
Time Efficiency of Digitally and Conventionally Produced Single-Unit Restorations


Abstract
:1. Introduction
2. Materials and Methods
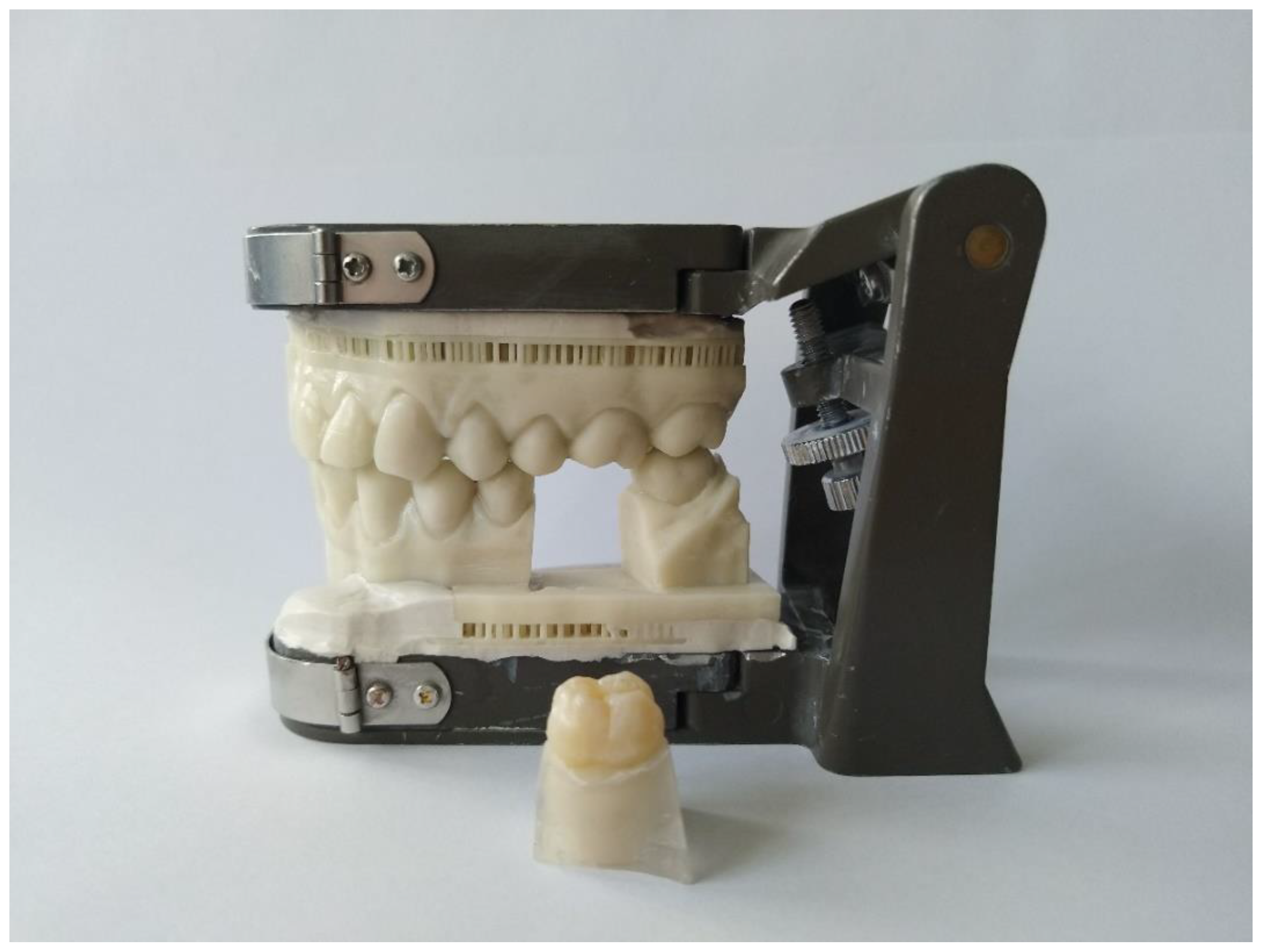
2.1. Model Fabrication
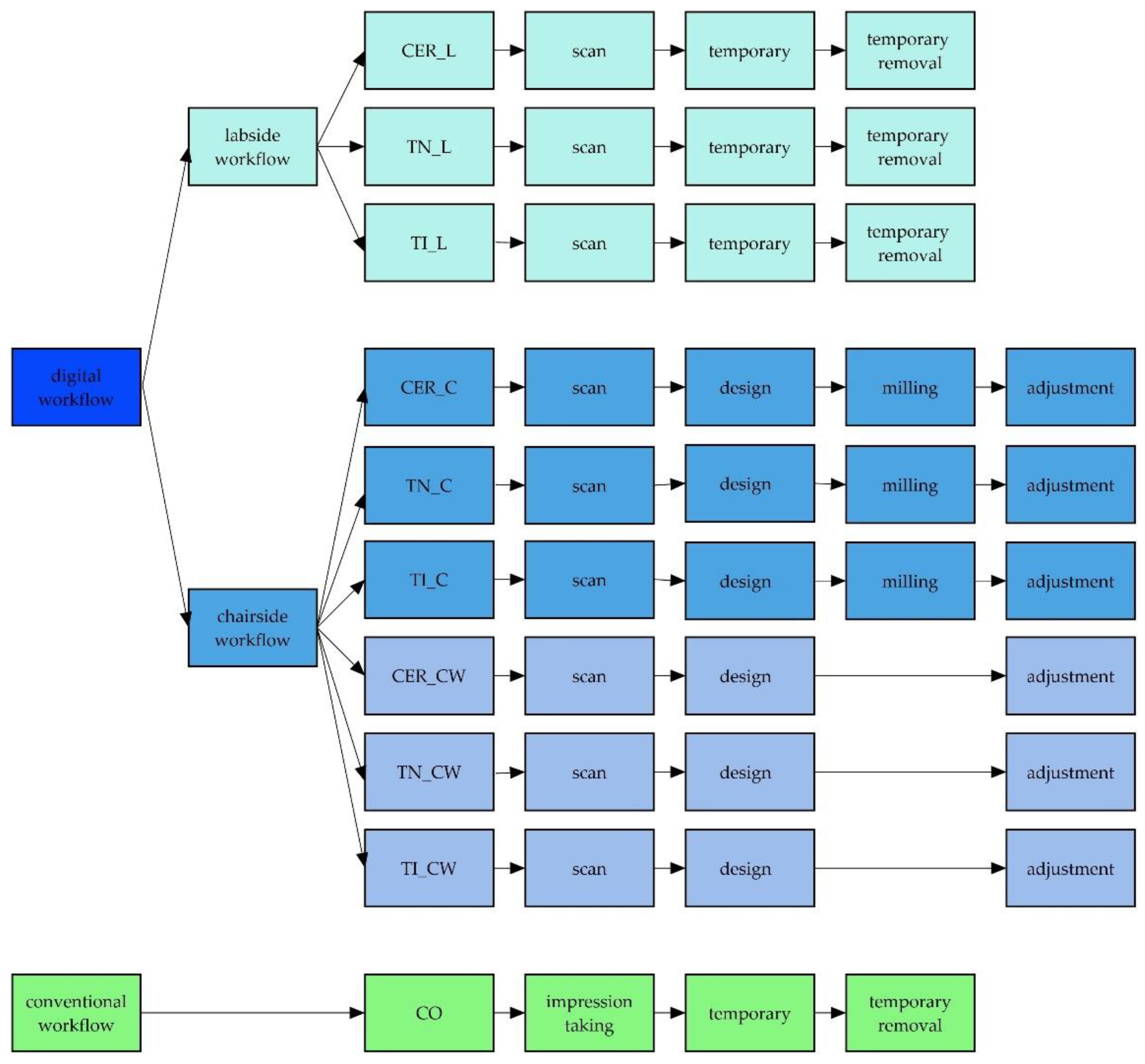
2.2. Overview of the Different Workflows
2.3. Labside Workflow
2.4. Chairside Workflow
2.5. Chairside Workflow Working Time
2.6. Conventional Workflow
2.7. Statistics
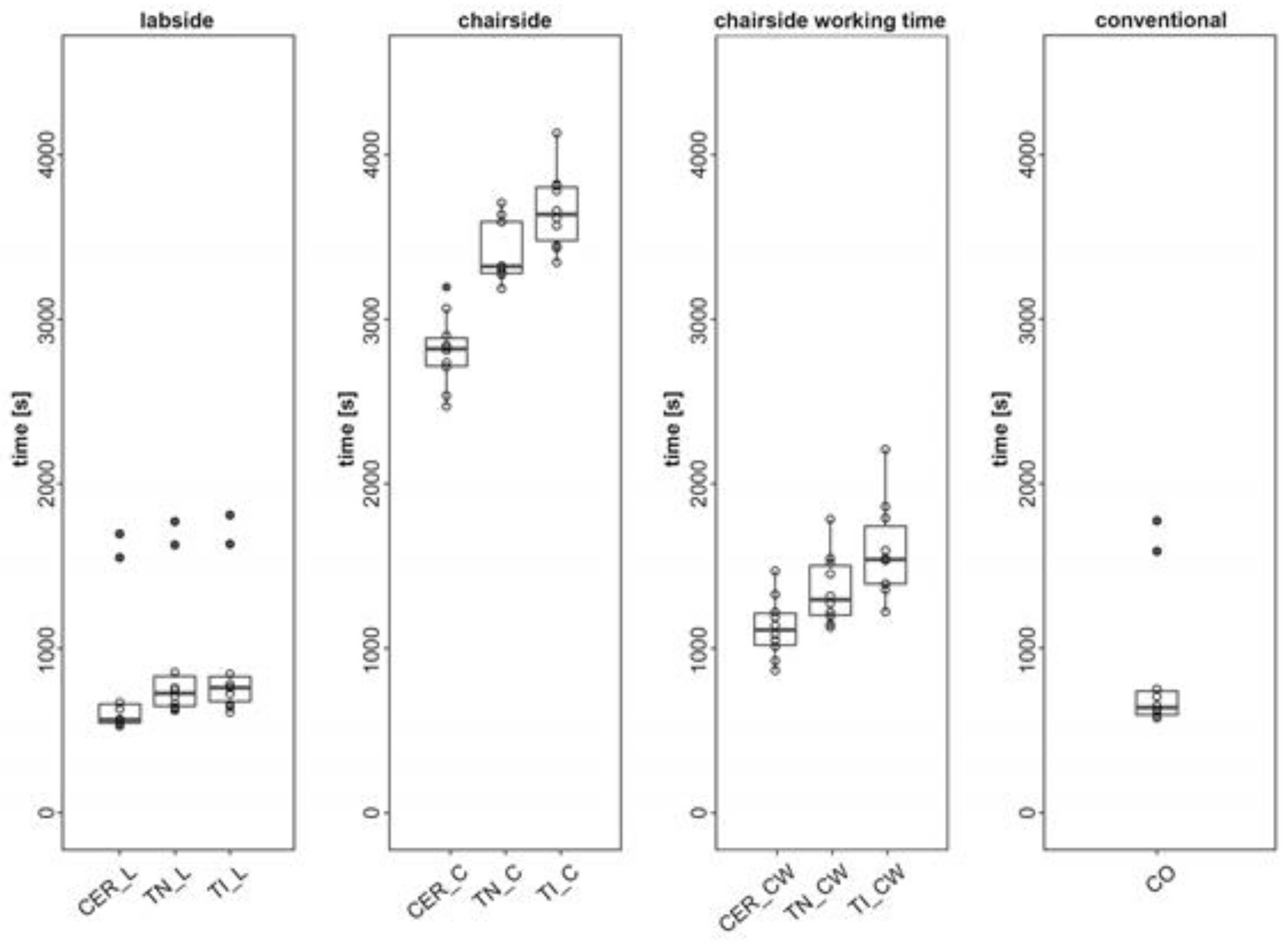
3. Results
3.1. Labside Workflow
3.2. Chairside Workflow
3.3. Chairside Workflow Working Time
3.4. Conventional Workflow
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Beuer, F.; Schweiger, J.; Edelhoff, D. Digital dentistry: An overview of recent developments for CAD/CAM generated restorations. Br. Dent. J. 2008, 204, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Davidowitz, G.; Kotick, P.G. The use of CAD/CAM in dentistry. Dent. Clin. N. Am. 2011, 55, 559–570. [Google Scholar] [CrossRef] [PubMed]
- van Noort, R. The future of dental devices is digital. Dent. Mater. 2012, 28, 3–12. [Google Scholar] [CrossRef]
- Poticny, D.J.; Klim, J. CAD/CAM in-office technology: Innovations after 25 years for predictable, esthetic outcomes. J. Am. Dent. Assoc. 2010, 141 (Suppl. 2), 5S–9S. [Google Scholar] [CrossRef]
- Sannino, G.; Germano, F.; Arcuri, L.; Bigelli, E.; Arcuri, C.; Barlattani, A. CEREC CAD/CAM Chairside System. Oral Implantol. 2014, 7, 57–70. [Google Scholar]
- Zimmermann, M.; Koller, C.; Rumetsch, M.; Ender, A.; Mehl, A. Precision of guided scanning procedures for full-arch digital impressions in vivo. J. Orofac. Orthop. 2017, 78, 466–471. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, T.; Hotta, Y.; Kunii, J.; Kuriyama, S.; Tamaki, Y. A review of dental CAD/CAM: Current status and future perspectives from 20 years of experience. Dent. Mater. J. 2009, 28, 44–56. [Google Scholar] [CrossRef] [Green Version]
- Ceyhan, J.A.; Johnson, G.H.; Lepe, X. The effect of tray selection, viscosity of impression material, and sequence of pour on the accuracy of dies made from dual-arch impressions. J. Prosthet. Dent. 2003, 90, 143–149. [Google Scholar] [CrossRef]
- Duret, F.; Blouin, J.L.; Duret, B. CAD-CAM in dentistry. J. Am. Dent. Assoc. 1988, 117, 715–720. [Google Scholar] [CrossRef] [Green Version]
- Mennito, A.S.; Evans, Z.P.; Lauer, A.W.; Patel, R.B.; Ludlow, M.E.; Renne, W.G. Evaluation of the effect scan pattern has on the trueness and precision of six intraoral digital impression systems. J. Esthet. Restor. Dent. 2018, 30, 113–118. [Google Scholar] [CrossRef]
- Ohlmann, B.; Gruber, R.; Eickemeyer, G.; Rammelsberg, P. Optimizing preparation design for metal-free composite resin crowns. J. Prosthet. Dent. 2008, 100, 211–219. [Google Scholar] [CrossRef]
- Henkel, G.L. A comparison of fixed prostheses generated from conventional vs. digitally scanned dental impressions. Compend. Contin. Educ. Dent. 2007, 28, 422–424, 426–428, 430–431. [Google Scholar] [PubMed]
- Ender, A. CEREC Basic Knowledge 4.0 A Clinical Guide. Available online: http://www.zzm.uzh.ch/de/zahnaerzte/kliniken-institute/ppk/cerec.html (accessed on 6 April 2018).
