Comparison of Two-Dimensional and Three-Dimensional Radiographs Using Clinically Relevant Parameters


 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Characteristics
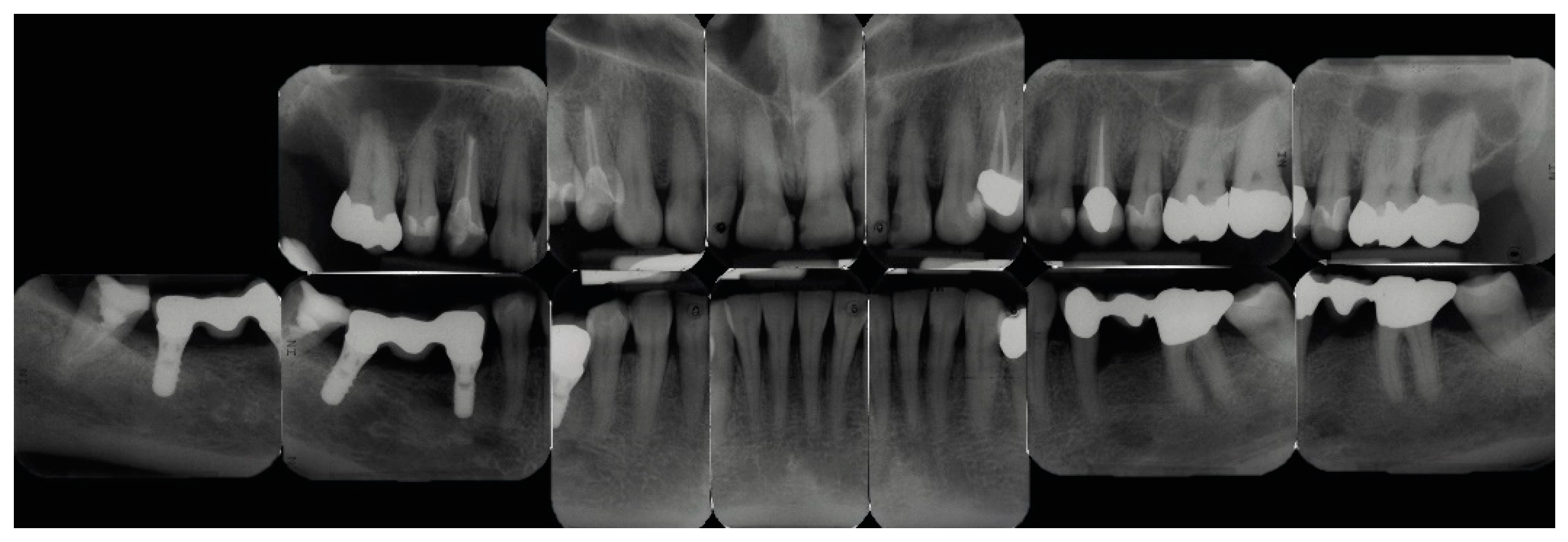
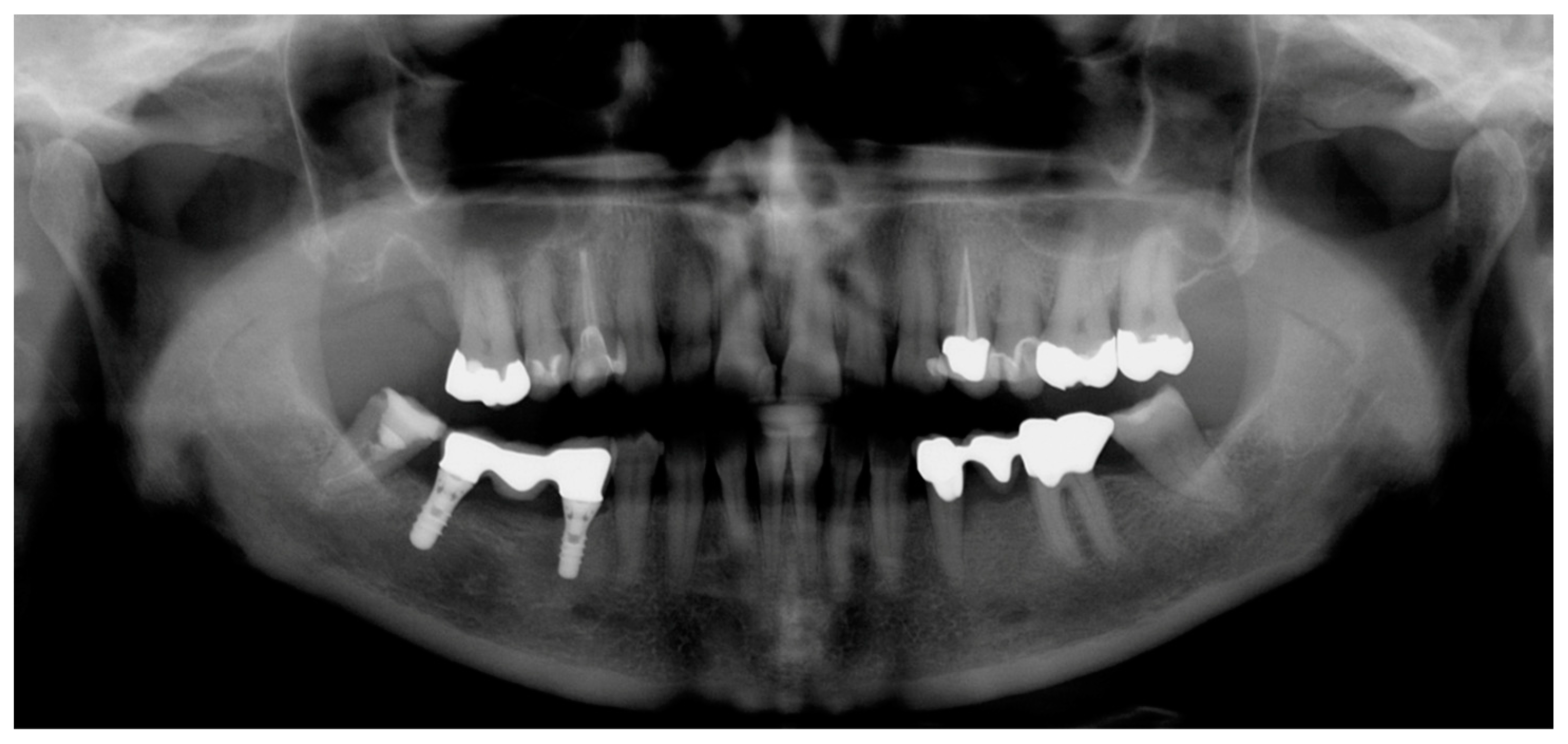
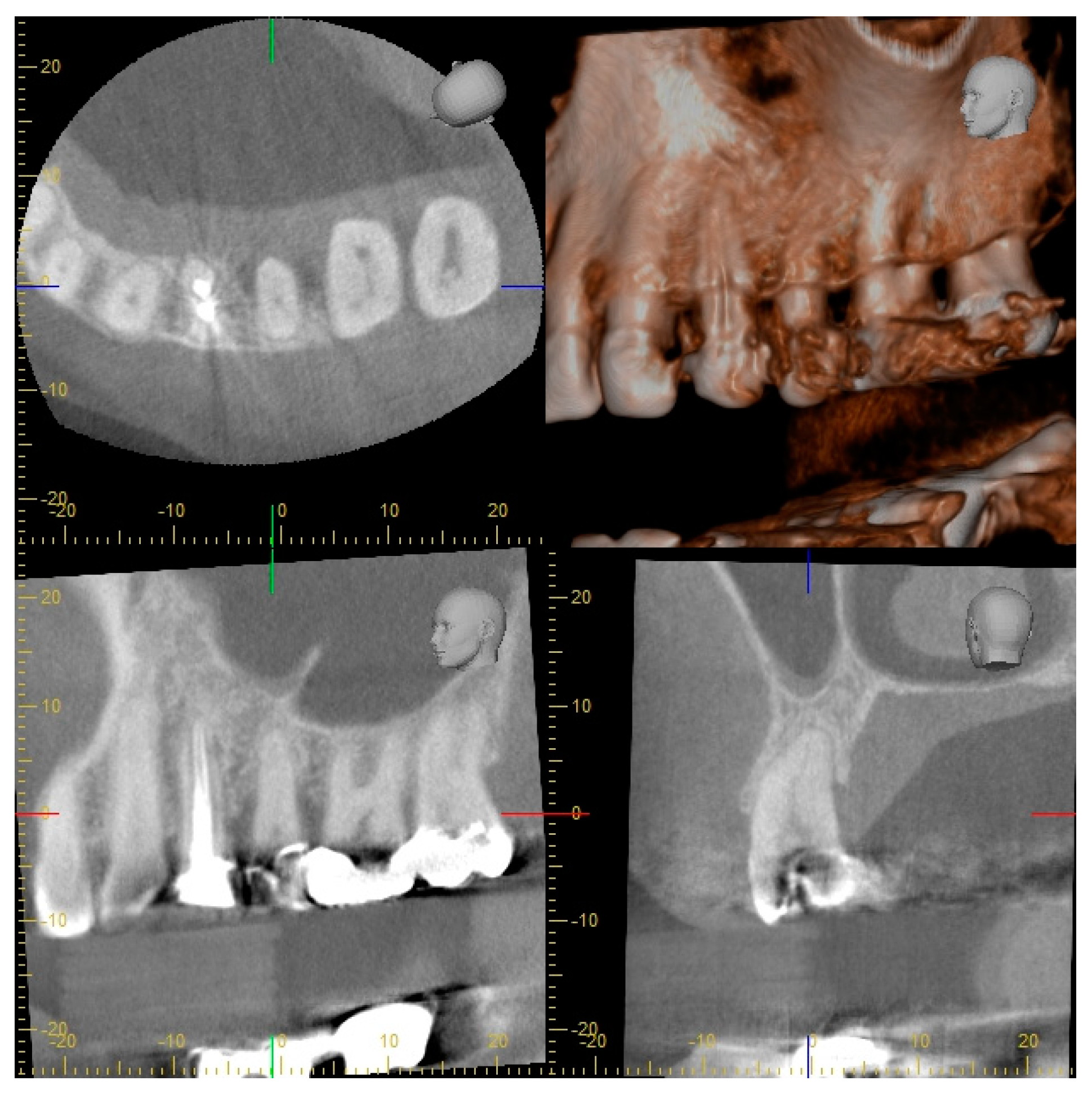
2.2. Radiographic Methods
2.3. Analysis of Radiographic Images
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Walter, C.; Buset, S.L.; Thillainathan, L.; Weiger, R.; Zitzmann, N.U. Evaluation of periodontal therapy in undergraduate courses of the University of Basle. Swiss Dent. J. 2013, 123, 861–869. [Google Scholar]
- Persson, R.E.; Tzannetou, S.; Feloutzis, A.G.; Brägger, U.; Persson, G.R.; Lang, N.P. Comparison between panoramic and intra-oral radiographs for the assessment of alveolar bone levels in a periodontal maintenance population. J. Clin. Periodontol. 2003, 30, 833–839. [Google Scholar] [CrossRef] [PubMed]
- Dula, K.; Bornstein, M.M.; Buser, D.; Dagassan-Berndt, D.; Ettlin, D.A.; Filippi, A.; Gabioud, F.; Katsaros, C.; Krastl, G.; Lambrecht, J.T.; et al. SADMFR Guidelines for the use of cone beam computed tomography/digital volume tomography. Swiss Dent. J. 2014, 124, 1170–1183. [Google Scholar]
- Dula, K.; Benic, G.I.; Bornstein, M.; Dagassan-Berndt, D.; Filippi, A.; Hicklin, S.; Kissling-Jeger, F.; Luebbers, H.T.; Sculean, A.; Sequeira-Byron, P.; et al. SADMFR guidelines for the use of cone-beam computed tomography/digital volume tomography—Endodontics, periodontology, reconstructive dentistry, pediatric dentistry. Swiss Dent. J. 2015, 125, 945–953. [Google Scholar] [PubMed]
- Bornstein, M.M.; Lauber, R.; Sendi, P.; von Arx, T. Comparison of periapical radiography and limited cone-beam computed tomography in mandibular molars for analysis of anatomical landmarks before apical surgery. J. Endod. 2011, 37, 151–157. [Google Scholar] [CrossRef]
- Walter, C.; Schmidt, J.C.; Dula, K.; Sculean, A. Cone beam computed tomography (CBCT) for diagnosis and treatment planning in periodontology: A systematic review. Quintessence Int. 2016, 47, 25–37. [Google Scholar]
- Armitage, G.C. Development of a classification system for periodontal diseases and conditions. Ann. Periodontol. 1999, 4, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Walter, C.; Saxer, U.P.; Bornstein, M.M.; Klingler, K.; Ramseier, C.A. Impact of tobacco use on the periodontium—An update (I)—Part 1: Epidemiologic and pathogenetic aspects of tobacco-related periodontal disease. Swiss Dent. J. 2007, 117, 45–60. [Google Scholar]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Clin. Periodontol. 2018, 45, S149–S161. [Google Scholar] [CrossRef]
- Rodriguez, F.R.; Taner, B.; Weiger, R.; Walter, C. Is smoking a predictor of apical periodontitis? Clin. Oral Investig. 2013, 17, 1947–1955. [Google Scholar] [CrossRef] [PubMed]
- Walter, C.; Kaner, D.; Berndt, D.C.; Weiger, R.; Zitzmann, N.U. Three-dimensional imaging as a pre-operative tool in decision making for furcation surgery. J. Clin. Periodontol. 2009, 36, 250–257. [Google Scholar] [CrossRef]
