
The Best Dentistry Professional Visual Acuity Measured under Simulated Clinical Conditions Provides Keplerian Magnification Loupe: A Cross-Sectional Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
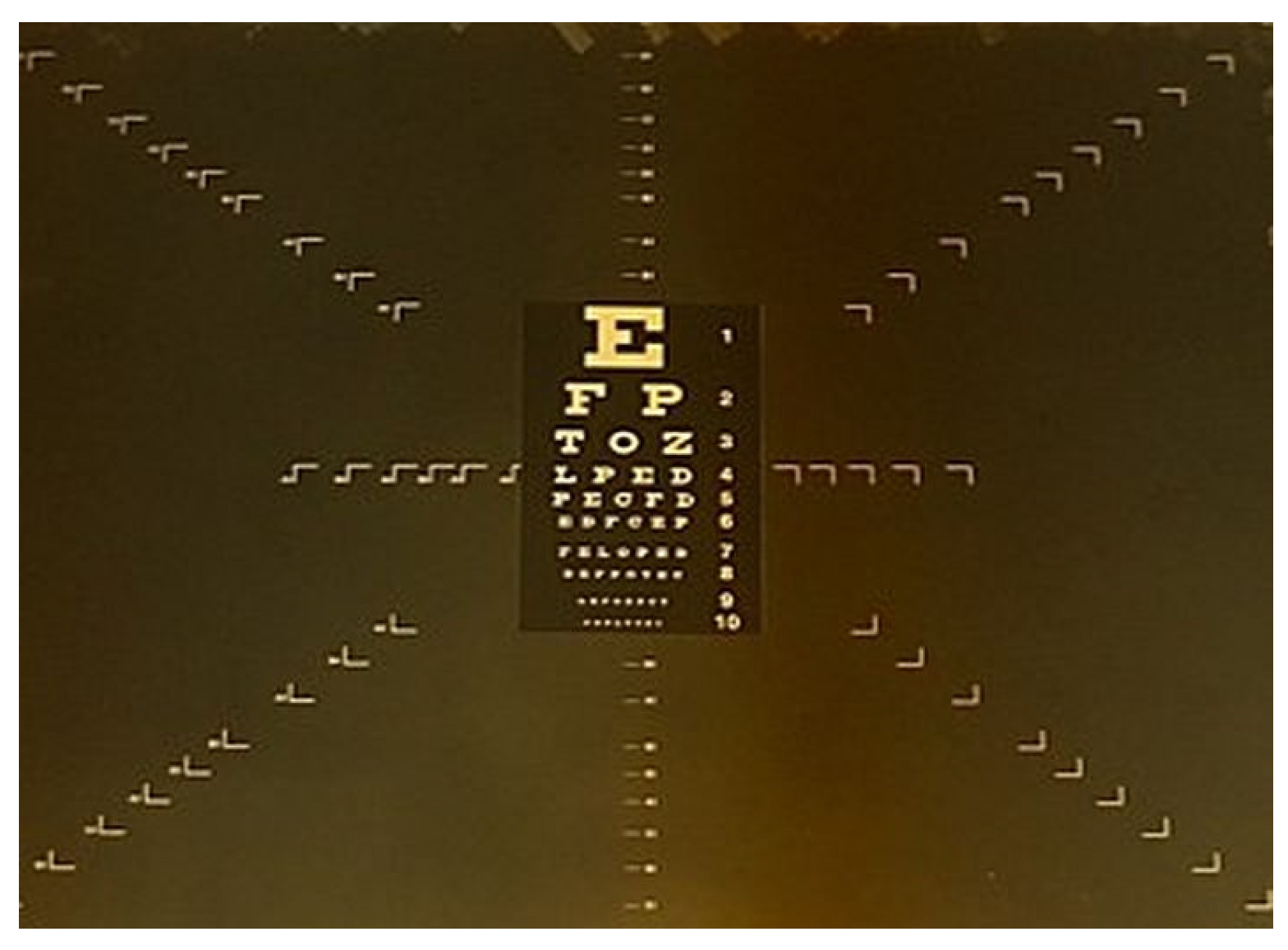
2.2. Miniature Snellen Visual Test
2.3. Dentistry Professional Visual Acuity with Magnification Telescopes
2.4. Statistical Analysis
3. Results
3.1. Standard Deviation of Dentistry Professional Visual Acuity
3.2. The Friedman Test
3.3. The Wilcoxon Signed Rank Test
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Strassler, H.E.; Syme, S.E.; Serio, F.; Kaim, J.M. Enhanced visualization during dental practise using magnification system. Compend. Contin. Educ. Dent. 1998, 9, 595–598. [Google Scholar]
- Sunell, S.; Rucker, L. Surgical magnification in dental hygiene practice. Int. J. Dent. Hyg. 2004, 2, 25–26. [Google Scholar] [CrossRef] [PubMed]
- Syrimi, M.; Ali, N. The role of stereopsis (three-dimensional vision) in dentistry: Review of current literature. Br. Dent. J. 2015, 218, 597–598. [Google Scholar] [CrossRef] [PubMed]
- Syme, S.E.; Fried, J.L.; Strassler, H.E. Enhanced visualization using magnification. J. Dent. Hyg. 1997, 71, 202–206. [Google Scholar] [PubMed]
- Telescopes and Microscopes. Available online: http://electron9.phys.utk.edu/optics421/modules/m3/telescopes.htm (accessed on 1 May 2009).
