The Association between D-Dimer and Prognosis in the Patients with Oral Cancer

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sample
2.2. Study Variables
2.3. Data Analyses
3. Results
3.1. Patient Characteristics
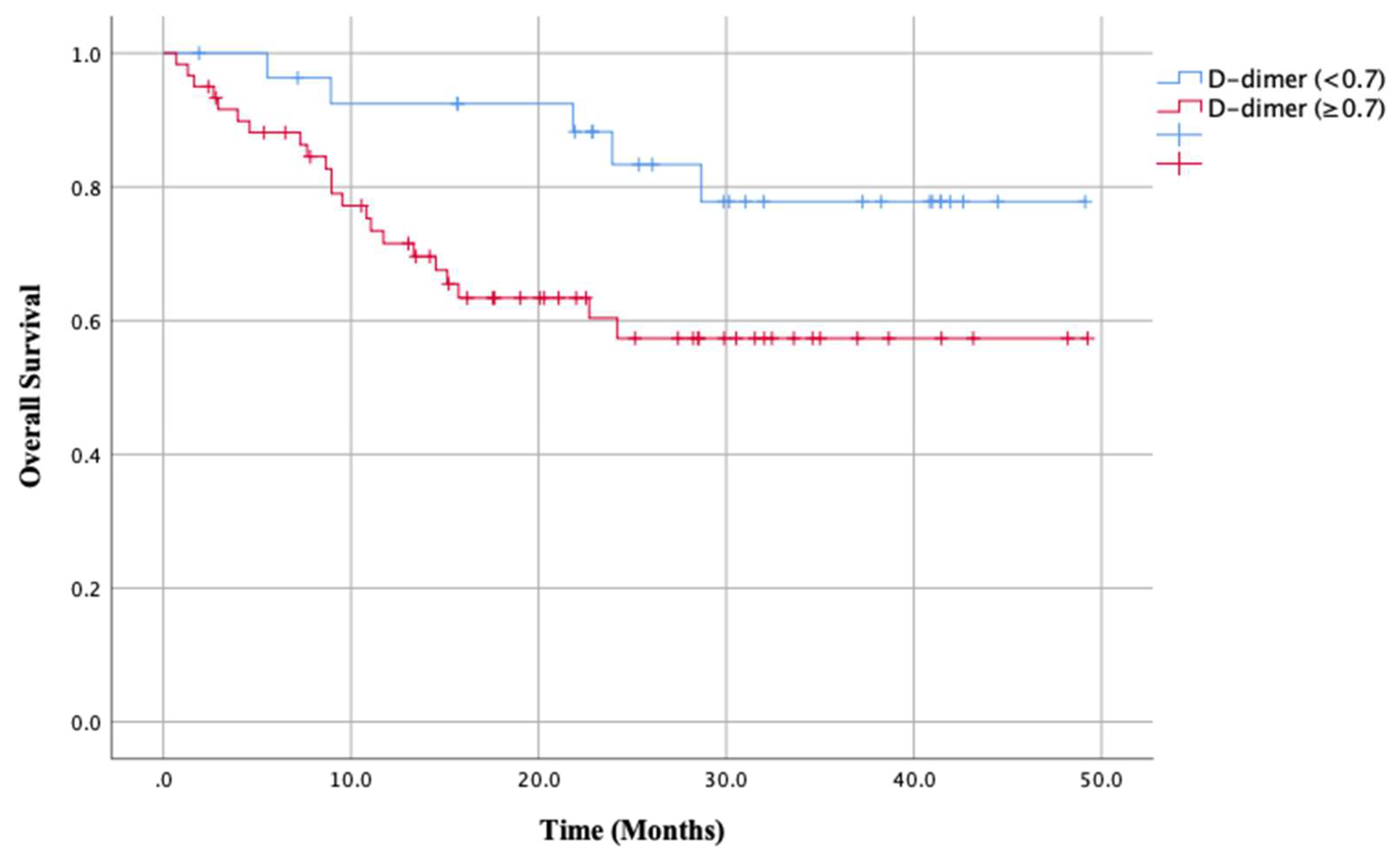
3.2. Clinical Factors and Survival
3.3. Cox Multivariate Regression Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Shiina, Y.; Nakajima, T.; Yamamoto, T.; Tanaka, K.; Sakairi, Y.; Wada, H.; Yoshino, I. The D-dimer level predicts the postoperative prognosis in patients with non-small cell lung cancer. PLoS ONE 2019, 14, e0222050. [Google Scholar] [CrossRef] [PubMed]
- Rong, G.; Fan, W.; Shen, J. High pretreatment plasma D-dimer levels predict poor prognosis in gastrointestinal cancers. Medicine 2019, 98, e16520. [Google Scholar] [CrossRef] [PubMed]
- Diao, D.; Zhu, K.; Wang, Z.; Cheng, Y.; Li, K.; Pei, L.; Dang, C. Prognostic Value of the D-Dimer Test in Oesophageal Cancer During the Perioperative Period. J. Surg. Oncol. 2013, 108, 34–41. [Google Scholar] [CrossRef]
- Ay, C.; Dunkler, D.; Pirker, R.; Thaler, J.; Quehenberger, P.; Wagner, O.; Zielinski, C.; Pabinger, I. High D-dimer levels are associated with poor prognosis in cancer patients. Haematologica 2012, 97, 1158–1164. [Google Scholar] [CrossRef] [Green Version]
- Mascitti, M.; Rubini, C.; De Michele, F.; Balercia, P.; Girotto, R.; Troiano, G.; Muzio, L.L.; Santarelli, A. American Joint Committee on Cancer staging system 7th edition versus 8th edition: Any improvement for patients with squamous cell carcinoma of the tongue? Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 126, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Li, D.; Lei, D.; Yuan, F.; Pei, F.; Zhang, H.; Yu, A.; Wang, K.; Chen, H.; Chen, L.; et al. Tumor-Specific D-Dimer Concentration Ranges and Influencing Factors: A Cross-Sectional Study. PLoS ONE 2016, 11, e0165390. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Tang, L.; Wang, F.; Li, C.; Tian, X.; Huang, X.; Mai, S.J.; Liao, Y.J.; Deng, H.X.; Chen, Q.Y.; et al. Elevated levels of plasma D-dimer predict a worse outcome in patients with nasopharyngeal carcinoma. BMC Cancer 2014, 14, 583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Satoh, T.; Matsumoto, K.; Tanaka, Y.O.; Akiyama, A.; Nakao, S.; Sakurai, M.; Ochi, H.; Onuki, M.; Minaguchi, T.; Sakurai, H.; et al. Incidence of venous thromboembolism before treatment in cervical cancer and the impact of management on venous thromboembolism after commencement of treatment. Thromb. Res. 2013, 131, e127–e132. [Google Scholar] [CrossRef] [PubMed]
- Lim, W.; Gal, L.; Bates, S.M.; Righini, M.; Haramati, L.B.; Lang, E.; Kline, J.A.; Chasteen, S.; Snyder, M.; Patel, P.; et al. American Society of Hematology 2018 guidelines for management of venous thromboembolism: Diagnosis of venous thromboembolism. Blood Adv. 2018, 2, 3226–3256. [Google Scholar] [CrossRef] [PubMed]
- Wu, K.; Lei, J.S.; Mao, Y.Y.; Cao, W.; Wu, H.J.; Ren, Z.H. Prediction of Flap Compromise by Preoperative Coagulation Parameters in Head and Neck Cancer Patients. J. Oral Maxillofac. Surg. 2018, 76, 2453.e1–2453.e7. [Google Scholar] [CrossRef] [PubMed]
- Bucek, R.A.; Reiter, M.; Quehhenberger, P.; Minar, E. C-reactive protein in the diagnosis of deep vein thrombosis. Br. J. Haematol. 2002, 119, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Altiay, G.; Ciftci, A.; Demir, M.; Kocak, Z.; Sut, N.; Tabakoglu, E.; Hatipoglu, O.N.; Caglar, T. High Plasma D-dimer Level Is Associated With Decreased Survival in Patients With Lung Cancer. Clin. Oncol. 2007, 19, 494–498. [Google Scholar] [CrossRef] [PubMed]
- McMillan, D.C.; Canna, K.; McArdle, C.S. Systemic inflammatory response predicts survival following curative resection of colorectal cancer. Br. J. Surg. 2003, 90, 215–219. [Google Scholar] [CrossRef] [PubMed]
- McMillan, D.C. The systemic inflammation-based Glasgow Prognostic Score: A decade of experience in patients with cancer. Cancer Treat. Rev. 2013, 39, 534–540. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.N.; Chuang, H.C.; Lin, Y.T.; Fang, F.M.; Li, S.H.; Chien, C.Y. Prognosis of neutrophil-to-lymphocyte ratio in clinical early-stage tongue (cT1/T2N0) cancer. OncoTargets Ther. 2017, 10, 3917–3924. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variable | D-Dimer (<0.7) (n = 28) | D-Dimer (≥0.7) (n = 60) | p Value |