- Lindhe, J.; Karring, T.; Araujo, M. The anatomy of periodontal tissues. In Clinical Periodontology and Implant Dentistry, 4th ed.; Lindhe, J., Karring, T., Lang, N.P., Eds.; Blackwell Munksgaard: Copenhagen, Denmark, 2003; pp. 3–48. [Google Scholar]
- Goldman, H.M.; Cohen, D.W. The intrabony pocket: Classification and treatment. J. Periodontol. 1957, 29, 272–279. [Google Scholar] [CrossRef]
- Papapanou, P.N.; Tonetti, M.S. Diagnosis and epidemiology of periodontal osseous lesions. Periodontol. 2000 2000, 22, 8–21. [Google Scholar] [CrossRef] [PubMed]
- Hamp, S.E.; Nyman, S.; Lindhe, J. Periodontal treatment of multirooted teeth. Results after 5 years. J. Clin. Periodontol. 1975, 2, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Vermylen, K.; De Quincey, G.N.; Van’t Hof, M.A.; Wolffe, G.N.; Renggli, H.H. Classification, reproducibility and prevalence of root proximity in periodontal patients. J. Clin. Periodontol. 2005, 32, 254–259. [Google Scholar] [CrossRef]
- Vertucci, F.J. Root canal anatomy of the human permanent teeth. Oral Surg. Oral Med. Oral Pathol. 1984, 58, 589–599. [Google Scholar] [CrossRef]
- Jou, Y.; Karabucak, B.; Levin, J.; Liu, D. Endodontic working width: Current concepts and techniques. Dent. Clin. N. Am. 2004, 48, 323–335. [Google Scholar] [CrossRef]
- Ørstavik, D.; Kerekes, K.; Eriksen, H.M. The periapical index: A scoring system for radiographic assessment of apical periodontitis. Dent. Traumatol. 1986, 2, 20–34. [Google Scholar] [CrossRef]
- Weiger, R.; Hitzler, S.; Hermle, G.; Löst, C. Periapical status, quality of root canal fillings and estimated endodontic treatment needs in an urban German population. Endod. Dent. Traumatol. 1997, 13, 69–74. [Google Scholar] [CrossRef]
- Pitts, N.B. Systems for grading approximal carious lesions diagnosed from bitewing radiographs. Proposals for future standardization. Community Dent. Oral Epidemiol. 1984, 12, 114–122. [Google Scholar] [CrossRef]
- Tronstad, L.; Asbjornsen, K.; Doving, L.; Pedersen, I.; Eriksen, H.M. Influence of coronal restorations on the periapical health of endodontically treated teeth. Endod. Dent. Traumatol. 2000, 16, 218–221. [Google Scholar] [CrossRef] [PubMed]
- Zadik, Y.; Yitschaky, O.; Pikovsky, A.; Zini, A.; Fridlander Barenboim, S. Detection of mandibular condyle pseudocysts in panoramic radiographs: Digital and film-based radiology. Quintessence Int. 2015, 46, 725–730. [Google Scholar]
- ICRP: Recommendation of the International Comission on Radiological Protection ICRP Publication 26; Pergamon Press: Oxford, UK, 1977.
- Sedentexct. Guidelines on CBCT for Dental and Maxillofacial Radiology. Available online: http://www.sedentexct.eu/content/guidelines-cbct-dental-and-maxillofacial-radiology.htm (accessed on 12 April 2019).
- Haiter-Neto, F.; Wenzel, A.; Gotfredsen, E. Diagnostic accuracy of cone beam computed tomography scans compared with intraoral image modalities for detection of caries lesions. Dentomaxillofac. Radiol. 2008, 37, 18–22. [Google Scholar] [CrossRef]