- Ender, A.; Attin, T.; Mehl, A. In vivo precision of conventional and digital methods of obtaining complete-arch dental impressions. J. Prosthet. Dent. 2016, 115, 313–320. [Google Scholar] [CrossRef] [Green Version]
- Joda, T.; Brägger, U. Patient-centered outcomes comparing digital and conventional implant impression procedures: A randomized crossover trial. Clin. Oral Implant. Res. 2016, 27, e185–e189. [Google Scholar] [CrossRef]
- Delize, V.; Bouhy, A.; Lambert, F.; Lamy, M. Intra-subject comparison of digital vs. conventional workflow for screw-retained single implant crowns: Prosthodontic and patient-centered outcomes. Clin. Oral Implant. Res. 2019, 30, 892–902. [Google Scholar] [CrossRef] [PubMed]
- Joda, T.; Brägger, U. Digital vs. conventional implant prosthetic workflows: A cost/time analysis. Clin. Oral Implant. Res. 2015, 26, 1430–1435. [Google Scholar] [CrossRef] [PubMed]
- Benic, G.I.; Mühlemann, S.; Fehmer, V.; Hämmerle, C.H.; Sailer, I. Randomized controlled within-subject evaluation of digital and conventional workflows for the fabrication of lithium disilicate single crowns. Part I: Digital versus conventional unilateral impressions. J. Prosthet. Dent. 2016, 116, 777–782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahrberg, D.; Lauer, H.C.; Ahrberg, M.; Weigl, P. Evaluation of fit and efficiency of CAD/CAM fabricated all-ceramic restorations based on direct and indirect digitalization: A double-blinded, randomized clinical trial. Clin. Oral Investig. 2016, 20, 291–300. [Google Scholar] [CrossRef]
- Christensen, G.J. Will digital impressions eliminate the current problems with conventional impressions? J. Am. Dent. Assoc. 2008, 139, 761–763. [Google Scholar] [CrossRef]
- Patzelt, S.B.; Lamprinos, C.; Stampf, S.; Att, W. The time efficiency of intraoral scanners: An in vitro comparative study. J. Am. Dent. Assoc. 2014, 145, 542–551. [Google Scholar] [CrossRef] [Green Version]
- Sailer, I.; Mühlemann, S.; Fehmer, V.; Hämmerle, C.H.F.; Benic, G.I. Randomized controlled clinical trial of digital and conventional workflows for the fabrication of zirconia-ceramic fixed partial dentures. Part I: Time efficiency of complete-arch digital scans versus conventional impressions. J. Prosthet. Dent. 2019, 121, 69–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seelbach, P.; Brueckel, C.; Wöstmann, B. Accuracy of digital and conventional impression techniques and workflow. Clin. Oral Investig. 2013, 17, 1759–1764. [Google Scholar] [CrossRef]
- Otto, T.; Mörmann, W.H. Clinical performance of chairside CAD/CAM feldspathic ceramic posterior shoulder crowns and endocrowns up to 12 years. Int. J. Comput. Dent. 2015, 18, 147–161. [Google Scholar]
- Wismeijer, D.; Mans, R.; van Genuchten, M.; Reijers, H.A. Patients’ preferences when comparing analogue implant impressions using a polyether impression material versus digital impressions (Intraoral Scan) of dental implants. Clin. Oral Implant. Res. 2014, 25, 1113–1118. [Google Scholar] [CrossRef]
- Lee, S.J.; Gallucci, G.O. Digital vs. conventional implant impressions: Efficiency outcomes. Clin. Oral Implant. Res. 2013, 24, 111–115. [Google Scholar] [CrossRef]
- Wurbs, M.; Simon, J.F.; Troeltzsch, M.; Denekas, T.; Wichmann, M.; Reich, S. Dentist-time expenditure for two different adhesive all-ceramic systems. J. Dent. 2006, 34, 450–453. [Google Scholar] [CrossRef]
- Gozdowski, S.; Reich, S. A comparison of the fabrication times of all-ceramic partial crowns: Cerec 3D vs. IPS Empress. Int. J. Comput. Dent. 2009, 12, 279–289. [Google Scholar] [PubMed]
- Ahlers, M.O.; Mörig, G.; Blunck, U.; Hajtó, J.; Pröbster, L.; Frankenberger, R. Guidelines for the preparation of CAD/CAM ceramic inlays and partial crowns. Int. J. Comput. Dent. 2009, 12, 309–325. [Google Scholar] [PubMed]
- Mehl, A.; Kunzelmann, K.H.; Folwaczny, M.; Hickel, R. Stabilization effects of CAD/CAM ceramic restorations in extended MOD cavities. J. Adhes. Dent. 2004, 6, 239–245. [Google Scholar]
- Kirsch, C.; Ender, A.; Attin, T.; Mehl, A. Trueness of four different milling procedures used in dental CAD/CAM systems. Clin. Oral Investig. 2017, 21, 551–558. [Google Scholar] [CrossRef]
- Mehl, A.; Blanz, V.; Hickel, R. Biogeneric tooth: A new mathematical representation for tooth morphology in lower first molars. Eur. J. Oral Sci. 2005, 113, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Pohlert, T. The Pairwise Multiple Comparison of Mean Ranks Package (PMCMR). Available online: http://CRAN.R-project.org/package=PMCMR (accessed on 6 August 2019).
