Evaluation of an In Situ Hardening β-Tricalcium Phosphate Graft Material for Alveolar Ridge Preservation. A Histomorphometric Animal Study in Pigs

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
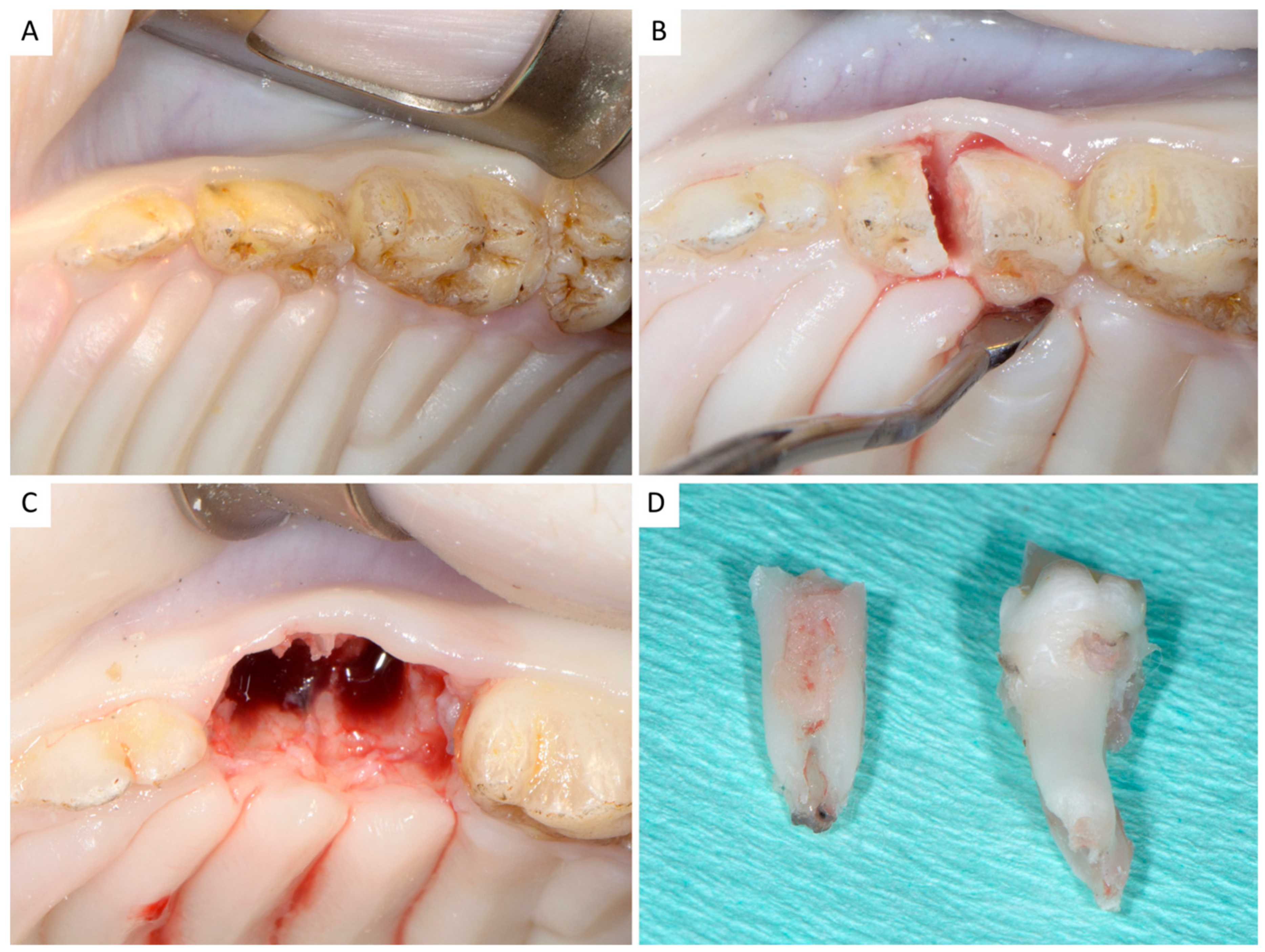
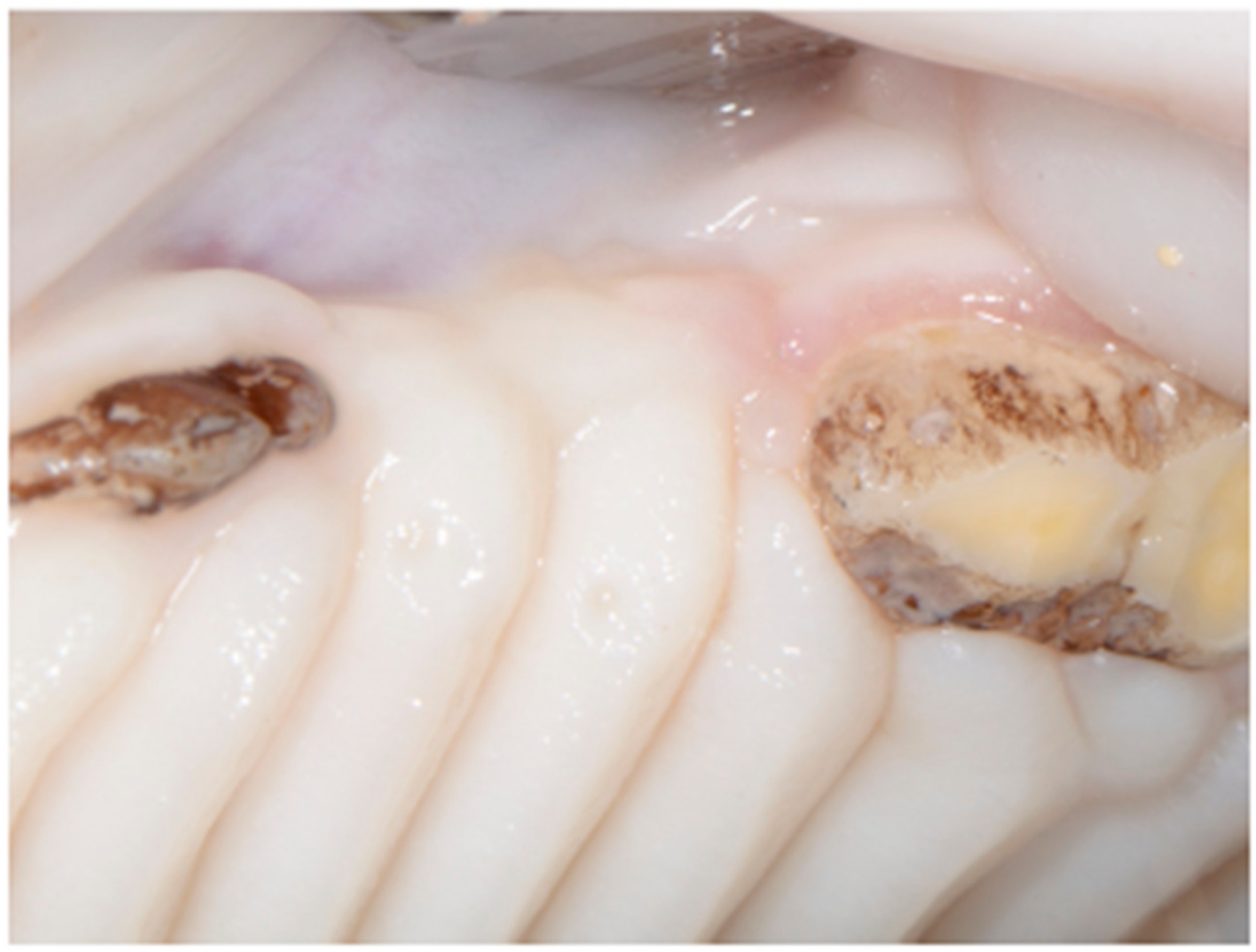
2.1. Surgical Procedures
2.2. Histological and Histomorphometric Evaluation
2.3. Statistical Analysis
3. Results
3.1. Overall
3.2. Alveolar Ridge Dimensional Changes
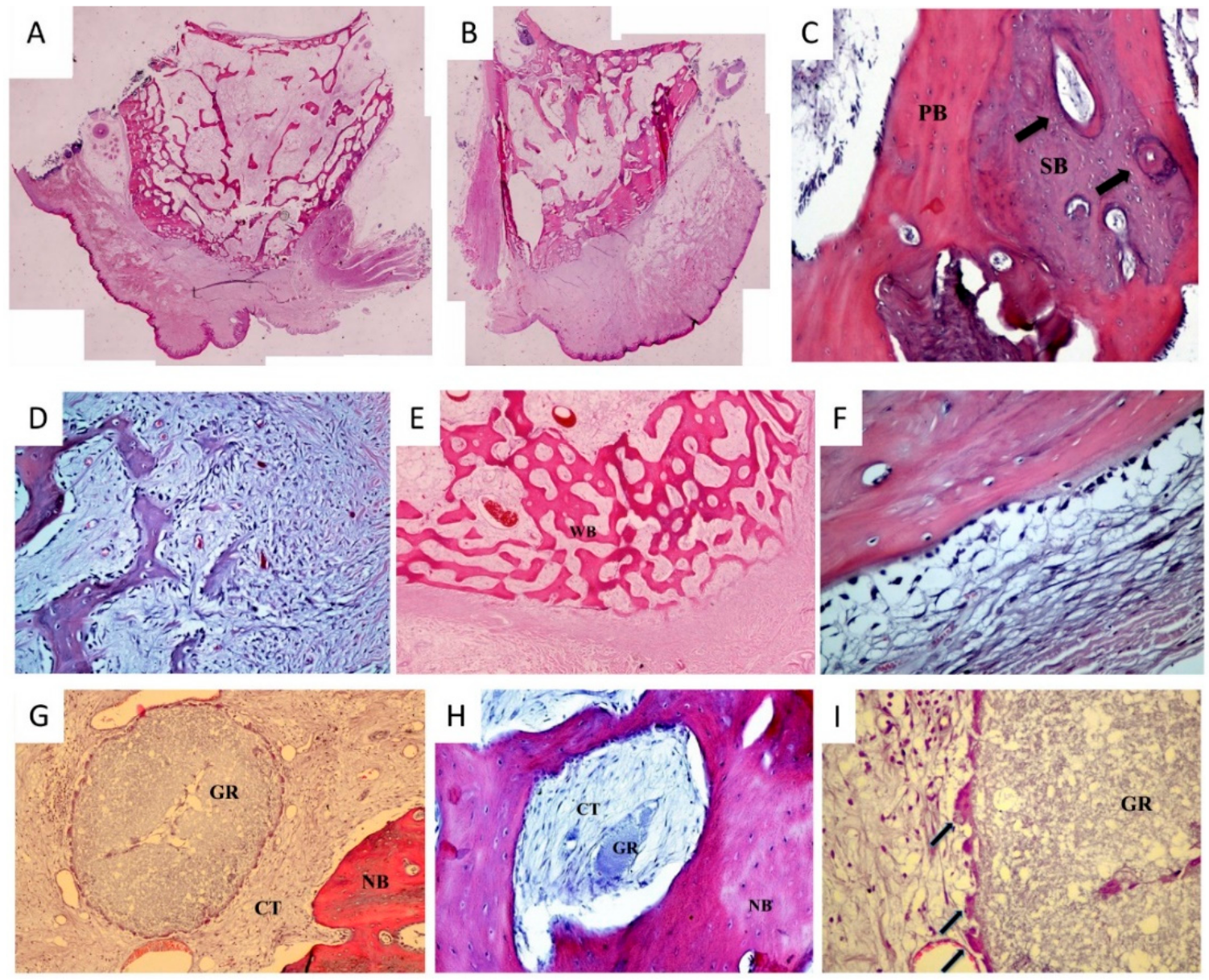
3.3. Histology
3.4. Histomorphometry
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Jambhekar, S.; Kernen, F.; Bidra, A.S. Clinical and histologic outcomes of socket grafting after flapless tooth extraction: A systematic review of randomized controlled clinical trials. J. Prosthet. Dent. 2015, 113, 371–382. [Google Scholar] [CrossRef] [PubMed]
- Vittorini Orgeas, G.; Clementini, M.; De Risi, V.; De Sanctis, M. Surgical techniques for alveolar socket preservation: A systematic review. Int. J. Oral Maxillofac. Implants 2013, 28, 1049–1061. [Google Scholar] [CrossRef] [PubMed]
- Horváth, A.; Mardas, N.; Mezzomo, L.A.; Needleman, I.G.; Donos, N. Alveolar ridge preservation. A systematic review. Clin. Oral Investig. 2013, 17, 341–363. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.E.; Lang, N.P. Ridge preservation after tooth extraction. Clin. Oral Implants Res. 2012, 23 (Suppl. 6), 147–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fickl, S.; Zuhr, O.; Wachtel, H.; Bolz, W.; Huerzeler, M.B. Hard tissue alterations after socket preservation: An experimental study in the beagle dog. Clin. Oral Implants Res. 2008, 19, 1111–1118. [Google Scholar] [CrossRef] [PubMed]
- Keith, J.D., Jr.; Salama, M.A. Ridge preservation and augmentation using regenerative materials to enhance implant predictability and esthetics. Compend. Contin. Educ. Dent. 2007, 28, 614–621. [Google Scholar] [PubMed]
