Dentinal Hypersensitivity Treatment Using Diode Laser 980 nm: In Vivo Study

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Statistical Analysis
2.2. Pulp Temperature Increase Measurements
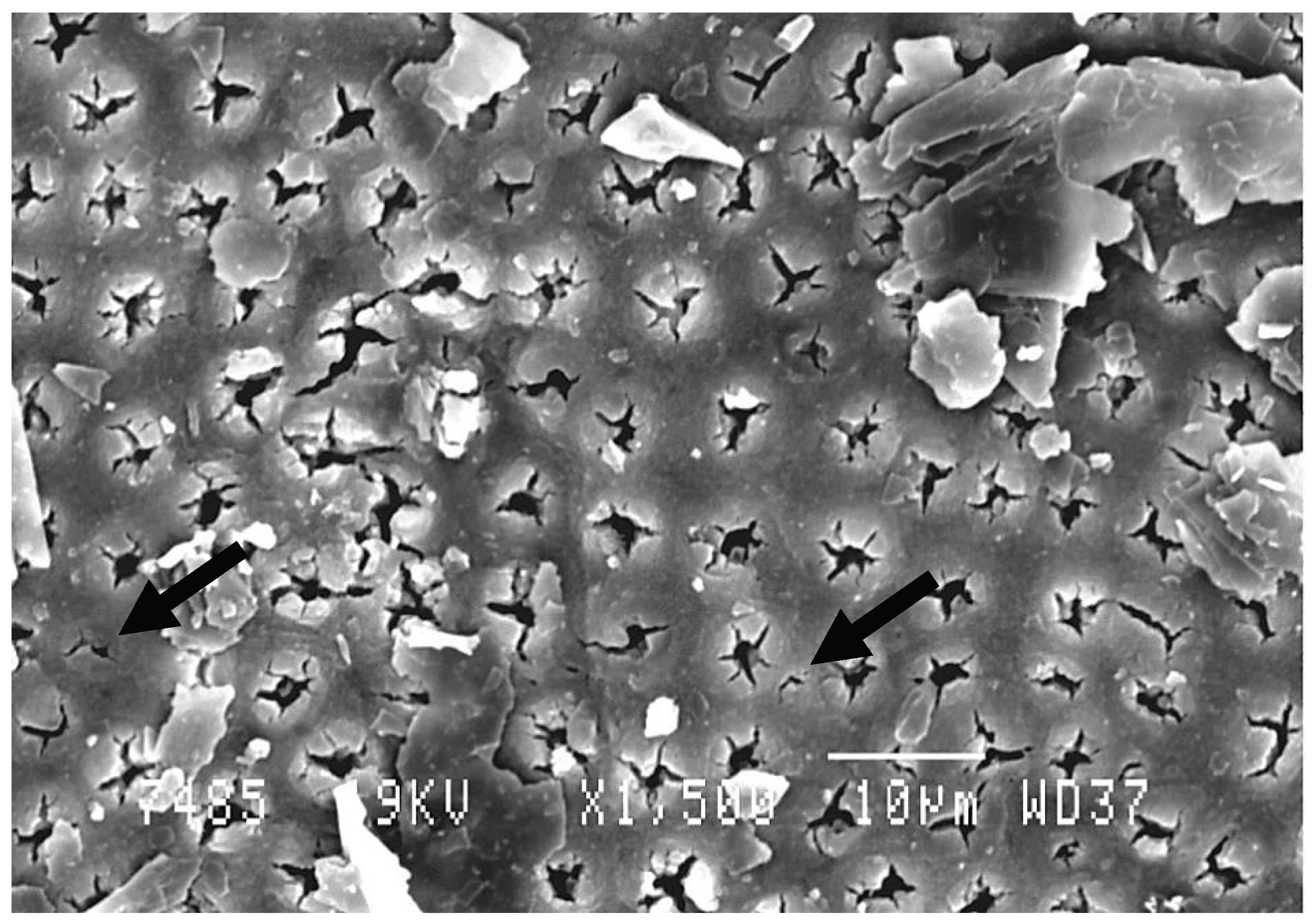
2.3. Scanning Electron Microscopy (SEM) Analysis
3. Results
3.1. Pulp Temperature Increase Measurements
3.2. Scanning Electron Microscopy (SEM) Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Patil, A.R.; Varma, S.; Suragimath, G.; Abbayya, K.; Zope, S.A.; Kale, V. Comparative Evaluation of Efficacy of Iontophoresis with 0.33% Sodium Fluoride Gel and Diode Laser Alone on Occlusion of Dentinal Tubules. J. Clin. Diagn. Res. 2017, 11, ZC123–ZC126. [Google Scholar] [CrossRef] [PubMed]
- Dowell, P.; Addy, M. Dentine Hypersensitivity—A Review. Aetiology, Symptoms and Theories of Pain Production. J. Clin. Periodontol. 1983, 10, 341–350. [Google Scholar] [CrossRef] [PubMed]
- Canadian Advisory Board on Dentin Hypersensitivity. Consensus-based recommendations for the diagnosis and management of dentin hypersensitivity. J. Can. Dent. Assoc. 2003, 69, 221–226. [Google Scholar]
- Porto, I.C.C.M.; Andrade, A.K.M.; Montes, M.A.J.R. Diagnosis and treatment of dentinal hypersensitivity. J. Oral Sci. 2009, 51, 323–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sgolastra, F.; Petrucci, A.; Gatto, R.; Monaco, A. Effectiveness of laser in dentinal hypersensitivity treatment: A systematic review. J. Endod. 2011, 37, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Bamise, C.T.; Esan, T.A. Mechanisms and treatment approaches of dentine hypersensitivity: A literature review. Oral Health Prev. Dent. 2011, 9, 353–367. [Google Scholar] [CrossRef] [PubMed]
- Davari, A.R.; Ataei, E.; Assarzadeh, H. Dentin Hypersensitivity: Etiology, Diagnosis and Treatment; A Literature Review. J. Dent. Shiraz Univ. Med. Sci. 2013, 14, 136–145. [Google Scholar]
- Namour, A.; Nammour, S.; Peremans, A.; Heysselaer, D.; De Moor, R.J.G. Treatment of Dentinal Hypersensitivity by means of Nd:YAP Laser: A Preliminary In Vitro Study. Sci. World J. 2014. [Google Scholar] [CrossRef]
- Nakamura, Y. Histopathological changes in dental pulp in rats after irradiation of Nd: YAG laser. Kokubyo Gakkai Zasshi 1987, 54, 705–721. (In Japanese) [Google Scholar] [CrossRef]
- Ishikawa, H. Histophathological study of rat dental pulp tissue after pulsed Nd: YAG laser irradiation. Jpn. J. Conserv. Dent. 2004, 47, 365–377. (In Japanese) [Google Scholar]
- Matsumoto, K.; Wakabayashi, H.; Funato, A.; Shirasuga, T. Histopathological findings of dental pulp irradiated by GaAlAs laser diode. Jpn. J. Conserv. Dent. 1985, 8, 1361–1365. (In Japanese) [Google Scholar]
- Melcer, J.; Chaumette, M.T.; Melcer, F.; Zeboulon, S.; Hasson, R.; Merard, R.; Pinaudeau, Y.; Dejardin, J.; Weill, R. Preliminary report on the effect of the CO2 laser beam on the dental pulp of the Macaca mulatta primate and the beagle dog. J. Endod. 1985, 11, 1–5. [Google Scholar] [CrossRef]