- R Core Team. A Language and Environment for Statistical Computing. Available online: https://www.R-project.org/ (accessed on 6 August 2019).
- Cayouette, M.J.; Burgess, J.O.; Jones, R.E.; Yuan, C.H. Three-dimensional analysis of dual-arch impression trays. Quintessence Int. 2003, 34, 189–198. [Google Scholar] [PubMed]
- Wesemann, C.; Muallah, J.; Mah, J.; Bumann, A. Accuracy and efficiency of full-arch digitalization and 3D printing: A comparison between desktop model scanners, an intraoral scanner, a CBCT model scan, and stereolithographic 3D printing. Quintessence Int. 2017, 48, 41–50. [Google Scholar]
- Ahlholm, P.; Lappalainen, R.; Lappalainen, J.; Tarvonen, P.L.; Sipilä, K. Challenges of the Direct Filling Technique, Adoption of CAD/CAM Techniques, and Attitudes Toward 3D Printing for Restorative Treatments Among Finnish Dentists. Int. J. Prosthodont. 2019, 32, 402–410. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Ding, Q.; Tang, L.; Zhang, L.; Xie, Q. Accuracy of a chairside fused deposition modeling 3D-printed single-tooth surgical template for implant placement: An in vitro comparison with a light cured template. J. Craniomaxillofac. Surg. 2019, 47, 1216–1221. [Google Scholar] [CrossRef] [PubMed]
- Muta, S.; Ikeda, M.; Nikaido, T.; Sayed, M.; Sadr, A.; Suzuki, T.; Tagami, J. Chairside fabrication of provisional crowns on FDM 3D-printed PVA model. J. Prosthodont. Res. 2020, 64, 401–407. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Material | Name | Brand | |
|---|---|---|---|
| a | flowable composit | Filtek Supreme XTE | 3M ESPE, St. Paul, Minnesota, USA |
| b | PMMA | DD Bio-splint | Dental Direkt GmbH, Spenge, Germany |
| c | light-curing plastic | Freeprint model | DETAX GmbH & Co. KG, Ettlingen, Germany |
| d | intraoral scanner | Cerec Omnicam | Dentsply Sirona, York, Pennsylvania, USA |
| e | intraoral scanner | Trios 3 | 3Shape A/S, Copenhagen, Denmark |
| f | software | CEREC SW 4.5 | Dentsply Sirona, York, Pennsylvania, USA |
| g | software | Trios Design Studio 1.17.2.4 & Sum 3D Dental 6.0.0.0 | 3Shape A/S, Copenhagen, Denmark & CIMsystems.r.l., Cinisello Balsamo, Italy |
| h | milling machine | CEREC MCXL Premium | Dentsply Sirona, York, Pennsylvania, USA |
| i | milling machine | Roland DWX-4W | Roland DG Bene-lux nv, Geel, Belgium |
| j | light-curing one-component material | Telio CS Inlay | Ivoclar Vivadent AG, Schaan, Liechtenstein |
| k | polymerisation lamp | Bluephase Polywave | Ivoclar Viva-dent AG, Schaan, Liechtenstein |
| l | prefabricated temporary composit crowns | Protemp Crown Temporization Material | 3M ESPE, St. Paul, Minnesota, USA |
| m | temporary cement | Temp-Bond | Kerr GmbH, Orange, California, USA |
| n | Feldspar-blank | Vita Mark ll I14 | Vita Zahnfabrik, Bad Säckingen, Germany |
| o | chairside burs | StepBur12; Cylinder Pointed Bur12; Cylinder Bur 12EF; Cylinder Pointed Bur 12EF | Dentsply Sirona, York, Pennsylvania, USA |