- Horowitz, R.; Holtzclaw, D.; Rosen, P.S. A review on alveolar ridge preservation following tooth extraction. J. Evid. Based Dent. Pract. 2012, 12 (Suppl. 3), 149–160. [Google Scholar] [CrossRef]
- Horowitz, R.A.; Leventis, M.D.; Rohrer, M.D.; Prasad, H.S. Bone grafting: History, rationale, and selection of materials and techniques. Compend. Contin. Educ. Dent. 2014, 35 (Suppl. 4), 1–6. [Google Scholar] [PubMed]
- Collins, J.R.; Jiménez, E.; Martínez, C.; Polanco, R.T.; Hirata, R.; Mousa, R.; Coelho, P.G.; Bonfante, E.A.; Tovar, N. Clinical and histological evaluation of socket grafting using different types of bone substitute in adult patients. Implant Dent. 2014, 23, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Barallat, L.; Ruiz-Magaz, V.; Levi, P.A., Jr.; Mareque-Bueno, S.; Galindo-Moreno, P.; Nart, J. Histomorphometric results in ridge preservation procedures comparing various graft materials in extraction sockets with nongrafted sockets in humans: A systematic review. Implant Dent. 2014, 23, 539–554. [Google Scholar] [CrossRef] [PubMed]
- Yip, I.; Ma, L.; Mattheos, N.; Dard, M.; Lang, N.P. Defect healing with various bone substitutes. Clin. Oral Implants Res. 2015, 26, 606–614. [Google Scholar] [CrossRef] [PubMed]
- Valkova, V.; Ubaidha Maheen, C.; Pommer, B.; Rausch-Fan, X.; Seeman, R. Hot Topics in Clinical Oral Implants Research: Recent Trends in Literature Coverage. Dent. J. 2016, 4, E13. [Google Scholar] [CrossRef] [PubMed]
- Gao, C.; Peng, S.; Feng, P.; Shuai, C. Bone biomaterials and interactions with stem cells. Bone Res. 2017, 5, 17059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Araújo, M.G.; Liljenberg, B.; Lindhe, J. β-tricalcium phosphate in the early phase of socket healing: An experimental study in the dog. Clin. Oral Implants Res. 2010, 21, 445–454. [Google Scholar] [CrossRef] [PubMed]
- Harel, N.; Moses, O.; Palti, A.; Ormianer, Z. Long-term results of implants immediately placed into extraction sockets grafted with β-tricalcium phosphate: A retrospective study. J. Oral Maxillofac. Surg. 2013, 71, E63–E68. [Google Scholar] [CrossRef] [PubMed]