- Valachi, B. Magnification in dentistry: How ergonomic features impact your health. Dent. Today 2009, 28, 133. [Google Scholar]
- Eichenberger, M.; Perrin, P.; Neuhaus, W.K.; Bringolf, U.; Lussi, A. Visual acuity of dentists under simulated clinical conditions. Clin. Oral Investig. 2013, 17, 725–729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eichenberge, M.; Perrin, P.; Neuhaus, W.K.; Bringolf, U.; Lussi, A. Influence of loupes and age on the near visual acuity of practicing dentists. J. Biomed. Opt. 2011, 16, 035003. [Google Scholar] [CrossRef] [Green Version]
- Perrin, P.; Ramseyer, S.T.; Eichenberger, M.; Lussi, A. Visual acuity of dentists in their respective clinical condition. Clin. Oral Investig. 2014, 18, 2055–2058. [Google Scholar] [CrossRef] [PubMed]
- Christensen, G.J. Magnification in dentistry: Useful tool or another gimmick? J. Am. Dent. Assoc. 2003, 134, 1647–1650. [Google Scholar] [CrossRef]
- Mahmoud, A.L.S. Arabic reading types. BMJ 1986, 70, 314–316. [Google Scholar]
- Urlic, I.; Verzak, Z.; Negovetić, V.D. Measuring the influence of Galilean loupe system on near visual acuity under simulated clinical conditions. Acta Stomatol. Croat. 2016, 3, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.M.; Chandler, N.P. Magnification: Magnifying the point. BDJ 2015, 218, 369. [Google Scholar] [CrossRef] [PubMed]
- Eichenberger, M.; Perrin, P.; Ramseyer, S.T.; Lussi, A. Visual acuity and experience with magnification devices in Swiss dental practices. Oper. Dent. 2015, 40, E142–E149. [Google Scholar] [CrossRef] [PubMed]
- Wajngarten, D.; Garcia, P.P.N.S. Effect of magnification devices on dental students’ visual acuity. PLoS ONE 2019, 14, e0212793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perrin, P.; Neuhaus, K.W.; Lussi, A. The impact of loupes and microscopes on vision in endodontics. Int. Endod. J. 2014, 47, 425–429. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Optical System | N | Mean | Std Dev | CV (%) | Median | Q1 | Q3 | Min | Max |
|---|---|---|---|---|---|---|---|---|---|
| VSC | 46 | 0.411 | 0.074 | 17.9 | 0.4 | 0.4 | 0.5 | 0.3 | 0.6 |
| VNL | 46 | 0.504 | 0.076 | 15.0 | 0.5 | 0.5 | 0.6 | 0.4 | 0.7 |
| VGA 2,5 | 46 | 0.517 | 0.077 | 14.9 | 0.5 | 0.5 | 0.6 | 0.4 | 0.7 |
| VKP 3,3 | 46 | 0.541 | 0.086 | 15.9 | 0.6 | 0.5 | 0.6 | 0.4 | 0.7 |
| VKP4,5 | 46 | 0.646 | 0.081 | 12.5 | 0.6 | 0.6 | 0.7 | 0.5 | 0.8 |
| Optical System Comparison | Test Statistics W | p-Value |
|---|---|---|
| VNL vs. VSC | 390,0 | <0.001 |
| VGA 2,5 vs. VSC | 403,5 | <0.001 |
| VKP 3,3 vs. VSC | 423,0 | <0.001 |
| VKP4,5 vs. VSC | 517,5 | <0.001 |
| VGA 2,5 vs. VNL | 22,5 | 0.288 |
| VKP 3,3 vs. VNL | 103,5 | 0.014 |
| VKP4,5 vs. VNL | 473,0 | <0.001 |
| VKP 3,3 vs. VGA 2,5 | 55,0 | 0.064 |
| VKP4,5 vs. VGA 2,5 | 480,5 | <0.001 |
| VKP4,5 vs. VKP 3,3 | 430,5 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Urlic, I.; Pavan, J.; Verzak, Z.; Karlovic, Z.; Negovetic Vranic, D. The Best Dentistry Professional Visual Acuity Measured under Simulated Clinical Conditions Provides Keplerian Magnification Loupe: A Cross-Sectional Study. Dent. J. 2021, 9, 69. https://doi.org/10.3390/dj9060069
Urlic I, Pavan J, Verzak Z, Karlovic Z, Negovetic Vranic D. The Best Dentistry Professional Visual Acuity Measured under Simulated Clinical Conditions Provides Keplerian Magnification Loupe: A Cross-Sectional Study. Dentistry Journal. 2021; 9(6):69. https://doi.org/10.3390/dj9060069
Chicago/Turabian StyleUrlic, Iris, Josip Pavan, Zeljko Verzak, Zoran Karlovic, and Dubravka Negovetic Vranic. 2021. "The Best Dentistry Professional Visual Acuity Measured under Simulated Clinical Conditions Provides Keplerian Magnification Loupe: A Cross-Sectional Study" Dentistry Journal 9, no. 6: 69. https://doi.org/10.3390/dj9060069
APA StyleUrlic, I., Pavan, J., Verzak, Z., Karlovic, Z., & Negovetic Vranic, D. (2021). The Best Dentistry Professional Visual Acuity Measured under Simulated Clinical Conditions Provides Keplerian Magnification Loupe: A Cross-Sectional Study. Dentistry Journal, 9(6), 69. https://doi.org/10.3390/dj9060069