Experiences of Being a Parent to a Child with Amelogenesis Imperfecta

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Recruitment of Participants
2.2. Interviews
2.3. Thematic Analysis
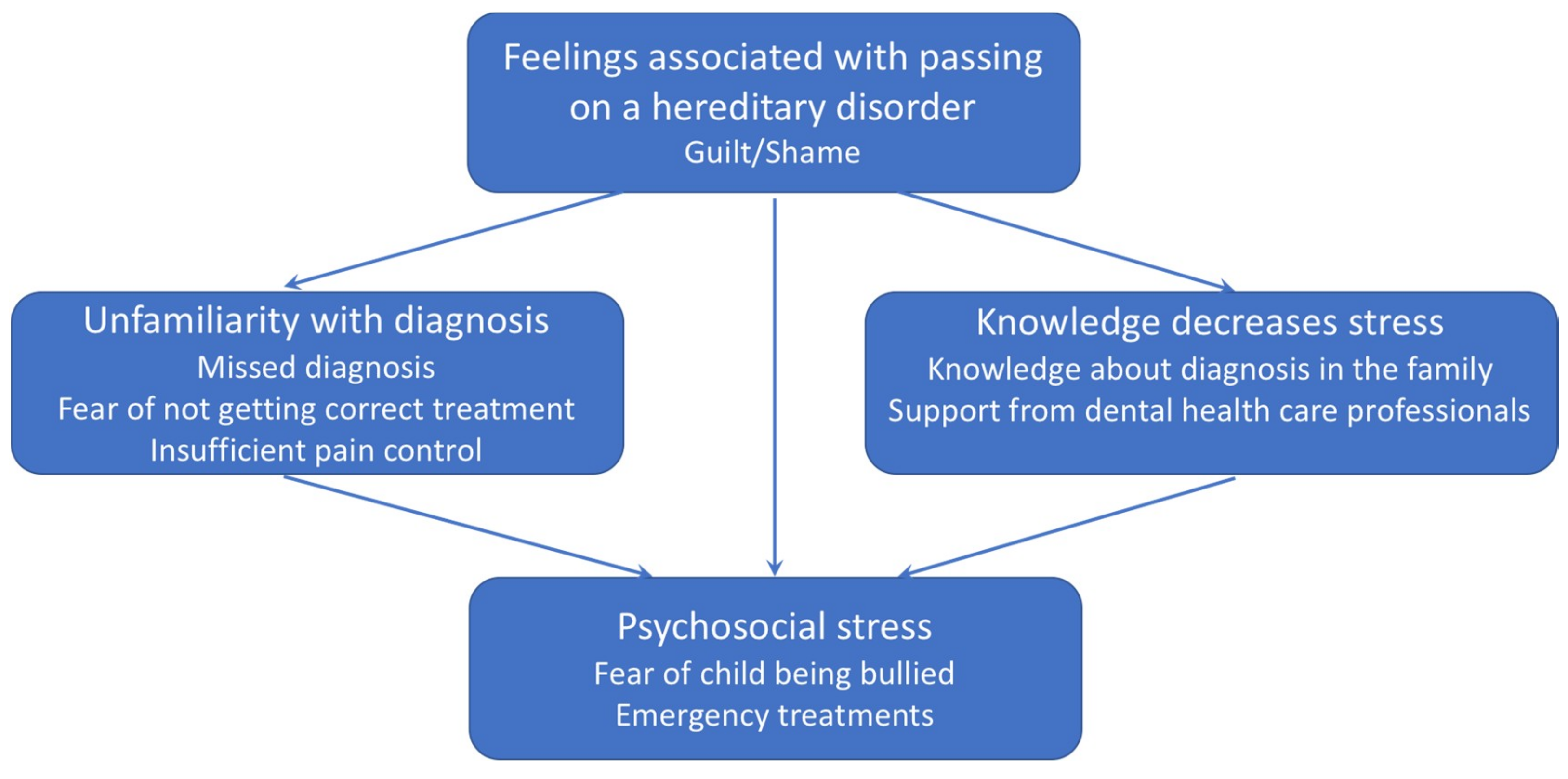
3. Results
3.1. Participants
3.2. Experience of Being a Parent to a Child with Severe AI
3.3. Feelings Associated with Passing on a Hereditary Disorder
Guilt/Shame
Now that he got the same as me, it was quite scary(John)
This has been something very difficult for my husband who also has the disease… that he has passed this on to his children, he finds this very difficult, he blames himself for it, of course…he says he shouldn’t have had children, because you don’t pass on bad genes, and in a way, I can understand his way of thinking… he feels it’s hard to have given something so bad to his children, something that they will live with for the rest of their lives.(Ann-Sofie)
My children have been angry with me saying ’why did I get your damn teeth?’(Monica)
I’m already worried about his children, he has not had any children yet but…you can’t really tell him not to have children just because of teeth…(John)
My husband said that he sometimes wished that you could genetically manipulate the children so that they would not get the disease.(Monica)
3.4. Knowledge Decreases Stress
3.4.1. Knowledge about Diagnosis in the Family
I knew [about having AI]…thanks to knowing that there were so many of my relatives having it(Sandra)
I knew there was something better [treatment], since I’ve experienced it myself.(Anita)
Now that we know and if Sara were to have a child, she will know where to look for help and so on. That’s nice.(Jessica)
3.4.2. Support from Dental Health Care Professionals
It was a young dentist, a girl, she had probably seen a lot in her schooling I can assume and she was curious. And she said straight away have you sought specialist care for this? I was like, finally someone reacts to this.(Christine)
When I got a new boss, and she just ’You go to the dentist so often with your daughter, do you really have to be away for a whole day? You really don’t want to see how she looks after a dental appointment, it doesn’t work to leave her at school in that state’. It would feel much better if you could give a leaflet that describes the disease and what it means for the patient. A lot of dental visits and a lot of problems.(Ann-Sofie)
3.5. Unfamiliarity with Diagnosis
3.5.1. Missed Diagnosis
Everyone knows what being lactose intolerant is or having celiac disease. If you are allergic to dogs everyone knows what it is, but if you say that you have AI people just go “okay so what is that?” I mean, no one has any idea of what it is.(Ann-Sofie)
I’ve experienced very little understanding and very little knowledge. Even though we are a small group, I think that if they are able to find out if there is a diagnosis in the records, they should be able to find out what it means.(Monica)