- Tate, Y.; Yoshiba, K.; Yoshiba, N.; Iwaku, M.; Okiji, T.; Ohshima, H. Odontoblast responses to GaAlAs laser irradiation in rat molars: An experimental study using heat-shock protein-25 immunohistochemistry. Eur. J. Oral Sci. 2006, 114, 50–57. [Google Scholar] [CrossRef]
- Umana, M.; Heysselaer, D.; Tielemans, M.; Compere, P.; Zeinoun, T.; Nammour, S. Dentinal Tubules Sealing by Means of Diode Lasers (810 and 980 nm): A Preliminary In Vitro Study. Photomed. Laser Surg. 2013, 31, 307–314. [Google Scholar] [CrossRef]
- Grossman, L.L. A systematic method for the treatment of hypersensitive dentin. J. Am. Dent. Assoc. 1935, 22, 592–602. [Google Scholar] [CrossRef]
- Lan, W.H.; Liu, H.C. A study of treatment on cervical dentin hypersensitivity with semiconductor laser. Chin. Dent. J. 1996, 15, 36–43. [Google Scholar]
- Bornstein, E. Near-infrared dental diode lasers. Scientific and photobiologic principles and applications. Dent. Today 2004, 23, 102–108. [Google Scholar]
- Brugnera, A., Jr.; Zanin, F.; Barbin, E.L.; Spano, J.C.; Santana, R.; Pécora, J.D. Effects of Er: YAG and Nd: YAG laser irradiation on radicular dentin permeability using different irrigating. Lasers Surg. Med. 2003, 33, 256–259. [Google Scholar] [CrossRef]
- Santos, C.; Sousa–Neto, M.D.; Alfredo, E.; Guerisoli, D.M.Z.; Pécora, J.D.; Lia, R.C. Morphologic evaluation of the radicular dentin irradiated with Nd: YAG laser under different parameters and angles of incidence. Photomed. Laser Surg. 2005, 23, 590–595. [Google Scholar] [CrossRef]
- Parker, S. Verifiable CPD paper: Laser-tissue interaction. Br. Dent. J. 2007, 202, 73–81. [Google Scholar] [CrossRef] [Green Version]
- Thomas, T.; Gopikrishna, V.; Kandaswamy, D. Comparative evaluation of maintenance of cell viability of an experimental transport media “coconut water” with Hank’s balanced salt solution and milk, for transportation of an avulsed tooth: An in vitro cell culture study. J. Conserv. Dent. 2008, 11, 22–29. [Google Scholar] [CrossRef]
- Tewari, S.; Goel, A. Effect of placement agitation and drying time on dentin shear bond strength: An in vivo study. Oper. Dent. 2009, 34, 524–530. [Google Scholar] [CrossRef]
- El Yazami, H.; Zeinoun, T.; Bou Saba, S.; Lamard, L.; Peremans, A.; Limme, M.; Geerts, S.; Lamy, M.; Nammour, S. Pulp temperature increase during photo-activated disinfection (PAD) of periodontal pockets: An in vitro study. Lasers Med. Sci. 2010, 25, 655–659. [Google Scholar] [CrossRef]
- Nammour, S.; Kowalyk, K.; Valici, C.; Zeinoun, T.; Rocca, J.P.; Powell, L.; Van Reck, J. Safety parameters for pulp temperature during selective ablation of caries by KTP laser in vitro. J. Clin. Laser Med. Surg. 2004, 22, 99–104. [Google Scholar] [CrossRef]