|---|---|---|---|
| Gender | 0.574 | ||
| Male | 19 (67.9%) | 37 (61.7%) | |
| Female | 9 (32.1%) | 23 (38.3%) | |
| Site | 0.962 | ||
| Tongue | 9 (32.1%) | 18 (30.0%) | |
| Lower gingiva | 8 (28.6%) | 17 (28.3%) | |
| Buccal mucosa | 3 (10.7%) | 9 (15.0%) | |
| Upper gingiva | 2 (7.1%) | 6 (10.0%) | |
| Floor of mouth | 3 (10.7%) | 3 (5.0%) | |
| Maxillary sinus | 1 (3.6%) | 3 (5.0%) | |
| Others | 2 (7.1%) | 4 (6.7%) | |
| T stage | 0.501 | ||
| T1 | 7 (25%) | 7 (11.7%) | |
| T2 | 7 (25%) | 20 (30.0%) | |
| T3 | 1 (3.6%) | 5 (8.3%) | |
| T4a | 9 (32.1%) | 21 (35.0%) | |
| T4b | 4 (14.3%) | 7 (11.6%) | |
| N stage | 0.402 | ||
| N0 | 20 (71.4%) | 31 (51.7%) | |
| N1 | 3 (10.7%) | 9 (15.0%) | |
| N2b | 5 (17.9%) | 16 (26.7%) | |
| N2c | 0 (0%) | 3 (5.0%) | |
| N3 | 0 (0%) | 1 (1.7%) | |
| Stage | 0.456 | ||
| I | 7 (25%) | 6 (10.0%) | |
| II | 6 (21.4%) | 14 (23.3%) | |
| III | 1 (3.6%) | 3 (5.0%) | |
| IVA | 11 (39.3%) | 31 (51.7%) | |
| IVB | 3 (10.7%) | 6 (10.0%) | |
| Management a | 0.157 | ||
| S | 16 (57.1%) | 34 (56.7%) | |
| S+RT | 4 (14.3%) | 4 (6.7%) | |
| S+CRT | 6 (21.4%) | 6 (10.0%) | |
| RT | 1 (3.6%) | 9(15.0%) | |
| RT+C | 1 (3.6%) | 7 (11.7%) | |
| Pathological diagnosis b | 0.093 | ||
| SCC | 25 (89.3%) | 59 (98.3%) | |
| ACC | 2 (7.1%) | 0 (0%) | |
| Others | 1 (3.6%) | 1 (1.7%) | |
| VTE c | 0.094 | ||
| Absent | 27 (96.4%) | 49 (81.7%) | |
| Present | 1 (3.6%) | 11 (18.3%) | |
| Smoking | 0.019 * | ||
| Absent | 22 (78.6%) | 34 (56.7%) | |
| Pre | 1 (3.6%) | 18 (30.0%) | |
| Present | 5 (17.9%) | 8 (13.3%) | |
| Alcohol | 0.299 | ||
| Absent | 20 (71.4%) | 36 (60.0%) | |
| Present | 8 (28.6%) | 24 (40.0%) |
| Variable Median (Range) | D-Dimer (<0.7) (n = 28) | D-Dimer (≥0.7) (n = 60) | p Value |
|---|---|---|---|
| Age (Years) | 65.5 (34~84) | 76.0 (39~93) | <0.0001 ** |
| BMI (Kg/m2) | 21.52 (16.81~29.48) | 22.26 (14.29~32.65) | 0.610 |
| Caprini Score | 6 (4~8) | 6 (4~8) | 0.064 |
