Light Activated Disinfection in Root Canal Treatment—A Focused Review



Abstract
:1. Introduction
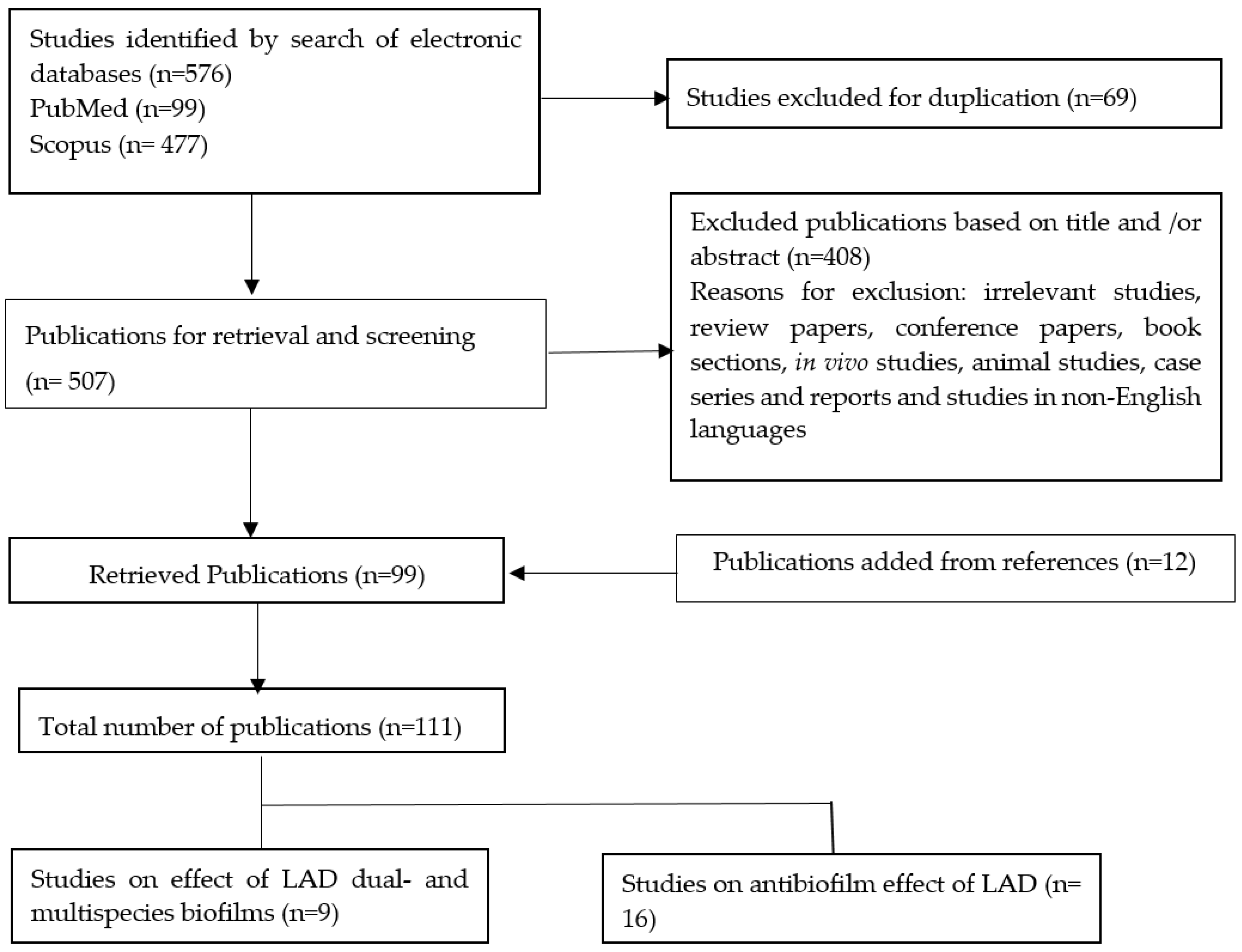
2. Methods
3. Results
3.1. Effect of LAD on Dual and Multispecies Biofilm
3.2. Antibioiflm Effect of Light Activated Disinfection
- -
- Inhibition or reduction of the biofilm formation of the target microorganisms in response to LAD; and/or
- -
- changes in biofilm characteristics, such as thickness, biomass, biovolume, and biofilm architecture in response to LAD.