- Kamburoglu, K.; Murat, S.; Yuksel, S.P.; Cebeci, A.R.; Paksoy, C.S. Occlusal caries detection by using a cone-beam CT with different voxel resolutions and a digital intraoral sensor. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 109, e63–e69. [Google Scholar] [CrossRef]
- Cheng, J.G.; Zhang, Z.L.; Wang, X.Y.; Zhang, Z.Y.; Ma, X.C. Detection accuracy of proximal caries by phosphorplate and cone-beam computerized tomography images scanned with different resolutions. Clin. Oral Investig. 2012, 16, 1015–1021. [Google Scholar] [CrossRef] [PubMed]
- Krzyzostaniak, J.; Kulczyk, T.; Czarnecka, B.; Surdacka, A. A comparative study of the diagnostic accuracy of cone beam computed tomography and intraoral radiographic modalities for the detection of nonconcavitated caries. Clin. Oral Investig. 2015, 19, 667–672. [Google Scholar] [CrossRef] [PubMed]
- Tsuchida, R.; Araki, K.; Okano, T. Evaluation of a limited cone-beam volumetric imaging system: Comparison with film radiography in detecting incipient proximal caries. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 104, 412–416. [Google Scholar] [CrossRef]
- Kayipmaz, S.; Sezgin, O.S.; Saricaoglu, S.T.; Can, G. An in vitro comparison of diagnostic abilities of conventional radiography, storage phosphor, and cone beam computed tomography to determine occlusal and approximal caries. Eur. J. Radiol. 2011, 80, 478–482. [Google Scholar] [CrossRef]
- Rathore, S.; Tyndall, D.; Wright, J.; Everett, E. Ex vivo comparison of Galileos cone beam CT and intraoral radiographs in detecting occlusal caries. Dentomaxillofac. Radiol. 2012, 41, 489–493. [Google Scholar] [CrossRef] [Green Version]
- Valizadeh, S.; Tavakkoli, M.A.; Karimi Vasigh, H.; Azizi, Z.; Zarrabian, T. Evaluation of cone beam computed tomography (CBCT) system: Comparison with intraoral periapical radiography in proximal caries detection. J. Dent. Res. Dent. Clin. Dent. Prosp. 2012, 6, 1–5. [Google Scholar]
- Gaalaas, L.; Tyndall, D.; Mol, A.; Everett, E.; Bangdiwala, A. Ex vivo evaluation of new 2D and 3D dental radiographic technology for detecting caries. Dentomaxillofac. Radiol. 2016, 45, 20150281. [Google Scholar] [CrossRef] [Green Version]
- Akkaya, N.; Kansu, O.; Kansu, H.; Cagirankaya, L.B.; Arslan, U. Comparing the accuracy of panoramic and intraoral radiography in the diagnosis of proximal caries. Dentomaxillofac. Radiol. 2006, 35, 170–174. [Google Scholar] [CrossRef]
- Akarslan, Z.Z.; Akdevelioglu, M.; Gungor, K.; Erten, H. A comparison of the diagnostic accuracy of bitewing, periapical, unfiltered and filtered digital panoramic images for approximal caries detection in posterior teeth. Dentomaxillofac. Radiol. 2008, 37, 458–463. [Google Scholar] [CrossRef]
- Kamburoglu, K.; Kolsuz, E.; Murat, S.; Yuksel, S.; Ozen, T. Proximal caries detection accuracy using intraoral bitewing radiography, extraoral bitewing radiography and panoramic radiography. Dentomaxillofac. Radiol. 2012, 41, 450–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matherne, R.P.; Angelopoulos, C.; Kulild, J.C.; Tira, D. Use of cone-beam computed tomography to identify root canal systems in vitro. J. Endod. 2008, 34, 87–89. [Google Scholar] [CrossRef] [PubMed]