3.5.2. Fear of Not Getting the Correct Treatment
I was a bit annoyed, I can tell you, when they didn’t take it seriously, especially when I had told them … they did see how … how it looked … that can’t have looked normal in the eyes of a dentist either.(Sandra)
You should probably stand up for yourself as a parent if you notice that something is wrong, yeah but like in her case that you probably shouldn’t count on that the dentist, refer you instead you have to stand up for yourself and if you suspect these things, say that we want a specialist to look at this.(Jessica)
He is studying in Uppsala so I have to try to find a dentist for him there so he can go and check his teeth.(Sandra)
3.5.3. Insufficient Pain Control
We had to explain about pain and the pain threshold to the dentists, that maybe it’s not enough with one anesthetic injection when they have to treat a tooth.(Monica)
They probably thought we were demanding parents, that we were overprotective regarding our children. That we… were kind of troublesome. I felt that way.(Monica)
3.6. Psychosocial Stress
3.6.1. Fear of Child Being Bullied
Ugly teeth, sensitive teeth, broken teeth, fractures, cavities/decays and above all, so terribly ugly.(Annika)
He was really teased so he has never smiled in a photo because he was teased in school. They asked if he didn’t brush his teeth and other mean things.(Monica)
You have been teased […] both myself and my children.(Annika)
I threatened the principal of the school to make complaint to the police regarding the bullying she was exposed to, it was not only the teeth, it was everything. It was such a relief when she finished school.(Sandra)
3.6.2. Emergency Dental Visits
Yeah but well it’s been so very much, very much with those teeth, because sometimes they fall apart and she is in really bad pain and then we like have to drop work and go straight to the dentist, if we get an appointment.(Ann-Sofie)
The teeth have fractures just about any time and when the children were small it was like panic every time, they called from kindergarten and school when they’ve been at things so you just have to go to the dentist with like half a front tooth.(Anita)
If you travel and the teeth fracture… when Emma was younger, we had to go to the dentist time and time again. It was like if you were in another city it was like, is there an on-call dentist here?(Annika)
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Wright, J.T.; Torain, M.; Long, K.; Seow, K.; Crawford, P.; Aldred, M.J.; Hart, P.S.; Hart, T.C. Amelogenesis imperfecta: Genotype-phenotype studies in 71 families. Cells Tissues Organs 2011, 194, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Crawford, P.J.; Aldred, M.; Bloch-Zupan, A. Amelogenesis imperfecta. Orphanet J. Rare Dis. 2007, 2, 17. [Google Scholar] [CrossRef] [PubMed]
