Spatial Cleaning Action of Ultrasonic Irrigation on Enterococcus faecalis Biofilm


Abstract
:1. Introduction
2. Materials and Methods
3. Results
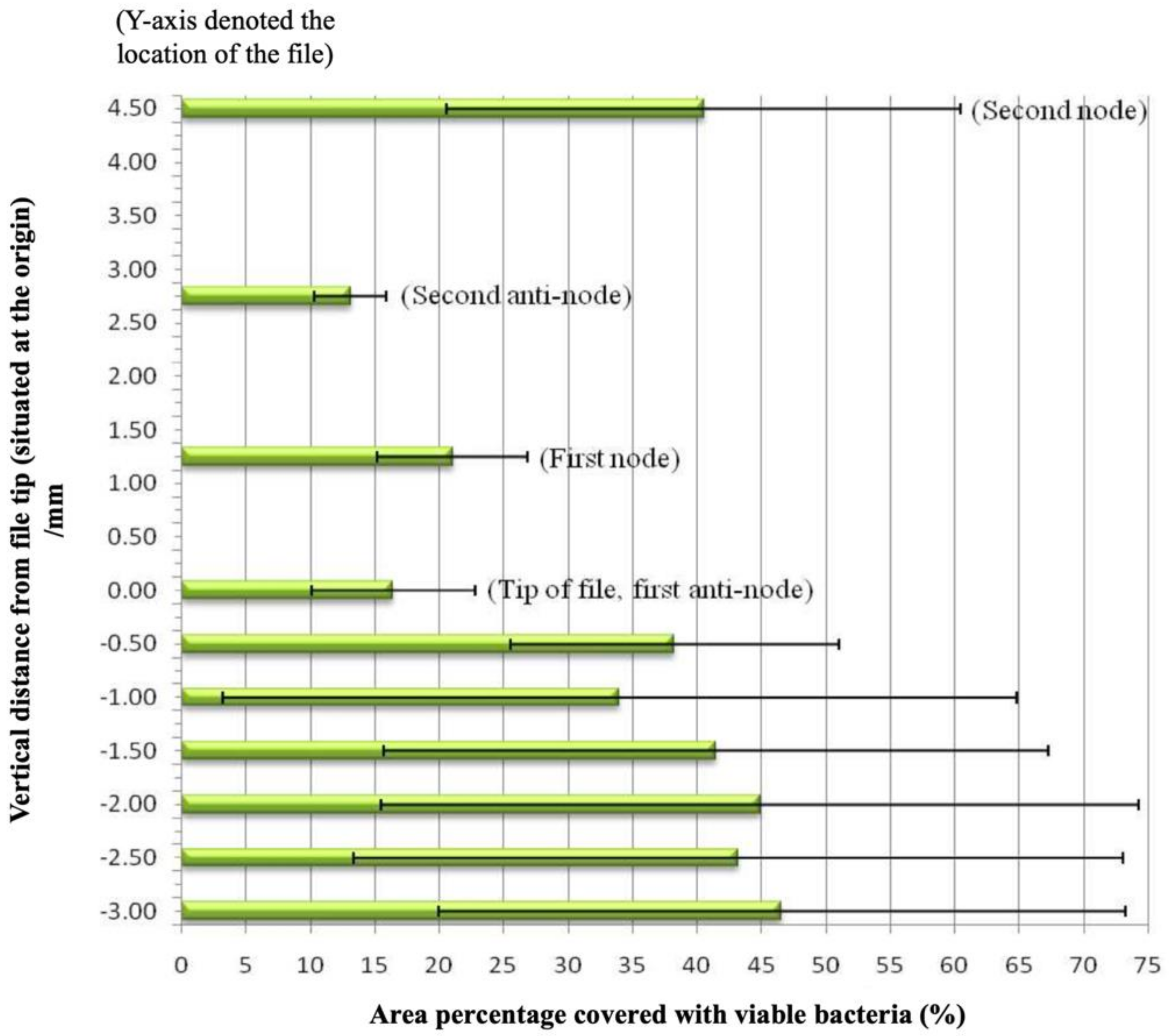
Quantification of Bacteria
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Sjögren, U.; Hagglund, B.; Sundqvist, G.; Wing, K. Factors affecting the long-term results of endodontic treatment. J. Endod. 1990, 16, 498–504. [Google Scholar] [CrossRef]
- Nair, P.N.; Sjögren, U.; Krey, G.; Kahnberg, K.E.; Sundqvist, G. Intraradicular bacteria and fungi in root-filled, asymptomatic human teeth with therapy-resistant periapical lesions: A long-term light and electron microscopic follow-up study. J. Endod. 1990, 16, 580–588. [Google Scholar] [CrossRef]
- Lint, L.; Skribnerm, J.; Gaengler, P. Factors associated with endodontic treatment. J. Endod. 1992, 18, 625–627. [Google Scholar] [CrossRef]
- Fabricius, L.; Dahlén, G.; Sundqvist, G.; Happonen, R.P.; Möller, A.J. Influence of residual bacteria on periapical tissue healing after chemomechanical treatment and root filling of experimentally infected monkey teeth. Europ. Oral. Sci. 2006, 114, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Nair, P. Light and electron microscopic studies of root canal flora and periapical lesions. J. Endod. 1987, 13, 29–39. [Google Scholar] [CrossRef]
- Nair, P.; Henry, S.; Cano, V.; Vera, J. Microbial status of apical root canal system of human mandibular first molars with primary apical periodontitis after “one-vist” endodontic treatment. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2005, 99, 231–252. [Google Scholar] [CrossRef] [PubMed]
- Park, H. A comparison of Greater Taper files, ProFiles, and stainless steel files to shape curved root canals. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2001, 91, 715–718. [Google Scholar] [CrossRef]
- Peters, O.A.; Barbakow, F.; Peters, C.I. An analysis of endodontic treatment with three nickel-titanium rotary root canal preparation techniques. Int. Endod. J. 2004, 37, 849–859. [Google Scholar] [CrossRef]