- Trisi, P.; Rao, W.; Rebaudi, A.; Fiore, P. Histologic effect of pure-phase beta-tricalcium phosphate on bone regeneration in human artificial jawbone defects. Int. J. Periodontics Restor. Dent. 2003, 23, 69–78. [Google Scholar]
- Henkel, J.; Woodruff, M.A.; Epari, D.R.; Steck, R.; Glatt, V.; Dickinson, I.C.; Choong, P.F.; Schuetz, M.A.; Hutmacher, D.W. Bone regeneration based on tissue engineering conceptions—A 21st century perspective. Bone Res. 2013, 1, 216–248. [Google Scholar] [CrossRef] [PubMed]
- Yuan, H.; Fernandes, H.; Habibovic, P.; de Boer, J.; Barradas, A.M.; de Ruiter, A.; Walsh, W.R.; van Blitterswijk, C.A.; de Bruijn, J.D. Osteoinductive ceramics as a synthetic alternative to autologous bone grafting. Proc. Nat. Acad. Sci. USA 2010, 107, 13614–13619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miron, R.J.; Zhang, Q.; Sculean, A.; Buser, D.; Pippenger, B.E.; Dard, M.; Shirakata, Y.; Chandad, F.; Zhang, Y. Osteoinductive potential of 4 commonly employed bone grafts. Clin. Oral Investig. 2016, 20, 2259–2265. [Google Scholar] [CrossRef] [PubMed]
- Barradas, A.M.; Yuan, H.; van Blitterswijk, C.; Habibovic, P. Osteoinductive biomaterials: Current knowledge of properties, experimental models and biological mechanisms. Eur. Cell. Mater. 2010, 21, 407–429. [Google Scholar] [CrossRef]
- Malhotra, A.; Habibovic, P. Calcium phosphates and angiogenesis: Implications and advances for bone regeneration. Trends Biotechnol. 2016, 34, 983–992. [Google Scholar] [CrossRef] [PubMed]
- Palti, A.; Hoch, T. A concept for the treatment of various dental bone defects. Implant Dent. 2002, 11, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Fairbairn, P.; Leventis, M. Protocol for Bone Augmentation with Simultaneous Early Implant Placement: A Retrospective Multicenter Clinical Study. Int. J. Dent. 2015, 2015, 589135. [Google Scholar] [CrossRef] [PubMed]