4. Discussion
4.1. Effect of LAD on Dual and Multispecies Biofilm
4.2. Antibiofilm Effect of Light Activated Disinfection
4.2.1. Methylene Blue
4.2.2. Chitosan Rose Bengal Conjugate
4.2.3. Indocyanine Green (ICG) and Its Modifications
4.2.4. Curcumin
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bystrom, A.; Sundqvist, G. Bacteriologic evaluation of the efficacy of mechanical root canal instrumentation in endodontic therapy. Scand. J. Dent. Res. 1981, 89, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Nair, P.N.; Henry, S.; Cano, V.; Vera, J. Microbial status of apical root canal system of human mandibular first molars with primary apical periodontitis after “one-visit” endodontic treatment. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2005, 99, 231–252. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, J.F., Jr.; Rocas, I.N. Clinical implications and microbiology of bacterial persistence after treatment procedures. J. Endod. 2008, 34, 1291.e3–1301.e3. [Google Scholar] [CrossRef] [PubMed]
- Neelakantan, P.; Romero, M.; Vera, J.; Daood, U.; Khan, A.U.; Yan, A.; Cheung, G.S.P. Biofilms in endodontics-current status and future directions. Int. J. Mol. Sci. 2017, 18. [Google Scholar] [CrossRef] [PubMed]
- Donlan, R.M.; Costerton, J.W. Biofilms: Survival mechanisms of clinically relevant microorganisms. Clin. Microbiol. Rev. 2002, 15, 167–193. [Google Scholar] [CrossRef] [PubMed]
- Flemming, H.C.; Neu, T.R.; Wozniak, D.J. The EPS matrix: The “house of biofilm cells”. J. Bacteriol. 2007, 189, 7945–7947. [Google Scholar] [CrossRef] [PubMed]
- Zehnder, M. Root canal irrigants. J. Endod. 2006, 32, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Neelakantan, P.; Cheng, C.Q.; Ravichandran, V.; Mao, T.; Sriraman, P.; Sridharan, S.; Subbarao, C.; Sharma, S.; Kishen, A. Photoactivation of curcumin and sodium hypochlorite to enhance antibiofilm efficacy in root canal dentin. Photodiagn. Photodyn. Ther. 2015, 12, 108–114. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, A.; Kishen, A. Polycationic chitosan-conjugated photosensitizer for antibacterial photodynamic therapy. Photochem. Photobiol. 2012, 88, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Kishen, A.; Shrestha, A.; Cohenca, N. Emerging technologies in root canal disinfection. In Disinfection of Root Canal Systems: The Treatment of Apical Periodontitis; Cohenca, N., Ed.; Wiley Blackwell: Hoboken, NJ, USA, 2014; pp. 277–296. ISBN 9781118914014. [Google Scholar]
- Cieplik, F.; Tabenski, L.; Buchalla, W.; Maisch, T. Antimicrobial photodynamic therapy for inactivation of biofilms formed by oral key pathogens. Front. Microbiol. 2014, 5, 405. [Google Scholar] [CrossRef] [PubMed]
- Dai, T.; Huang, Y.Y.; Hamblin, M.R. Photodynamic therapy for localized infections-state of the art. Photodiagn. Photodyn. Ther. 2009, 6, 170–188. [Google Scholar] [CrossRef] [PubMed]
- Maisch, T.; Baier, J.; Franz, B.; Maier, M.; Landthaler, M.; Szeimies, R.M.; Baumler, W. The role of singlet oxygen and oxygen concentration in photodynamic inactivation of bacteria. Proc. Natl. Acad. Sci. USA 2007, 104, 7223–7228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Upadya, M.H.; Kishen, A. Influence of bacterial growth modes on the susceptibility to light-activated disinfection. Int. Endod. J. 2010, 43, 978–987. [Google Scholar] [CrossRef] [PubMed]