- Blattner, T.C.; George, N.; Lee, C.C.; Kumar, V.; Yelton, C.D. Efficacy of cone-beam computed tomography as a modality to accurately identify the presence of second mesiobuccal canals in maxillary first and second molars: A pilot study. J. Endod. 2010, 36, 867–870. [Google Scholar] [CrossRef] [PubMed]
- Michetti, J.; Maret, D.; Mallet, J.P.; Diemer, F. Validation of cone beam computed tomography as a tool to explore root canal anatomy. J. Endod. 2010, 36, 1187–1190. [Google Scholar] [CrossRef]
- Zhang, R.; Wang, H.; Tian, Y.Y.; Yu, X.; Hu, T.; Dummer, P.M.H. Use of cone-beam computed tomography to evaluate root and canal morphology of mandibular molars in Chinese individuals. Int. Endod. J. 2011, 44, 990–999. [Google Scholar] [CrossRef]
- Brady, E.; Mannocci, F.; Brown, J.; Wilson, R.; Patel, S. A comparison of cone beam computed tomography and periapical radiography for the detection of vertical root fractures in nonendodontically treated teeth. Int. Endod. J. 2013, 46. [Google Scholar] [CrossRef]
- Lofthag-Hansen, S.; Huumonen, S.; Gröndahl, K.; Gröndahl, H.G. Limited conebeam CT and intraoral radiography for the diagnosis of periapical pathology. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 103, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Low, K.M.; Dula, K.; Bürgin, W.; von Arx, T. Comparison of periapical radiography and limited cone-beam tomography in posterior maxillary teeth referred for apical surgery. J. Endod. 2008, 34, 557–562. [Google Scholar] [CrossRef]
- Venskutonis, T.; Daugela, P.; Strazdas, M.; Juodzbalys, G. Accuracy of digital radiography and cone beam computed tomography on periapical radiolucency detection in endodontically treated teeth. J. Oral Maxillofac. Res. 2014, 5. [Google Scholar] [CrossRef] [PubMed]
- Kruse, C.; Spin-Neto, R.; Wenzel, A.; Kirkevang, L.L. Cone beam computed tomography and periapical lesions: A systematic review analysing studies on diagnostic efficacy by a hierarchical model. Int. Endod. J. 2015, 48, 815–828. [Google Scholar] [CrossRef] [PubMed]
- Weissman, J.; Johnson, J.D.; Anderson, M.; Hollender, L.; Huson, T.; Paranjpe, A.; Patel, S.; Cohenca, N. Association between the presence of apical periodontitis and clinical symptoms in endodontic patients using cone-beam computed tomography and periapicel radiographs. J. Endod. 2015, 41, 1824–1829. [Google Scholar] [CrossRef]
- Davies, A.; Patel, S.; Foschi, F.; Andiappan, M.; Mitchell, P.J.; Mannocci, F. The detection of periapical pathoses using digital periapical radiography and cone beam computed tomography in endodontically retreated teeth—part 2: A 1 year post-treatment follow-up. Int. Endod. J. 2016, 49, 623–635. [Google Scholar] [CrossRef] [PubMed]