- McDonald, S.; Arkutu, N.; Malik, K.; Gadhia, K.; McKaig, S. Managing the paediatric patient with amelogenesis imperfecta. Br. Dent. J. 2012, 212, 425–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pousette Lundgren, G.; Dahllöf, G. Outcome of restorative treatment in young patients with amelogenesis imperfecta. a cross-sectional, retrospective study. J. Dent. 2014, 42, 1382–1389. [Google Scholar] [CrossRef] [PubMed]
- Coffield, K.D.; Phillips, C.; Brady, M.; Roberts, M.W.; Strauss, R.P.; Wright, J.T. The psychosocial impact of developmental dental defects in people with hereditary amelogenesis imperfecta. J. Am. Dent. Assoc. 2005, 136, 620–630. [Google Scholar] [CrossRef] [PubMed]
- Lundgren, G.P.; Wickström, A.; Hasselblad, T.; Dahllöf, G. Amelogenesis Imperfecta and Early Restorative Crown Therapy: An Interview Study with Adolescents and Young Adults on Their Experiences. PLoS ONE 2016, 11, e0156879. [Google Scholar]
- Pousette Lundgren, G.; Karsten, A.; Dahllöf, G. Oral health-related quality of life before and after crown therapy in young patients with amelogenesis imperfecta. Health Qual. Life Outcomes 2015, 13, 197. [Google Scholar] [CrossRef] [PubMed]
- Dogba, M.J.; Bedos, C.; Durigova, M.; Montpetit, K.; Wong, T.; Glorieux, F.H.; Rauch, F. The impact of severe osteogenesis imperfecta on the lives of young patients and their parents—A qualitative analysis. BMC Pediatr. 2013, 13, 153. [Google Scholar] [CrossRef]
- Cousino, M.K.; Hazen, R.A. Parenting stress among caregivers of children with chronic illness: A systematic review. J. Pediatr. Psychol. 2013, 38, 809–828. [Google Scholar] [CrossRef]
- Santos, M.C.D.; Pires, A.F.; Soares, K.; Barros, L. Family experience with osteogenesis imperfecta type 1: The most distressing situations. Disabil. Rehabil. 2018, 40, 2281–2287. [Google Scholar] [CrossRef]
- Pousette Lundgren, G.; Vestlund, G.M.; Dahllöf, G. Crown therapy in young individuals with amelogenesis imperfecta: Long term follow-up of a randomized controlled trial. J. Dent. 2018, 76, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Clarke, A. Anticipated stigma and blameless guilt: Mothers’ evaluation of life with the sex-linked disorder, hypohidrotic ectodermal dysplasia (XHED). Soc. Sci. Med. 2016, 158, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Trulsson, U.; Klingberg, G. Living with a child with a severe orofacial handicap: Experiences from the perspectives of parents. Eur. J. Oral. Sci. 2003, 111, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Bradford, R. Staff accuracy in predicting the concerns of parents of chronically ill children. Child Care Health Dev. 1991, 17, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Davies, R.; Davis, B.; Sibert, J. Parents’ stories of sensitive and insensitive care by paediatricians in the time leading up to and including diagnostic disclosure of a life-limiting condition in their child. Child Care Health Dev. 2003, 29, 77–82. [Google Scholar] [CrossRef]