| Neutrocyte count (×103/µL) | 4.129 (1.995~6.845) | 4.513 (1.666~8.880) | 0.182 |
| CRP (mg/µL) | 0.40 (0~0.60) | 0.15 (0.03~10.92) | 0.002 ** |
| PLT count (×103/µL) | 216.50 (164.0~384.0) | 226.5 (68.0~454.0) | 0.750 |
| Lymphocyte count (×103/µL) | 1.653 (0.630~2.843) | 1.570 (0.529~3.081) | 0.979 |
| Monocyte count (×103/µL) | 0.358 (0.168~0.820) | 0.384 (0.122~0.792) | 0.232 |
| LMR | 4.72 (1.66~9.85) | 3.98 (1.461~19.263) | 0.216 |
| NLR | 2.34 (1.38~6.99) | 2.91 (0.96~12.22) | 0.173 |
| PLR | 150.8 (82.7~344.5) | 148.5 (70.6~319.6) | 0.795 |
| Variable | No of Patients (%) | Overall Survival (%) | p Value |
|---|---|---|---|
| Gender | 0.842 | ||
| Male | 56 (63.6) | 61.8 | |
| Female | 32 (36.4) | 67.3 | |
| Site | 0.588 | ||
| Tongue | 27 (30.7) | 59.6 | |
| Lower gingiva | 25 (28.4) | 76.1 | |
| Buccal mucosa | 12 (13.6) | 46.9 | |
| Upper gingiva | 8 (9.1) | 75.0 | |
| Floor of mouth | 6 (6.8) | 62.5 | |
| Maxillary sinus | 4 (4.5) | 50.0 | |
| Others | 6 (6.8) | 80.0 | |
| T stage | 0.270 | ||
| T1 | 14 (15.9) | 68.2 | |
| T2 | 27 (30.7) | 77.2 | |
| T3 | 6 (6.8) | 55.6 | |
| T4a | 30 (34.1) | 58.3 | |
| T4b | 11 (12.5) | 39.8 | |
| N stage | 0.899 | ||
| N0 | 51 (58.0) | 65.2 | |
| N1 | 12 (13.6) | 73.3 | |
| N2b | 21 (23.9) | 55.1 | |
| N2c | 3 (3.4) | 66.7 | |
| N3 | 1 (1.1) | 100 | |
| Stage | 0.364 | ||
| I | 13 (14.8) | 75.0 | |
| II | 20 (22.7) | 72.6 | |
| III | 5 (5.7) | 50.0 | |
| IVA | 42 (4.8) | 62.4 | |
| IVB | 9 (10.2) | 41.7 | |
| Management a | <0.0001 ** | ||
| S | 50 (56.8) | 90.0 | |
| S+RT | 8 (9.1) | 37.5 | |
| S+CRT | 12 (13.6) | 40.0 | |
| R | 10 (11.4) | 28.1 | |
| R+C | 8 (9.1) | 21.9 | |
| Pathological diagnosis b | 0.719 | ||
| SCC | 84 (95.5) | 63.3 | |
| ACC | 2 (2.3) | 100 | |
| Others | 2 (2.3) | 50.0 | |
| VTE c | 0.387 | ||
| Absent | 76 (86.4) | 71.1 | |
| Present | 12 (13.6) | 58.3 | |
| Smoking | 0.922 | ||
| Absent | 56 (63.6) | 63.1 | |
| Pre | 19 (21.6) | 73.0 | |
| Present | 13 (14.8) | 61.5 | |
| Alcohol | 0.345 | ||
| Absent | 56 (63.6) | 65.9 | |
| Present | 32 (36.4) | 59.6 |
| Factor | HR | 95% CI | p Value |