- Aminoshariae, A.; Kulild, J.C.; Syed, A. Cone-beam computed tomography compared with intraoral radiographic lesions in endodontic outcome studies: A systematic review. J. Endod. 2018, 44, 1626–1631. [Google Scholar] [CrossRef]
- Bornstein, M.M.; Bingisser, A.C.; Reichart, P.A.; Sendi, P.; Bosshardt, D.D.; von Arx, T. Comparison between radiographic (2-dimensional and 3-dimensional) and histologic findings of periapical lesions treated with apical surgery. J. Endod. 2015, 41, 804–811. [Google Scholar] [CrossRef] [PubMed]
- De Faria Vasconcelos, K.; Evangelista, K.M.; Rodrigues, C.D.; Estrela, C.; de Sousa, T.O.; Silva, M.A. Detection of periodontal bone loss using cone beam CT and intraoral radiography. Dentomaxillofac. Radiol. 2012, 41, 64–69. [Google Scholar] [CrossRef] [Green Version]
- Grimard, B.A.; Hoidal, M.J.; Mills, M.P.; Mellonig, J.T.; Nummikoski, P.V.; Mealey, B.L. Comparison of clinical, periapical radiograph, and conebeam volume tomography measurement techniques for assessing bone level changes following regenerative periodontal therapy. J. Periodontol. 2009, 80, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Walter, C.; Schmidt, J.C.; Dula, K.; Sculean, A. Einsatz der digitalen volumentomographie zur diagnostik und behandlungsplanung in der parodontologie—Eine systematische übersicht. Quintessenz 2017, 68, 1151–1165. [Google Scholar]
- Hirschfeld, L.; Wasserman, B. A long-term survey of tooth loss in 600 treated periodontal patients. J. Periodontol. 1978, 49, 225–237. [Google Scholar] [CrossRef]
- Loos, B.; Nylund, K.; Claffey, N.; Egelberg, J. Clinical effects of root debridement in molar and non-molar teeth. A 2-year follow-up. J. Clin. Periodontol. 1989, 16, 498–504. [Google Scholar] [CrossRef]
- Nordland, P.; Garrett, S.; Kiger, R.; Vanooteghem, R.; Hutchens, L.H.; Egelberg, J. The effect of plaque control and root debridement in molar teeth. J. Clin. Periodontol. 1987, 14, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Walter, C.; Weiger, R.; Zitzmann, N.U. Periodontal surgery in furcation-involved maxillary molars revisited: An introduction of guidelines for comprehensive treatment. Clin. Oral Investig. 2011, 15, 9–20. [Google Scholar] [CrossRef]
- Walter, C.; Weiger, R.; Zitzmann, N.U. Accuracy of three-dimensional imaging in assessing maxillary molar furcation involvement. J. Clin. Periodontol. 2010, 37, 436–441. [Google Scholar] [CrossRef]
- Walter, C.; Weiger, R.; Dietrich, T.; Lang, N.P.; Zitzmann, N.U. Does three-dimensional imaging offer a financial benefit for treating maxillary molars with furcation involvement? A pilot clinical case series. Clin. Oral Implants. Res. 2012, 23, 351–358. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Scoring System/Classification | Criteria for Scoring/Classification of Parameters | ||
|---|---|---|---|---|
| Number of roots | 1 | 1 root | • complete root fusion = 1 root • incomplete root fusion = multirooted teeth (≥2 roots) | |
| 2 | 2 roots | |||
| 3 | 3 roots | |||
| Dehiscence | 0 | not present | • distance between alveolar crest and CEJ > 2 mm, resulting in exposed cervical root surface [12], buccally assessed | |
