
Molar Incisor Hypomineralization in Children with Intellectual Disabilities

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Weerheijm, K.L. Molar incisor hypomineralization (MIH): Clinical presentation, aetiology and management. Dent. Update 2004, 31, 9–12. [Google Scholar] [CrossRef] [PubMed]
- Lygidakis, N.A.; Wong, F.; Jälevik, B.; Vierrou, A.M.; Alaluusua, S.; Espelid, I. Best Clinical Practice Guidance for clinicians dealing with children presenting with Molar-Incisor-Hypomineralisation (MIH): An EAPD Policy Document. Eur. Arch. Paediatr. Dent. 2010, 11, 75–81. [Google Scholar] [CrossRef]
- William, V.; Messer, L.B.; Burrow, M.F. Molar incisor hypomineralization: Review and recommendations for clinical management. Pediatr Dent. 2006, 28, 224–232. [Google Scholar] [PubMed]
- Lygidakis, N.A.; Dimou, G.; Marinou, D. Molar-incisor-hypomineralisation (MIH). A retrospective clinical study in Greek children. II. Possible medical aetiological factors. Eur. Arch. Paediatr. Dent. 2008, 9, 207–217. [Google Scholar] [CrossRef] [PubMed]
- Kemoli, A.M. Prevalence of molar incisor hypomineralisation in six to eight year-olds in two rural divisions in Kenya. East Afr. Med. J. 2008, 85, 514–519. [Google Scholar] [CrossRef]
- Rodd, H.D.; Boissonade, F.M.; Day, P.F. Pulpal status of hypomineralised permanent molars. Pediatr. Dent. 2007, 29, 514–520. [Google Scholar]
- Raposo, F.; de Carvalho Rodrigues, A.C.; Lia, É.N.; Leal, S.C. Prevalence of Hypersensitivity in Teeth Affected by Molar-Incisor Hypomineralization (MIH). Caries Res. 2019, 53, 424–430. [Google Scholar] [CrossRef]
- Discepolo, K.E.; Baker, S. Adjuncts to traditional local anesthesia techniques in instance of hypomineralized teeth. N. Y. State Dent. J. 2011, 77, 22–27. [Google Scholar]
- Jälevik, B.; Klingberg, G.A. Dental treatment, dental fear and behaviour management problems in children with severe enamel hypomineralization of their permanent first molars. Int. J. Paediatr. Dent. 2002, 12, 24–32. [Google Scholar]
- Hočevar, L.; Kovač, J.; Podkrajšek, K.T.; Battelino, S.; Pavlič, A. The possible influence of genetic aetiological factors on molar–incisor hypomineralisation. Arch. Oral Biol. 2020, 118, 104848. [Google Scholar] [CrossRef]
- Fagrell, T. Molar incisor hypomineralization. Morphological and chemical aspects, onset and possible etiological factors. Swed. Dent. J. Suppl. 2011, 216, 11–83. [Google Scholar]
- Subramaniam, P.; Gupta, T.; Sharma, A. Prevalence of molar incisor hypomineralization in 7–9-year-old children of Bengaluru City, India. Contemp. Clin. Dent. 2016, 7, 11–15. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, R.J.P.B.; Andrade, N.S.; Queiroz, L.C.C.; Mendes, F.M.; Moura, M.S.; Moura, L.F.A.D.; Lima, M.D.M. Exploring the association between genetic and environmental factors and molar incisor hypomineralization: Evidence from a twin study. Int. J. Paediatr. Dent. 2018, 28, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Brogårdh-Roth, S.; Matsson, L.; Klingberg, G. Molar-incisor hypomineralization and oral hygiene in 10-to-12-yr-old Swedish children born preterm. Eur. J. Oral Sci. 2011, 119, 33–39. [Google Scholar] [CrossRef]