- Henriques, F.C.; Moritz, A.R. Studies of thermal injuries. 1. The conduction of heat to and through skin and temperature therein. A theoretical and an experimental investigation. Am. J. Pathol. 1947, 23, 531–549. [Google Scholar]
- Nammour, S.; Zeinoun, T.; Bogaerts, I.; Lamy, M.; Geerts, S.O.; Bou Saba, S.; Lamard, L.; Peremans, A.; Limme, M. Evaluation of dental pulp temperature rise during photo-activated decontamination (PAD) of caries: An in vitro study. Lasers Med. Sci. 2010, 25, 651–654. [Google Scholar] [CrossRef]
- Dickers, B.; Lamard, L.; Peremans, A.; Geerts, S.; Lamy, M.; Limme, M.; Rompen, E.; De Moor, R.J.; Mahler, P.; Rocca, J.P.; et al. Temperature rise during photo-activated disinfection of root canals. Lasers Med. Sci. 2009, 24, 81–85. [Google Scholar] [CrossRef]
- Nammour, S.; Rocca, J.P.; Keiani, K.; Balestra, C.; Snoeck, T.; Powell, L.; Reck, J.V. Pulpal and periodontal temperature rise during KTP laser use as a root planning complement in vitro. Photomed. Laser Surg. 2005, 23, 10–14. [Google Scholar] [CrossRef]
- Nammour, S.; Kowaly, K.; Powell, G.L.; Van Reck, J.; Rocca, J.P. External temperature during KTP-Nd:YAG laser irradiation in root canals: An in vitro study. Lasers Med. Sci. 2004, 19, 27–32. [Google Scholar] [CrossRef]
- Orchardson, R.; Gillam, D.G. Managing dentin hypersensitivity. J. Am. Dent. Assoc. 2006, 137, 990–998. [Google Scholar] [CrossRef]
- Chu, C.H.; Lo, E.C.M. Dentin hypersensitivity: A review. Hong Kong Dent. J. 2010, 7, 15–22. [Google Scholar]
- Oncu, E.; Karabekiroglu, S.; Unlu, N. Effects of different desensitizers and lasers on dentine tubules: An in-vitro analysis. Microsc. Res. Tech. 2017, 80, 737–744. [Google Scholar] [CrossRef]
- Brännström, M. A Hydrodynamic Mechanism in the Transmission of Pain Producing Stimuli through the Dentine. Sensory Mechanisms in Dentine; Pergamon Press: Oxford, UK, 1963; pp. 73–79. [Google Scholar]
- Gutknecht, N. Proceedings of the 1st International Workshop of Evidence Based Dentistry on Lasers in Dentistry; Quintessence: New Maiden, UK, 2007; ISBN 978-1-85097-167-2. [Google Scholar]
- Zach, L.; Cohen, G. Pulp response to externally applied heat. Oral Surg. Oral Med. Oral Pathol. 1965, 19, 515–530. [Google Scholar] [CrossRef]
- Hulsmann, M.; Heckendorff, M.; Lennon, A. Chelating agents in root canal treatment: Mode of action and indications for their use. Int. Endod. J. 2003, 36, 810–830. [Google Scholar] [CrossRef]
- Pandey, R.; Koppolu, P.; Kalakonda, B.; Lakshmi, B.V.; Mishra, A.; Reddy, P.K.; Bollepalli, A.C. Treatment of dentinal hypersensitivity using low-level laser therapy and 5% potassium nitrate: A randomized, controlled, three arm parallel clinical study. Int. J. Appl. Basic Med. Res. 2017, 7, 63–66. [Google Scholar] [CrossRef]
- Sgolastra, F.; Petrucci, A.; Severino, M.; Gatto, R.; Monaco, A. Lasers for the Treatment of Dentin Hypersensitivity: A Meta-analysis. J. Dent. Res. 2013, 92, 492–499. [Google Scholar] [CrossRef]