| 1 | present | |||
| Fenestration | 0 | not present | • lack of alveolar bone, not affecting the marginal alveolar bone and resulting in exposed root surface [12], buccally assessed | |
| 1 | present | |||
| Vertical bone defect | 0 | not present | • apical location of the base of the pocket with regard to the residual alveolar crest [13,14] • intrabony = infrabony component of the defect affecting one tooth/implant • crater = defect affecting two adjacent root/implant surfaces | |
| 1 | intrabony defect | |||
| 2 | crater | |||
| Number of bone walls | 1 | one-wall defect | • number of residual alveolar bone walls in intrabony defects [14] | |
| 2 | two-wall defect | |||
| 3 | three-wall defect | |||
| 4 | combination defect | |||
| Furcation involvement | 0 | not present | • horizontal loss of periodontal tissue support, that is, radiolucency in the furcation area [15] • classification according to Hamp et al. [15] | |
| 1 | present (I, II, III) | I | horizontal loss of periodontal tissue support ≤ 3 mm | |
| II | horizontal loss > 3 mm but not “through and through” destruction | |||
| III | horizontal “through and through” tissue destruction in the furcation | |||
| Root fusion | 0 | not present | • lack of a separating periodontal ligament between two adjacent roots [11] | |
| 1 | present | |||
| Root proximity | 0 | not present | • separating periodontal ligaments between two adjacent roots ≤ 0.8 mm [16] | |
| 1 | present | |||
| Root canal anatomy | I | 1 canal, 1 foramen | • classification according to Vertucci [17] • evaluation of each root separately | |
| II | 2 canals, fusion, 1 foramen | |||
| III | 1 canal, division, fusion, 1 foramen | |||
| IV | 2 canals, no fusion, 2 foramina | |||
| V | 1 canal, division, 2 foramina | |||
| VI | 2 canals, fusion, division, 2 foramina | |||
| VII | 1 canal, division, fusion, division, 2 foramina | |||
| VIII | 3 canals, no fusion, 3 foramina | |||
| Root canal cross-section | 1 | round | • classification according to Jou et al. [18] • evaluation of each root canal separately | |
| 2 | oval | |||
| 3 | long oval | |||
| 4 | flattened | |||
| 5 | irregular | |||
| Periapical status | 1 | healthy (PAI 1, 2) | • scoring system according to Ørstavik et al. [19] | |
| PAI 1 | normal periapical structure | |||
| PAI 2 | small changes in bone structure | |||
| PAI 3 | changes in bone structure with mineral loss | |||
| 2 | diseased (PAI 3, 4, 5) | PAI 4 | apical periodontitis with well-defined radiolucent areas | |
| PAI 5 | severe apical periodontitis with exacerbating features | |||
| • multirooted teeth were given the highest score detected at any root [10] | ||||
| Root canal filling | 0 | insufficient (score >1) | • scoring system according to Weiger et al. [20] • length: (1) 0-2 mm short of the radiographic apex, (2) >2 mm short of the radiographic apex, (3) extruded beyond the radiographic apex • density: (1) no voids and close adaptation to root canal walls, (2) voids or insufficient adaptation | |