- Cheung, G.S.; Liu, C.S. A retrospective study of endodontic treatment outcome between nickel-titanium rotary and stainless steel hand filing techniques. J. Endod. 2009, 35, 938–943. [Google Scholar] [CrossRef]
- Hülsmann, M.; Schade, M.; Schäfers, F. A comparative study of root canal preparation with HERO 642 and Quantec SC rotary Ni-Ti instruments. Int. Endod. J. 2001, 34, 538–546. [Google Scholar] [CrossRef]
- Peters, O.A.; Schonenberger, K.; Laib, A. Effects of four Ni-Ti preparation techniques on root canal geometry assessed by micro computed tomography. Int. Endod. J. 2001, 34, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.K.; Wesselink, P.R. A primary observation on the preparation and obturation of oval canals. Int. Endod. J. 2001, 34, 137–141. [Google Scholar] [CrossRef] [Green Version]
- Barbizam, J.; Fariniuk, L.; Marchesan, M.; Pecora, J.; Sousa-Neto, M. Effectiveness of manual and rotary instrumentation techniques for cleaning flattened root canals. J. Endod. 2002, 28, 365–366. [Google Scholar] [PubMed]
- Bergmans, L.; Van Cleynenbreugel, J.; Beullens, M.; Wevers, M.; Van Meerbeek, B.; Lambrechts, P. Progressive versus constant tapered shaft design using NiTi rotary instruments. Int. Endod. J. 2003, 36, 288–295. [Google Scholar] [CrossRef] [PubMed]
- Rödig, T.; Hülsmann, M.; Mühge, M.; Schäfers, F. Quality of preparation of oval distal root canals in mandibular molars using nickel-titanium instruments. Int. Endod. J. 2002, 35, 919–928. [Google Scholar] [CrossRef]
- Ferreira, R.B.; Alfredo, E.; Porto de Arruda, M.; Silva Sousa, Y.T.; Sousa-Neto, M.D. Histological analysis of the cleaning capacity of nickel-titanium rotary instrumentation with ultrasonic irrigation in root canals. Austral. Endod. J. 2004, 30, 56–58. [Google Scholar] [CrossRef]