| p | chairside burs | 1 mm Round Cylinder; 0.6 Pointed Bur | Roland DG Bene-lux nv, Geel, Belgium |
| q | ceramic polishing cups | Optrafine | Ivoclar Vivadent AG, Schaan, Liechtenstein |
| r | polishing paste | HATHO | Rodent AG, Montlingen, Switzerland |
| s | impression tray | Triple Tray | Premier Dental, Plymouth Meeting, Pennsylvania, USA |
| t | adhesive | Univesal Adhesive | Kulzer GmbH, Hanau, Germany |
| u | low viscosity vinylsiloxanether | Identium Light | Kettenbach GmbH & Co. KG, Eschenburg, Germany |
| v | high viscosity vinylsiloxanether | Identium Heavy | Kettenbach GmbH & Co. KG, Eschenburg, Germany |
| Labside | Chairside | Chairside Working Time | Conventional | |
|---|---|---|---|---|
| Groups | CER_L/TN_L/TI_L | CER_C/TN_C/TI_C | CER_CW/TN_CW/TI_CW | CO |
| Impression | patient administration | patient administration | patient administration | impression-tray try-in |
| scan | scan | scan | tray adhesive | |
| model calculation | model calculation | model calculation | impression taking | |
| CAD | design | design | ||
| CAM | preparation for milling | preparation for milling | ||
| milling | ||||
| Adjustment of the Restoration | remove sprue | remove sprue | ||
| approximal adjustment | approximal adjustment | |||
| occlusal adjustment | occlusal adjustment | |||
| polishing | polishing | |||
| Temporary Restoration | fabrication of a temporary | fabrication of a temporary | ||
| adjustment | adjustment | |||
| remove temporarily | remove temporarily | |||
| cleaning the die | cleaning the die |
| System |
Median (Min: Sec) |
IQR (Min: Sec) | |
|---|---|---|---|
| Labside | CER_L | 09:27 | 01:54 |
| TN_L | 12:07 | 03:02 | |
| TI_L | 12:41 | 02:31 | |
| Chairside | CER_C | 47:00 | 02:50 |
| TN_C | 55:22 | 05:12 | |
| TI_C | 60:38 | 05:24 | |
| Chairside Working Time | CER_CW | 18:32 | 03:13 |
| TN_CW | 21:36 | 05:01 | |
| TI_CW | 25:40 | 05:51 | |
| Conventional | CO | 10:39 | 02:24 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stromeyer, S.; Wiedemeier, D.; Mehl, A.; Ender, A. Time Efficiency of Digitally and Conventionally Produced Single-Unit Restorations. Dent. J. 2021, 9, 62. https://doi.org/10.3390/dj9060062
Stromeyer S, Wiedemeier D, Mehl A, Ender A. Time Efficiency of Digitally and Conventionally Produced Single-Unit Restorations. Dentistry Journal. 2021; 9(6):62. https://doi.org/10.3390/dj9060062
Chicago/Turabian StyleStromeyer, Sofia, Daniel Wiedemeier, Albert Mehl, and Andreas Ender. 2021. "Time Efficiency of Digitally and Conventionally Produced Single-Unit Restorations" Dentistry Journal 9, no. 6: 62. https://doi.org/10.3390/dj9060062
APA StyleStromeyer, S., Wiedemeier, D., Mehl, A., & Ender, A. (2021). Time Efficiency of Digitally and Conventionally Produced Single-Unit Restorations. Dentistry Journal, 9(6), 62. https://doi.org/10.3390/dj9060062