- Miclea, D.; Peca, L.; Cuzmici, Z.; Pop, I.V. Genetic testing in patients with global developmental delay/intellectual disabilities. A review. Clujul. Med. 2015, 88, 288–292. [Google Scholar] [CrossRef] [Green Version]
- Jindal, C.; Palaskar, S.; Kler, S. The Prevalence of the Developmental Defects of Enamel in a Group of 8–15 Years Old Indian Children with Developmental Disturbances. J. Clin. Diagn. Res. 2011, 5, 669–674. [Google Scholar]
- Farah, R.A.; Swain, M.V.; Drummond, B.K.; Cook, R.; Atieh, M. Mineral density of hypomineralised enamel. J. Dent. 2010, 38, 50–58. [Google Scholar] [CrossRef]
- Weerheijm, K.L.; Duggal, M.; Mejàre, I.; Papagiannoulis, L.; Koch, G.; Martens, L.C.; Hallonsten, A.L. Judgement criteria for molar incisor hypomineralisation (MIH) in epidemiologic studies: A summary of the European meeting on MIH held in Athens, 2003. Eur. J. Paediatr. Dent. 2003, 4, 110–113. [Google Scholar]
- Ghanim, A.; Elfrink, M.; Weerheijm, K.; Mariño, R.; Manton, D. A practical method for use in epidemiological studies on enamel hypomineralisation. Eur. Arch. Paediatr. Dent. 2015, 16, 235–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franco, K.M.; Line, S.R.; de Moura-Ribeiro, M.V. Prenatal and neonatal variables associated with enamel hypoplasia in deciduous teeth in low birth weight preterm infants. J. Appl. Oral Sci. 2007, 15, 518–523. [Google Scholar] [CrossRef]
- Ng, J.J.; Eu, O.C.; Nair, R.; Hong, C.H. Prevalence of molar incisor hypomineralization (MIH) in Singaporean children. Int. J. Paediatr. Dent. 2015, 25, 73–78. [Google Scholar] [CrossRef]
- Martínez, A.; Cubillos, P.; Jiménez, M.; Brethauer, U.; Catalán, P.; González, U. Prevalence of developmental enamel defects in mentally retarded children. ASDC J. Dent. Child. 2002, 69, 151–155. [Google Scholar]
- Zawaideh, F.I.; Al-Jundi, S.H.; Al-Jaljoli, M.H. Molar incisor hypomineralisation: Prevalence in Jordanian children and clinical characteristics. Eur. Arch. Paediatr. Dent. 2011, 12, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Ghanim, A.; Bagheri, R.; Golkari, A.; Manton, D. Molar-incisor hypomineralisation: A prevalence study amongst primary schoolchildren of Shiraz, Iran. Eur. Arch. Paediatr. Dent. 2014, 6, 75–82. [Google Scholar] [CrossRef]
- Glodkowska, N.; Emerich, K. Molar Incisor Hypomineralization: Prevalence and severity among children from Nothern Poland. Eur. J. Paediatr. Dent. 2019, 20, 59–66. [Google Scholar] [PubMed]
- Ordonez-Romero, I.; Jijon-Granja, Y.; Ubilla-Mazzini, W.; Porro-Porro, L.; Alvarez-Giler, G. Distribution of Molar Incisor Hypomineralization in Ecuadorian Children. Dent. Hypotheses 2019, 10, 65–69. [Google Scholar] [CrossRef]