- Leventis, M.D.; Fairbairn, P.; Kakar, A.; Leventis, A.D.; Margaritis, V.; Lückerath, W.; Horowitz, R.A.; Rao, B.H.; Lindner, A.; Nagursky, H. Minimally invasive alveolar ridge preservation utilizing an in situ hardening β-tricalcium phosphate bone substitute: A multicenter case series. Int. J. Dent. 2016, 2016, 5406736. [Google Scholar] [CrossRef] [PubMed]
- Schmidlin, P.R.; Nicholls, F.; Kruse, A.; Zwahlen, R.A.; Weber, F.E. Evaluation of moldable, in situ hardening calcium phosphate bone graft substitutes. Clin. Oral Implants Res. 2013, 24, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Khan, R.; Witek, L.; Breit, M.; Colon, D.; Tovar, N.; Janal, M.N.; Jimbo, R.; Coelho, P.G. Bone regenerative potential of modified biphasic graft materials. Implant Dent. 2015, 24, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Kakar, A.; Rao, B.H.S.; Hegde, S.; Deshpande, N.; Lindner, A.; Nagursky, H.; Patney, A.; Mahajan, H. Ridge preservation using an in situ hardening biphasic calcium phosphate (β-TCP/HA) bone graft substitute—A clinical, radiological, and histological study. Int. J. Implant Dent. 2017, 3, 25. [Google Scholar] [CrossRef] [PubMed]
- Ruffieux, K. New syringe-delivered, moldable, alloplastic bone graft substitute. Compend. Contin. Educ. Dent. 2014, 35 (Suppl. 4), 8–10. [Google Scholar] [PubMed]
- Murray, K.A.; Collins, M.N.; O’Sullivan, R.P.; Ren, G.; Devine, D.M.; Murphy, A.; Sadło, J.; O’Sullivan, C.; McEvoy, B.; Vrain, O.; et al. Influence of gamma and electron beam sterilization on the stability of a premixed injectable calcium phosphate cement for trauma indications. J. Mech. Behav. Biomed. Mater. 2018, 77, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Dimitriou, R.; Mataliotakis, G.I.; Calori, G.M.; Giannoudis, P.V. The role of barrier membranes for guided bone regeneration and restoration of large bone defects: Current experimental and clinical evidence. BMC Med. 2012, 10, 81. [Google Scholar] [CrossRef] [PubMed]