- Liu, Y.; Gao, J.; Gao, Y.; Xu, S.; Zhan, X.; Wu, B. In Vitro Study of Dentin Hypersensitivity Treated by 980-nm Diode Laser. J. Lasers Med. Sci. 2013, 4, 111–119. [Google Scholar]
- Lund, R.G.; Silva, A.F.; Piva, E.; DaRosa, W.L.; Heckmann, S.S.; Demarco, F.F. Clinical evaluation of two desensitizing treatments. Lasers Med. Sci. 2013, 4, 111–119. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| P Initial | P (Just after Treatment) | P 3 Months | P 6 Months | |
|---|---|---|---|---|
| Number of values | 184 | 184 | 184 | 184 |
| Mean | 6.505 | 0.8909 | 1.318 | 1.409 |
| Std. Deviation | 1.608 | 1.045 | 2.124 | 2.153 |
| Std. Error | 0.3429 | 0.2227 | 0.4529 | 0.4590 |
| Repeated Measures ANOVA | ||||
|---|---|---|---|---|
| P value | <0.0001 | |||
| P value summary | - | |||
| Are means signif. Different? (P < 0.05) | Yes | |||
| Number of groups | 4 | |||
| F | 139.4 | |||
| R Squared | 0.8691 | |||
| Newman–Keuls Multiple Comparison test | Mean Diff. | Q | Significant? | Summary |
| P After vs. P Initial | −5.614 | 24.68 | Yes | - |
| P After vs. P 3 months | −0.4273 | 1.878 | No | ns |
| P After vs. P 6 months | −0.3364 | - | No | ns |
| P 6 months vs. P Initial | −5.277 | 23.20 | Yes | - |
| P 6 months vs. P 3 months | −0.09091 | - | No | ns |
| P 3 months vs. P Initial | −5.186 | 22.80 | Yes | - |
| Pulp Temperature at 1 Watt + Graphite | |
|---|---|
| Number of values | 36 |
| Minimum | 0.8000 °C |
| Maximum | 1.500 °C |
| Mean | 1.200 °C |
| Std. Deviation | 0.1954 |
| Std. Error | 0.05641 |
| Lower 95% CI of mean | 1.076 |
| Upper 95% CI of mean | 1.324 |
| Kolmogorov Smirnov normality test | |
| KS distance | 0.1667 |
| P value | >0.10 |
| Passed normality test (α = 0.05)? | Yes |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
El Mobadder, M.; Namour, A.; Namour, M.; Dib, W.; El Mobadder, W.; Maalouf, E.; Geerts, S.; Zeinoun, T.; Nammour, S. Dentinal Hypersensitivity Treatment Using Diode Laser 980 nm: In Vivo Study. Dent. J. 2019, 7, 5. https://doi.org/10.3390/dj7010005
El Mobadder M, Namour A, Namour M, Dib W, El Mobadder W, Maalouf E, Geerts S, Zeinoun T, Nammour S. Dentinal Hypersensitivity Treatment Using Diode Laser 980 nm: In Vivo Study. Dentistry Journal. 2019; 7(1):5. https://doi.org/10.3390/dj7010005
Chicago/Turabian StyleEl Mobadder, Marwan, Amaury Namour, Mélanie Namour, Walid Dib, Wassim El Mobadder, Elie Maalouf, Sabine Geerts, Toni Zeinoun, and Samir Nammour. 2019. "Dentinal Hypersensitivity Treatment Using Diode Laser 980 nm: In Vivo Study" Dentistry Journal 7, no. 1: 5. https://doi.org/10.3390/dj7010005
APA StyleEl Mobadder, M., Namour, A., Namour, M., Dib, W., El Mobadder, W., Maalouf, E., Geerts, S., Zeinoun, T., & Nammour, S. (2019). Dentinal Hypersensitivity Treatment Using Diode Laser 980 nm: In Vivo Study. Dentistry Journal, 7(1), 5. https://doi.org/10.3390/dj7010005