Study of Treatment Methods for Surrounding Soft Tissues of Implants Following Mandibular Reconstructions with Fibula-Free Flaps

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Representative Cases
3.1. Case 2 (Method 1)
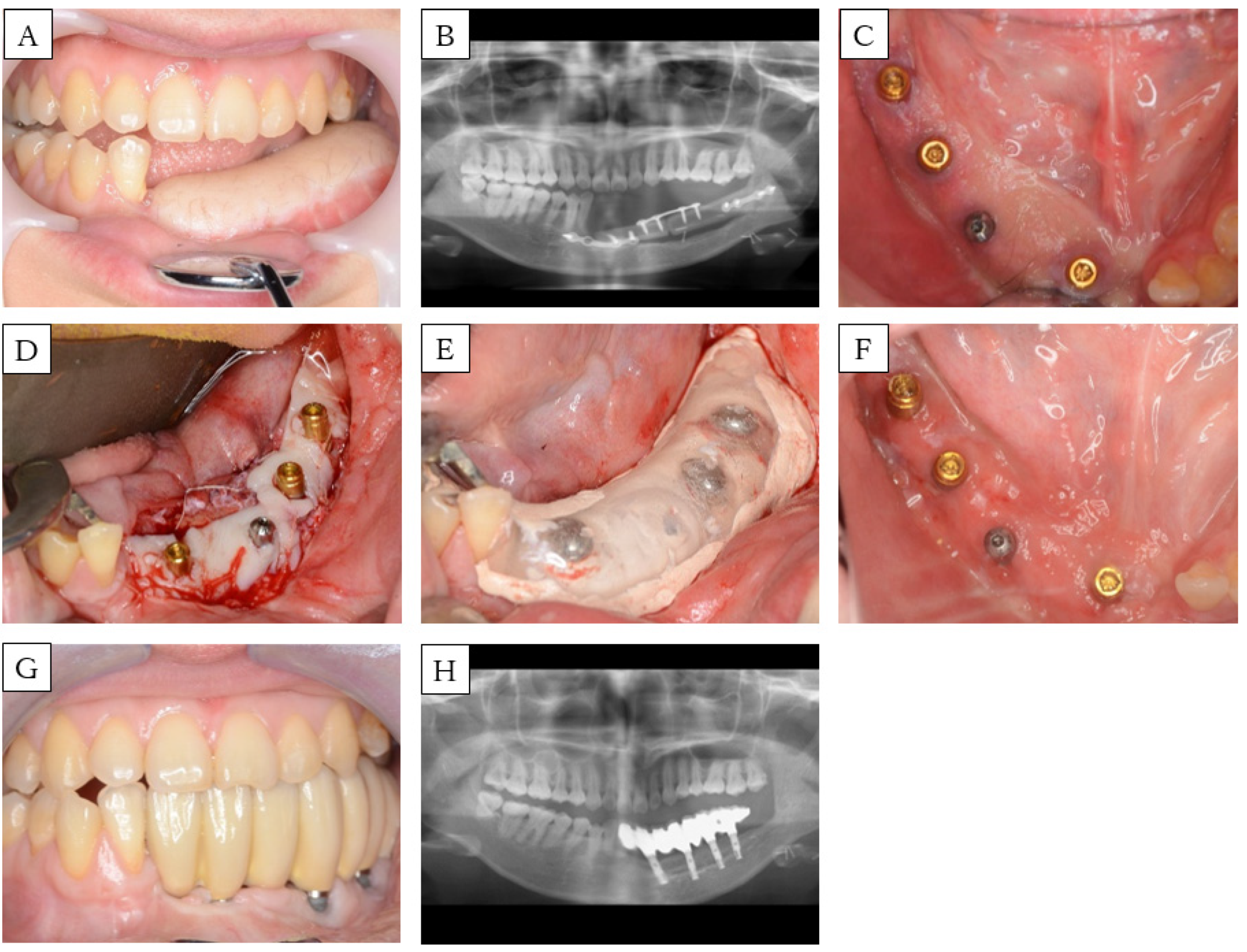
3.2. Case 3 (Method 2)
3.3. Case 5 (Method 3)
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Attia, S.; Wiltfang, J.; Pons-Kühnemann, J.; Wilbrand, J.F.; Streckbein, P.; Kähling, C. Survival of dental implants placed in vascularized fibula free flaps after jaw reconstruction. J. Craniofac. Surg. 2018, 46, 1205–1210. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V.V.; Ebenezer, S.; Kämmerer, P.W.; Jacob, P.C.; Kuriakose, M.A.; Hedne, N. Implants in free fibula flap supporting dental rehabilitation-implant and peri-implant related outcomes of a randomized clinical trial. J. Cranio-Maxillofac. Surg. 2016, 44, 1849–1858. [Google Scholar] [CrossRef] [PubMed]
- Frodel, J.L., Jr.; Funk, G.F.; Capper, D.T.; Fridrich, K.L.; Blumer, J.R.; Haller, J.R.; Hoffman, H.T. Osseointegrated implants: A comparative study of bone thickness in four vascularized bone flaps. Plast. Reconstr. Surg. 1993, 92, 449–458. [Google Scholar] [CrossRef] [PubMed]
- Sagheb, K.; Kumar, V.V.; Azaripour, A.; Walter, C.; Al-Nawas, B.; Kämmerer, P.W. Comparison of conventional twist drill protocol and piezosurgery for implant insertion: An ex vivo study on different bone types. Clin. Oral Implant. Res. 2017, 28, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Sozzi, D.; Novelli, G.; Silva, R.; Connelly, S.T.; Tartaglia, G.M. Implant rehabilitation in fibula-free flap reconstruction: A retrospective study of cases at 1–18 years following surgery. J. Craniofac. Surg. 2017, 45, 1655–1661. [Google Scholar] [CrossRef]
- Warrer, K.; Buser, D.; Lang, N.P.; Karring, T. Plaque—Induced peri-implantitis in the presence or absence of keratinized mucosa. An experimental study in monkeys. Clin. Oral Implants Res. 1995, 6, 131–138. [Google Scholar] [CrossRef]
- Listgarten, M.A.; Lang, N.P.; Schroeder, H.E.; Schroeder, A. Periodontal tissues and their counterparts around endosseous implants. Clin. Oral Implants Res. 1991, 2, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Matsui, T. Soft tissue management around the restorative teeth and implant. Ann. Jpn. Prosthodont. Soc. 2016, 8, 275–280. [Google Scholar] [CrossRef] [Green Version]
- Cairo, F.; Pagliaro, U.; Nieri, M. Soft tissue management at implant sites. J. Clin. Periodontol. 2008, 35, 163–167. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.M.; Wallace, C.G.; Tsai, C.Y.; Shen, Y.F.; Hsu, Y.M.; Wei, F.C. Dental implant outcome after primary implantation into double-barreled fibula osteoseptocutaneous free flap-reconstructed mandible. Plast. Reconstr. Surg. 2011, 128, 1220–1228. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V.V.; Jacob, P.C.; Kuriakose, M.A. Sub-periosteal dissection with denture-guided epithelial regeneration: A novel method for peri-implant soft tissue management in reconstructed mandibles. J. Oral Maxillofac. Surg. 2016, 15, 449–455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogasawara, T.; Sano, K.; Kitagawa, Y.; Miyauchi, K.; Nakamura, M.; Yamada, T. Dermabrasion technique for peri-implant soft tissue management in the mandible reconstructed by free osteocutaneous flap. J. Jpn. Soc. Oral Implantol. 2004, 17, 351–356. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Age (years) | Sex | Cause | Mandible Defect Size (cm) | Mucosal Defect Size (cm) | No. of Implants | View | FGG | Fixing Method of Mucosal Graft | Prosthesis | Timing * (months) | Implant Lost |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 46 | M | SCC | 6.5 | 3 × 2 | 2 |  | no | - | Fixed | - | 1 |
| 2 | 58 | F | SCC | 5 | 4.5 × 1.5 | 3 |  | yes ** | Method 1 | Fixed | 0 | 0 |
| 3 | 30 | F | OS | 7 | 5 × 1 | 4 |  | yes | Method 2 | Fixed | 3 | 0 |
| 4 | 63 | M | SCC | 5 | 5 × 4 | 4 |  | yes | (1) Method 2 *** (2) Method 3 | Removable | (1) 7 (2) 31 | 0 |
| 5 | 66 | M | ORN | 17 | All Gingiva | 4 |  | yes | Method 3 | Removable | 0 | 0 |
| Width of Keratinized Mucosa (mm) | |||||||
|---|---|---|---|---|---|---|---|
| n | Buccal | Lingual | |||||
| (p/i) | Mean | Median | SD | Mean | Median | SD | |
| Method 1 | 1/3 | 0 | 0 | 0 | 0 | 0 | 0 |
| Method 2 | 2/8 | 1.6 | 2 | 0.9 | 1 | 0.5 | 1.2 |
| Method 3 | 2/8 | 5.9 | 5 | 2.1 | 6.4 | 7 | 1.9 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakaue, K.; Horita, S.; Imada, M.; Yamamoto, K.; Sugiura, T.; Ueda, N.; Yamakawa, N.; Nakayama, Y.; Kirita, T. Study of Treatment Methods for Surrounding Soft Tissues of Implants Following Mandibular Reconstructions with Fibula-Free Flaps. Dent. J. 2020, 8, 67. https://doi.org/10.3390/dj8030067
Nakaue K, Horita S, Imada M, Yamamoto K, Sugiura T, Ueda N, Yamakawa N, Nakayama Y, Kirita T. Study of Treatment Methods for Surrounding Soft Tissues of Implants Following Mandibular Reconstructions with Fibula-Free Flaps. Dentistry Journal. 2020; 8(3):67. https://doi.org/10.3390/dj8030067
Chicago/Turabian StyleNakaue, Kazuhiko, Satoshi Horita, Mitsuhiko Imada, Kazuhiko Yamamoto, Tsutomu Sugiura, Nobuhiro Ueda, Nobuhiro Yamakawa, Yohei Nakayama, and Tadaaki Kirita. 2020. "Study of Treatment Methods for Surrounding Soft Tissues of Implants Following Mandibular Reconstructions with Fibula-Free Flaps" Dentistry Journal 8, no. 3: 67. https://doi.org/10.3390/dj8030067
APA StyleNakaue, K., Horita, S., Imada, M., Yamamoto, K., Sugiura, T., Ueda, N., Yamakawa, N., Nakayama, Y., & Kirita, T. (2020). Study of Treatment Methods for Surrounding Soft Tissues of Implants Following Mandibular Reconstructions with Fibula-Free Flaps. Dentistry Journal, 8(3), 67. https://doi.org/10.3390/dj8030067