- Cheung, G.S.; Stock, C.J. In vitro cleaning ability of root canal irrigants with and without endosonics. Int. Endod. J. 1993, 26, 334–343. [Google Scholar] [CrossRef]
- Sabins, R.A.; Johnson, J.D.; Hellstein, J.W. A comparison of the cleaning efficacy of short-term sonic and ultrasonic passive irrigation after hand instrumentation in molar root canals. J. Endod. 2003, 29, 674–678. [Google Scholar] [CrossRef]
- Burleson, A.; Nusstein, J.; Reader, A.; Beck, M. The in vivo evaluation of hand/rotary/ultrasound instrumentation in necrotic, human mandibular molars. J. Endod. 2007, 33, 782–787. [Google Scholar] [CrossRef]
- Lee, S.J.; Wu, M.K.; Wesselink, P.R. The effectiveness of syringe irrigation and ultrasonics to remove debris from simulated irregularities within prepared root canal walls. Int. Endod. J. 2004, 37, 672–678. [Google Scholar] [CrossRef]
- Jiang, L.-M.; Verhaagen, B.; Versluis, M.; Langedijk, J.; Wesselink, P.; van der Sluis, L.W.M. The influence of the ultrasonic intensity on the cleaning efficacy of passive ultrasonic irrigation. J. Endod. 2011, 37, 688–692. [Google Scholar] [CrossRef] [PubMed]
- Bhuva, B.; Patel, S.; Wilson, R.; Niazi, S.; Beighton, D.; Mannocci, F. The effectiveness of passive ultrasonic irrigation on intraradicular Enterococcus faecalis biofilms in extracted single-rooted human teeth. Int. Endod. J. 2010, 43, 241–250. [Google Scholar] [CrossRef] [PubMed]
- Weller, R.N.; Brady, J.M.; Bernier, W.E. Efficacy of ultrasonic cleaning. J. Endod. 1980, 6, 740–743. [Google Scholar] [CrossRef]
- Van der Sluis, L.W.; Versluis, M.; Wu, M.K.; Wesselink, P.R. Passive ultrasonic irrigation of the root canal: A review of the literature. Int. Endod. J. 2007, 40, 415–426. [Google Scholar] [CrossRef]
- Walmsley, A.D.; Williams, A.R. Effects of constraint on the oscillatory pattern of endosonic files. J. Endod. 1989, 15, 189–194. [Google Scholar] [CrossRef]
- Lea, S.C.; Walmsley, A.D.; Lumley, P.J. Analysing endosonic root canal file oscillations: An in vitro evaluation. J. Endod. 2010, 36, 880–883. [Google Scholar] [CrossRef]