- Giannoudis, P.V.; Einhorn, T.A.; Marsh, D. Fracture healing: The diamond concept. Injury 2007, 38, S3–S6. [Google Scholar] [CrossRef]
- Troedhan, A.; Schlichting, I.; Kurrek, A.; Wainwright, M. Primary implant stability in augmented sinuslift-sites after completed bone regeneration: A randomized controlled clinical study comparing four subantrally inserted biomaterials. Sci. Rep. 2014, 4, 5877. [Google Scholar] [CrossRef] [PubMed]
- Carmagnola, D.; Adriaens, P.; Berglundh, T. Healing of human extraction sockets filled with Bio-Oss. Clin. Oral Implants Res. 2003, 14, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.Y.; Lee, J.S.; Pang, E.K.; Jung, U.W.; Choi, S.H.; Kim, C.K. Impact of different synthetic bone fillers on healing of extraction sockets: An experimental study in dogs. Clin. Oral Implants Res. 2014, 25, E30–E37. [Google Scholar] [CrossRef] [PubMed]
- Araújo, M.G.; Lindhe, J. Ridge preservation with the use of Bio-Oss collagen: A 6-month study in the dog. Clin. Oral Implants Res. 2009, 20, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Chan, H.L.; Lin, G.H.; Fu, J.H.; Wang, H.L. Alterations in bone quality after socket preservation with grafting materials: A systematic review. Int. J. Oral Maxillofac. Implants 2013, 28, 710–720. [Google Scholar] [CrossRef] [PubMed]
- Artzi, Z.; Weinreb, M.; Givol, N.; Rohrer, M.D.; Nemcovsky, C.E.; Prasad, H.S.; Tal, H. Biomaterial Resorption Rate and Healing Site Morphology of Inorganic Bovine Bone and β-Tricalcium Phosphate in the Canine: A 24-month Longitudinal Histologic Study and Morphometric Analysis. Int. J. Oral Maxillofac. Implants 2004, 19, 357–368. [Google Scholar] [PubMed]
- Jensen, S.S.; Broggini, N.; Hjørting-Hansen, E.; Schenk, R.; Buser, D. Bone healing and graft resorption of autograft, anorganic bovine bone and beta-tricalcium phosphate. A histologic and histomorphometric study in the mandibles of minipigs. Clin. Oral Implants Res. 2006, 17, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Leventis, M.D.; Fairbairn, P.; Horowitz, R.A. Extraction site preservation using an in-situ hardening alloplastic bone graft substitute. Compend. Contin. Educ. Dent. 2014, 35 (Suppl. 4), 11–13. [Google Scholar] [PubMed]