| 1 | sufficient (score =1) | |||
| Caries | R0 | sound (no radiolucency) | • scoring system according to Pitts [21] • evaluation of each tooth surface separately • each tooth was given the highest score detected at any tooth surface | |
| R1 | outer half enamel lesion | |||
| R2 | inner half enamel lesion | |||
| R3 | outer half dentin lesion | |||
| R4 | inner half dentin lesion | |||
| Restoration quality | 0 | intact | • scoring system according to Tronstad et al. [22] • not intact = sign of overhangs, recurrent decay or open margins • intact = any restoration that appeared intact radiographically | |
| 1 | not intact | |||
| In addition to all scores: | N not assessable | • for example, due to artefacts, overlapping effects, resolution capacity and/or contrast limitations | ||
| Parameter | Number of Assessed Structures | Distribution of the Scores of Parameters (Number of Structures) * | ||
|---|---|---|---|---|
| CBCT | I-O | OPT | ||
| Number of roots | 23 teeth | 1 (19), 2 (1), 3 (3) | 1 (19), 2 (1), 3 (3) | 1 (19), 2 (1), 3 (1), N (2) |
| Dehiscence | 27 roots | 0 (16), 1 (11) | N (27) | N (27) |
| Fenestration | 27 roots | 0 (18), 1 (9) | N (27) | N (27) |
| Vertical bone defect | 23 teeth, 2 implants | 0 (22), 1 (3) | 0 (20), 1 (3), 2 (2) | 0 (23), 2 (2) |
| Number of bone walls | 2-5 vertical defects | 3 (1), 4 (2) | N (5) | N (2) |
| Furcation involvement | 11 furcation entrances | 0 (11) | 0 (4), N (7) | 0 (1), N (10) |
| Root fusion | 10 pairs of roots | 0 (10) | 0 (4), N (6) | 0 (2), N (8) |
| Root proximity | 10 pairs of roots | 0 (8), 1 (2) | 0 (2), 1 (2), N (6) | 0 (1), 1 (1), N (8) |
| Root canal anatomy | 30 roots | I (24), II (4), N (2) | I (18), II (2), N (10) | I (16), II (2), N (12) |
| Root canal cross-section | 34 root canals | 1 (30), N (4) | N (34) | N (34) |
| Periapical status | 30 roots, 2 implants | 1 (30), 2 (2) | 1 (31), 2 (1) | 1 (21), N (11) |
| Root canal filling | 2 root canal fillings | 1 (2) | 1 (2) | 0 (1), 1 (1) |
| Caries | 23 teeth | R0 (6), R3 (1), N (16) | R0 (23) | R0 (16), N (7) |
| Restoration quality | 16 restorations | 0 (2), N (14) | 0 (14), 1 (1), N (1) | 0 (4), 1 (1), N (11) |
| CBCT versus I-O | CBCT versus OPT | I-O versus OPT | CBCT vs. I-O vs. OPT | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CBCT = I-O | CBCT > I-O | CBCT < I-O | Overall | CBCT = OPT | CBCT > OPT | CBCT < OPT | Overall | I-O = OPT | I-O > OPT | I-O < OPT | Overall | Overall | |
| Number of roots 1 | 23 (13, 10) | 0 | 0 | CBCT = I-O (100) | 21 (11, 10) | 2 (2, 0) | 0 | CBCT > OPT (9) | 21 (11, 10) | 2 (2, 0) | 0 | I-O > OPT (9) | CBCT = I-O > OPT |
| Dehiscence | 0 | 27 (16, 11) | 0 | CBCT > I-O (100) | 0 | 27 (16, 11) | 0 | CBCT > OPT (100) | 27 (16, 11) | 0 | 0 | I-O = OPT (100) | CBCT > I-O = OPT |
| Fenestration | 0 | 27 (16, 11) | 0 | CBCT > I-O (100) | 0 | 27 (16, 11) | 0 | CBCT > OPT (100) | 27 (16, 11) | 0 | 0 | I-O = OPT (100) | CBCT > I-O = OPT |