- Garcez, A.S.; Núñez, S.C.; Azambuja, N.; Fregnani, E.R.; Rodriguez, H.M.H.; Hamblin, M.R.; Suzuki, H.; Ribeiro, M.S. Effects of photodynamic therapy on gram-positive and gram-negative bacterial biofilms by bioluminescence imaging and scanning electron microscopic analysis. Photomed. Laser Surg. 2013, 31, 519–525. [Google Scholar] [CrossRef] [PubMed]
- Diogo, P.; Fernandes, C.; Caramelo, F.; Mota, M.; Miranda, I.M.; Faustino, M.A.F.; Neves, M.; Uliana, M.P.; de Oliveira, K.T.; Santos, J.M.; et al. Antimicrobial photodynamic therapy against endodontic enterococcus faecalis and candida albicans mono and mixed biofilms in the presence of photosensitizers: A comparative study with classical endodontic irrigants. Front. Microbiol. 2017, 8, 498. [Google Scholar] [CrossRef] [PubMed]
- Rosa, R.A.D.; Santini, M.F.; Figueiredo, J.A.P.; Visioli, F.; Pereira, J.R.; Vivan, R.R.; Montagner, F.; So, M.V.R. Effectiveness of photodynamic therapy associated with irrigants over two biofilm models. Photodiagn. Photodyn. Ther. 2017, 20, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, A.; Kishen, A. Antibiofilm efficacy of photosensitizer-functionalized bioactive nanoparticles on multispecies biofilm. J. Endod. 2014, 40, 1604–1610. [Google Scholar] [CrossRef] [PubMed]
- Ng, R.; Singh, F.; Papamanou, D.A.; Song, X.; Patel, C.; Holewa, C.; Patel, N.; Klepac-Ceraj, V.; Fontana, C.R.; Kent, R.; et al. Endodontic photodynamic therapy ex vivo. J. Endod. 2011, 37, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Stojicic, S.; Amorim, H.; Shen, Y.; Haapasalo, M. Ex vivo killing of enterococcus faecalis and mixed plaque bacteria in planktonic and biofilm culture by modified photoactivated disinfection. Int. Endod. J. 2013, 46, 649–659. [Google Scholar] [CrossRef] [PubMed]
- Fimple, J.L.; Fontana, C.R.; Foschi, F.; Ruggiero, K.; Song, X.; Pagonis, T.C.; Tanner, A.C.R.; Kent, R.; Doukas, A.G.; Stashenko, P.P.; et al. Photodynamic treatment of endodontic polymicrobial infection in vitro. J. Endod. 2008, 34, 728–734. [Google Scholar] [CrossRef] [PubMed]
- Muhammad, O.H.; Chevalier, M.; Rocca, J.P.; Brulat-Bouchard, N.; Medioni, E. Photodynamic therapy versus ultrasonic irrigation: Interaction with endodontic microbial biofilm, an ex vivo study. Photodiagn. Photodyn. Ther. 2014, 11, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Schiffner, U.; Cachovan, G.; Bastian, J.; Sculean, A.; Eick, S. In vitro activity of photoactivated disinfection using a diode laser in infected root canals. Acta Odontol. Scand. 2014, 72, 673–680. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, B.P.; Aguiar, C.M.; Camara, A.C.; de Albuquerque, M.M.; Correia, A.C.; Soares, M.F. The efficacy of photodynamic therapy and sodium hypochlorite in root canal disinfection by a single-file instrumentation technique. Photodiagn. Photodyn. Ther. 2015, 12, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Hoedke, D.; Enseleit, C.; Gruner, D.; Dommisch, H.; Schlafer, S.; Dige, I.; Bitter, K. Effect of photodynamic therapy in combination with various irrigation protocols on an endodontic multispecies biofilm ex vivo. Int. Endod. J. 2018, 51 (Suppl. 1), e23–e34. [Google Scholar] [CrossRef] [PubMed]
- Diogo, P.; Goncalves, T.; Palma, P.; Santos, J.M. Photodynamic antimicrobial chemotherapy for root canal system asepsis: A narrative literature review. Int. J. Dent. 2015, 2015, 269205. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, A.; Kishen, A. The effect of tissue inhibitors on the antibacterial activity of chitosan nanoparticles and photodynamic therapy. J. Endod. 2012, 38, 1275–1278. [Google Scholar] [CrossRef] [PubMed]