|---|---|---|---|
| Univariate analysis | |||
| Age | 1.035 | 1.001–1.069 | 0.042 * |
| BMI | 0.968 | 0.860–1.089 | 0.377 |
| Smoking (Present vs. Pre, Absent) | 1.161 | 0.438–3.076 | 0.764 |
| Caprini Score | 0.877 | 0.630–1.222 | 0.439 |
| Stage (I, II vs. II, IV) | 0.443 | 0.179–1.098 | 0.079 |
| PLT | 1.001 | 0.996–1.006 | 0.767 |
| Neutrocyte count | 1.297 | 1.061–1.585 | 0.011 * |
| Lymphocyte count | 0.625 | 0.313–1.413 | 0.289 |
| Monocyte count | 6.610 | 0.597–73.151 | 0.124 |
| NLR | 1.172 | 1.007–1.364 | 0.041 * |
| LMR | 0.855 | 0.693–1.055 | 0.144 |
| PLR | 1.002 | 0.996–1.007 | 0.583 |
| CRP | 1.174 | 1.036–1.329 | 0.012 * |
| D-dimer (<0.7 vs. ≥0.7) | 2.744 | 1.034–7.281 | 0.043 * |
| Management (Mainly S vs. R) | 4.972 | 2.282–10.834 | 0.0002 * |
| Multivariate survival analysis | |||
| Age | 1.027 | 0.984–1.072 | 0.222 |
| Neutrocyte count | 1.247 | 0.957–1.625 | 0.101 |
| CRP | 0.969 | 0.821–1.1441 | 0.713 |
| D-dimer (<0.7 vs. ≥0.7) | 1.332 | 0.440–4.032 | 0.612 |
| Management (Mainly S vs. R) | 3.274 | 1.397–7.676 | 0.006 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamagata, K.; Fukuzawa, S.; Ishibashi-Kanno, N.; Uchida, F.; Yanagawa, T.; Bukawa, H. The Association between D-Dimer and Prognosis in the Patients with Oral Cancer. Dent. J. 2020, 8, 84. https://doi.org/10.3390/dj8030084
Yamagata K, Fukuzawa S, Ishibashi-Kanno N, Uchida F, Yanagawa T, Bukawa H. The Association between D-Dimer and Prognosis in the Patients with Oral Cancer. Dentistry Journal. 2020; 8(3):84. https://doi.org/10.3390/dj8030084
Chicago/Turabian StyleYamagata, Kenji, Satoshi Fukuzawa, Naomi Ishibashi-Kanno, Fumihiko Uchida, Toru Yanagawa, and Hiroki Bukawa. 2020. "The Association between D-Dimer and Prognosis in the Patients with Oral Cancer" Dentistry Journal 8, no. 3: 84. https://doi.org/10.3390/dj8030084
APA StyleYamagata, K., Fukuzawa, S., Ishibashi-Kanno, N., Uchida, F., Yanagawa, T., & Bukawa, H. (2020). The Association between D-Dimer and Prognosis in the Patients with Oral Cancer. Dentistry Journal, 8(3), 84. https://doi.org/10.3390/dj8030084