- Graungaard, A.H.; Skov, L. Why do we need a diagnosis? A qualitative study of parents’ experiences, coping and needs, when the newborn child is severely disabled. Child Care Health Dev. 2007, 33, 296–307. [Google Scholar] [CrossRef]
- Wondimu, B.; Dahllöf, G. Attitudes of Swedish dentists to pain and pain management during dental treatment of children and adolescents. Eur. J. Paediatr. Dent. 2005, 6, 66–72. [Google Scholar]
- Ghanei, M.; Arnrup, K.; Robertson, A. Procedural pain in routine dental care for children: A part of the Swedish BITA study. Eur. Arch. Paediatr. Dent. 2018, 19, 365–372. [Google Scholar] [CrossRef]
- Hallberg, U.; Strandmark, M.; Klingberg, G. Dental health professionals’ treatment of children with disabilities: A qualitative study. Acta Odontol. Scand. 2004, 62, 319–327. [Google Scholar] [CrossRef]
- Tiemens, K.; Nicholas, D.; Forrest, C.R. Living with difference: Experiences of adolescent girls with cleft lip and palate. Cleft Palate Craniofac. J. 2013, 50, e27–e34. [Google Scholar] [CrossRef] [PubMed]
- Sneller, J.; Buchanan, H.; Parekh, S. The impact of amelogenesis imperfecta and support needs of adolescents with AI and their parents: An exploratory study. Int. J. Paediatr. Dent. 2014, 24, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Patton, M. Qualitative Research & Evaluation Methods; SAGE: Thousand Oaks, CA, USA, 2015. [Google Scholar]


{kind=link}
| Name | Sex | Age | Parental AI | Number of Children | Children with AI |
|---|---|---|---|---|---|
| Annika | F | 52 | Yes | 1F/1M | 2/2 |
| Monica | F | 45 | No ** | 1F/2M | 2/3 |
| Ann-Sofie | F | 43 | Yes | 1F/2M | 2/3 |
| Sandra | F | 50 | Yes | 1F/1M | 2/2 |
| Christine | F | 48 | No ** | 2F | 1/2 |
| Jessica | F | 45 | Yes * | 1F/1M | 1/2 |
| John | M | 50 | Yes | 1M | 1/1 |
| Anita | F | 45 | Yes | 3F | 3/3 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pousette Lundgren, G.; Hasselblad, T.; Johansson, A.S.; Johansson, A.; Dahllöf, G. Experiences of Being a Parent to a Child with Amelogenesis Imperfecta. Dent. J. 2019, 7, 17. https://doi.org/10.3390/dj7010017
Pousette Lundgren G, Hasselblad T, Johansson AS, Johansson A, Dahllöf G. Experiences of Being a Parent to a Child with Amelogenesis Imperfecta. Dentistry Journal. 2019; 7(1):17. https://doi.org/10.3390/dj7010017
Chicago/Turabian StylePousette Lundgren, Gunilla, Tove Hasselblad, Anna Stigsdotter Johansson, Anna Johansson, and Göran Dahllöf. 2019. "Experiences of Being a Parent to a Child with Amelogenesis Imperfecta" Dentistry Journal 7, no. 1: 17. https://doi.org/10.3390/dj7010017
APA StylePousette Lundgren, G., Hasselblad, T., Johansson, A. S., Johansson, A., & Dahllöf, G. (2019). Experiences of Being a Parent to a Child with Amelogenesis Imperfecta. Dentistry Journal, 7(1), 17. https://doi.org/10.3390/dj7010017