- George, S.; Kishen, A. Augmenting the antibiofilm efficacy of advanced noninvasive light activated disinfection with emulsified oxidizer and oxygen carrier. J. Endod. 2008, 34, 1119–1123. [Google Scholar] [CrossRef] [PubMed]
- Kishen, A.; Upadya, M.; Tegos, G.P.; Hamblin, M.R. Efflux pump inhibitor potentiates antimicrobial photodynamic inactivation of enterococcus faecalis biofilm. Photochem. Photobiol. 2010, 86, 1343–1349. [Google Scholar] [CrossRef] [PubMed]
- Upadya, M.; Shrestha, A.; Kishen, A. Role of efflux pump inhibitors on the antibiofilm efficacy of calcium hydroxide, chitosan nanoparticles, and light-activated disinfection. J. Endod. 2011, 37, 1422–1426. [Google Scholar] [CrossRef] [PubMed]
- Pourhajibagher, M.; Chiniforush, N.; Shahabi, S.; Ghorbanzadeh, R.; Bahador, A. Sub-lethal doses of photodynamic therapy affect biofilm formation ability and metabolic activity of enterococcus faecalis. Photodiagn. Photodyn. Ther. 2016, 15, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, A.; Hamblin, M.R.; Kishen, A. Characterization of a conjugate between rose bengal and chitosan for targeted antibiofilm and tissue stabilization effects as a potential treatment of infected dentin. Antimicrob. Agents Chemother. 2012, 56, 4876–4884. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, A.; Hamblin, M.R.; Kishen, A. Photoactivated rose bengal functionalized chitosan nanoparticles produce antibacterial/biofilm activity and stabilize dentin-collagen. Nanomed. Nanotechnol. Biol. Med. 2014, 10, 491–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiniforush, N.; Pourhajibagher, M.; Parker, S.; Shahabi, S.; Bahador, A. The in vitro effect of antimicrobial photodynamic therapy with indocyanine green on enterococcus faecalis: Influence of a washing vs non-washing procedure. Photodiagn. Photodyn. Ther. 2016, 16, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Akbari, T.; Pourhajibagher, M.; Hosseini, F.; Chiniforush, N.; Gholibegloo, E.; Khoobi, M.; Shahabi, S.; Bahador, A. The effect of indocyanine green loaded on a novel nano-graphene oxide for high performance of photodynamic therapy against enterococcus faecalis. Photodiagn. Photodyn. Ther. 2017, 20, 148–153. [Google Scholar] [CrossRef] [PubMed]
- Devaraj, S.; Jagannathan, N.; Neelakantan, P. Antibiofilm efficacy of photoactivated curcumin, triple and double antibiotic paste, 2% chlorhexidine and calcium hydroxide against enterococcus fecalis in vitro. Sci. Rep. 2016, 6. [Google Scholar] [CrossRef] [PubMed]
- Lim, Z.; Cheng, J.L.; Lim, T.W.; Teo, E.G.; Wong, J.; George, S.; Kishen, A. Light activated disinfection: An alternative endodontic disinfection strategy. Aust. Dent. J. 2009, 54, 108–114. [Google Scholar] [CrossRef] [PubMed]
- George, S.; Kishen, A. Influence of photosensitizer solvent on the mechanisms of photoactivated killing of enterococcus faecalis. Photochem. Photobiol. 2008, 84, 734–740. [Google Scholar] [CrossRef] [PubMed]
- George, S.; Kishen, A. Photophysical, photochemical, and photobiological characterization of methylene blue formulations for light-activated root canal disinfection. J. Biomed. Opt. 2007, 12. [Google Scholar] [CrossRef] [PubMed]