- Calderara, P.C.; Gerthoux, P.M.; Mocarelli, P.; Lukinmaa, P.L.; Tramacere, P.L.; Alaluusua, S. The prevalence of Molar Incisor Hypomineralisation (MIH) in a group of Italian school children. Eur. J. Paediatr. Dent. 2005, 6, 79–83. [Google Scholar]
- Jasulaityte, L.; Veerkamp, K.L.; Weerheijm, K.L. Molar incisor hypomineralisation: Review and prevalence data from a study of primary school children in Kaunas (Lithuania). Eur. Arch. Paediatr. Dent. 2007, 8, 87–94. [Google Scholar] [CrossRef]
- Muratbegovic, A.; Marcovic, M.; Ganibegovic, S.M. Molar Incisor Hypomineralisation in Bosnia and: Prevalence, Aetiology and Clinical Consequences in Medium Caries Activity Population. Eur. Arch. Paediatr. Dent. 2007, 8, 189–194. [Google Scholar] [CrossRef]
- Temilola, O.D.; Folayan, M.O.; Oyedele, T. The prevalence and pattern of deciduous molar hypomineralization and molar-incisor hypomineralization in children from a suburban population in Nigeria. BMC Oral Health 2015, 15, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koruyucu, M.; Özel, S.; Tuna, E.B. Prevalence and etiology of molar-incisor hypomineralization (MIH) in the city of Istanbul. J. Dent. Sci. 2018, 13, 318–328. [Google Scholar] [CrossRef] [PubMed]
- Buchgraber, B.; Kqiku, L.; Ebeleseder, K.A. Molar incisor hypomineralization: Proportion and severity in primary public school children in Graz, Austria. Clin. Oral Investig. 2018, 22, 757–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdalla, H.E.; Abuaffan, A.H.; Kemoli, A.M. Molar incisor hypomineralization, prevalence, pattern and distribution in Sudanese children. BMC Oral Health. 2021, 21, 9. [Google Scholar] [CrossRef] [PubMed]
- Fearne, J.; Anderson, P.; Davis, G.R. 3D X-ray microscopic study of the extent of variations in enamel density in first permanent molars with idiopathic enamel hypomineralisation. Br. Dent. J. 2004, 196, 634–638; discussion 625. [Google Scholar] [CrossRef] [Green Version]
- Mužinić, D.; Vrček, D.; IvaniševićMalčić, A.; Matijević, J.; RošinGrget, K.; JukićKrmek, S. The Concentration of Fluorides in tap Water and Commercial Bottled Beverages. Acta Stomatol. Croat. 2012, 46, 23–30. [Google Scholar]
- Da Costa-Silva, C.M.; Ambrosano, G.M.; Jeremias, F.; De Souza, J.F.; Mialhe, F.L. Increase in severity of molar-incisor hypomineralization and its relationship with the colour of enamel opacity: A prospective cohort study. Int. J. Paediatr. Dent. 2011, 21, 333–341. [Google Scholar] [CrossRef]
- Talwar, M.; Borzabadi-Farahani, A.; Lynch, E.; Borsboom, P.; Ruben, J. Remineralization of Demineralized Enamel and Dentine Using 3 Dentifrices-An InVitro Study. Dent. J. 2019, 7, 91. [Google Scholar] [CrossRef] [Green Version]