- Căpută, P.E.; Retsas, A.; Kuijk, L.; Chávez de Paz, L.E.; Boutsioukis, C. Ultrasonic irrigant activation during root canal treatment: A systematic review. J. Endod. 2019, 45, 31–44. [Google Scholar] [CrossRef]
- Ahmad, M.; Pitt Ford, T.R.; Crum, L.A. Ultrasonic debridement of root canals: An insight into the mechanisms involved. J. Endod. 1987, 13, 93–101. [Google Scholar] [CrossRef]
- Felver, B.; King, D.C.; Lea, S.C.; Price, G.J.; Walmsley, A.D. Cavitation occurrence around ultrasonic dental scalers. Ultrasonics Sonochem. 2009, 16, 692–697. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, M.; Pitt Ford, T.R.; Crum, L.A.; Walton, A.J. Ultrasonic debridement of root canals: Acoustic cavitation and its relevance. J. Endod. 1988, 14, 486–493. [Google Scholar] [CrossRef]
- Ahmad, M.; Roy, R.A.; Kamarudin, A.G.; Safar, M. The vibratory pattern of ultrasonic files driven piezoelectrically. Int. Endod. J. 1993, 26, 120–124. [Google Scholar] [CrossRef] [PubMed]
- Krell, K.V.; Johnson, R.J. Irrigation patterns of ultrasonic endodontic files. Part II. Diamond-coated files. J. Endod. 1988, 14, 535–537. [Google Scholar] [CrossRef]
- Wu, M.K.; R’Oris, A.; Barkis, D.; Wesselink, P.R. Prevalence and extent of long oval canals in the apical third. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2000, 89, 739–743. [Google Scholar] [CrossRef] [Green Version]
- Pinheiro, E.T.; Gomes, B.P.F.A.; Ferraz, C.C.R.; Sousa, E.L.R.; Teixeira, F.B.; Souza-Filho, F.J. Microorganisms from canals of root-filled teeth with periapical lesions. Int. Endod. J. 2003, 47, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rôças, I.N.; Siqueira, J.F.; Santos, K.R.N. Association of Enterococcus faecalis with different forms of periradicular diseases. J. Endod. 2004, 30, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Sedgley, C.; Nagel, A.; Dahlen, G.; Reit, C.; Molander, A. Real-time quantitative polymerase chain reaction and culture analyses of Enterococcus faecalis in root canals. J. Endod. 2006, 32, 173–177. [Google Scholar] [CrossRef]