- Veerapandian, M.; Yun, K. Functionalization of biomolecules on nanoparticles: Specialized for antibacterial applications. Appl. Microbiol. Biotechnol. 2011, 90, 1655–1667. [Google Scholar] [CrossRef] [PubMed]
- Rabea, E.I.; Badawy, M.E.T.; Stevens, C.V.; Smagghe, G.; Steurbaut, W. Chitosan as antimicrobial agent: Applications and mode of action. Biomacromolecules 2003, 4, 1457–1465. [Google Scholar] [CrossRef] [PubMed]
- Venugopal, J.; Prabhakaran, M.P.; Low, S.; Choon, A.T.; Zhang, Y.Z.; Deepika, G.; Ramakrishna, S. Nanotechnology for nanomedicine and delivery of drugs. Curr. Pharm. Des. 2008, 14, 2184–2200. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, A.; Kishen, A. Antibacterial nanoparticles in endodontics: A review. J. Endod. 2016, 42, 1417–1426. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, A.; Kishen, A. Antibacterial efficacy of photosensitizer functionalized biopolymeric nanoparticles in the presence of tissue inhibitors in root canal. J. Endod. 2014, 40, 566–570. [Google Scholar] [CrossRef] [PubMed]
- Kranz, S.; Huebsch, M.; Guellmar, A.; Voelpel, A.; Tonndorf-Martini, S.; Sigusch, B.W. Antibacterial photodynamic treatment of periodontopathogenic bacteria with indocyanine green and near-infrared laser light enhanced by trolox(tm). Lasers Surg. Med. 2015, 47, 350–360. [Google Scholar] [CrossRef] [PubMed]
- Ocsoy, I.; Isiklan, N.; Cansiz, S.; Ozdemir, N.; Tan, W. Icg-conjugated magnetic graphene oxide for dual photothermal and photodynamic therapy. RSC Adv. 2016, 6, 30285–30292. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-W.; Fu, Y.-Y.; Peng, Q.; Guo, S.-S.; Liu, G.; Li, J.; Yang, H.-H.; Chen, G.-N. Dye-enhanced graphene oxide for photothermal therapy and photoacoustic imaging. J. Mater. Chem. B 2013, 1, 5762–5767. [Google Scholar] [CrossRef]
- Tyagi, P.; Singh, M.; Kumari, H.; Kumari, A.; Mukhopadhyay, K. Bactericidal activity of curcumin i is associated with damaging of bacterial membrane. PLoS ONE 2015, 10, e0121313. [Google Scholar] [CrossRef] [PubMed]
- Santezi, C.; Reina, B.D.; Dovigo, L.N. Curcumin-mediated photodynamic therapy for the treatment of oral infections-a review. Photodiagn. Photodyn. Ther. 2018, 21, 409–415. [Google Scholar] [CrossRef] [PubMed]
- Da Frota, M.F.; Guerreiro-Tanomaru, J.M.; Tanomaru-Filho, M.; Bagnato, V.S.; Espir, C.G.; Berbert, F.L.C.V. Photodynamic therapy in root canals contaminated with enterococcus faecalis using curcumin as photosensitizer. Lasers Med. Sci. 2015, 30, 1867–1872. [Google Scholar] [CrossRef] [PubMed]
- Pileggi, G.; Wataha, J.C.; Girard, M.; Grad, I.; Schrenzel, J.; Lange, N.; Bouillaguet, S. Blue light-mediated inactivation of enterococcus faecalis in vitro. Photodiagn. Photodyn. Ther. 2013, 10, 134–140. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Search Builder | Words Used | Results |
|---|---|---|
| #1 | “root canal” OR dentin OR biofilm | 99,272 |
| #2 | photodynamic OR “photodynamic therapy” OR photosensitizers OR “light activated disinfection” OR “photo-activated disinfection” OR “photodynamic disinfection” OR “photodynamic therapy” AND endodontics OR “light activated disinfection” AND endodontics OR “light activated disinfection” AND “root canal” OR “photo-activated disinfection” AND “root canal” OR “photo-activated disinfection” AND endodontics | 54,750 |
| #3 | root canal irrigants” OR “endodontic irrigants” OR “intracanal medicaments” OR “root canal antiseptics” OR “intracanal dressings” OR “sodium hypochlorite” OR hypochlorite OR chlorhexidine OR alexidine OR MTAD OR Qmix OR “calcium hydroxide” OR “double antibiotic paste” OR “triple antibiotic paste | 26,078 |