- Schropp, L.; Wenzel, A.; Kostopoulos, L.; Karring, T. Bone healing and soft tissue contour changes following single-tooth extraction: A clinical and radiographic 12-month prospective study. Int. J. Periodontics Restor. Dent. 2003, 23, 313–323. [Google Scholar]
- Tan, W.L.; Wong, T.L.; Wong, M.C.; Lang, N.P. A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. Clin. Oral Implants Res. 2012, 23 (Suppl. 5), 1–21. [Google Scholar] [CrossRef] [PubMed]
- Elian, N.; Cho, S.C.; Froum, S.; Smith, R.B.; Tarnow, D.P. A simplified socket classification and repair technique. Pract. Proced. Aesthet. Dent. 2007, 19, 99–104. [Google Scholar] [PubMed]
- Huynh-Ba, G.; Pjetursson, B.E.; Sanz, M.; Cecchinato, D.; Ferrus, J.; Lindhe, J.; Lang, N.P. Analysis of the socket bone wall dimensions in the upper maxilla in relation to immediate implant placement. Clin Oral Implants Res. 2010, 21, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Tarnow, D.P.; Chu, S.J. Human histologic verification of osseointegration of an immediate implant placed into a fresh extraction socket with excessive gap distance without primary flap closure, graft, or membrane: A case report. Int. J. Periodontics Restor. Dent. 2011, 31, 515–521. [Google Scholar]
- Naenni, N.; Sapata, V.; Bienz, S.P.; Leventis, M.; Jung, R.; Hämmerle, C.H.; Thoma, D.S. Effect of flapless ridge preservation with two different alloplastic materials in sockets with buccal dehiscence defects—Volumetric and linear changes. Clin. Oral Investig. 2017, 22, 2187–2197. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N | Mean (mm) | SD | p-Value | |
|---|---|---|---|---|
| Initial | ||||
| Graft | 10 | 7.93 | 0.44 | 0.319 |
| Control | 4 | 7.63 | 0.63 | |
| 12 weeks postop | ||||
| Graft | 10 | 7.32 | 0.59 | 0.233 |