- Scribante, A.; DermenakiFarahani, M.R.; Marino, G.; Matera, C.; Rodriguez YBaena, R.; Lanteri, V.; Butera, A. Biomimetic Effect of Nano-Hydroxyapatite in Demineralized Enamel before Orthodontic Bonding of Brackets and Attachments: Visual, Adhesion Strength, and Hardness in In Vitro Tests. Biomed. Res. Int. 2020, 2020, 6747498. [Google Scholar] [CrossRef] [Green Version]
- Khanduri, N.; Kurup, D.; Mitra, M. Quantitative evaluation of remineralizing potential of three agents on artificially demineralized human enamel using scanning electron microscopy imaging and energy-dispersive analytical X-ray element analysis: An in vitro study. Dent. Res. J. 2020, 17, 366–372. [Google Scholar] [CrossRef]


{kind=link}
| Gender | Children with Intellectual Disabilities (N/%) | Control Group (N/%) |
|---|---|---|
| Male | 46 (63.9) | 38 (52.8) |
| Female | 26 (36.1) | 34 (47.2) |
| Total | 72 (100) | 72 (100) |
| Age Group | Children with Intellectual Disabilities (N/%) | Control Group (N/%) |
|---|---|---|
| 5–7 | 6 (8.3) | 6 (8.3) |
| 8–13 | 31 (43.1) | 36 (50.0) |
| 14–18 | 35 (48.6) | 30 (41.7) |
| Characteristics of Enamel Defects | Group of Children with Intellectual Disabilities | Control Group |
|---|---|---|
| Number of children affected (p = 0.033) | 8 (11.1%) | 1 (1.4%) |
| Number of index teeth affected | 19 (12 molars, 7 incisors) | 2 (2 molars) |
| Number of affected index teeth per child | 2 index teeth, 4 children 1 index tooth, 2 children 3 index teeth, 1 child 5 index teeth, 1 child | 2 index teeth |
| Mean number of affected teeth | 2 index teeth | 2 index teeth |
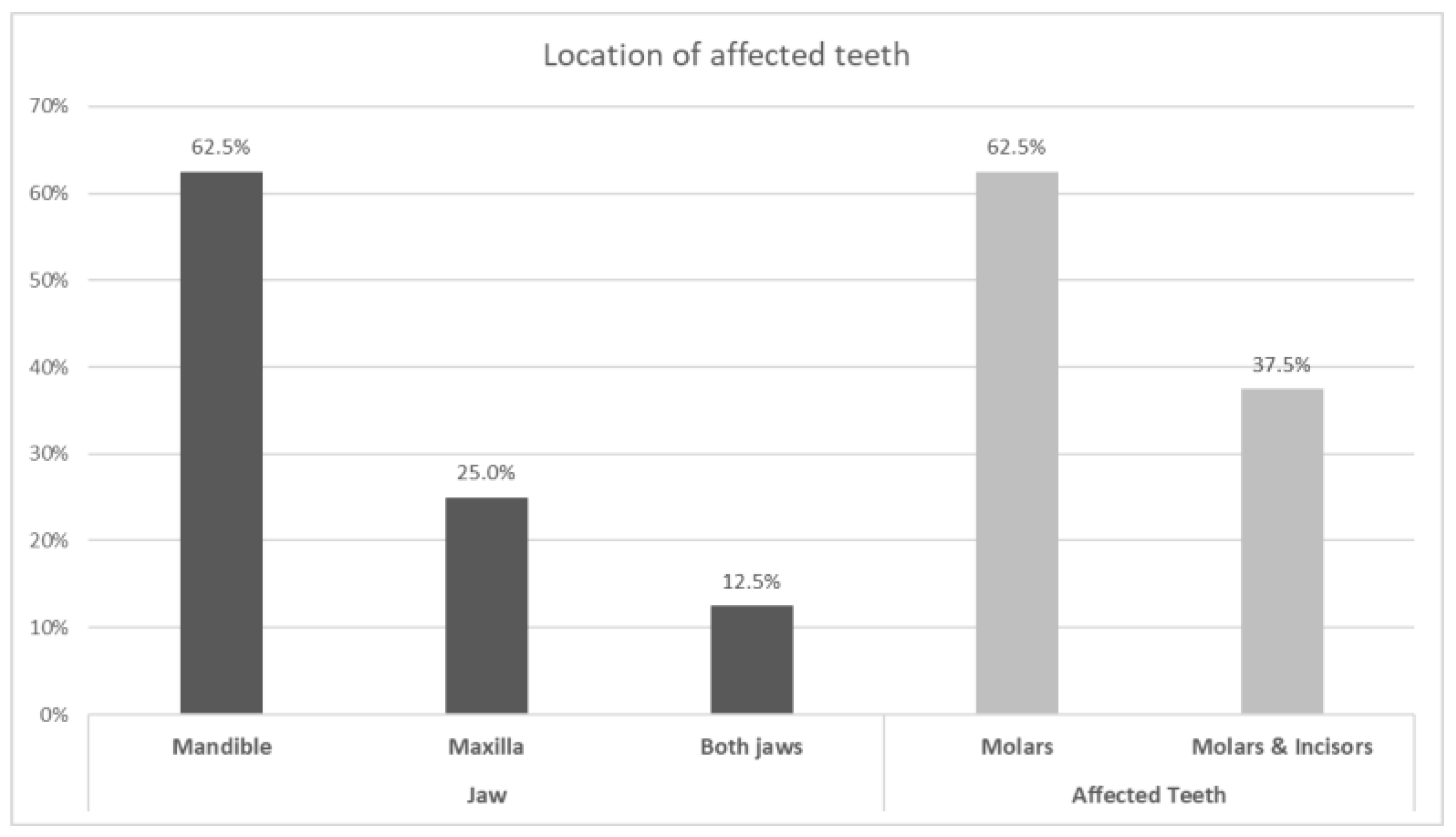
| Location | Jaw, mandible (62.5%) maxilla (25%) both jaws (12.5%) Teeth, only molars (62.5%) molars and incisors (37.5%) Surfaces, buccal (62.5%), occlusal (12.5), palatal (12.5%), buccal and occlusal (12.5%) | Jaw—only maxilla Teeth—only molars Surfaces- Buccal and occlusal |
| Color | White (87.5%) Brown (12.5%) | Brown |
| Shape of enamel defects | Asymmetric (75%) Symmetric (25%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brzovic Rajic, V.; Modric, V.E.; Ivanisevic Malcic, A.; Gorseta, K.; Karlovic, Z.; Verzak, Z. Molar Incisor Hypomineralization in Children with Intellectual Disabilities. Dent. J. 2021, 9, 21. https://doi.org/10.3390/dj9020021
Brzovic Rajic V, Modric VE, Ivanisevic Malcic A, Gorseta K, Karlovic Z, Verzak Z. Molar Incisor Hypomineralization in Children with Intellectual Disabilities. Dentistry Journal. 2021; 9(2):21. https://doi.org/10.3390/dj9020021
Chicago/Turabian StyleBrzovic Rajic, Valentina, Vesna Erika Modric, Ana Ivanisevic Malcic, Kristina Gorseta, Zoran Karlovic, and Zeljko Verzak. 2021. "Molar Incisor Hypomineralization in Children with Intellectual Disabilities" Dentistry Journal 9, no. 2: 21. https://doi.org/10.3390/dj9020021
APA StyleBrzovic Rajic, V., Modric, V. E., Ivanisevic Malcic, A., Gorseta, K., Karlovic, Z., & Verzak, Z. (2021). Molar Incisor Hypomineralization in Children with Intellectual Disabilities. Dentistry Journal, 9(2), 21. https://doi.org/10.3390/dj9020021