 2020 [51] | Ortega-Mejia H et al., 2020 [52] | AI P Otero et al., 2022 [53] | Pocaterra A et al., 2016 [54] | Rickert D et al., 2011 [55] | Schliephake H, 2013 [56] | Sivakumar I. et al., 2023 [57] | Stähli A et al., 2018 [58] | Stumbas A et al., 2019 [59] | Suárez-López del Amo F. et Monje A., 2022 [60] | Trimmel B. et al., 2021 [7] | |
| Did the research questions and inclusion criteria for the review include the components of PICO? | Y | N | Y | Y | N | Y | Y | Y | N | N | N | Y | Y | Y | Y | Y |
| Did the report of the review contain an explicit statement that the review methods were established prior to the conduct of the review and did the report justify any significant deviations from the protocol? | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N |
| Did the review authors explain their selection of the study designs for inclusion in the review? | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | PY |
| Did the review authors use a comprehensive literature search strategy? | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | Y |
| Did the review authors perform study selection in duplicate? | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | NR | Y | Y | NR | Y | Y |
| Did the review authors perform data extraction in duplicate? | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | NR | Y | Y | Y | Y | Y |
| Did the review authors provide a list of excluded studies and justify the exclusions? | N | N | Y | Y | N | N | Y | Y | Y | N | N | N | Y | Y | Y | Y |
| Did the review authors describe the included studies in adequate detail? | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | PY | Y | Y |
| Did the review authors use a satisfactory technique for assessing the risk of bias (RoB) in individual studies that were included in the review? | Y | N | Y | Y | Y | Y | PY | Y | Y | N | N | Y | Y | Y | Y | Y |
| Did the review authors report on the sources of funding for the studies included in the review? | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | N | Y | Y |
| If meta-analysis was performed did the review authors use appropriate methods for statistical combination of results? | Nm | Nm | Y | Y | Y | Y | Nm | Nm | Y | Y | Nm | Nm | Nm | Nm | Nm | Y |
| If meta-analysis was performed did the review authors assess the potential impact of RoB in individual studies on the results of the meta-analysis or other evidence synthesis? | Nm | Nm | N | Y | Y | Y | Nm | Nm | Y | N | Nm | Nm | Nm | Nm | Nm | Y |
| Did the review authors account for RoB in individual studies when interpreting/discussing the results of the review? | Y | N | Y | Y | Y | Y | Y | Y | Y | N | N | Y | Y | N | Y | Y |
| Did the review authors provide a satisfactory explanation for, and discussion of, any heterogeneity observed in the results of the review? | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | Y |
| If they performed quantitative synthesis did the review authors carry out an adequate investigation of publication bias (small study bias) and discuss its likely impact on the results of the review? | Nm | Nm | N | N | N | N | Nm | Nm | Y | N | Nm | Nm | Nm | Nm | Nm | Y |
| Did the review authors report any potential sources of conflict of interest, including any funding they received for conducting the review? | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | Y |
| OVERALL QUALITY ASSESSMENT | M | CL | H | H | H | H | M | M | H | L | CL | M | M | CL | M | H |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gasparro, R.; Di Lauro, A.E.; Campana, M.D.; Rosiello, N.; Mariniello, M.; Sammartino, G.; Marenzi, G. Effectiveness of Autologous Platelet Concentrates in the Sinus Lift Surgery: Findings from Systematic Reviews and Meta-Analyses. Dent. J. 2024, 12, 101. https://doi.org/10.3390/dj12040101
Gasparro R, Di Lauro AE, Campana MD, Rosiello N, Mariniello M, Sammartino G, Marenzi G. Effectiveness of Autologous Platelet Concentrates in the Sinus Lift Surgery: Findings from Systematic Reviews and Meta-Analyses. Dentistry Journal. 2024; 12(4):101. https://doi.org/10.3390/dj12040101
Chicago/Turabian StyleGasparro, Roberta, Alessandro Espedito Di Lauro, Maria Domenica Campana, Nicola Rosiello, Mauro Mariniello, Gilberto Sammartino, and Gaetano Marenzi. 2024. "Effectiveness of Autologous Platelet Concentrates in the Sinus Lift Surgery: Findings from Systematic Reviews and Meta-Analyses" Dentistry Journal 12, no. 4: 101. https://doi.org/10.3390/dj12040101
APA StyleGasparro, R., Di Lauro, A. E., Campana, M. D., Rosiello, N., Mariniello, M., Sammartino, G., & Marenzi, G. (2024). Effectiveness of Autologous Platelet Concentrates in the Sinus Lift Surgery: Findings from Systematic Reviews and Meta-Analyses. Dentistry Journal, 12(4), 101. https://doi.org/10.3390/dj12040101