| Control | 4 | 6.93 | 0.29 | |
| N | Mean (%) | SD | p-Value | |
|---|---|---|---|---|
| Initial to 12 weeks postop | ||||
| Graft | 10 | −7.69 | 5.46 | 0.727 |
| Control | 4 | −8.86 | 5.92 | |
| Parameter | Group | N | Mean | SD | p-Value |
|---|---|---|---|---|---|
| New bone % | Graft | 10 | 20.33 | 8.10 | 0.268 |
| Control | 4 | 15.40 | 3.01 | ||
| Connective tissue % | Graft | 10 | 76.24 | 10.01 | 0.198 |
| Control | 4 | 83.26 | 1.63 | ||
| Residual graft % | Graft | 10 | 0.26 | 0.38 | - |
| Control | 4 | - | - |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leventis, M.; Agrogiannis, G.; Fairbairn, P.; Vasiliadis, O.; Papavasileiou, D.; Theodoropoulou, E.; Horowitz, R.; Kalyvas, D. Evaluation of an In Situ Hardening β-Tricalcium Phosphate Graft Material for Alveolar Ridge Preservation. A Histomorphometric Animal Study in Pigs. Dent. J. 2018, 6, 27. https://doi.org/10.3390/dj6030027
Leventis M, Agrogiannis G, Fairbairn P, Vasiliadis O, Papavasileiou D, Theodoropoulou E, Horowitz R, Kalyvas D. Evaluation of an In Situ Hardening β-Tricalcium Phosphate Graft Material for Alveolar Ridge Preservation. A Histomorphometric Animal Study in Pigs. Dentistry Journal. 2018; 6(3):27. https://doi.org/10.3390/dj6030027
Chicago/Turabian StyleLeventis, Minas, George Agrogiannis, Peter Fairbairn, Orestis Vasiliadis, Danai Papavasileiou, Evangelia Theodoropoulou, Robert Horowitz, and Demos Kalyvas. 2018. "Evaluation of an In Situ Hardening β-Tricalcium Phosphate Graft Material for Alveolar Ridge Preservation. A Histomorphometric Animal Study in Pigs" Dentistry Journal 6, no. 3: 27. https://doi.org/10.3390/dj6030027
APA StyleLeventis, M., Agrogiannis, G., Fairbairn, P., Vasiliadis, O., Papavasileiou, D., Theodoropoulou, E., Horowitz, R., & Kalyvas, D. (2018). Evaluation of an In Situ Hardening β-Tricalcium Phosphate Graft Material for Alveolar Ridge Preservation. A Histomorphometric Animal Study in Pigs. Dentistry Journal, 6(3), 27. https://doi.org/10.3390/dj6030027