- Ahmed, F.I.K.; Russel, C. Synergism between ultrasonic waves and hydrogen peroxide in the killing of micro-organisms. J. Appl. Bacteriol. 1975, 39, 31–40. [Google Scholar] [CrossRef]
- Bryce, G.; O’Donnell, D.; Ready, D.; Ng, Y.L.; Pratten, J.; Gulabivala, K. Contemporary root canal irrigants are able to disrupt and eradicate single- and dual-species biofilms. J. Endod. 2009, 35, 1243–1248. [Google Scholar] [CrossRef]
- Boutsioukis, C.; Verhaagen, B.; Walmsley, A.D.; Versluis, M.; van der Sluis, L.W.M. Measurement and visualization of file-to-wall contact during ultrasonically activated irrigation in simulated canals. Int. Endod. J. 2013, 46, 1046–1055. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
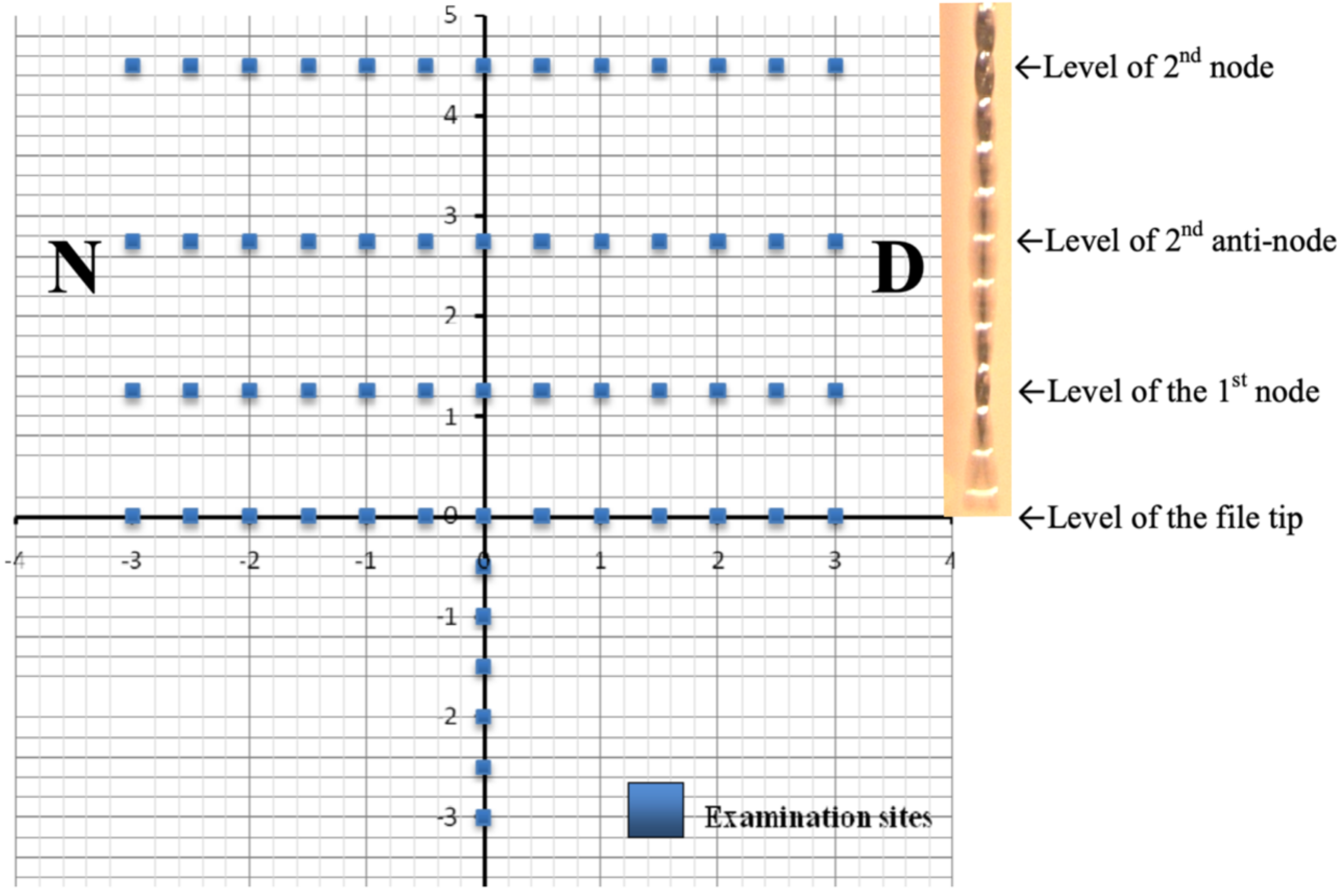
| Distance From the File Tip/mm | Location on y-Axis (see Figure 2) Where Examination Was Made/mm | |
|---|---|---|
| 2nd Node | 4.60 | 4.50 |
| 2nd Anti-node | 2.71 | 2.75 |
| 1st Node | 1.34 | 1.25 |
| 1st Anti-node | 0 | 0 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tse, M.C.C.; Cheung, G.S.P. Spatial Cleaning Action of Ultrasonic Irrigation on Enterococcus faecalis Biofilm. Dent. J. 2020, 8, 42. https://doi.org/10.3390/dj8020042
Tse MCC, Cheung GSP. Spatial Cleaning Action of Ultrasonic Irrigation on Enterococcus faecalis Biofilm. Dentistry Journal. 2020; 8(2):42. https://doi.org/10.3390/dj8020042
Chicago/Turabian StyleTse, Michael C.C., and Gary S.P. Cheung. 2020. "Spatial Cleaning Action of Ultrasonic Irrigation on Enterococcus faecalis Biofilm" Dentistry Journal 8, no. 2: 42. https://doi.org/10.3390/dj8020042
APA StyleTse, M. C. C., & Cheung, G. S. P. (2020). Spatial Cleaning Action of Ultrasonic Irrigation on Enterococcus faecalis Biofilm. Dentistry Journal, 8(2), 42. https://doi.org/10.3390/dj8020042