| #4 | antibacterial OR antimicrobial OR antibiofilm | 1,614,194 |
| #5 | #1 AND #2 AND #3 AND #4 | 99 |
| Study | Biofilm Characteristics | Photosensitizer/Irradiation Parameters | Experimental Groups | Methods of Evaluation | Main Results |
|---|---|---|---|---|---|
| Fimple et al. [21] | Multispecies (72 h)
| MB (25 µg/mL) dissolved in BHI or PBS (with or without light activation) PIT: 10 min 665-nm diode laser PD: 10 mW/cm2 E: 30 J/cm2 Irradiation for 2.5 min, 2.5 min break, 2nd exposure for 2.5 min | No comparative groups. Only MB was tested | DNA probe analysis CFU CLSM |
|
| Ng et al. [19] | Multispecies (39 species from teeth with necrotic pulp and associated periradicular radiolucencies) | MB (50 µg/mL) 665-nm diode laser PD: 100 mW/cm2 E: 30 J/cm2 Irradiation for 2.5 min, 2.5 min break, 2nd exposure for 2.5 min |
| CFU and whole genomic probe assay | LAD after 6% NaOCl reduced bacterial survival and posttreatment detection levels compared to 6% NaOCl only |
| Garcez et al. [15] | Dual species (72 h)
| MB (60 µM dissolved in distilled water) PIT: 2 min 660-nm diode laser P: 40 mWE: 9.6 J Irradiation for 4 min | No comparative groups. Only MB was tested | SEM |
|
| Muhammad et al. [22] | Multispecies (7 days)
| TB PIT: 1 min Aseptium Plus® LED light Irradiation for 2 min. TB (15 µg/mL) PIT: 1 min 650-nm diode laser P: 60 mW Irradiation for 2 min | All root canals were disinfected with PUI using 17% EDTA and 2.6% NaOCl prior to LAD with TB | Microbiological sampling and culturing SEM |
|
| Schiffner et al. [23] |
| TB PIT: 2 min 632–644 nm red light. P: 200 mW. Irradiation for 1 min |
| CFU |
|
| Shrestha and Kishen [18] | Multispecies (21 days)
| RB (10 mmol/L) RBCnps (0.3 mg/mL) PIT: 15 min 540-nm fiber light E: 60 J/cm2 |
| SEM CLSM |
|
| De Oliveira et al. [24] | Multispecies (72 h)
| MB (15 µg/mL) PIT: 2 min 660-nm diode laser P: 100 mW E: 8 J/sample Irradiation for 90 s |
| CFU |
|
| Diogo et al. [16] | Dual species (48 h)
|
557-nm green LED light P: 42 mW/cm2 E: 3780 J/cm2
627-nm red LED light P:35 mW/cm2 E: 3150 J/cm2 Irradiation for 60 and 90 s |
| Safranin red assay Microscopic imaging techniques * |
|
| Hoedke et al. [25] | Multispecies (5 days)
| Phenothiazine chloride (10 mg/mL) PIT: 60 s 660-nm diode laser PD:100 mW/m2 E: 2.4 J/root canal Irradiation for 60 s. |
| CFU |
|
| Study | Biofilm Characteristics | Photosensitizer/Irradiation Parameters | Experimental Groups | Methods of Evaluation | Main Results |
|---|---|---|---|---|---|
| George and Kishen [28] | Enterococcus faecalis (7 days) | Water-based MB (100 µmol/L) Emulsion-based MB (*) PIT: 10 min 664-nm diode laser P: 30 mW E:31.84 J/cm2 |
| CLSM | Emulsion-based MBreduced biofilm thickness and caused marked biofilm disruption compared to water-based MB |
| Kishen et al. [29] | Enterococcus faecalis (4 days, 2 weeks) | MB, MB + EPI, and RB (100 µM) PIT: 15 min. Non-coherent light (660-nm for MB, 540-nm for RB) P: 300–600 mW E: 10–40 J/cm2 |
| CFU assay of biofilm cells and biofilm derived cells (4 days biofilm) CLSM (2 weeks biofilm) |
|
| Upadya and Kishen [14] | Enterococcus faecalis Pseudomonas aeruginosa Monospecies biofilms (2 weeks) | Water-based MBMIX-based MB (**) MB in MIX and Emulsion combination PIT: 15 min. 660-nm non-coherent light P: 0.106 W E: 2–40 J/cm 2 |