| Vertical bone defect 2 | 22 (11, 11) | 3 (2, 1) | 0 | CBCT > I-O (12) | 21 (10, 11) | 4 (3, 1) | 0 | CBCT > OPT (16) | 22 (12, 10) | 3 (1, 2) | 0 | I-O > OPT (12) | CBCT > I-O > OPT |
| Number of bone walls | 0 | 3 (2, 1) | 0 | CBCT > I-O (100) | 0 | 1 (1, 0) | 0 | CBCT > OPT (100) | 2 (2, 0) | 0 | 0 | I-O = OPT (100) | CBCT > I-O = OPT |
| Furcation involvement 3 | 4 (3, 1) | 7 (6, 1) | 0 | CBCT > I-O (64) | 1 (0, 1) | 10 (9, 1) | 0 | CBCT > OPT (91) | 8 (6, 2) | 3 (3, 0) | 0 | I-O > OPT (27) | CBCT > I-O > OPT |
| Root fusion | 4 (3, 1) | 6 (6, 0) | 0 | CBCT > I-O (60) | 2 (1, 1) | 8 (8, 0) | 0 | CBCT > OPT (80) | 8 (7, 1) | 2 (2, 0) | 0 | I-O > OPT (20) | CBCT > I-O > OPT |
| Root proximity | 4 (3, 1) | 6 (6, 0) | 0 | CBCT > I-O (60) | 2 (1, 1) | 8 (8, 0) | 0 | CBCT > OPT (80) | 8 (7, 1) | 2 (2, 0) | 0 | I-O > OPT (20) | CBCT > I-O > OPT |
| Root canal anatomy | 21 (12, 9) | 9 (7, 2) | 0 | CBCT > I-O (30) | 19 (10, 9) | 11 (9, 2) | 0 | CBCT > OPT (37) | 28 (17, 11) | 2 (2, 0) | 0 | I-O > OPT (7) | CBCT > I-O > OPT |
| Root canal cross-section | 5 (4, 1) | 29 (18, 11) | 0 | CBCT > I-O (85) | 5 (4, 1) | 29 (18, 11) | 0 | CBCT > OPT (85) | 34 (22, 12) | 0 | 0 | I-O = OPT (100) | CBCT > I-O = OPT |
| Periapical status | 31 (18, 13) | 1 (1, 0) | 0 | CBCT > I-O (3) | 19 (6, 13) | 13 (13, 0) | 0 | CBCT > OPT (41) | 20 (7, 13) | 12 (12, 0) | 0 | I-O > OPT (38) | CBCT > I-O > OPT |
| Root canal filling | 2 (2, 0) | 0 | 0 | CBCT = I-O (100) | 1 (1, 0) | 1 (1, 0) | 0 | CBCT > OPT (50) | 1 (1, 0) | 1 (1, 0) | 0 | I-O > OPT (50) | CBCT = I-O > OPT |
| Caries | 6 (1, 5) | 1 (0, 1) | 16 (12, 4) | CBCT < I-O (70) | 11 (6, 5) | 2 (1, 1) | 10 (6, 4) | CBCT < OPT (43) | 16 (6, 10) | 7 (7, 0) | 0 | I-O > OPT (30) | I-O > OPT > CBCT |
| Restoration quality | 2 (1, 1) | 1 (1, 0) | 13 (9, 4) | CBCT < I-O (81) | 12 (9, 3) | 1 (1, 0) | 3 (1, 2) | CBCT < OPT (19) | 6 (3, 3) | 10 (8, 2) | 0 | I-O > OPT (63) | I-O > OPT > CBCT |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schmidt, J.C.; Gutekunst, C.-J.; Dagassan-Berndt, D.; Schmidlin, P.R.; Walter, C. Comparison of Two-Dimensional and Three-Dimensional Radiographs Using Clinically Relevant Parameters. Dent. J. 2019, 7, 50. https://doi.org/10.3390/dj7020050
Schmidt JC, Gutekunst C-J, Dagassan-Berndt D, Schmidlin PR, Walter C. Comparison of Two-Dimensional and Three-Dimensional Radiographs Using Clinically Relevant Parameters. Dentistry Journal. 2019; 7(2):50. https://doi.org/10.3390/dj7020050
Chicago/Turabian StyleSchmidt, Julia C., Claudia-Julie Gutekunst, Dorothea Dagassan-Berndt, Patrick R. Schmidlin, and Clemens Walter. 2019. "Comparison of Two-Dimensional and Three-Dimensional Radiographs Using Clinically Relevant Parameters" Dentistry Journal 7, no. 2: 50. https://doi.org/10.3390/dj7020050
APA StyleSchmidt, J. C., Gutekunst, C.-J., Dagassan-Berndt, D., Schmidlin, P. R., & Walter, C. (2019). Comparison of Two-Dimensional and Three-Dimensional Radiographs Using Clinically Relevant Parameters. Dentistry Journal, 7(2), 50. https://doi.org/10.3390/dj7020050