| CLSM |
|
| Upadya et al. [30] | Enterococcus faecalis (4 days) | MB, MB + EPI PIT: 15 min 660-nm non-coherent light P: 0.106 W E: 2–40 J/cm 2 |
| CFU assay of biofilm cells and biofilm derived cells |
|
| Shrestha and Kishen [9] | Enterococcus faecalis Pseudomonas aeruginosa Monospecies biofilm (7 days) | MB (10 µM) RB (10 µM) CSRB (0.3 mg/mL) White light source (540-nm for RB and CSRB, 660-nm for MB) E: 20, 40 and 60 J/cm2 (PIT: 15 min.) 40 J/cm2 (PIT: 30 and 60 min.) |
| CFU assay of biofilm cells CLSM |
|
| Shrestha et al. [32] | Enterococcus faecalis (7 days) | RB (10 µM) CSRB (0.3 mg/mL) PIT: 15 min. 540-nm light E: 20, 40 and 60 J/cm2 | RBCSRB | CFU assay of biofilm cells | CSRP induced a significantly higher LAD mediated bacterial killing compared to RB at 40 and 60 J/cm2 |
| Shrestha et al. [33] | Enterococcus faecalis (21 days) | RB (10 µM) RBCnps (0.1 and 0.3 mg/mL) PIT: 15 min. 540-nm light P: 50 mW E: 20, 40, 60 and fractionated dosage of 10 and 20 J/cm2 twice |
| CFU assay of biofilm cells CLSM |
|
| Neelakantan et al. [8] | Enterococcus faecalis (4 weeks) | Curcumin (2.5 mg/mL) 380–515 nm blue light E:1200 mW/cm2 Irradiation for 4 min |
| CLSM |
|
| Chiniforush et al. [34] | Enterococcus faecalis (24 h) | ICG (3–2000 µg/mL) PIT: 5 min 808-nm diode laser P: 250 mW E: 39.06 J/cm2 Irradiation for 60 s | No comparative groups Only ICG was tested | CV assay | Non-washed ICG induced higher reduction in biofilm formation, development and higher rate of biofilm degradation compared to washed ICG |
| Deveraj et al. [36] | Enterococcus faecalis (4 weeks) | Curcumin (2.5 mg/mL of polyethylene glycol) 380–315 nm blue light P: 1200 mW/cm2 Irradiation for 4 min |
| CLSM | Light activated curcumin and TAP reduced biofilm thickness, disrupted biofilm architecture and killed bacterial cells more than other medicaments |
| Pourhajibagher et al. [31] | Enterococcus faecalis (24 h) | Sublethal concentrations of TB, MB (6.2 µg/mL) and ICG (31.2 µg/mL) Diode laser: 660 nm (MB), 635 nm (TB) and 810 nm (ICG) P: 150 mW (MB), 220 mW (TBO) and 200 mW (ICG) E: 70.31 J/cm2 (MB) 103.12 J/cm2 (TBO) 15.62 J/cm2 (ICG) |
| CV assay SEM |
|
| Akbari et al. [35] | Enterococcus faecalis (24 h) | ICG (1000 µg/mL) NGO-ICG (200 µg/mL) 810-nm diode laser P: 250 mW E: 31.2 J/cm2 Irradiation for 60 s |
| CV assay | Photoactivated NGO-ICG reduced biofilm formation more than photoactivated ICG |
| Rosa et al. [17] | Multispecies biofilm developed intraorally (72 h) | 0.01%MB. PIT: 1 min 650-nm red diode laser P: 100 mW Irradiation for 1 min |
| CLSM | LAD after NaOCl reduced biofilm biovolume |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ali, I.A.A.; Neelakantan, P. Light Activated Disinfection in Root Canal Treatment—A Focused Review. Dent. J. 2018, 6, 31. https://doi.org/10.3390/dj6030031
Ali IAA, Neelakantan P. Light Activated Disinfection in Root Canal Treatment—A Focused Review. Dentistry Journal. 2018; 6(3):31. https://doi.org/10.3390/dj6030031
Chicago/Turabian StyleAli, Islam A. Abdelaziz, and Prasanna Neelakantan. 2018. "Light Activated Disinfection in Root Canal Treatment—A Focused Review" Dentistry Journal 6, no. 3: 31. https://doi.org/10.3390/dj6030031
APA StyleAli, I. A. A., & Neelakantan, P. (2018). Light Activated Disinfection in Root Canal Treatment—A Focused Review. Dentistry Journal, 6(3), 31. https://doi.org/10.3390/dj6030031